Back to Journals » Clinical Interventions in Aging » Volume 18
Patient Outcomes Associated with the First Remote Monitoring Experience of Cardiac Implantable Electronic Devices in South Korea
Received 23 May 2023
Accepted for publication 5 September 2023
Published 22 September 2023 Volume 2023:18 Pages 1587—1595
DOI https://doi.org/10.2147/CIA.S422626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
YouMi Hwang,1,2 Hannah Bae3
1Department of Cardiology, St. Vincent’s Hospital, the Catholic University of Korea, Suwon, Republic of Korea; 2Catholic Research Institute for Intractable Cardiovascular Disease (CRID), College of Medicine, the Catholic University of Korea, Seoul, Republic of Korea; 3Department of Economics, University of California - San Diego, La Jolla, CA, USA
Correspondence: YouMi Hwang, Department of Cardiology, St. Vincent’s Hospital, the Catholic University of Korea, Suwon, 16247, Republic of Korea, Tel +82-31-249-7548, Fax +82-31-253-8898, Email [email protected]
Purpose: Remote monitoring of cardiac devices reduces unnecessary outpatient visits and increases patient satisfaction. We aimed to evaluate remote monitoring in terms of patient satisfaction, economic efficiency, and safety.
Patients and Methods: This was a single university hospital survey. The time/medical cost efficacy and satisfaction index were evaluated using a questionnaire to investigate patient satisfaction before and after remote monitoring in patients using Biotronik implantable cardiac devices. The questionnaire was adopted and modified from Hwang’s 2020 Survey on Telehealth Patient Experience.
Results: Remote monitoring was associated with a decrease in total outpatient visits. Of 1270 remote monitoring-related alerts clinicians received during the study period, more than 95% were from patients with pacemakers. Still, the severity of alerts was higher for implantable cardioverter defibrillators and cardiac resynchronization therapy with defibrillators. The post-RM survey results demonstrated that patients were generally satisfied with RM, perceived it as cost-effective, and found that RM facilitated health management without disrupting their daily routines.
Conclusion: The study participants were satisfied with their first remote monitoring experience and reported having time- and cost-savings by using remote monitoring. Remote monitoring-related alerts from high-voltage devices were more severe and required medical intervention.
Keywords: pacemaker, artificial, cardiac resynchronization therapy devices, defibrillators
Graphical Abstract:

Introduction
Telehealth has become a concept that is familiar to laypersons as monitoring of vital signs, such as smartwatches and smartphones, has been established.1–6 As wearable devices have increased in popularity after the coronavirus disease 2019 pandemic, the demand for telehealth has also increased. Remote monitoring is a type of telehealth, and its effectiveness, efficiency, and safety have already been verified.7–12 Although remote monitoring of cardiac devices had been adopted for over a decade in other countries due to its effectiveness and safety, the introduction of remote monitoring was delayed. This delay was attributed to conflicting expert opinions from various fields about its introduction and the unique domestic medical insurance system in the country. In light of this situation, this study was conducted to gather empirical data for evaluating the safety and effectiveness of remote monitoring among patients with cardiac implantable electronic devices and to explore the potential consequences of RM adoption within the National Health Insurance system framework.
Materials and Methods
Study Design and Population
Remote-Care was a prospective study conducted at a single university hospital. Its primary objective was to assess the effectiveness and safety of remote monitoring for cardiac implantable electronic devices. The study also aimed to gather patient experiences regarding remote monitoring through surveys that were designed to reflect the medical context in Korea. Figure 1 provides an overview of the study process. The study participants comprised patients using Biotronik (Berlin, Germany) cardiac implantable electronic devices (pacemakers, implantable cardioverter defibrillators, and cardiac resynchronization therapy with defibrillators) compatible with the Biotronik Home Monitoring system. To compare conventional in-office visits before and after remote monitoring implementation, the study was comprised of patients who had undergone outpatient treatment with a cardiac implantable electronic device implanted for at least 6 months before they enrolled in the study. The study participants were followed up for 12 (±1) months for their remote monitoring use, in-person visits, and related out-of-pocket costs.
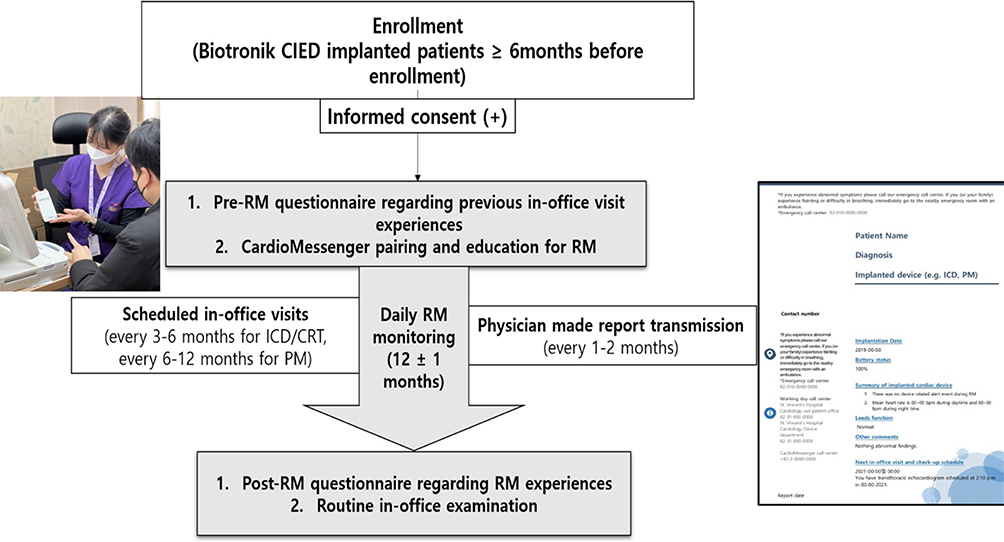 |
Figure 1 Study flowchart, in-office instructions for cardiomessenger and remote device monitoring, and embedded patient report form during follow-up period. |
This study was approved by the Catholic University of Korea, St. Vincent’s Hospital Institutional Review Board (Suwon, South Korea; Institutional Review Board No. VC20DISF0160). The Remote-Care study was registered at ClinicalTrials.gov with the study ID NCT04557111. This study was conducted following the Declaration of Helsinki and supported by Biotronik.
Data Collection
After obtaining informed consent, participants were requested to complete a questionnaire13 regarding their prior experience with conventional in-office visits before using remote monitoring. After completing the pre-remote monitoring questionnaire, patients (±caregivers) received a mobile CardioMessenger Smart device, which was immediately paired with their cardiac implantable electronic devices, along with instructions for CardioMessenger Smart and remote monitoring use.
During the 12 months of remote monitoring, the primary investigator (YMH) reviewed the remote monitoring alerts and sent summary reports to each patient about their cardiac implantable electronic device status every other month, according to the patient’s preferred means (mail, e-mail, or Multimedia Messaging Service). Following the 12-month post-period, patients were invited to provide feedback on their experience with remote patient monitoring. This was done by completing an adapted Korean version of the Home Monitoring Acceptance and Satisfaction Questionnaire developed by Hwang (2020) (Supplementary Table 1).
We collected data from electronic medical records (EMR) about medical histories and the frequency of outpatient visits. Routine follow-up visits were scheduled at 6–12 months for patients with pacemakers and 3–6 months for patients with implantable cardioverter defibrillators, except in patients on warfarin or those with other relevant medical issues. Any unexpected visits or admission during the study period were classified as (a) device-management visits due to CardioMessenger Smart device pairing problems, (b) participants’ cardiovascular condition-related, and non-cardiovascular condition-related visits. We categorized non-routine visits into three groups: a) patient-initiated visits (medication-related consult or consultation from other departments for preoperative evaluation/mode change before imaging or elective operation) and b) physician-initiated visits (physician requested hospital visits based on RM finding or alerts; CM connection error related hospital visit request for a checkup for device pairing).
The primary endpoint was patient satisfaction after remote monitoring. The secondary endpoints included comparing time and qualitative evaluations, including medical costs between contact medical care and remote monitoring for cardiac implantable electronic device recipients and medical personnel. Subgroup analysis was conducted based on pre-RM survey responses, considering the hospital-to-home travel distance and the device type.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation. The categorical variables obtained by the survey were described using numbers, frequencies, and multiple-choice analysis, as appropriate. A paired t-test was used for pre-and post-remote monitoring measurements. All tests were two-sided, and a p-value of <0.05 was considered statistically significant. Statistical analyses were performed using R version 4.05 statistical software (R Foundation for Statistical Computing, Vienna, Austria) and Stata, version 16 (StataCorp LLC, College Station, TX, USA).
Results
Baseline Patient Characteristics
A total of 102 patients agreed to participate in the study. We excluded five pacemaker patients who passed away from non-cardiac-related causes (malignancy, bystander traffic accident, and an intracranial hemorrhage) during the post-remote monitoring period from the analysis. The analyzed sample included 79 pacemaker patients, 15 implantable cardioverter defibrillator patients, and 3 cardiac resynchronization therapy with defibrillator patients (Table 1). Information on travel time to the hospital was collected from the pre-RM survey: 42% of patients took less than 30 minutes, 34% took 30–60 minutes, and 24% took over an hour. 47% of patients indicated the need for caregiver accompaniment during in-person visits in the survey.
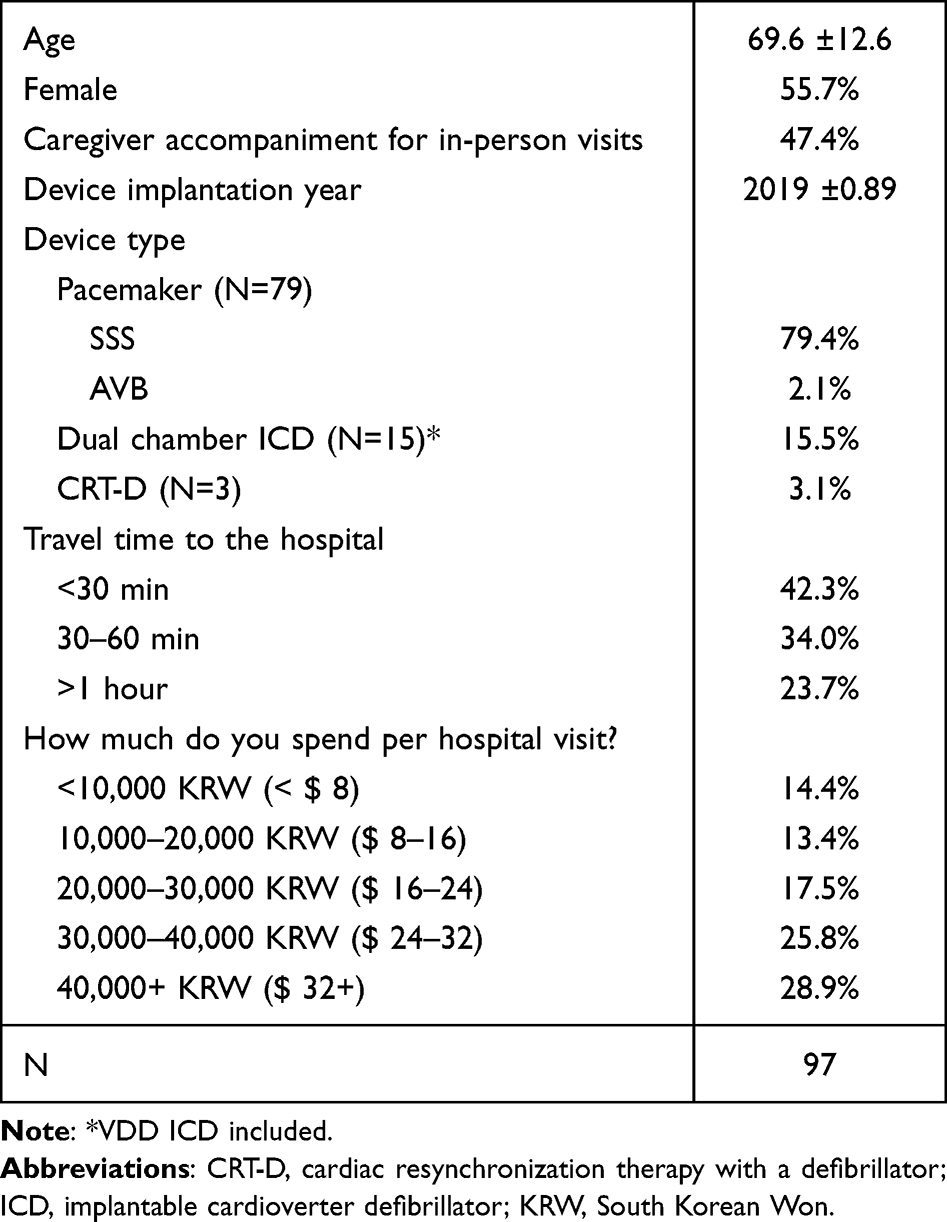 |
Table 1 Baseline Patient Characteristics |
Changes in Total Outpatient Visits Associated with Remote Monitoring Adoption
Remote monitoring decreased total outpatient visits from 3.7 to 2.7 per patient (Figure 2). In Figure 3A, total outpatient visits for pacemaker patients dropped from 3.6 to 2.6 (P < 0.001), whereas patients with ICD/CRT-D experienced a decrease from 3.8 to 3.2 (P = 0.36). People whose travel time to the hospital exceeded an hour experienced a drop in total outpatient visits from 3.8 to 2.3 during the post-RM period (P < 0.001), while those with travel times under 30 minutes saw a decrease from 3.8 to 2.9 visits (P = 0.03) (Figure 3B). Furthermore, a comparable trend in total out-of-pocket cost during hospital visits was associated with hospital visits observed among different device types (Figure 4).
 |
Figure 2 Pre- and post-remote monitoring total outpatient visit comparison. |
 |
Figure 3 Pre- and post-remote monitoring total outpatient visit comparison by device type (Panel A) and travel time to hospital (Panel B). |
 |
Figure 4 Pre- and post-remote monitoring costs during hospital visit comparison by device type (displayed in Korean Won). |
Unplanned Visits During Remote Monitoring
During the post-remote monitoring period, the study participants made 301 outpatient visits during the post-period. Out of the 65 non-routine visits, only 11 were initiated by physicians. Among these, 5 were related to device management problems, resulting in hospital visits due to pairing issues with the Cardio Messenger Smart device. Most of the non-routine visits during the post-implementation period were prompted by patients. Out of the 54 patient-initiated visits, only 13 involved medical consultations or discussions related to their health conditions.
Remote Monitoring Alerts (Immediate Actionable, Non-Emergent Actionable, and Non-Actionable Alerts)
During the 12-month follow-up period, a total of 1270 alerts for remote monitoring were received. Over 98% (1255 alerts) were determined to be nonactionable. Among 15 actionable alerts, 8 were non-emergent cases tied to CardioMessenger Smart or device parameter adjustments, promptly addressed within five business days. The remaining 7 urgent alerts originated from three patients: 2 from a patient undergoing cardiac resynchronization therapy with a defibrillator, involving ventricular tachyarrhythmia, and five from two patients with implantable cardioverter defibrillators. Four instances were attributed to a ventricular tachyarrhythmia storm in one patient. In all cases, clinical interventions were implemented within 24 hours of the remote monitoring alert.
Post-Remote Monitoring Patient Satisfaction Survey
Post-RM satisfaction survey showed increased patient satisfaction, cost-effectiveness, and facilitated health management without disrupting daily life.14 In Table 2, over 90% of the participants reported no discomfort with the remote monitoring, were willing to continue using it, and would like to recommend it to other patients with CEID. Less than 4% of participants reported feeling uneasy about not being able to see the medical staff in person and hesitated to use remote monitoring service. We found similar patterns across various patient device types, travel distances to the hospital, and whether caregiver assistance was needed during hospital trips.
 |
Table 2 Post-RM Patient Satisfaction Survey Results by Patient Device Type |
Discussion
Through telehealth, communication between medical staff and patients is improved. As the use of medical data expands, the storage, processing, and analysis of massive data and the resulting increase in workload are emerging problems.15 Appropriately integrating and visualizing such biometric data in electronic medical records is a significant burden.16 Data responsibility and security issues are also of concern.17 Removing and processing noise from the data obtained from a telehealth device may be required. In this respect, patients with a cardiac implantable electronic device can receive data under relatively constant conditions, such as heart rhythm or thoracic impedance measured by the heart.10,18,19
Patients with cardiac implantable electronic devices usually have an underlying arrhythmia or structural heart disease as an indication for electronic device implantation.20,21 Although most cardiac implantable electronic device recipients benefit from cardiac implantable electronic devices and experience a better quality of life after device implantation, they have concerns and uncertainty regarding post-cardiac implantable electronic device conditions.22,23 However, through this study, the researchers considered that the most significant advantage of remote monitoring was the improvement of patient satisfaction and quality of life. The CardioMessenger Smart-based remote monitoring used in this study enabled stable daily patient cardiac implantable electronic device monitoring, which decreased the workload of medical staff. In addition, due to daily remote monitoring, patients and guardians had much more trust in the medical staff. In addition, patients had more confidence in their health management without significant discomfort after remote monitoring (Table 2).
The National Health Insurance System in Korea is well established. Its comprehensive coverage enables high-quality medical services at relatively low costs to beneficiaries.24,25 While it is helpful to most people to maintain this insurance system, there is a problem in that insurance regulations become tighter. Delays occur when introducing new medical technologies compared to Western countries.26 Consequently, a patient imbalance exists between university/tertiary hospitals and small hospitals/primary clinics. In addition, there is a significant preference for regular hospital visits owing to low medical costs as an insurance benefit, which causes an increase in the number of patients per clinic, especially in tertiary or academic hospitals. This, in turn, results in a short clinic time per patient in many university or tertiary hospitals. Resolving existing information imbalances between patients and physicians in the real world is almost impossible. It is natural that the shorter the treatment time, the more significant this information gap will become. These factors lead to dissatisfaction among patients and inadequate cardiac implantable electronic device recipient management and may eventually worsen the clinical outcomes of patients with cardiac implantable electronic devices.
Remote monitoring in cardiac implantable electronic devices is a system that can provide individualized treatment and management tailored to each patient.27–29 But to apply this system, it is necessary to provide sufficient remote monitoring-related education to patients before remote monitoring implementation and to maintain adequate communication between patients and medical staff after the remote monitoring application. Additional prerequisites are required to reach optimal remote monitoring: dedicated and well-experienced personnel, facilities, and proper education of medical experts/caregivers/patients. The workload, as mentioned earlier, data management issues, responsibility, and security of data16,17,30 are also important matters.
The present study included a first survey on patient experience with remote monitoring.14 This study evaluated the safety and efficacy of remote monitoring and patient satisfaction after using remote monitoring in the necessity of domestic evidence for remote monitoring-related policy or insurance guidance. Based on this study, there are undeniable time and socioeconomic benefits for patients with cardiac implantable electronic devices following the remote monitoring application. Ultimately, the investigators hope that this study will serve as a basis for representing the needs of patients and medical staff, thereby providing an opportunity for cardiac implantable electronic device remote monitoring to be widely applied in Korea.
This study had several limitations. First, since it was performed in a single university hospital with a relatively small number of patients, the results might be generalizable to only some cardiac implantable electronic device recipients. Even though the study aimed to reflect cardiac implantable electronic device recipient satisfaction with remote monitoring, the survey was adopted and revised by a physician and had the limitation of perhaps not representing patient opinions fully. A high proportion of pacemaker patients were included in study. RM benefits primarily observed in this group for reduced hospital visits and cost-effectiveness. To determine the clinical safety and efficacy of remote monitoring in patients with cardiac implantable electronic devices, it is thought that the benefit of remote monitoring would have been higher if the proportion of implantable cardioverter defibrillator/cardiac resynchronization therapy with defibrillators was more significant. Finally, since this was a short-term follow-up study, the burden of medical staff, time, and cost reduction might have been underestimated in the present study. A more extended evaluation should be considered to confirm its efficacy and safety in a follow-up study.
Conclusion
Based on the survey, most patients with cardiac implantable electronic devices with remote monitoring experience were satisfied with the remote monitoring system using a CardioMessenger Smart device. Investigators confirmed that there were definite time- and cost-saving effects after remote monitoring. Nevertheless, to settle remote monitoring in practice in Korea, many things need to be supplemented by referring to other countries that apply remote monitoring, such as proper education and communication for patients and medical experts, the problem of leaving appropriate medical records, the safety of information related to remote monitoring, and legal liability issues. Setting reimbursement agreements and getting insurance coverage in Korea should be prioritized. The investigators speculate that the results of this study will serve as a basis for speeding up the realization of remote monitoring in Korea.
Data Sharing Statement
Due to the sensitive nature of the data, information created and analyzed during the current study is available from the corresponding author on reasonable request to bona fide researchers.
Acknowledgments
We sincerely thank Jin-gyu Choi and Jayhyeok Choi for their full support during the project and GangHyun Lee and JinAh Hwang for their help in remote monitoring and dedication to patient education. We want to thank Editage for the English language editing.
Funding
Biotronik supported funding the study and providing Cardiomessenger. Sponsors had no involvement from the study design to submitting the paper for publication.
Disclosure
Biotronik supported this study by providing Cardiomessenger and remote monitoring use. The authors report no conflicts of interest in this work.
References
1. Perino AC, Gummidipundi SE, Lee J, et al. Arrhythmias other than atrial fibrillation in those with an irregular pulse detected with a smartwatch: findings from the apple heart study. Circ Arrhythm Electrophysiol. 2021;14:e010063. doi:10.1161/CIRCEP.121.010063
2. Turakhia MP, Desai M, Hedlin H, et al. Rationale and design of a large-scale, app-based study to identify cardiac arrhythmias using a smartwatch: the apple heart study. Am Heart J. 2019;207:66–75.
3. Inui T, Kohno H, Kawasaki Y, et al. Use of a smart watch for early detection of paroxysmal atrial fibrillation: validation study. JMIR Cardio. 2020;4:e14857. doi:10.2196/14857
4. MacKinnon GE, Brittain EL. Mobile health technologies in cardiopulmonary disease. Chest. 2020;157:654–664.
5. Velmovitsky PE, Alencar P, Leatherdale ST, et al. Using apple watch ECG data for heart rate variability monitoring and stress prediction: a pilot study. Front Digit Health. 2022;4:1058826. doi:10.3389/fdgth.2022.1058826
6. Wasserlauf J, You C, Patel R, et al. Smartwatch performance for the detection and quantification of atrial fibrillation. Circ Arrhythm Electrophysiol. 2019;12:e006834.
7. Lopez-Liria R, Lopez-Villegas A, Leal-Costa C, et al. Effectiveness and safety in remote monitoring of patients with pacemakers five years after an implant: the poniente study. Int J Environ Res Public Health. 2020;17:1431. doi:10.3390/ijerph17041431
8. Briongos-Figuero S, Garcia-Alberola A, Rubio J, et al. Long-term outcomes among a nationwide cohort of patients using an implantable cardioverter-defibrillator: UMBRELLA study final results. J Am Heart Assoc. 2021;10:e018108. doi:10.1161/JAHA.120.018108
9. Tajstra M, Sokal A, Gadula-Gacek E, et al. Remote supervision to decrease hospitalization rate (RESULT) study in patients with implanted cardioverter-defibrillator. Europace. 2020;22:769–776. doi:10.1093/europace/euaa072
10. Zakeri R, Morgan JM, Phillips P, et al. Impact of remote monitoring on clinical outcomes for patients with heart failure and atrial fibrillation: results from the REM-HF trial. Eur J Heart Fail. 2020;22:543–553. doi:10.1002/ejhf.1709
11. Varma N, Kondo Y, Park SJ, et al. Utilization of remote monitoring among patients receiving cardiac resynchronization therapy and comparison between Asia and the Americas. Heart Rhythm O2. 2022;3:868–870. doi:10.1016/j.hroo.2022.06.013
12. Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Europace. 2022;24:71–164. doi:10.1093/europace/euab232
13. Hwang YM, Kim JH. The first survey on patient needs for remote monitoring of cardiac implantable electronic device in South Korea. Medicine. 2022;101:e29414. doi:10.1097/MD.0000000000029414
14. Hwang Y, Bae H. The first remote monitoring experience in South Korea: results of a remote-care study. Europace. 2023;25(6):euad150. doi:10.1093/europace/euad150
15. Tuckson RV, Edmunds M, Hodgkins ML. Telehealth. N Engl J Med. 2017;377:1585–1592. doi:10.1056/NEJMsr1503323
16. O’Shea CJ, Middeldorp ME, Hendriks JM, et al. Remote monitoring alert burden: an analysis of transmission in 26,000 patients. JACC Clin Electrophysiol. 2021;7(7):226–234. doi:10.1016/j.jacep.2020.08.029
17. Das S, Siroky GP, Lee S, et al. Cybersecurity: the need for data and patient safety with cardiac implantable electronic devices. Heart Rhythm. 2021;18:473–481. doi:10.1016/j.hrthm.2020.10.009
18. Della Rocca DG, Albanese M, Placidi F, et al. Feasibility of automated detection of sleep apnea using implantable pacemakers and defibrillators: a comparison with simultaneous polysomnography recording. J Interv Card Electrophysiol. 2019;56:327–333. doi:10.1007/s10840-019-00631-x
19. Auld JP, Mudd JO, Gelow JM, et al. Device-detected congestion is associated with worse patient-reported outcomes in heart failure. Heart Lung. 2019;48(3):208–214. doi:10.1016/j.hrtlng.2018.12.003
20. Kelly SE, Clifford TJ, Coyle D, et al. Virtual follow-up and care for patients with cardiac electronic implantable devices: protocol for a systematic review. Syst Rev. 2020;9:153. doi:10.1186/s13643-020-01406-6
21. Kelly SE, Clifford TJ, Skidmore B, et al. Patient and healthcare provider reported barriers and enablers to virtual or remote-only follow-up models for cardiovascular implantable electronic devices: protocol for a qualitative framework synthesis. Syst Rev. 2020;9:151. doi:10.1186/s13643-020-01410-w
22. Catalan-Matamoros D, Lopez-Villegas A, Tore-Lappegard K, et al. Patients’ experiences of remote communication after pacemaker implant: the NORDLAND study. PLoS One. 2019;14:e0218521. doi:10.1371/journal.pone.0218521
23. Haugaa KH, Potpara TS, Boveda S, et al. Patients’ knowledge and attitudes regarding living with implantable electronic devices: results of a multicentre, multinational patient survey conducted by the European Heart Rhythm Association. Europace. 2018;20:386–391. doi:10.1093/europace/eux365
24. Kim HB, Lee SM. When public health intervention is not successful: cost sharing, crowd-out, and selection in Korea’s National Cancer Screening Program. J Health Econ. 2017;53:100–116. doi:10.1016/j.jhealeco.2017.02.006
25. Kim YK. Forecasting the future reimbursement system of Korean National Health Insurance: a contemplation focusing on global budget and Neo-KDRG-based payment systems. J Korean Med Sci. 2012;27:S25–32. doi:10.3346/jkms.2012.27.S.S25
26. Boriani G, Burri H, Svennberg E, et al. Current status of reimbursement practices for remote monitoring of cardiac implantable electrical devices across Europe. Europace. 2022;24:1875–1880. doi:10.1093/europace/euac118
27. Treskes RW, Beles M, Caputo ML, et al. Clinical and economic impact of HeartLogic compared with standard care in heart failure patients. ESC Heart Fail. 2021;8:1541–1551. doi:10.1002/ehf2.13252
28. Wintrich J, Pavlicek V, Brachmann J, et al. Remote monitoring with appropriate reaction to alerts was associated with improved outcomes in chronic heart failure: results from the optilink HF study. Circ Arrhythm Electrophysiol. 2021;14:e008693. doi:10.1161/CIRCEP.120.008693
29. Ruiz Diaz MA, Egea Garcia M, Munoz Aguilera R, et al. Patient satisfaction with remote monitoring of cardiac implantable electronic devices: the VALIOSA questionnaire. BMC Health Serv Res. 2020;20:354. doi:10.1186/s12913-020-05216-3
30. Slotwiner DJ, Al-Khatib SM. Digital health in electrophysiology and the COVID-19 global pandemic. Heart Rhythm O2. 2020;1:385–389.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.