Back to Journals » Patient Preference and Adherence » Volume 13
Patient Perspectives on Factors Influencing Medication Adherence Among People with Coronary Heart Disease (CHD) and CHD Risk Factors
Authors Mondesir FL, Levitan EB ![]() , Malla G, Mukerji R, Carson AP, Safford MM, Turan JM
, Malla G, Mukerji R, Carson AP, Safford MM, Turan JM
Received 6 July 2019
Accepted for publication 25 October 2019
Published 29 November 2019 Volume 2019:13 Pages 2017—2027
DOI https://doi.org/10.2147/PPA.S222176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Favel L Mondesir,1 Emily B Levitan,2 Gargya Malla,2 Reshmi Mukerji,3 April P Carson,2 Monika M Safford,4 Janet M Turan5
1Division of Cardiovascular Medicine, School of Medicine, University of Utah, Salt Lake City, UT, USA; 2Department of Epidemiology, School of Public Health, University of Alabama at Birmingham, Birmingham, AL, USA; 3School of Medicine, Department of Microbiology, University of Alabama at Birmingham, Birmingham, AL, USA; 4Department of Medicine, Weill Cornell Medicine, New York, NY, USA; 5Department of Health Care Organization and Policy, School of Public Health, University of Alabama at Birmingham, Birmingham, AL, USA
Correspondence: Favel L Mondesir
Division of Cardiovascular Medicine, School of Medicine, University of Utah, Room 4A100, 30 N 1900 E, Salt Lake City, UT 84132, USA
Tel +1-801-587-9048
Email [email protected]
Background: Few qualitative studies have explored factors influencing medication adherence among people with coronary heart disease (CHD) or CHD risk factors. We explored how factors related to the patient (e.g. self-efficacy), social/economic conditions (e.g. social support and cost of medications), therapy (e.g. side effects), health condition (e.g. comorbidities), and the healthcare system/healthcare team (e.g. support from healthcare providers and pharmacy access) influence medication adherence, based on the World Health Organization Multidimensional Adherence Model (WHO-MAM).
Methods: We conducted 18 in-depth qualitative interviews from April to July 2018 with ambulatory care patients aged ≥45 years (8 black men, 5 black women, 2 white men, and 3 white women) who were using medications for diabetes, hypertension, dyslipidemia and/or CHD. We used thematic analysis to analyze the data, and sub-themes emerged within each WHO-MAM dimension.
Findings: Patient-related factors included beliefs about medications as important for self and faith; the desire to follow the advice of family, friends, and influential others; and self-efficacy. Social/economic factors included observations of social network members and information received from them; social support for medication adherence and pharmacy utilization; and economic influences. Therapy-related barriers included side effects and medicine schedules. Only a few participants mentioned condition-related factors. Healthcare system/healthcare team-related factors included support from doctors and pharmacists; and ease of pharmacy access and utilization.
Conclusion: These results underscore the need for multidimensional interventions aimed at improving medication adherence and overall health of patients with CHD and CHD risk factors.
Keywords: medication adherence, qualitative research, coronary heart disease, diabetes, hypertension, dyslipidemia
Introduction
According to the American Heart Association, heart disease is the leading cause of death in the US, with direct and indirect costs of cardiovascular disease (CVD) projected at $749 and $368 billion respectively, by 2035.1 Coronary heart disease (CHD), the principal cause of CVD deaths, accounts for 43.2% of those deaths.1 Yet, a meta-analysis revealed that medications which reduce the risk of CHD events and mortality are taken as prescribed by only 50–66% of patients with CHD and CHD risk factors.2
The World Health Organization Multidimensional Adherence Model (WHO-MAM) emphasizes 5 dimensions which interact to influence medication adherence: patient-related factors including self-efficacy, perceived health, beliefs about the efficacy of medications and knowledge of medications; social/economic factors including social support, family functioning, and costs; therapy-related factors including side effects and dose complexity; condition-related factors including comorbidities; and healthcare system/healthcare team-related factors including support from healthcare providers, negative interactions with providers, and pharmacy access.
Qualitative studies conducted separately among people with hypertension, diabetes, heart failure, and following percutaneous coronary intervention also revealed the multidimensional nature of medication adherence.3–7 One systematic review of quantitative studies using the WHO-MAM found that patient-related barriers to anti-hypertensive medication use were studied more frequently than social/economic, therapy, and condition related factors.8 The findings from other prior quantitative studies indicated that factors within all dimensions of the WHO-MAM influenced medication adherence among people with CVD, diabetes, heart failure, and those who took cholesterol medications.9–12
However, few qualitative studies have focused on barriers to medication adherence among a racially diverse group of participants with more than one CHD risk factor in one of the states of the US Deep South region (Georgia, Alabama, South Carolina, Mississippi, and Louisiana) where Christianity is at the forefront of daily living and strongly influences family life and values.13 There is a need for additional data on patient perspectives and factors influencing medication adherence (both barriers and facilitators) in people with a combination of risk factors such as diabetes, hypertension, dyslipidemia, and/or CHD. These data may inform the development of interventions to improve medication adherence among people with CHD and CHD risk factors. Coupled with this is the need for further studies of social/economic, therapy and healthcare system/healthcare team-related factors which influence medication adherence in this population. Therefore, we explored how these factors at multiple levels influence medication use among people who use medications for diabetes, hypertension, dyslipidemia, and/or CHD, guided by the WHO-MAM.
Methods
Sampling and Recruitment
Ambulatory patients who used prescribed medications for diabetes, hypertension, dyslipidemia and/or CHD were recruited from the University of Alabama at Birmingham Health System’s Endocrinology and Cardiology clinics between April and July 2018. We used purposive sampling,14,15 while considering data saturation, to recruit equal numbers of men and women who self-identified as black or white and who were aged ≥ 45 years Purposive sampling was employed to be similar to the demographic distribution of the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, an on-going cohort study of black and white men and women, which our team has used to quantitatively study barriers to medication adherence in people with CHD and CHD risk factors.16 The burden of CHD and CHD risk factors increases with age; therefore, adherence to medications for diabetes, hypertension, dyslipidemia, and/or CHD is most relevant in this age group.1
One member of the study team (FLM) recruited participants and conducted the interviews. The electronic health records for patients of two clinician investigators at the Endocrinology and Cardiology clinics were initially screened for potential participants aged ≥ 45 years with a diagnosis of diabetes, hypertension, dyslipidemia, and/or CHD. These two specialty clinics were chosen because in combination, their patient population includes patients with more severe diabetes, hypertension, dyslipidemia and/or CHD who were, therefore, at greater risk of CHD events compared to those of primary care clinics. Potential participants were screened by phone and invited to participate if they were ≥ 45 years, of black or white race and self-identified as having and using medications for diabetes, hypertension, dyslipidemia, and/or CHD. Twenty-two participants were recruited; however, one did not participate due to scheduling difficulties, one was unwilling to sign the consent form, and two could not be re-contacted to schedule the study visit, resulting in a sample of 18 participants. Participants were given a $20 Visa gift card incentive.
Data Collection
Study visits were scheduled to coincide with regular clinic visits and were conducted in a private area in the clinic building. Participants completed a brief demographic questionnaire and participated in individual face-to-face in-depth interviews which lasted about 40 mins on average. A semi-structured interview field guide with open-ended questions was initially designed to assess how social support and pharmacy access influence medication use among people with CHD and CHD risk factors. However, the findings revealed that factors influencing medication use were more multi-faceted and encompassed patient, social/economic, therapy, condition, and healthcare system/healthcare team-related factors. Interviews were audio-recorded and transcribed verbatim. We conducted pilot interviews with two healthcare providers (a physician and a pharmacist) to assess the appropriateness of the interview guide questions. Additionally, we probed more deeply on social support, pharmacy access, perceived health, perceived importance of treatment, and patient-provider relationships, as the interviews progressed based on findings from the initial interviews indicating the importance of these themes.
Digital recorders were handled only by study personnel and kept in a locked drawer when not in use. Interviews were transcribed by a professional Health Insurance Portability and Accountability Act (HIPAA) compliant company, ensuring that all identifying information was removed from the transcripts. Further, all qualitative data were stored on password-protected computers. Paper records and completed demographic questionnaires were stored in secure filing cabinets. The study protocol was approved by the Institutional Review Board at the University of Alabama at Birmingham and all participants provided written informed consent.
Data Analysis
We employed an inductive thematic analysis approach to analyze and code the transcripts and identify themes within the data (Table 1).17 Themes were identified at the semantic level with a focus on the surface meaning of participants’ words as opposed to deeper assumptions or ideas of what those words might mean.17 Broad and fine codes were initially created by one researcher (FLM) using an a priori list of codes based on, the interview guide, and an initial examination of the data. These broad codes were discussed with two other members of the study team (GM and RM). Based on this discussion, the codes were modified and then discussed with the rest of the investigative team. Three researchers (FLM, GM and RM) coded the transcripts using NVivo version 12, a computer-assisted qualitative data analysis software package.
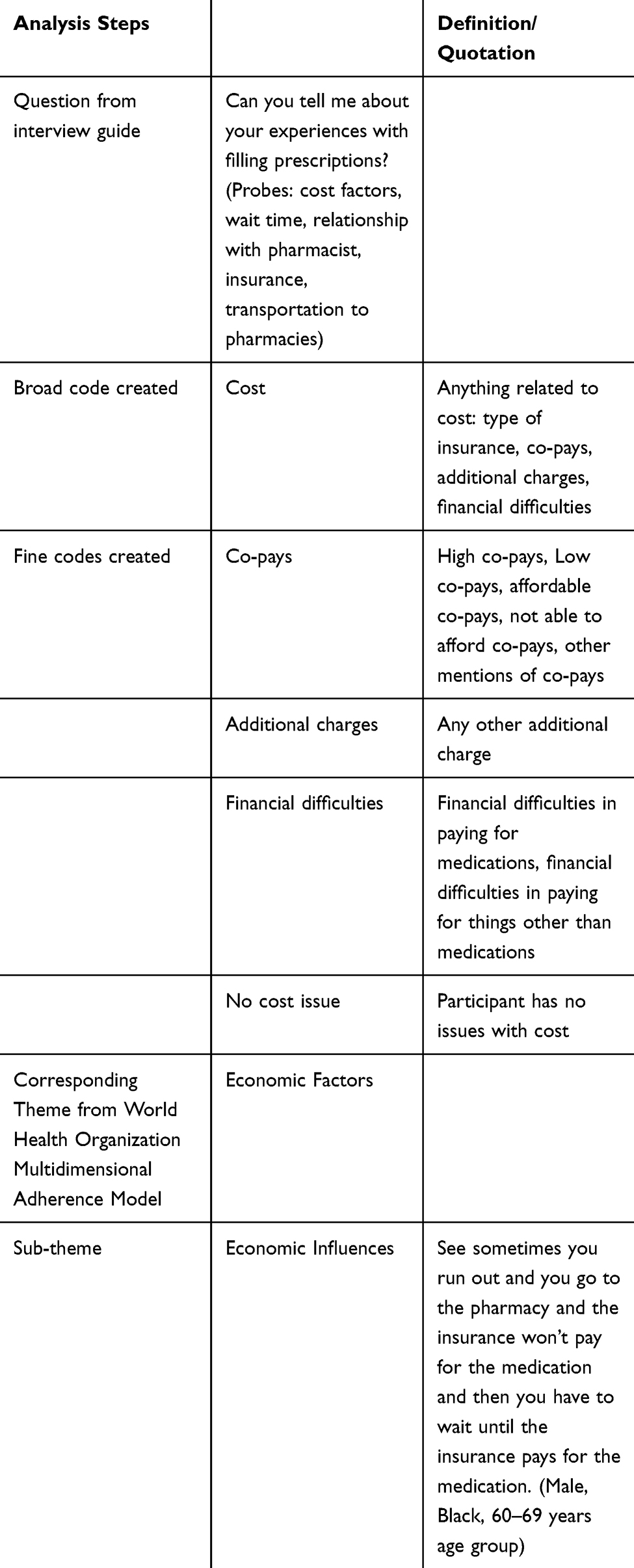 |
Table 1 Example of How Thematic Analysis Was Used |
The coding process was iterative. This facilitated discussions, changes, and clarifications during the coding process and resulted in the development of additional codes. One transcript was initially triple coded to establish agreement on coding definitions. Discrepancies were resolved through discussion by coding team members. A second transcript was also triple coded after resolving discrepancies. This further increased reliability and substantiated codebook definitions. For the remaining transcripts, each coder focused on a specific set of codes. We used the WHO-MAM to structure an initial analytical report of the results based on the emerging themes and sub-themes from the data. However, the data that emerged on condition-related factors were limited. Therefore, this WHO-MAM dimension was not analyzed in detail. The analytical report was shared with other members of the research team; this generated more ideas and comments, which were incorporated into the report.
Findings
The mean age of participants was 57.7 years (SD = 8.0) and most identified as black (13 of 18) and male (10 of 18) (Table 2). All participants had health insurance with prescription drug coverage (Table 1). Participants described many factors that influenced their medication use both positively and negatively. There were 2–4 sub-themes which emerged from the data within each WHO-MAM dimension. Patient-related factors included beliefs about medications as important for self and faith; the desire to follow the advice of family, friends, and influential others; and self-efficacy. Social/economic factors included observations of social network members and information received from them; social support for medication adherence and pharmacy utilization; and economic influences. Therapy-related barriers included side effects and medicine schedules. Only a few participants mentioned condition-related factors. Healthcare system/healthcare team-related factors included support from doctors and pharmacists; and ease of pharmacy access and utilization.
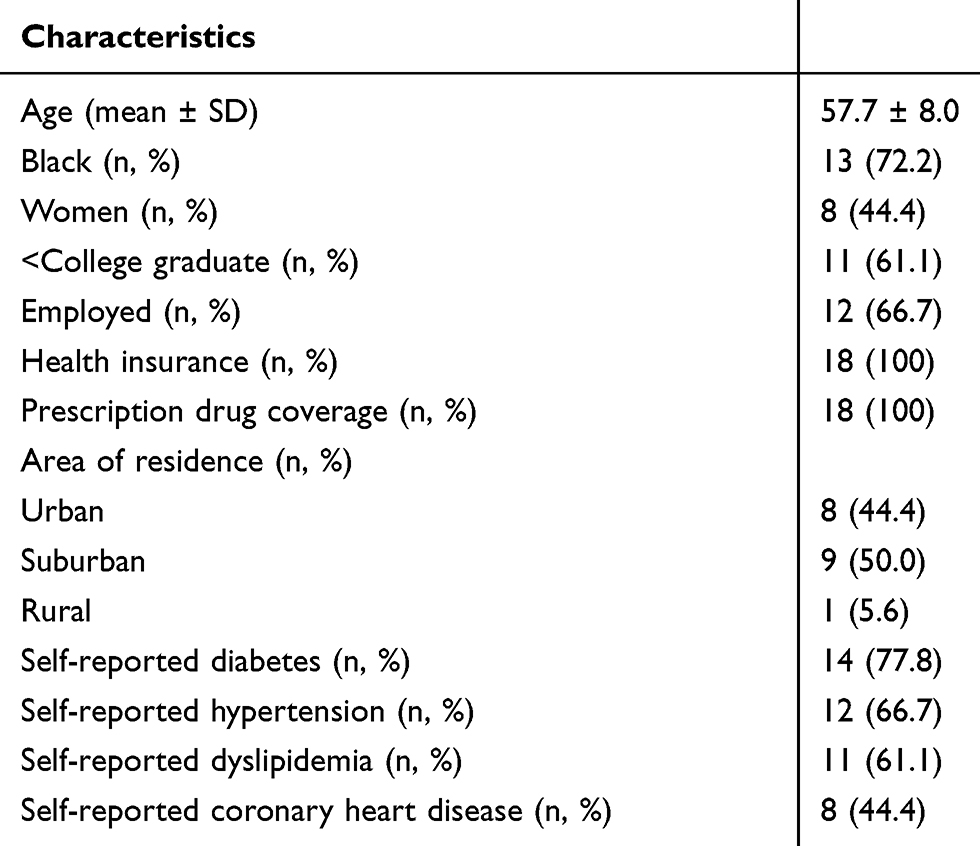 |
Table 2 Characteristics of the Study Participants (N =18) |
Patient-Related Factors
Beliefs About Medications as Important for Self and Faith
A few participants noted that because of their faith in God, they felt that they knew that the medications would work. These participants described needing to take their medications as prescribed in order to carry out God’s will.
This is what I need to do. I have to remind myself that God blesses obedience. If I’m not going to take the medicine like it’s instructed, then I don’t need to waste the doctor’s time or my money. So that’s what pushes me to take it … (Female, Black, 60–69 years age group)
Some participants also felt that taking medications was important to be able to work, to maintain health, and to feel good; leading to better adherence.
My appetites have changed, my relationship to my medication, the whole protocol of taking care of myself really is front and center. It’s very important to watch what I’m eating, watch my exercise, make sure that I’m doing the medicine, the insulin protocol correctly … So it’s just something I realized how important it is to do, so I’m always doing that. (Male, White, 60–69 years age group)
However, there were participants who expressed that it was “overwhelming” and difficult to take medications in the right way every time although they believed it was the right thing:
And I think some of it is, when you have a chronic illness, you want to do the right thing but it’s just overwhelming to take all your medicines and do everything just right every day. It’s just to me difficult … sometimes I’m immaculate with taking my medication, and I don’t miss a dose. And then sometimes I just can’t swallow another pill. (Female, Black, 60–69 years age group)
Desire to Follow the Advice of Family, Friends, and Influential Others
We explored how relationships with family members, friends, and others influence medication beliefs among people who took medications for CHD and CHD risk factors.
A few participants noted that they took their medications because their pastor and fellow members of their congregation repeatedly suggested that they should.
… they [church members] pray for us … They always talk about they want me to get healed, so yeah, they’re very supportive … my pastor always says take your medicine. So, even though you’ve got prescribed medicine make sure you take it … (Male, Black, 40–49 years age group)
Self-Efficacy
Participants’ stories revealed that self-efficacy played a role in their decisions regarding obtaining and using their medications. A sense of self-confidence in achieving the goals of accessing and using the medications, employing lifestyle changes related to their conditions, and feeling better because of those events were seen as leading to better adherence.
Most of the participants explained that they picked up their own medications from the pharmacy.
Most of the time, I usually pick up my own medicine. So, I pick it up even when I’m at work. (Male, Black, 50–59 years age group)
One participant expressed that she was independent when it came to taking her medications.
I’m totally independent when it comes to that. I’m not dependent upon someone else telling me to take my medication. (Female, White, 60–69 years age group)
Aside from taking medications, some participants identified lifestyle changes they had to make as part of self-management of their conditions.
Diet, exercise, and pretty much medication. Make sure you take your medicine that’s required. Basically yes, the food, the exercise, and the constantly taking medicine. That has had to be a change. These are how to classes on how to eat better, how to take your insulin, because I didn’t start off with insulin. How to cook, well not really cook, but how to read your labels with foods. (Female, Black, 60–69)
Social/Economic Factors
Observations of Social Network Members and Information Received from Them
A few participants received information and observed behavior around medication use from friends who also used the same medications, which positively influenced their beliefs about medications.
My best friend, she is on one of the same meds that I take. I ask her how did the medicine make her feel? She gave me her opinion on how it makes her feel. I said, ‘It’s okay. I see now. I felt the same way … ’ (Female, Black, 50–59 years age group)
Social Support for Medication Adherence
Some participants talked about receiving emotional support (receiving encouraging words, hope and care provided and having someone to listen) from family members, friends, or others, which helped them cope with the daily stresses and challenges of their conditions.
But they [family members] are constantly encouraging me and asking about my progress … They influence me by saying stuff, giving me compliments like, ‘You’re really doing good.’ Or whatever. That’s about the influence. (Female, Black, 60–69 years age group)
Many participants also talked about receiving functional support (having someone to pick up medications, to provide reminders about medications, to provide financial help, to care for you, provide food or take you to the doctor when sick) from family members, friends or others, which they cited as helping with their medication adherence.
But I had my friend, she would set my medicine out and stuff like that … You know, like set it up for the week. She’d be right there with me. So, that when things would happen to me where I couldn’t set my medicine out, I’d have her to set it out … (Male, Black, 50–59 years age group)
Some have roles that they feel are important to the functioning of their family and thus promoted medication adherence.
… I have two sisters and a mother that’s 86 years old, I know I need to be around because they need me for certain things. Cut the grass or do some carpenter work on the house, whatever they need I know that’s my job. (Male, Black, 60–69 years age group)
Social Support for Pharmacy Utilization
Many participants also received functional support from family members, friends, or others specifically in relation to pharmacy access and utilization.
… my husband … if I don’t have time to run to the pharmacy and he’s out and about, can you pick up my meds? … he helps in picking up medication, and at nighttime, if I’m exhausted or my muscles are tired, and I’m really sore, and I’m not moving very fast, he can grab stuff for me. (Female, White, 40–49 years age group)
Economic Influences
All participants expressed that they had health insurance coverage for prescribed medications and that most of them were able to afford their medication copays.
… the insurance cover what they going to cover. Now, I usually get that money back after I do a refund form that I send back to the health provider. And I get sent money back on what the prescription costs. (Male, Black, 50–59 years age group)
However, one participant explained that he did not have medication because he sometimes had to wait for his insurance to pay for the medications. He shared his experience as follows:
See sometimes you run out and you go to the pharmacy and the insurance won’t pay for the medication and then you have to wait until the insurance pays for the medication. (Male, Black, 60–69 years age group)
Another participant described the experiences of other people he knows who had financial difficulties and had to make decisions about which medications to get.
I’ve talked with people who are diabetic and financially there have been times when they’ve had to make some decisions of what medicine to get or whatever, and it’s not just with diabetes it’s period. (Male, Black, 50–59 years age group)
Therapy-Related Factors
Side Effects
One participant described the experiences of other people who had side effects from their medications. He noted that they stopped the medications for a short period of time but resumed because of their beliefs in the importance of taking their medication.
I’ve had people that have had bad experiences. Sometimes some of the insulin will disrupt their digestive system. Metformin I think is probably one of the most common that people take that they’ve said they experienced some digestive issues. That’s one of the side effects of it, but it is what it is … They’ll discontinue it maybe for like a couple hours or a day or so, but then they know that they have to take the medicine. It’s not an option. (Male, Black, 50–59 years age group)
One participant explained that she had side effects from medication that were not adequately addressed by her doctors. This had a negative influence on her medication adherence:
I take Simvastatin or Zocor or something, one of the statin drugs. I think that was the beginning of my muscle problems, when I started to take that. So as a result, I will not take that on a regular basis … With that medication … I have talked to the eye doctor, the GYN [gynecologist], the internal medicine, I’ve talked to everyone about it, and they kind of just brush it off. Like no big deal, why are you worried about that? … But then I got that letter from [name of public health institute] or somewhere that says, was the combination of the high dose of my Benazepril or whatever medication I was on, and the Simvastatin that was causing muscle atrophy, and nobody had shared that with me, and they just discounted it. (Female, Black, 60–69 years age group)
Medicine Schedules
One participant expressed that although she only takes two medications, they are on different schedules. Therefore, she has to go to the pharmacy twice per month, which is inconvenient.
I do the two, pretty much those are the only two medicines that I’m on, and I can’t get them both at the same time. So at least twice a month I’m having to do one or the other … (Female, Black, 60–69 years age group)
Healthcare System/Healthcare Team-Related Factors
Support from Doctors and Pharmacists
Many participants cited that their beliefs regarding the efficacy of medications were the result of having a good relationship with and support of doctors in relation to their conditions and medications; this had a positive influence on their medication adherence.
Yes, [doctors] they have been very helpful in providing and suggesting the medications that I take and have always cared about how it has affected after I’ve started taking it, how it’s affected the problem. (Female, White, 60–69 years age group)
One participant noted that his faith/trust in doctors made it easier for him to take his medications because the doctor said to do so.
Well, the doctor is the doctor, so if he tells me I need to take something that’s telling me he’s concerned about my health - my overall health. (Male, Black, 60–69 years age group)
Many participants also cited that receiving information from pharmacists positively influenced their beliefs about medications and improved medication adherence.
Oh I will speak to any pharmacy. I will pick up a telephone and just dial any pharmacist and ask them about a medication, so it doesn’t matter … While I’m at work, I’ll overhear a pharmacist talking to a patient about medicines, and I’ll listen to that too. So I try to gather information from a lot of places. (Female, Black, 60–69 years age group)
Many participants cited that having a good relationship with their doctors helped to promote their medication adherence.
Oh, I’m close to all of my providers. Yeah. I’ve got a doctor for probably every part of my body, but my cardiologist, my oncologist, one of my surgeons … I have a close relationship to. I can call them, and they’ll call me … Well, get back with me. I’ve got a good group that I can discuss things with, and I’ve used the patient portal to ask questions as well just like I can send a question to my primary and she’ll get back with me within 24 hours. (Female, Black, 50–59 years age group)
Additionally, many participants expressed the opinion that having a good relationship with pharmacists helped to promote their medication adherence.
They have my prescription history. If I have questions they can look back and ask me anything, answer questions for me. But yeah, I think it just makes it a lot simpler for me. (Female, Black, 40–49 years age group)
Clinical support from doctors was also identified as being beneficial in promoting medication adherence among interviewed participants.
I have a good team of doctors that I like, and that’s hard to find some doctors that you really have confidence in. Even when I had the surgery, everything just went smooth. My family doctor is a good doctor. My cardio doctor, and the surgeon that did the surgery is a good doctor. (Male, Black, 50–59 years age group)
However, some participants mentioned having negative interactions with their providers which in some cases negatively affected medication adherence.
We’ve only had to terminate our relationship with one specialist, and it wasn’t because they were not doing their job, it was because the head nurse was not doing their job … So, I had to terminate that relationship last year. Because she was calling in prescriptions that were not approved for me and sending me into a tailspin … And so we had to fire them. And that is the only bad experience I’ve had. (Female, White, 40–49 years age group)
Ease of Pharmacy Access and Utilization
Most participants noted that the ease of getting to the pharmacy (transportation availability, close distance and short time to pharmacy and lower number of pharmacies used) resulted in improved medication access.
My pharmacist is about probably four to five minutes from my home. I used the pharmacist right there in my neighborhood, and this is literally less than five minutes from my house. (Female, Black, 50–59 years age group)
Most interviewed participants had no travel concerns in getting to the pharmacy.
Not in that small little town. No, I feel pretty safe and secure … Bad roads? We’re lucky too. We live in the city, within the city limits. The neighborhood we live in the city maintains streets and all that stuff. (Female, White, 70–79 years age group)
A few black participants talked about having some minor travel concerns in getting to the pharmacy. However, they did not report an effect on medication adherence.
… the way I would normally go to [name of pharmacy2], you have to go down this other long street, which is a straight shot. There are not lights or anything on [name of street2]. I just don’t like it. They don’t ever have to worry about me being on [name of street2] at night, because there are basically no lights on [name of street2] … So I would rather go all the way around [name of street1] and come back up the lighted area where I know there’s a lot of traffic, because it’s not going to be that much on [name of street2] … (Female, Black, 60–69 years age group)
For participants who used mail order pharmacies, the cheaper cost of this service compared to getting medications at physical pharmacy locations was cited as a reason for using mail order pharmacies. They noted that this led to improved medication access and adherence.
The cost that I’ve gotta pay today. The mail order, I’ll order and I’ll save maybe five dollars … I have one drug like that. So if I mail order it, I know that’s gonna save me so I can go ahead on and order two, three other drugs also, if I do that. (Male, Black, 60–69 years age group)
One participant who used mail order pharmacies cited the convenience of having the medications delivered to their homes as facilitating medication access and adherence.
You don’t have to get out and drive. They come right to your mailbox, and it’s always refrigerated when it comes, very helpful. (Female, White, 60–69 years age group)
On the other hand, some participants who did not use mail order pharmacies shared the perspective that the service results in inconvenience because of the possibility of receiving the wrong medication. This medication would have to be mailed back causing medication access and adherence to be negatively affected.
I always said to myself could they send you the wrong prescription and you have to send it back or the dose might not be right, so I’d rather go pick it up in person. (Male, Black, 50–59 years age group)
Some participants cited a lack of privacy as a reason for not using mail order pharmacies. They noted that sometimes mail is delivered to the wrong mailbox and by extension, their medications are easily accessible to others. For them, use of the mail order service could result in poor medication access and adherence.
I don’t like the idea of medication coming in through the mail and someone … having a missed package or having someone rifle through our mailbox. (Female, White, 40–49 years age group)
Discussion
In the current study, black and white men and women with CHD and CHD risk factors shared perceptions and experiences on how beliefs about medications, relationships with different people or organizations, and pharmacy access and utilization influence their medication use. These perceptions and experiences occurred within the dimensions of the WHO-MAM: patient; social/economic; therapy; and healthcare system/healthcare team. The current study included a racially diverse group of participants from the US Deep South region, with participants being black and white men and women aged 45 and older with a combination of risk factors (diabetes, hypertension, dyslipidemia, and/or CHD).
The results of the current study are similar to that of prior qualitative studies focused on barriers and facilitators of medication adherence in different patient groups. A qualitative study by Johnson et al found that a belief in the efficacy of medications facilitated medication adherence while inability to access medications and forgetting were barriers to medication adherence among older patients with hypertension.5 Ogedegbe et al, in a qualitative study, showed that medication adherence barriers included patient, therapy and condition related barriers among African American patients with hypertension while facilitators included use of reminders, knowledge about condition, having social support and good communication with doctors.6 Another qualitative study conducted among patients with heart failure indicated that facilitators of medication adherence were a desire to be healthy, having a knowledge of disease and symptoms, and having a good relationship with family members as well as health care providers.3 Further, a recent qualitative study by Pettersen et al found that lack of knowledge about disease severity, side effects of medications and poor informational support from providers acted as barriers to medication adherence among people who had their first percutaneous coronary intervention.4 Additionally, Shiyanbola et al showed that among African Americans with diabetes, medication adherence barriers included side effects and lack of access to medications while facilitators included trusting the recommendations of doctors and the need to be healthy and alive to perform roles that participants felt were important to the functioning of the family.7 The combination of these findings indicate that while medication adherence is part of a complex process, that process may be similar across different CVD-related conditions.
The current study findings are also in line with results from a systematic review of quantitative studies focused on barriers to medication adherence among people who took antihypertensive medications.8 This review found that patient-related factors (e.g. self-efficacy, patient’s knowledge and beliefs about medication), social/economic factors (e.g. social support and cost of medications), therapy-related barriers (e.g. medication side effects, medication efficacy and dose complexity), condition-related factors (e.g. ability to open or close the medication bottle, perceived health and severity of symptoms), and healthcare system/healthcare team-related barriers (e.g. medication reimbursement and poor patient-provider relationships) were influences on medication adherence.8 Similar to the current study, the systematic review did not find support for factors such as patient’s beliefs about nonadherence, lack of health literacy, lack of medical support for dealing with side effects, and distance from healthcare facilities as barriers to medication adherence.8
In another systematic review of quantitative studies investigating barriers to medication adherence among older adults (aged ≥ 65 years), patient-related factors included disease-related knowledge, health literacy, and cognitive function.11 These results were in contrast with that of the current study (average age of participants = 57.7), but such differences may be the result of the differing ages of the study participants, as older retired patients may be more likely to experience cognitive decline and encounter the added burden of logistical barriers due to their age11 and health conditions. Social/economic factors in this systematic review included cost of medications and therapy-related factors included medication side effects.11 Healthcare system/healthcare team-related factors included poor patient-provider relationships, lack of transportation to the pharmacy and not having health insurance coverage for medications.11 There were similarities with the results of the current study; medication side effects and poor patient-provider relationships emerged as important barriers to medication adherence. The combination of these results suggests that certain healthcare system/healthcare team-related factors may act as barriers irrespective of age.
In other quantitative studies of barriers to medication adherence among people with CVD, poorly controlled diabetes, advanced heart failure, or medication-treated high cholesterol, common factors such as lack of social support, cost of medications, and medication side effects were associated with low medication adherence.9,10,12,18,19 The barriers to medication adherence in people with CVD and CVD risk factors found in these studies were similar to those discussed by the participants in the current study. The results of these studies also indicated that perceived health, perceived importance of treatment, remembering doses, difficulty swallowing medications, and depression were not actually associated with lower medication adherence; these factors also failed to emerge in the present study.9,10,12,18,19 We may not have observed the emergence of some of these factors because we did not specifically probe for them, but we did probe on perceived health, perceived importance of treatment, and patient-provider relationships; the quantitative nature of the prior studies compared to the qualitative nature of the current study may have contributed to the differences. The patient populations may also have contributed to differences, since our sample was recruited from specialty clinics, which may attract more adherent patients who already understand the seriousness of their disease and the benefits of medications.
In two past studies in a large national cohort of community-dwelling adults, seeing more than ten friends or relatives at least monthly was associated with higher medication adherence16 while pharmacy access based on geography was not associated with medication adherence among people with diabetes, hypertension, dyslipidemia, and/or CHD.20 Our study supported both of these findings, but it is important to bear in mind that all participants in the current study had ease of pharmacy access which may have affected the results.
Limitations
This study’s strengths include the in-depth understanding of how theoretically important factors can influence medication adherence among people who not only have prescription drug coverage but also have access to the pharmacy. Few qualitative studies have focused on black and white men and women aged 45 and older with multiple CHD risk factors from the US Deep South region. The use of in-depth interviews as opposed to focus groups helps to mitigate social desirability bias, as some participants may not want to admit to not taking their medications in the presence of other patients. Our findings should also be interpreted in light of some limitations. The findings may not be representative of all black and white men and women aged 45 years and older with CHD or CHD risk factors. Importantly, all study participants had health insurance and prescription drug coverage. There was also limited variability in participants’ experiences related to physical access to the pharmacy. Additionally, while the current study included participants with CHD or CHD risk factors, other comorbidities may have influenced perceptions about medication adherence. Our results included few findings on condition-related factors, therefore, we could not draw any conclusions for this WHO-MAM dimension. In addition, participants were from two university specialty care clinics; this suggests that the patients may be highly motivated as they complied with recommendations to seek specialist care. Therefore, the sample may have been enriched for people who are more likely to be adherent.
Conclusion
We found that from the perspective of patients with multiple CHD risk factors attending specialty clinics, barriers and facilitators to medication adherence occur in the context of the patient, social/economic, therapy, and healthcare system/healthcare team. This underscores the need for multidimensional interventions aimed at improving medication adherence and overall health of patients with CHD and CHD risk factors. Such interventions may seek to: 1) promote social support for medication use and pharmacy utilization within participants’ social networks and 2) capitalize on and build supportive patient-provider relationships with the goal of enhancing continued education and explanation of medication benefits as well as side effects.
Acknowledgements
We thank Drs. Todd Brown and Fernando Ovalle for their assistance with patient recruitment, Ms. Cynthia Johnson and Ms. Julie Schach for their advice on effective patient recruitment, Ms. Lee Howard for her administrative assistance, and Dr. Whitney Rice for her mentoring during this project. This work was funded by American Heart Association Greater Southeast Affiliate Grant 16PRE29640015 (MONDESIR) and supplemental funding from the University of Alabama at Birmingham Department of Epidemiology (LEVITAN).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
E.B.L receives funding from Amgen for unrelated work, has served on Amgen advisory boards and as a consultant for a Novartis-sponsored research project, and reports person fees from Novartis, outside the submitted work. A.P.C receives funding from Amgen for unrelated work and reports grants from NIH/NINDS during the conduct of the study. M.M.S receives funding from Amgen for unrelated work. The authors report no other conflicts of interest in this work.
References
1. Benjamin EJ, Muntner P, Alonso A, et al. Heart disease and stroke statistics-2019 update: a report from the american heart association. Circulation. 2019;139:e56–e528.
2. Naderi SH, Bestwick JP, Wald DS. Adherence to drugs that prevent cardiovascular disease: meta-analysis on 376,162 patients. Am J Med. 2012;125:882–887. doi:10.1016/j.amjmed.2011.12.013
3. Wu JR, Moser DK, Lennie TA, Peden AR, Chen YC, Heo S. Factors influencing medication adherence in patients with heart failure. Heart Lung. 2008;37(8–16):16.
4. Pettersen TR, Fridlund B, Bendz B, et al. Challenges adhering to a medication regimen following first-time percutaneous coronary intervention: a patient perspective. Int J Nurs Stud. 2018;88:16–24. doi:10.1016/j.ijnurstu.2018.07.013
5. Johnson MJ, Williams M, Marshall ES. Adherent and nonadherent medication-taking in elderly hypertensive patients. Clin Nurs Res. 1999;8:318–335. doi:10.1177/10547739922158331
6. Ogedegbe G, Harrison M, Robbins L, Mancuso CA, Allegrante JP. Barriers and facilitators of medication adherence in hypertensive African Americans: a qualitative study. Ethn Dis. 2004;14:3–12.
7. Shiyanbola OO, Brown CM, Ward EC. “I did not want to take that medicine”: African-Americans’ reasons for diabetes medication nonadherence and perceived solutions for enhancing adherence. Patient Prefer Adherence. 2018;12:409. doi:10.2147/PPA.S152146
8. AlGhurair SA, Hughes CA, Simpson SH, Guirguis LM. A systematic review of patient self-reported barriers of adherence to antihypertensive medications using the world health organization multidimensional adherence model. J Clin Hypertens (Greenwich). 2012;14:877–886. doi:10.1111/j.1751-7176.2012.00699.x
9. Wu J-R, Moser DK, Chung ML, Lennie TA. Predictors of medication adherence using a multidimensional adherence model in patients with heart failure. J Card Fail. 2008;14:603–614. doi:10.1016/j.cardfail.2008.02.011
10. Dunbar-Jacob J, Bohachick P, Mortimer MK, Sereika SM, Foley SM. Medication adherence in persons with cardiovascular disease. J Cardiovasc Nurs. 2003;18:209–218. doi:10.1097/00005082-200307000-00006
11. Gellad WF, Grenard JL, Marcum ZA. A systematic review of barriers to medication adherence in the elderly: looking beyond cost and regimen complexity. Am J Geriatr Pharmacother. 2011;9:11–23. doi:10.1016/j.amjopharm.2011.02.004
12. Sung JC, Nichol MB, Venturini F, Bailey KL, McCombs JS, Cody M. Factors affecting patient compliance with antihyperlipidemic medications in an HMO population. Am J Manag Care. 1998;4:1421–1430.
13. Schweiger BB, Mathews DG. Religion in the American South: Protestants and Others in History and Culture. Univ of North Carolina Press; 2005.
14. Tongco MDC. Purposive Sampling as a Tool for Informant Selection. Manoa: University of Hawaii at Manoa; 2007.
15. Mack N, Woodsong C, MacQueen KM, Guest G, Namey E. Qualitative research methods: a data collectors field guide. Family Health Int. 2005.
16. Mondesir FL, Carson AP, Durant RW, Lewis MW, Safford MM, Levitan EB. Association of functional and structural social support with medication adherence among individuals treated for coronary heart disease risk factors: findings from the REasons for Geographic and Racial Differences in Stroke (REGARDS) study. PLoS One. 2018;13:e0198578. doi:10.1371/journal.pone.0198578
17. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. doi:10.1191/1478088706qp063oa
18. Gazmararian JA, Kripalani S, Miller MJ, Echt KV, Ren J, Rask K. Factors associated with medication refill adherence in cardiovascular-related diseases: a focus on health literacy. J Gen Intern Med. 2006;21:1215–1221. doi:10.1111/j.1525-1497.2006.00591.x
19. Odegard PS, Gray SL. Barriers to medication adherence in poorly controlled diabetes mellitus. Diabetes Educ. 2008;34:692–697. doi:10.1177/0145721708320558
20. Mondesir FL, Creger TN, Bress AP, et al. Association of distance to nearest pharmacy and pharmacy density with medication adherence among individuals treated for coronary heart disease risk factors.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.