Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Patient Participation in Multidisciplinary Tumor Conferences from the Providers’ Perspective: Is It Feasible in Routine Cancer Care?
Authors Heuser C ![]() , Diekmann A
, Diekmann A ![]() , Schellenberger B
, Schellenberger B ![]() , Bohmeier B, Kuhn W, Karbach U, Ernstmann N, Ansmann L
, Bohmeier B, Kuhn W, Karbach U, Ernstmann N, Ansmann L ![]()
Received 22 September 2020
Accepted for publication 16 November 2020
Published 27 November 2020 Volume 2020:13 Pages 1729—1739
DOI https://doi.org/10.2147/JMDH.S283166
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Christian Heuser,1 Annika Diekmann,1 Barbara Schellenberger,1 Barbara Bohmeier,1 Walther Kuhn,2 Ute Karbach,3 Nicole Ernstmann,1 Lena Ansmann4
1Center for Health Communication and Health Services Research (CHSR), Department for Psychosomatic Medicine and Psychotherapy, Center for Integrated Oncology (CIO Bonn), University Hospital Bonn, Bonn, Germany; 2Gynecological Cancer Center Deggendorf, DONAUISAR Hospital, Deggendorf, Germany; 3Sociology in Rehabilitation, Faculty of Rehabilitation Sciences, Technical University Dortmund, Dortmund, Germany; 4Division for Organizational Health Services Research, School of Medicine and Health Sciences, Carl von Ossietzky University Oldenburg, Oldenburg, Germany
Correspondence: Christian Heuser
University Hospital Bonn, Venusberg-Campus 1, Building 02, Bonn 53127, Germany
Tel +49 228 287 11545
Fax +49 228 287 9011545
Email [email protected]
Objective: Recent studies from Germany show that a small amount of breast and gynecological cancer patients participate in multidisciplinary tumor conferences (MTCs) at some cancer centers. One reason for the variation by center might be the providers’ attitudes about and experiences with MTC patient participation (MTCpp), which has not been analyzed before. Therefore, it is the aim of this study to analyze the providers’ expected or experienced feasibility concerning MTCpp at breast and gynecological cancer centers in Germany.
Methods: This paper presents cross-sectional qualitative interview data from the PINTU study. From April to December 2018, n=30 health-care providers from n=6 breast and gynecological cancer centers in North-Rhine-Westphalia, Germany, were interviewed. One-half of the providers had no experience and the other half had experience with MTCpp. Inductive and deductive coding was performed in order to capture the feasibility aspects of participation.
Results: MTCpp seems not to be feasible in routine cancer care following providers’ expected barriers and negative experiences. However, MTCpp seems to be feasible for selected cancer patients following providers’ expected opportunities and positive experiences. Our results show that both provider groups report positive and negative experiences or expectations.
Conclusion: The mixed findings regarding expected or experienced feasibility of MTCpp provide first insights into differences concerning MTCpp between organizations. Our results suggest that the providers’ perceptions (expectations and experiences) influence the possibility for patients to participate in an MTC in a cancer center.
Keywords: multidisciplinary tumor conference, multidisciplinary tumor board, multidisciplinary team meeting, patient participation, health-care provider, content analysis
Introduction
Multidisciplinary tumor conferences (MTCs) are a well-established structure for decision-making in oncological healthcare worldwide.1–3 Research done on MTCs has revealed benefits and limitations for providers and patients.4 Among providers, more effective coordination of healthcare and decision-making was found, which can be explained by a more efficient diagnostic discussion within a multidisciplinary team.5–9 From the providers’ perspective, making recommendations in MTCs is seen as part of physicians’ professional self-concept.10,11 Weekly meetings enable team-based decision-making and better communication between providers of different professions.12–14 Among patients, MTCs were shown to improve health-related quality of life,15,16 and a positive effect on patient’s overall survival has been suggested.17,18 Prior studies show that patients have a positive opinion of multidisciplinary teams.19 However, international studies have found that patients perceive a lack of communication about and representation in MTCs.20–22 Furthermore, a lack of patient information within MTCs, especially about their preferences, can decrease the adherence and effectiveness of MTC decisions significantly.23–26 This has led to the question how patient characteristics and preferences can be included in MTC decision-making.27,28 In this context, the question of patient participation in MTCs (MTCpp) has been discussed.
In Germany, different certification programs with their own requirement catalogues exist for breast and gynecological cancer centers: eg by the German Cancer Society (Germany-wide) and by the Medical Association of Westphalia-Lippe (for the state of North Rhine-Westphalia).29,30 In both requirement catalogues MTCs are mandatory for all certified cancer centers. MTCpp is allowed if patients wish to attend but this is only mentioned in the Medical Association Westphalia’s requirement catalog. Previous studies have shown that in Germany, participation is a rare but constant reality in healthcare, with 5–7% of breast cancer patients participating in MTCs, regardless of the certification program.31–33 The results of these studies also suggest that MTCpp varies by patient characteristics and between the breast cancer centers themselves.31,33 So far, no explanations for the variation between organizations as well as the feasibility of MTCpp from the providers’ perspective exist.
Few studies have explored the attitudes of providers toward MTCpp as well as its potential benefits and risks.34–38 Still, the question if and how MTCpp is feasible in routine cancer care remains unanswered. Analyzing the providers’ perspective is important since their expectations or experiences might influence the possibility for patients to participate in an MTC in a cancer center. To take providers’ expectations or experiences into account the conceptual framework for patient-provider communication in cancer care from Feldman-Stewart et al39 can be used. According to the model, providers’ expected or experienced external factors, their attitudes and goals, can be analyzed – in this case regarding the feasibility of MTCpp. External factors can be defined as organizational and system-level factors influencing the providers’ communication in MTCs through their impact on provider attitudes. Attitudes, including the providers’ needs, skills, values, beliefs and emotions affect the content and form of MTC communication. Providers’ goals are defined as the objective of the providers’ communication.
The aim of this study was to analyze the providers’ expected or experienced feasibility of patient participation in MTCs in breast and gynecological cancer centers in order to explain differences in MTCpp between organizations.
Materials and Methods
Study Design and Sample
The methods section is based on the consolidated criteria for reporting qualitative research, a 32-item checklist for interviews and focus groups.40 The presented data is part of the multicenter, non-interventional mixed-methods PINTU study conducted at six breast and gynecological cancer centers in Germany’s most populous state of North Rhine-Westphalia. PINTU stands for “patient involvement in multidisciplinary tumor conferences in breast cancer care – an exploratory study” and aimed to answer three main research questions: 1) How do MTC with and without patient participation differ in terms of organization, interaction and patient orientation? 2) How do patients experience participation and what are the immediate effects of participation? 3) How do health-care providers evaluate patient participation in MTC in terms of feasibility and quality of decision-making?41 The study has been approved by the Ethics Committee of the Medical Faculty of the University of Cologne. At three centers, patients regularly participate in MTCs, and at the other three centers, patients do not participate in MTCs. Cancer centers were selected using purposeful sampling criteria,42,43 varying the size of the center (case volume) and the teaching status (teaching hospital vs non-teaching hospital) because center structures can have an impact on the organization of MTCs.44
This paper presents data from qualitative interviews with health-care providers conducted as part of the larger PINTU study. The inclusion criterion for health-care providers was frequent participation in MTCs. With regard to the above-mentioned purposeful sampling, participants are to represent all professional (medical and non-medical) groups and different hierarchical levels involved in MTCs at breast and gynecological cancer centers. Providers with and without experiences with MTCpp were included in the sample in order to capture expected and experienced feasibility of MTCpp at the same time.
Data Collection
To capture these different perspectives, n=116 providers were invited by e-mail and telephone to participate in the study, and approximately five interviews were conducted at each of the six breast and gynecological cancer centers (n=30, see Table 1). Data were collected from April 2018 until December 2018 by four different researchers (CH, AD, BS, BB) experienced with qualitative research in their field of expertise (sociology, psychology, health services research). Written informed consent was obtained from all participants. The interviews took place at the breast and gynecological cancer centers or were conducted via telephone, they took between 24 and 81 minutes, and no other person was present besides the researcher and the participant. All interviews were recorded by means of an audio device for future transcription and analyses, according to established standards.45 Two interviews were not recorded due to lack of participant consent. Instead, memory protocols were obtained. In all cases, field notes were used as additional data. The interview guideline was adjusted after each interview if relevant new aspects were mentioned. When no new aspects emerged in the interviews, data collection was stopped.
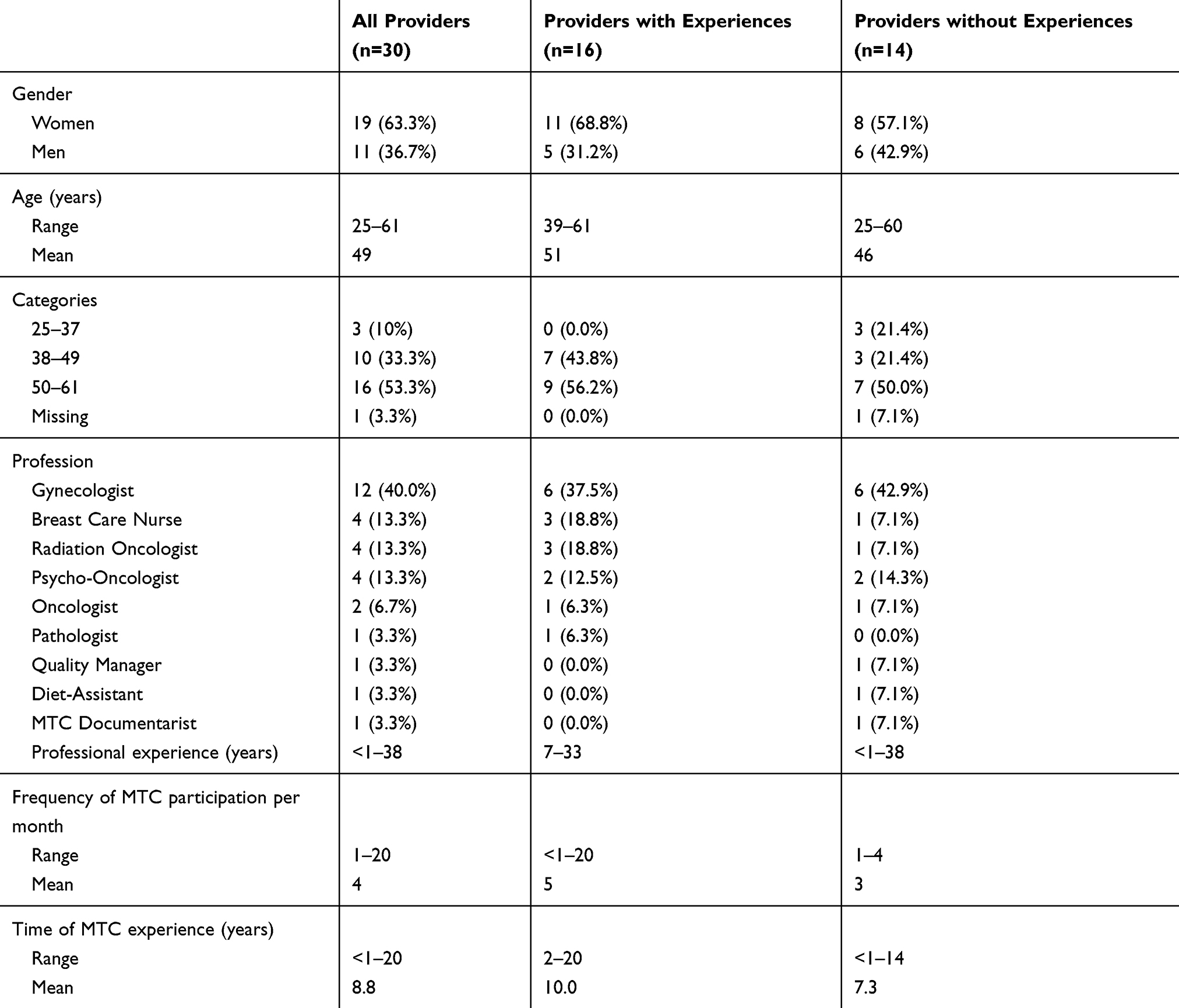 |
Table 1 Description of the Sample (n=30 Providers) |
Measures
Semi-structured interviews were conducted to capture the experiences, opinions and concerns of the providers participating in MTCs, especially concerning their external factors, attitudes and goals concerning MTCpp. In general, the interview guideline included the topics of MTC organization, interaction and decision-making. Furthermore, providers were asked for the differences they expected or experienced between MTCs with and without patient participation in order to capture expected and experienced feasibility of MTCpp at the same time. Further details of the interview guideline have been reported in the study protocol.41
Data Analysis
The audiotaped interviews were transcribed verbatim, pseudonymized, entered into the software program MAXQDA and analyzed by two independent researchers (CH, AD) from different disciplines (sociology, psychology) in accordance with the well-established methods of content analysis46,47 in order to increase inter-rater reliability. First, inductively identified codes were modified by deductively derived codes from previous international research on MTCpp.37,48–50 These codes were used as a coding system for the whole material. Next, categories were inductively developed throughout the material, modified by derived categories from the above-mentioned Feldman-Stewart conceptual framework and compiled by CH and AD. Last, the entire material was coded using the differentiated coding system. Subsequently, the analysis was interpreted and consented within the research team (CH, AD, BS, NE, LA) and the findings were discussed in a group consisting of 8 former interview participants with and without MTCpp experiences and the research team.
Results
Sample
The sample consisted of n=19 women and n=11 men from different professional disciplines (Table 1). One-half of the providers (n=16) had experience with MTCpp (see experienced feasibility), whereas the other half of the providers (n=14) had no experience (see expected feasibility). There was a wide range of ages (25–61 years) and work experience (<1–38 years).
Expected Feasibility of MTC Patient Participation
The coding of the n=14 provider interviews without experience in MTCpp revealed the following possible barriers: greater time requirements and organizational effort, interference with discussion and with the use of medical terminology, lack of own communication skills, lack of patient comprehension of clinical information, emotional reactions of patients and data protection issues. As potential benefits, these providers expected patients’ increased involvement in the MTC decision-making process, patients’ better understanding of their own clinical data and competitive advantages for the cancer center. There was a uniform opinion concerning possible barriers and benefits across all three cancer centers without MTCpp. No major differences between the medical and non-medical professions or hierarchical levels could be observed, even if Breast Care Nurses (BCN) were slightly more open for the idea of MTCpp.
Experienced Feasibility of MTC Patient Participation
The coding of the n=16 providers with experience in MTCpp revealed greater time requirements and organizational effort for some providers, interference with discussion and with the use of medical terminology, lack of patient comprehension as well as emotional reactions of patients during the MTC as negative experiences. Patients’ emotional reactions were often addressed directly after the MTC since many providers reported that a BCN or a familiar doctor accompanies patients before and after the MTC. The argument of increased time requirements and organizational effort was not relevant for all MTCpp experienced providers compared to non-experienced providers because only 1–2 patients participate per MTC weekly. The argument of interference with discussion varied among the providers since some reported not adjusting their use of medical terminology in the presence of patients. As positive experiences, providers reported a more effective decision-making process since the goal of the treatment can be defined immediately together with the patients. Furthermore, faster appointments with specialists, a more patient-oriented communication climate and more patient-centered decisions because patients’ preferences are included earlier in the treatment process were mentioned. To ensure the success of MTCpp, the providers suggested a small setting and the preselection of informed and interested patients. Overall, there were no major differences between the different professions’ opinions. Characteristic quotes of the providers with and without MTCpp experiences are presented in Table 2.
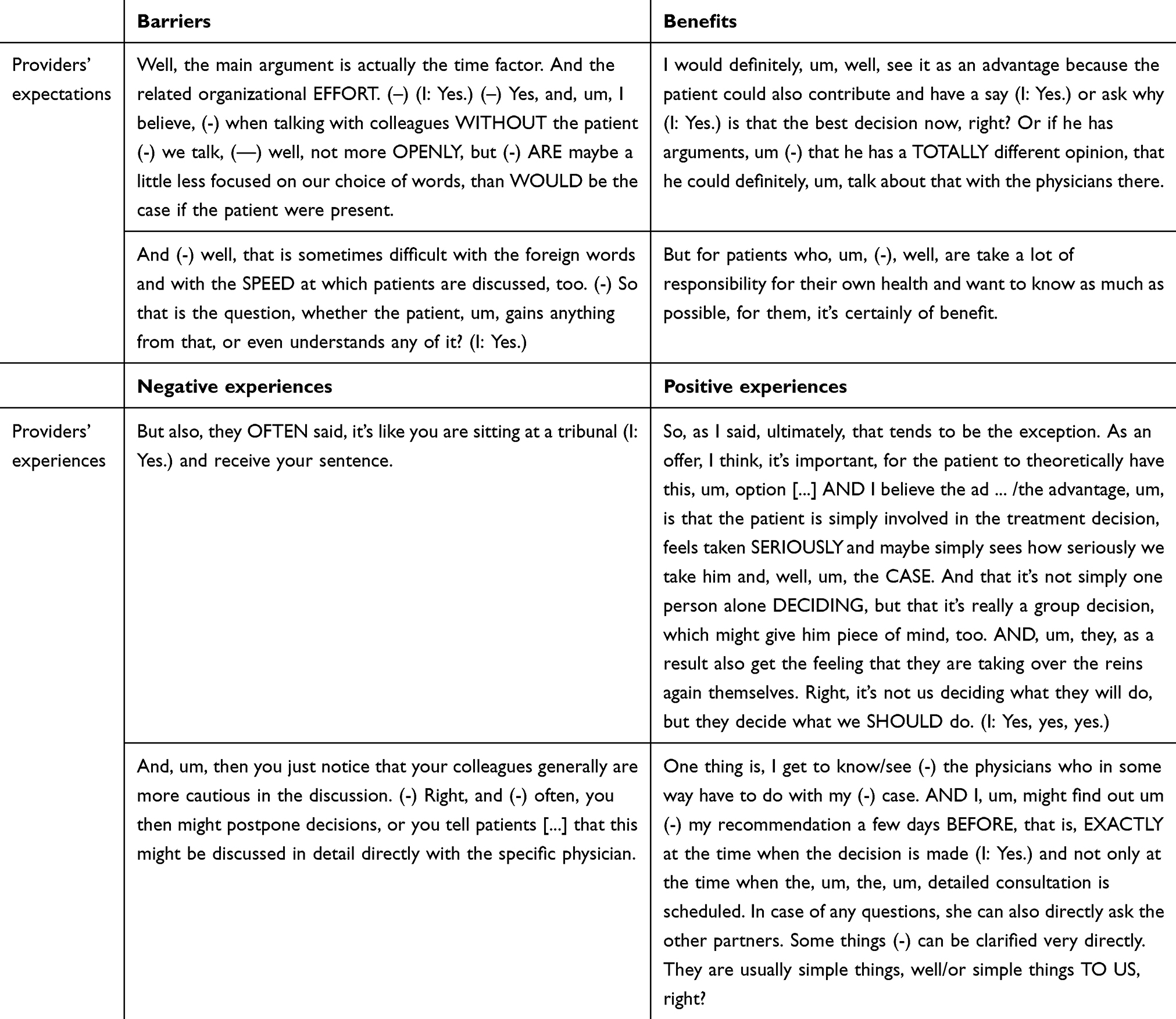 |
Table 2 Characteristic Quotes of the Providers |
External Factors of MTCpp
Providers with MTCpp experience reported that the requirement catalog for cancer center accreditation, center self-image, clinical guideline and awareness of patients and their related information are highly important for MTCpp. The different requirement catalogs for cancer center accreditation were often mentioned. With regard to patient participation, multidisciplinarity was regarded as helpful for patients since it allows discussing the diagnostic information in the presence of different professionals. Some providers mentioned that the chief physician was trained at a center where MTCpp was practiced and transferred this practice to the present center. Consequently, the self-image of the whole center is affected, and MTCpp is implemented at the center in question. The content of clinical guidelines was described as strongly guiding the MTC recommendation. Concerning patient participation, on the one hand, it was emphasized that the recommendation must be based on the clinical guideline, and patient preferences were not allowed to change the recommendation. As a result, MTCpp was not regarded as helpful. On the other hand, providers also described that they discussed the clinical-guideline-based recommendation with patients to arrive at a shared decision. Deviation of the final treatment decision from the clinical-guideline-based MTC recommendation was regarded as highly important by some providers since those deviations are often based on patient preferences. In this context, the criterion of providers' awareness of patient personality and patient-related information becomes important because all of the providers believe that patients and their preferences must be known and diagnostics must be completed before the MTC. These aspects can be summarized as external factors as they possibly affect providers' attitudes concerning MTCpp.
Attitudes Concerning MTCpp Including Needs, Skills, Values, Beliefs and Emotions
Across all interviews, the providers’ central need was to find the best recommendation (“need for truth”). For the providers, the best recommendation should be found on the basis of objectivity, facts and clinical guidelines through a multidisciplinary discussion. Patient or provider emotions should not play any role in the recommendation process. Providers’ MTCpp-related skills largely involve aspects of communication and organization. Concerning communication, some providers reported that the patients’ presence and the switch to lay language interfered with the discussion. Adequately discussing medical information in the multidisciplinary team but at the same time keeping it understandable for patients is perceived as a challenge. In this context, MTC organization becomes relevant because in some centers, patients enter the MTC after the medical discussion between providers. In this setting, providers did not report conflicts between expert and lay language and discussion. Furthermore, in the view of many providers, patients must be accompanied before, during and after the MTC, for example, by a breast care nurse. Some providers implemented an additional MTCpp setting with fewer providers present. Others described a “natural” preselection of patients since only 5˗10% of patients were willing to participate. The providers’ values concerning MTCpp may be shaped by the above-mentioned external factor of “center self-image.” Two types of values can be differentiated, of which the first one was mentioned by every provider and the second one seen as an add-on. Firstly, MTCs are a professional instrument to make treatment decisions (medical logic). Secondly, MTCs are an instrument for considering patient information, preferences and emotions and involving patients in the decision-making process (social logic). MTC-related beliefs are reflected by the providers’ understanding of patient-provider roles in the MTC. Making treatment recommendations was seen as part of the physician’s expertise; thus, patients might experience MTCs as a tribunal and therefore should not enter this “field of expertise.” Other providers believe that patients should be allowed to enter this “field of expertise” because of transparency reasons and in order to better understand the treatment decision. Furthermore, patient involvement in decision-making was generally regarded as positive, but since this involvement is not ensured by patient participation for some providers, MTCpp was not supported. Several providers mentioned that the patient’s sociodemographic background has an immense impact on the quality and efficiency of the MTC discussion, thereby making participation more or less helpful for different patients. Providers’ emotions were hardly addressed in the interviews. Very few situations of uncertainty were mentioned, in which medical information had to be explained to the patient in lay language in front of all colleagues, although providers wanted to be seen as professional.
Goals Concerning MTCpp
Across all interviews, the main goal was to discuss and establish the best recommendation in accordance with clinical guidelines in a multidisciplinary manner. With regard to MTCpp, potential goal conflicts can be described. MTCs without patients are an important instrument to establish the guideline-based recommendation as the “best decision” in the view of the medical specialists and can be seen as a tool for advanced education in teaching hospitals. Some providers experienced MTCs with patient participation to have a different character: MTCs with patients are seen as a place to ask for information that is not always important for decision-making or treatment. Other providers reported that patient participation leads to decisions that are more congruent with the patients’ goals because the jointly defined treatment goal incorporates patient preferences. In the first case, MTCpp was regarded as possibly conflicting with the providers’ goal, and in the second case, as supporting the providers’ goal.
Discussion
The aim of the study was to analyze the providers’ expected or experienced feasibility of patient participation in MTCs at breast and gynecological cancer centers in order to explain why MTCpp differs between cancer centers. Inductive coding revealed feasibility aspects in the form of opportunities and barriers expressed by providers without MTCpp experience as well as positive and negative experiences from providers experienced with MTCpp. Deductive coding added important themes of the feasibility of MTCpp. These findings suggest that providers’ experienced external factors, attitudes and goals can hinder or foster MTCpp. In the following sections, specific aspects of these results are discussed in detail.
Feasibility of MTC Patient Participation
MTCpp seems not to be feasible in routine cancer care following the providers’ anticipated barriers and negative experiences. However, MTCpp seems to be feasible for selected cancer patients following the providers’ perceived opportunities and positive experiences. Our results confirm previous findings from international research concerning providers’ views on MTCpp.34–37,51 Butow et al 2007 reported providers mentioning potential patient anxiety during and after the MTC as well as a conflict between medical and lay language.35 We can expand Butow’s findings concerning the management of patient involvement by describing variations of MTCpp: Patients may enter the MTC after the medical discussion, a smaller MTC setting may be implemented, and patients may be supported by a breast care nurse before, during and after the meeting. Support by a breast care nurse seemed to be an important aspect that was also described by O´Brien et al51 Whereas providers and patients shared some views of a good MTCpp, physicians “may underestimate the importance [for patients] of feeling comfortable” during the MTC. Our findings from providers experienced with MTCpp show that significant changes in organization and setting are made if patients take part during the discussion of their own case. Furthermore, communication skills to address patients’ emotional reactions were seen as highly important by providers experienced with MTCpp which we analyzed more detailed in a different publication on MTCpp.52 Van Dongen et al and Choy et al recommend adequate support and preparation for the meeting, eg paying attention to patients’ willingness and ability to participate, which were also mentioned by providers in this present study. In addition, it seems important for all necessary information to be shared with patients before the MTC.34,37 The main remaining barrier is increased time requirements, which might be surprising since in Germany, only 5–10% of patients actually participate in an MTC. Concerning decision-making, no hard facts can be presented with this data, but providers reported that MTCpp leads to earlier consideration of patient preferences in the treatment process, potentially leading to more patient-oriented treatment decisions.
Differences in MTC Patient Participation Between Organizations
Furthermore, our results expand the findings from previous international research concerning the reasons for differences in MTCpp between cancer centers. Previous German studies have shown significant differences in the frequency of MTCpp between breast cancer centers31,33 but could not explain them. We were able to explain potential reasons for these differences by studying the providers’ experienced external factors, attitudes and goals concerning the feasibility of MTCpp. Importantly, the main MTC goal of defining the best recommendation remains unchanged in MTCs with patients but in a slightly different manner: On the one hand, a medical recommendation must be made and MTCs without patients being perceived as a medical recommendation-issuing committee free from interference by patients’ emotions, wishes or questions. On the other hand, the decision-making process with patients’ personal and social aspects has to be discussed and MTCs with patient participation are regarded as medical recommendation-issuing committees that need to address patients’ emotions, wishes, preferences, questions and social characteristics. These conflicts might be reflected by differences in the possibility for patients to participate in an MTC. These results suggest that providers’ expectations and experiences with MTCpp feasibility explain why patient participation in MTCs differs between organizations (cancer centers). Nevertheless, it has to be discussed why on the one hand no major differences between the professions’ perceptions in all six cancer centers exist, but on the other hand differences in MTCpp between these centers exist. One hypothesis is that MTCpp is more frequently in non-university hospitals and centers with a lower case volume. As sampling intended to take this variation into account there must be further explanations, eg the degree of patient-centeredness22 in the center.
Limitations and Strengths
Our sample consists exclusively of providers from breast and gynecological cancer centers. Therefore, the providers’ experiences are based only on MTC communication with women as none of the providers remembered a male breast cancer patient participating in an MTC. Our conclusions consider this important limitation. In general, breast and gynecological cancers are solid tumors, which means that our sample does not include non-solid tumors, eg those of hematological cancer patients, and providers have no experience with non-solid cancer patients. Furthermore, feasibility aspects are based on subjective experiences from providers who might have participated in the interviews because they were more supportive of MTCpp. However, with data from 30 interviews, we have obtained a wide range of detailed expectations and experiences. Nevertheless, we have no comprehensive picture of MTCs in general since observations are not matched to interview data and no patient data or patient interview data concerning their experiences in MTCs has been analyzed. No patient interview data, eg concerning their reasons for and experiences with MTCpp were included in this study. Patient interview data are also not a part of the PINTU study and a limitation of the project. Instead, patient survey data on their experiences with MTCpp is analyzed in a different study of the PINTU project. Lastly, the study used an observational design as a first step to analyze existing MTC processes, but future research would benefit from interventional study designs.
However, this is one of the first studies analyzing providers’ experiences and their external factors, attitudes and goals concerning MTCpp and if MTCpp is feasible in routine cancer care. The interviews are not biased by hierarchies or other professional groups, which is a common problem while conducting focus groups with providers. The presented results are the first explanation of differences in MTCpp between cancer centers. This is an important step for getting deeper insights into determinants of MTCpp evolving from providers’ perceptions. Lastly, this is the first use and adaption of the well-established Feldman-Stewart framework of communication in cancer care for MTC and MTCpp.
Implications
The findings can help explain differences concerning MTCpp between German breast and gynecological cancer centers as external factors, attitudes and goals of providers take important feasibility aspects into account. However, we only analyzed the providers’ characteristics within the framework. Thus, future research should firstly address patients’ external factors, attitudes and goals influencing their MTC communication with providers with the help of patient interview data, eg concerning their reasons for and experiences with MTCpp. Secondly, the feasibility analyzed for providers at breast and gynecological cancer centers should be transferred to other cancer entities, eg non-solid tumors or cancer entities that affect mainly men. Thirdly, for research on MTCs, a time dimension could be added to the framework in order to analyze communication processes before, during and after the MTC or other healthcare processes in general. Lastly, our analysis revealed an important difference between the guideline-based recommendation that must be established during MTCs and decision-making with patients during or after MTC. For future research, we strongly recommend defining and differentiating the unit of analysis by breaking it down into the recommendation or decision. This might explain divergent results concerning the need for MTCpp: While Massoubre et al36 found that 97% of MTC recommendations without patient participation were followed and concluded that MTCpp is not essential, Hollunder et al found a great lack of MTC decision adherence caused by missing patient information and failure to consider their preferences23 which might increase the need for MTCpp, even in the case of limited clinical evidence53 or limited multidisciplinary discussion.54,55 For future research, this should firstly mean that patient outcomes have to be analyzed as they are an important part of general MTC outcome quality.49,50,56–59 Some patient outcomes will be analyzed in the quantitative part of the PINTU study. Secondly, this underlines the need for a patient-centered approach in oncological healthcare taking into account patients’ preferences regardless of whether patients participate in MTC or not. As shared-decision-making in MTCs seems to be challenging60 different ways of involving patient preferences in MTCs have to be discussed in the future.
Conclusions
This study has contributed to filling the research gap on providers’ experiences of and expectations for the feasibility of MTCpp. The providers’ perceptions of feasibility are one influencing factor for MTCpp and therefore provide first insights into differences concerning MTCpp between cancer centers. Overall, future research and practice should focus on processes in MTCs, eg by considering differences in communication between MTCs with and without patient participation and their impact on the quality of decision-making and on patient outcomes (eg anxiety, quality of life) and patient-reported experiences (eg experienced patient-centered care). These questions must be answered before any specific recommendations for patients, providers and cancer centers concerning MTCs can be developed.
Data Sharing Statement
Data and all other materials for this study are kept at the Center for Health Communication and Health Services Research, University of Bonn, University Hospital Bonn, Germany. The datasets generated and analyzed during the current study are not publicly available due to terms of written informed consent to which the participants agreed but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the ethics committee of the Medical Faculty of the University of Cologne, Germany. Written informed consent was obtained from all individual participants included in the study.
Trial Registration
German Clinical Trials Register (DRKS), DRKS00012552, registered prospectively on 16.06.2017, https://www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00012552.
Acknowledgments
We would like to thank all of the providers and all breast and gynecological cancer centers for participating in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by The German Cancer Aid (Grant number: 70112286).
Disclosure
Prof. Dr. Lena Ansmann report grants from German Cancer Aid, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Fleissig A, Jenkins V, Catt S, Fallowfield L. Multidisciplinary teams in cancer care: are they effective in the UK? Lancet Oncol. 2006;7(11):935–943. doi:10.1016/S1470-2045(06)70940-8
2. Saini KS, Taylor C, Ramirez A-J, et al. Role of the multidisciplinary team in breast cancer management: results from a large international survey involving 39 countries. Ann Oncol. 2012;23(4):853–859. doi:10.1093/annonc/mdr352
3. Taylor C, Munro AJ, Glynne-Jones R, et al. Multidisciplinary team working in cancer: what is the evidence? BMJ. 2010;340(mar23 2):c951. doi:10.1136/bmj.c951
4. Soukup T, Lamb BW, Arora S, Darzi A, Sevdalis N, Green JS. Successful strategies in implementing a multidisciplinary team working in the care of patients with cancer: an overview and synthesis of the available literature. J Multidiscip Healthc. 2018;11:49–61. doi:10.2147/JMDH.S117945
5. Raine R, Wallace I, Nic A’ Bhaird C, et al. Improving the effectiveness of multidisciplinary team meetings for patients with chronic diseases: a prospective observational study. Health Ser Deliv Res. 2014;37(2). doi:10.3310/hsdr02370
6. National Cancer Action Team. The Characteristics of an Effective Multidisciplinary Team (MDT). London; 2010.
7. Chang JH, Vines E, Bertsch H, et al. The impact of a multidisciplinary breast cancer center on recommendations for patient management. Cancer. 2001;91(7):1231–1237. doi:10.1002/1097-0142(20010401)91:7<1231:AID-CNCR1123>3.0.CO;2-K
8. Cianfrocca ME, Shelby M, Birdi S, et al. A multidisciplinary team approach to efficient breast cancer diagnosis. JCO. 2016;34(7_suppl):88. doi:10.1200/jco.2016.34.7_suppl.88
9. Rosell L, Wihl J, Nilbert M, Malmström M. Health professionals’ views on key enabling factors and barriers of national multidisciplinary team meetings in cancer care: a qualitative study. J Multidiscip Healthc. 2020;13:179–186. doi:10.2147/JMDH.S240140
10. Salloch S, Ritter P, Wascher S, Vollmann J, Schildmann J. Medical expertise and patient involvement: a multiperspective qualitative observation study of the patient’s role in oncological decision making. Oncologist. 2014;19(6):654–660. doi:10.1634/theoncologist.2013-0268
11. National Cancer Action Team. Multidisciplinary Team Members’ Views About MDT Working: Results from a Survey Commissioned by the National Cancer Action Team. London; 2009.
12. Harrison JD, Choy ET, Spillane A, Butow P, Young JM, Evans A. Australian breast cancer specialists’ involvement in multidisciplinary treatment planning meetings. Breast. 2008;17(4):335–340. doi:10.1016/j.breast.2008.03.001
13. Macaskill EJ, Thrush S, Walker EM, Dixon JM. Surgeons’ views on multi-disciplinary breast meetings. Eur J Cancer. 2006;42(7):905–908. doi:10.1016/j.ejca.2005.12.014
14. Devitt B, Philip J, McLachlan S-A. Team dynamics, decision making, and attitudes toward multidisciplinary cancer meetings: health professionals’ perspectives. J Oncol Pract. 2010;6(6):e17–20. doi:10.1200/JOP.2010.000023
15. Croke JM, El-Sayed S. Multidisciplinary management of cancer patients: chasing a shadow or real value? An overview of the literature. Curr Oncol. 2012;19(4):232–238. doi:10.3747/co.19.944
16. Street RL, Elwyn G, Epstein RM. Patient preferences and healthcare outcomes: an ecological perspective. Expert Rev Pharmacoecon Outcomes Res. 2012;12(2):167–180. doi:10.1586/erp.12.3
17. Hong NJL, Wright FC, Gagliardi AR, Paszat LF. Examining the potential relationship between multidisciplinary cancer care and patient survival: an international literature review. J Surg Oncol. 2010;102(2):125–134. doi:10.1002/jso.21589
18. Kesson EM, Allardice GM, George WD, Burns HJG, Morrison DS. Effects of multidisciplinary team working on breast cancer survival: retrospective, comparative, interventional cohort study of 13 722 women. BMJ. 2012;344(apr26 1):e2718. doi:10.1136/bmj.e2718
19. Lamb BW, Jalil RT, Shah S, et al. Cancer patients’ perspectives on multidisciplinary team working: an exploratory focus group study. Urol Nurs. 2014;34(2):83–91. doi:10.7257/1053-816X.2014.34.2.83
20. Taylor C, Finnegan-John J, Green JSA. “No decision about me without me” in the context of cancer multidisciplinary team meetings: a qualitative interview study. BMC Health Serv Res. 2014;14:488. doi:10.1186/s12913-014-0488-2
21. Hamilton DW, Heaven B, Thomson RG, Wilson JA, Exley C. Multidisciplinary team decision-making in cancer and the absent patient: a qualitative study. BMJ Open. 2016;6(7):e012559. doi:10.1136/bmjopen-2016-012559
22. Hahlweg P, Hoffmann J, Harter M, Frosch DL, Elwyn G, Scholl I. In absentia: an exploratory study of how patients are considered in multidisciplinary cancer team meetings. PLoS One. 2015;10(10):e0139921. doi:10.1371/journal.pone.0139921
23. Hollunder S, Herrlinger U, Zipfel M, et al. Cross-sectional increase of adherence to multidisciplinary tumor board decisions. BMC Cancer. 2018;18(1):936. doi:10.1186/s12885-018-4841-4
24. Rajan S, Foreman J, Wallis MG, Caldas C, Britton P. Multidisciplinary decisions in breast cancer: does the patient receive what the team has recommended? Br J Cancer. 2013;108(12):2442–2447. doi:10.1038/bjc.2013.267
25. Morement H, Harrison R, Taylor-Robinson SD. The multidisciplinary team meeting in the UK from the patients’ perspective: comments and observations from cholangiocarcinoma patients and their families. Int J Gen Med. 2017;10:305–310. doi:10.2147/IJGM.S145029
26. Hoinville L, Taylor C, Zasada M, Warner R, Pottle E, Green J. Improving the effectiveness of cancer multidisciplinary team meetings: analysis of a national survey of MDT members’ opinions about streamlining patient discussions. BMJ Open Qual. 2019;8(2):e000631. doi:10.1136/bmjoq-2019-000631
27. Lamb BW, Taylor C, Lamb JN, et al. Facilitators and barriers to teamworking and patient centeredness in multidisciplinary cancer teams: findings of a national study. Ann Surg Oncol. 2013;20(5):1408–1416. doi:10.1245/s10434-012-2676-9
28. Bate J, Wingrove J, Donkin A, Taylor R, Whelan J. Patient perspectives on a national multidisciplinary team meeting for a rare cancer. Eur J Cancer Care (Engl). 2019;28(2):e12971. doi:10.1111/ecc.12971
29. German Cancer Aid. Interdisciplinary S3-Guideline for Diagnostic, Therapy, and Rehabilitation of Breast Cancer: [Interdisziplinäre S3-Leitlinie Für Die Diagnostik, Therapie Und Nachsorge Des Mammakarzinoms]. 2012.
30. Ärztekammer W-L. Certification of breast cancer centers in North-Rhine Westphalia. Requirement catalogue breast cancer centers: [Verfahren zur Zertifizierung von Brustzentren in NRW. Anforderungskatalog-Brustzentren]. 2018.
31. Heuser C, Diekmann A, Kowalski C, et al. Health literacy and patient participation in multidisciplinary tumor conferences in breast cancer care: a multilevel modeling approach. BMC Cancer. 2019;19(1):330. doi:10.1186/s12885-019-5546-z
32. Diekmann A, Heuser C, Ernstmann N, et al. How do breast cancer patients experience multidisciplinary tumor conferences? - a description from the patient perspective. Breast. 2019;44:66–72. doi:10.1016/j.breast.2018.12.012
33. Ansmann L, Kowalski C, Pfaff H, Wuerstlein R, Wirtz MA, Ernstmann N. Patient participation in multidisciplinary tumor conferences. Breast. 2014;23(6):865–869. doi:10.1016/j.breast.2014.09.004
34. Choy ET, Chiu A, Butow P, Young J, Spillane A. A pilot study to evaluate the impact of involving breast cancer patients in the multidisciplinary discussion of their disease and treatment plan. Breast. 2007;16(2):178–189. doi:10.1016/j.breast.2006.10.002
35. Butow P, Harrison JD, Choy ET, Young JM, Spillane A, Evans A. Health professional and consumer views on involving breast cancer patients in the multidisciplinary discussion of their disease and treatment plan. Cancer. 2007;110(9):1937–1944. doi:10.1002/cncr.23007
36. Massoubre J, Lapeyre M, Pastourel R, et al. Will the presence of the patient at multidisciplinary meetings influence the decision in head and neck oncology management? Acta Otolaryngol. 2018;138(2):185–189. doi:10.1080/00016489.2017.1384059
37. van Dongen JJJ, Habets IGJ, Beurskens A, van Bokhoven MA. Successful participation of patients in interprofessional team meetings: a qualitative study. Health Expect. 2017;20(4):724–733. doi:10.1111/hex.12511
38. van Dongen JJJ, de Wit M, Smeets HWH, Stoffers E, van Bokhoven MA, Daniëls R. “They are talking about me, but not with me”: a focus group study to explore the patient perspective on interprofessional team meetings in primary care. Patient. 2017;10(4):429–438. doi:10.1007/s40271-017-0214-3
39. Feldman-Stewart D, Brundage MD, Tishelman C. A conceptual framework for patient-professional communication: an application to the cancer context. Psychooncology. 2005;14(10):801–809. doi:10.1002/pon.950
40. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
41. Heuser C, Diekmann A, Ernstmann N, Ansmann L. Patient participation in multidisciplinary tumour conferences in breast cancer care (PINTU): a mixed-methods study protocol. BMJ Open. 2019;9(4):e024621. doi:10.1136/bmjopen-2018-024621
42. Patton MQ. Enhancing the quality and credibility of qualitative analysis. Health Serv Res. 1999;34(5 Pt 2):1189–1208.
43. Palinkas LA, Aarons GA, Horwitz S, Chamberlain P, Hurlburt M, Landsverk J. Mixed method designs in implementation research. Adm Policy Ment Health. 2011;38(1):44–53. doi:10.1007/s10488-010-0314-z
44. Radecki SE, Nyquist JG, Gates JD, Abrahamson S, Henson DE. Educational characteristics of tumor conferences in teaching and non‐teaching hospitals. J Cancer Educ. 2009;9(4):204–216.
45. Flick U, Kvale S, Angrosino MV, et al. eds. The Sage Qualitative Research Kit. London: SAGE; 2007.
46. Kuckartz U. Qualitative Inhaltsanalyse: Methoden, Praxis, Computerunterstützung.
47. Kuckarzt U. Analyzing Qualitative Data with MAXQDA: Text, Audio, and Video. [Place of Publication Not Identified]. SPRINGER; 2019.
48. Soukup T, Lamb BW, Sarkar S, et al. Predictors of treatment decisions in multidisciplinary oncology meetings: a quantitative observational study. Ann Surg Oncol. 2016;23(13):4410–4417. doi:10.1245/s10434-016-5347-4
49. Taylor C, Atkins L, Richardson A, Tarrant R, Ramirez A-J. Measuring the quality of MDT working: an observational approach. BMC Cancer. 2012;12(1):202. doi:10.1186/1471-2407-12-202
50. Hahlweg P, Didi S, Kriston L, Härter M, Nestoriuc Y, Scholl I. Process quality of decision-making in multidisciplinary cancer team meetings: a structured observational study. BMC Cancer. 2017;17(1):772. doi:10.1186/s12885-017-3768-5
51. O’Brien MA, Ellis PM, Whelan TJ, et al. Physician-related facilitators and barriers to patient involvement in treatment decision making in early stage breast cancer: perspectives of physicians and patients. Health Expect. 2013;16(4):373–384. doi:10.1111/j.1369-7625.2011.00712.x
52. Diekmann A, Heuser C, Schellenberger B, et al. Patient participation in multidisciplinary tumor conferences: providers’ perceptions of patients’ need satisfaction and emotional experiences. Psychooncology. 2020;29(8):1263–1271. doi:10.1002/pon.5413
53. Lassalle R, Marold J, Schöbel M, et al. Entscheidungsprozesse im Tumorboard bei eingeschränkter Evidenzlage. Laryngorhinootologie. [Decision process in a multidisciplinary cancer team with limited evidence]. 2014;93(4):237–243. doi:10.1055/s-0033-1353199
54. Soukup T, Murtagh G, Lamb BW, Green J, Sevdalis N. How Multidisciplinary are Multidisciplinary Case Reviews in Cancer Care? Analysis of Team Decision-Making Fidelity. 2019.
55. Horlait M, Baes S, Dhaene S, van Belle S, Leys M. How multidisciplinary are multidisciplinary team meetings in cancer care? An observational study in oncology departments in Flanders, Belgium. J Multidiscip Healthc. 2019;12:159–167. doi:10.2147/jmdh.s196660
56. Offermanns G, Koldžić E, Schweiger A. Qualitätsentwicklung in der onkologischen Versorgung durch multiprofessionelle Teamarbeit am Beispiel von Tumorboards: ein Überblick. Public Health Forum. 2019;27(3):205–207. doi:10.1515/pubhef-2019-0050
57. Lamb BW, Brown KF, Nagpal K, Vincent C, Green JSA, Sevdalis N. Quality of care management decisions by multidisciplinary cancer teams: a systematic review. Ann Surg Oncol. 2011;18(8):2116–2125. doi:10.1245/s10434-011-1675-6
58. Evans L, Donovan B, Liu Y, Shaw T, Harnett P. A tool to improve the performance of multidisciplinary teams in cancer care. BMJ Open Qual. 2019;8(2):e000435. doi:10.1136/bmjoq-2018-000435
59. Houssami N, Sainsbury R. Breast cancer: multidisciplinary care and clinical outcomes. Eur J Cancer. 2006;42(15):2480–2491. doi:10.1016/j.ejca.2006.05.023
60. Bohmeier B, Schellenberger B, Diekmann A, Ernstmann N, Ansmann L, Heuser C. Opportunities and limitations of shared decision making in multidisciplinary tumor conferences with patient participation - a qualitative interview study with providers. Patient Educ Couns. 2020. doi:10.1016/j.pec.2020.09.007
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.