Back to Journals » Patient Preference and Adherence » Volume 20
Patient Engagement in Person-Centered Communication About Medication Adherence: Perspectives From Patients, Next of Kin, and Healthcare Professionals
Authors Kudusova T ![]() , Devold HM, Lilleheim NE, Sletvold H
, Devold HM, Lilleheim NE, Sletvold H
Received 11 February 2026
Accepted for publication 2 May 2026
Published 4 June 2026 Volume 2026:20 602451
DOI https://doi.org/10.2147/PPA.S602451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Tamara Kudusova,1– 3 Helene Margrethe Devold,2 Nils Espen Lilleheim,4 Hege Sletvold1
1Division of Medicines and Medication Management, Faculty of Nursing and Health Sciences, Nord University, Stjørdal, Norway; 2Aalesund Hospital Pharmacy, Central Norway Pharmaceutical Trust, Aalesund, Norway; 3Department of Clinical and Molecular Medicine, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Trondheim, Norway; 4Independent Patient Research Partner, Aalesund, Norway
Correspondence: Tamara Kudusova, Division of Medicines and Medication Management, Faculty of Nursing and Health Sciences, Nord University, Stjørdal, Norway, Tel +47-40099021, Email [email protected]
Purpose: To explore how patients can be actively engaged in medication adherence communication in a person-centered manner.
Patients and Methods: A design thinking approach was applied, involving patients, next of kin, physicians, nurses, and pharmacists through workshops and individual interviews. Data was analyzed using reflexive thematic analysis.
Results: Two main themes were identified. The first, Reassurance as a foundation for person-centered communication about medication adherence, described adherence communication as a multi-layered and co‑constructed process. Reassurance was established through relational engagement and mutual trust, enabling patients to participate more openly and confidently in discussions about their medication use. The second theme, Healthcare professional as fellow human and expert, highlighted patients’ need to be met “as a person” while simultaneously relying on the healthcare professional’s expertise. Participants emphasized the importance of professionals who “know their stuff but speak my language” translating clinical knowledge into understandable, meaningful dialogue. A “reassuring mindset” where human and expert qualities converge, was identified as central to fostering patient engagement in adherence conversations.
Conclusion: Reassurance was identified as a central enabling factor for engaging patients in medication-adherence communication. The findings emphasize that a synergistic combination of human connection and professional competence is essential. These results can inform the development of communication strategies and professional skills aimed at building partnerships in adherence. Further research should explore how reassurance can be operationalized in person-centered adherence interventions and its impact on treatment outcomes.
Plain Language Summary: Why was this study done? Taking medications as prescribed is essential for managing chronic conditions, yet many people struggle to do so consistently. Less is known about how communication between patients and healthcare providers can support medication adherence. We wanted to understand what makes these conversations helpful and how patients can be actively engaged in them.
What did we do? We used a design thinking approach, conducting workshops and individual interviews with patients, their next of kin, and healthcare professionals (physicians, nurses, and pharmacists). We explored their experiences and perspectives on communication about medication adherence.
What did we find? Two key themes emerged. First, reassurance is central to enabling person-centered adherence communication. Reassurance involves feeling safe, understood, and supported, and is built through ongoing interactions between patients and healthcare professionals. Second, the healthcare professional’s dual role as both a fellow human and an expert is essential. Patients need to be seen as individuals, not just as patients, and they need clear, trustworthy guidance delivered in understandable language.
What does this mean? Healthcare providers can support medication adherence by building trusting, person-centered relationships, not just by providing information. Combining empathy and professional expertise fosters the reassurance patients need to engage in their treatment. These findings have implications for training healthcare professionals and designing communication strategies for chronic care settings.
Keywords: medication use behavior, reassurance, therapeutic alliance, person-centered pharmacy service
Introduction
Medication adherence (henceforth, adherence only) refers to the extent to which a patient takes his/her medicines as agreed with the doctor, ie., at the right time, with the appropriate dosage and frequency.1 Adherence is particularly challenging for patients with chronic diseases.2–4 Systematic literature reviews and meta-analyses show that patients with cardiovascular disease have challenges with adherence, for example, in cases of hypertension (45.2%),2 after stroke (35.9%),3 and atrial fibrillation (34%).4 Non-adherence to treatment has unfortunate consequences, particularly for the individual patient and society.1 Non-adherence is associated with increased mortality and morbidity, reduced treatment efficacy, and higher healthcare costs.5 A study reports up to US$44,000 in annual per-person expenses attributable to non-adherence and estimates that increasing adherence to antihypertensive agents to 70% in five European countries would prevent 82,235 cardiovascular events and save more than $330 million over ten years.6
Adherence behavior is complex and influenced by numerous interacting factors that can change over time, including those related to the healthcare system, healthcare professionals (HCPs), patients, the therapy or condition itself, and broader social or economic factors.1,7 More than 700 factors potentially affecting adherence have been identified, making it challenging to predict the reasons for non-adherence.8 Given the complexity of these interacting factors, it becomes essential to explore theoretical frameworks that explain adherence behavior. Numerous models have been established to elucidate health behavior and adherence, including the Health Belief Model (HBM),9 the Theory of Planned Behavior (TPB),9 the Social Cognitive Theory (SCT),9 Self-Determination Theory (SDT),10,11 and others. These models emphasize patients’ attitudes, beliefs, and self-efficacy. Notably, Self-Determination Theory (SDT) is particularly relevant in this context, as it provides a theoretical bridge between person-centered care and adherence behavior. SDT explains health-related behavior through the satisfaction of basic psychological needs for autonomy, competence, and relatedness.10,12 Applied to medication adherence, SDT suggests that long-term adherence is more likely when patients are autonomously motivated, when treatment decisions are understood, accepted, and integrated into the patient’s own values and daily life.11,13 This theoretical perspective highlights the importance of healthcare encounters that actively support patients’ autonomy, understanding, and sense of partnership in treatment decisions.
Medicines Use Review (MUR), New Medicines Service (NMS), and Medication Therapy Management (MTM) are person-centered consultations in pharmacies that support medication use and adherence.14–16 While generally perceived positively by patients and pharmacists,17–19 a scoping review found that pharmacist-led consultations have limited engagement with patients and their health problems.15 Further research is needed to address facilitators and barriers to patient participation in such services.20 Moreover, counseling and interventions aimed at improving adherence should be aware of differing perspectives on non-adherence between patients and providers.21 Additionally, engaging multiple stakeholders in the development of tools and systems to facilitate person-centered medication management initiatives is advisable.22
Despite extensive research, there remains a need to identify feasible approaches to patient-HCP relationships and communication strategies that actively engage patients in medication management and adherence, and that are implementable in routine practice.23,24 In Norway, two structured, pharmacy-led adherence services are currently available: an inhalation technique assessment service25 and Medisinstart, inspired by the NMS and targeting patients initiating cardiovascular therapy.26 However, Norwegian community pharmacies have yet to implement MUR or MTM services to support long-term therapies. Consequently, further research is needed to develop person-centered care services that promote sustained adherence in the Norwegian context. Such services must be tailored to meet patients’ individual needs and preferences during adherence consultations, while also being adaptable to collaborating HCPs, other stakeholders, and the realities of the practice field.15,18,19,21
This study aims to explore how patients can be actively engaged in medication adherence communication in a person-centered manner, drawing on the perceptions and lived experiences of patients, next of kin, and healthcare professionals. Using a bottom-up, human-centered methodology, the study draws on stakeholders’ experiences and direct feedback, where the overarching goal is to establish a foundation for designing a service that supports long-term adherence among patients using cardiovascular medications.
Material and Methods
Study Design
This study adopts a Design Thinking (DT) approach, selected for its effectiveness in solving complex problems through a human-centered lens.27,28 DT prioritizes a deep understanding of users’ needs and experiences, ensuring that the perspectives of patients, next of kin, and HCP are continuously integrated throughout the development process. This methodology is particularly suited to designing interventions that are empathetic, feasible, and sustainable. The Stanford University Design Thinking model comprises five iterative stages: Empathize, Define, Ideate, Prototype, and Test.27
In this study, the Empathize and Define stages were addressed through literature review and questionnaire surveys, which helped identify stakeholder needs, experiences, and motivations related to medication adherence. The Ideate and Prototype stages involved individual interviews and co-creation workshops with a diverse group of stakeholders. Further details on data collection methods and participant recruitment are provided in subsequent sections.
Research Team and Reflexivity
In this study, we bring a preconception based on HS and HMD’s previous academic research in the field of adherence; TK, HS, and HMD’s clinical experience with patient counseling; and NEL’s personal experiences with disease and medication management.
TK had prior experience conducting qualitative research using interviews; HMD had experience with quantitative research, including surveys and literature reviews; and HS had extensive experience with qualitative, quantitative, and mixed-methods research.
Coding and categorization were conducted by two researchers (TK and HS) and subsequently refined through iterative discussions within the research group to ensure transparency, reflexivity, and confirmability of the analysis. Potential preconceptions were systematically addressed through a continuous, reflexive process maintained throughout all stages of the research.
Study Setting, Sampling Strategy, and Recruitment
The study was conducted in More and Romsdal county, located in the northernmost part of western Norway.
Three stakeholder groups were included: patients, next of kin, and HCP. Recruitment was conducted through purposive sampling to capture variation in experiences related to medication use, adherence, and communication with healthcare services. Patients and next of kin were primarily recruited through the Norwegian Association for Heart and Lung Patients (LHL) and the Aalesund hospital pharmacy. Healthcare professionals were recruited through General Practitioners’ (GPs) offices, hospital departments (Aalesund Hospital), and local pharmacies, including one hospital pharmacy. Inclusion criteria varied by stakeholder group: HCPs (GPs, nurses, pharmacists) were eligible if they had experience in guiding or following up patients using medication for chronic conditions. Patients were eligible if they were aged 18 years or older and had been taking one or more cardiovascular medications for at least 1 year. Next of kin were included if they had experience caring for a person who was taking medication for a chronic illness.
Data
Data was collected from January 2023 to December 2023. A multi-method approach was used to ensure richness and depth of the qualitative inquiry. The following methods were used:
- Literature review: A targeted literature review was conducted to identify relevant research on theoretical perspectives of medication adherence and patient - HCP communication. Searches were performed in PubMed and Google Scholar using relevant keywords. The review informed the study design, the development of the interview guides, and the conceptual approach to data analysis.
- Questionnaires: A brief anonymous paper-based questionnaire (see Figure S1 in Appendix 1) was voluntarily offered to patients collecting cardiovascular medications at a hospital pharmacy (TK). The open-ended questionnaire aimed to gather insights into patients’ priorities, decision-making processes, challenges, motivations, and their need for support from pharmacists regarding medication use. Responses (n = 23), along with findings from a literature review, were used to design the interview guide and prepare for workshops. The questionnaire data were used solely for preparatory purposes and are not included in the thematic analysis; the results presented in this article are based solely on data from interviews and workshops.
- Interviews: In total, 12 participants were interviewed; ten were interviewed individually for approximately 30–45 minutes using a semi-structured interview guide (see Figure S2 in Appendix 2 and Figure S3 in Appendix 3). Two participants were interviewed together in a single session lasting 90 minutes (interview guide, see Figure S4 in Appendix 4). All interviews were audio-recorded and transcribed verbatim (TK).
- Workshops: Workshops were designed to facilitate dialogue and co-creation among participants regarding their understanding and experiences of medication adherence, and their views on how HCPs can support medication adherence. Appendix 5 provides an overview of pre-workshop activities and the workshop program, including the discussion guide (see Figure S5 in Appendix 5). Two workshop sessions were conducted, comprising six and eight participants, respectively. Some participants attended both workshops, and some subsequently participated in an interview. TK and HS facilitated the workshops, while HMD and NEL participated actively. Each workshop lasted approximately 180 minutes and was audio-recorded and transcribed verbatim.
Data Analysis
Data from workshops and semi-structured interviews were analyzed using reflexive thematic analysis, as outlined by Braun and Clarke.29–31 The process was iterative and researcher-generated, where all researchers were actively engaged and emphasized reflexive, meaning-based interpretation. Researchers (TK and HS) initially read the transcripts repeatedly to familiarize themselves with the dataset, making preliminary reflective notes and highlighting early analytical insights. Coding was conducted across the entire dataset, generating interpretative, flexible codes that captured patterns of meaning relevant to the research aim. Codes were then grouped into initial themes by grouping conceptually related meanings (TK and HS). Themes were reviewed, refined, and further developed through collaborative discussions (TK, HS, HMD, and NEL). Data extracts were revisited to ensure that the themes were coherent, meaningful, and grounded in the dataset (TK, HS, and NEL). The final themes were iteratively shaped into a coherent analytical narrative (TK and HS), supported by illustrative quotations selected to capture the essence of each theme.
Results
A total of 25 participants contributed data to the reflexive thematic analysis (Table 1): 19 females and six males. Two participants contributed to both workshops and individual interviews.
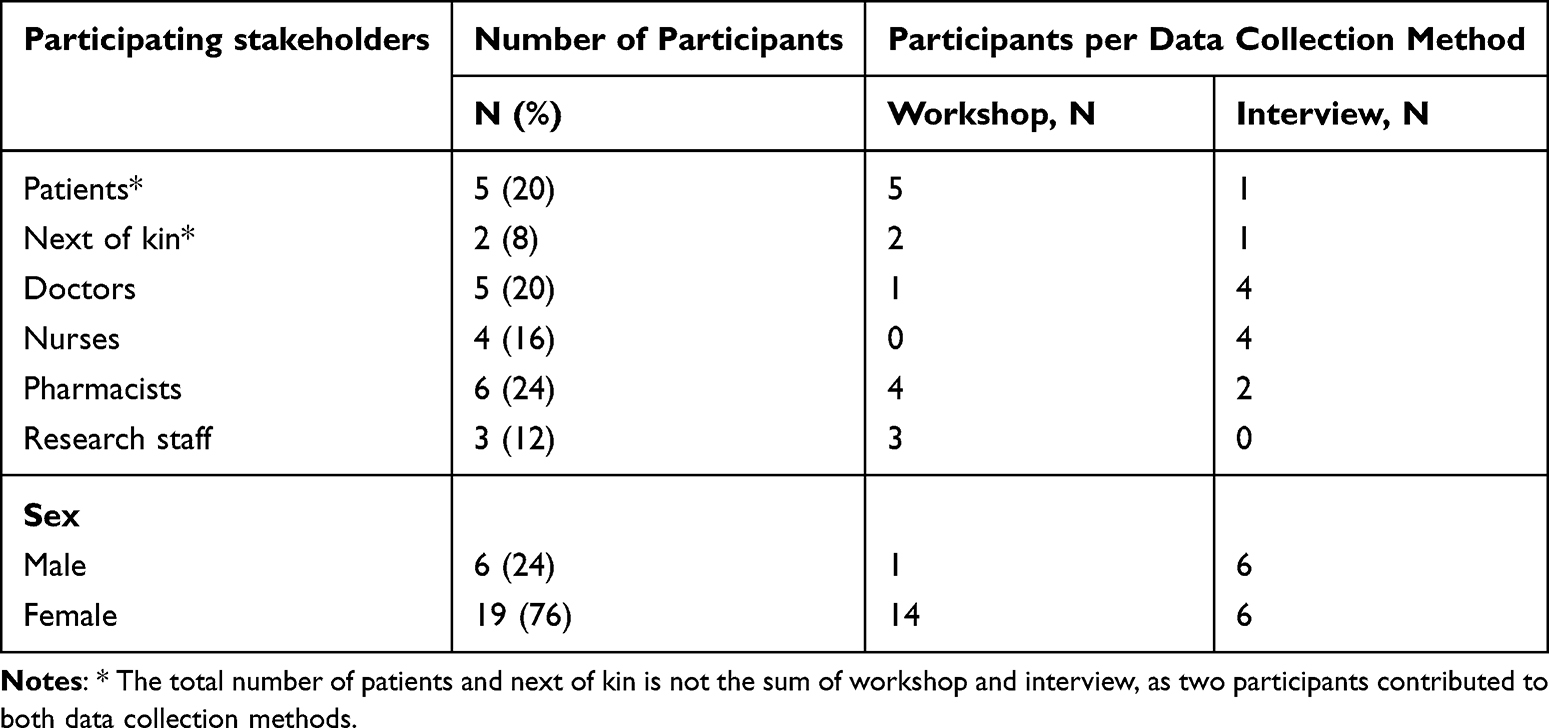 |
Table 1 Information About Study Participants |
The analysis yielded two main themes, each comprising subthemes that shed light on how patients can be actively engaged in person-centered adherence communication (Figure 1). The main themes were: 1) Reassurance as a foundation for person-centered communication about medication adherence; 2) Healthcare professional as fellow human and expert. These themes and their associated subthemes are described and illustrated in the following section, supported by participant quotes that substantiate the thematic interpretations.
 |
Figure 1 Overview of themes and subthemes representing how patients can be actively engaged in medication adherence communication in a person-centered manner. |
Reassurance as a Foundation for Person-Centered Communication About Medication Adherence
The analysis revealed that reassurance plays a central role in enabling person-centered communication about medication adherence. Rather than being a single event or message, reassurance is a co-constructed process. It is shaped by ongoing interactions among HCPs, patients, and their support networks, and is deeply embedded in the quality of the therapeutic relationship.
A Multi-Layered and Co-Constructed Process
Reassurance emerged as a dynamic, relational process woven through multiple interrelated aspects that shaped patients’ confidence and willingness to engage in adherence communication. At its core was the relational aspect, where being seen, heard, and met with empathy and respect provided the foundation for trust. Participants stressed that without trust, dialogue about medication use was impossible.
I can’t discuss medication use with a person I don’t trust, Patient 2, workshop.
This relational base was reinforced by the cognitive aspect, where clear, individually tailored information enabled patients to understand their treatment and participate actively. Knowledge was empowering, but reassurance also depended on clinical experience, a sense of positive outcomes, and confidence that the treatment was evidence-based and adapted to individual needs, such as kidney function.
The context of care also mattered. A calm environment, sufficient time, and freedom from distractions were seen as essential for meaningful dialogue.
When you’re in a conversation, it’s important that the patient is at the center. Not your email. Not the computer screen. Not incoming messages – Patient 3, interview.
The presence of next of kin during consultations further enhanced reassurance by providing additional support and information.
We become an extra set of eyes and ears. We can gather information, ask questions, and help recall what has been said. If the patient has any questions afterward, we can confirm or deny, provide reassurance – Next of kin 1, interview.
Beyond consultation, reassurance was strengthened by support from family and friends, who played a key role in encouraging adherence, and by a well-functioning health system, in which coordinated communication provided security and continuity.
Finally, reassurance was shaped by personal strategies for managing uncertainty, such as trusting one’s own decisions and filtering external influences.
I don’t have that kind of inner conflict, because. I have chosen to trust the GP… and I have decided to close my eyes and ears to such [social media] discussions about the use of medicines, Patient 3, interview.
Establishing Reassurance Through Relational Engagement and Mutual Trust
Participants described reassurance as a process that requires active collaboration between HCPs and patients. However, they emphasized that HCPs are responsible for initiating the process of establishing reassurance due to the inherent demand of their professional roles. Furthermore, participants highlighted that trust cannot be assumed but must be built, creating a foundation for a positive and mutually beneficial relationship.
The true value [of communication between HCP and patient] really rests on trust: whether there is trust or not….and the benefits are perceived on a completely different level, Pharmacist 1, interview.
Reassurance begins with an invitation to engage in open, meaningful dialogue, in which HCPs demonstrate genuine interest in the patient’s concerns, needs, and experiences. First impressions, such as feeling welcomed, respected, and unhurried, were considered essential.
Participants noted that sufficient time is critical, as patients may need space to process and express their thoughts.
I have to search for words… search for meaning… and that can be a bit frustrating. But it usually works out, as long as we have time and I am allowed to search for the words, Patient 3, interview.
Empathic communication was described as promoting reassurance by signaling that patients are heard, understood, and supported. Listening to subtle cues and responding appropriately is important, enabling HCPs to create an environment where patients feel safe sharing their challenges, needs, and expectations.
Knowledge of the patient’s disease and life situation provided reassurance. Patients valued consultations tailored to their current health status, while repeating difficult information could awaken distressing emotions and diminish the effect of reassurance.
It is tough to repeat difficult things. Maybe I’ll handle it the first time, but if I come the second time, I can’t bear to go through it, Patient 1, workshop.
The manner in which information was conveyed also influenced patients’ sense of reassurance. Patients valued dialogical interactions rather than unidirectional information delivery, particularly when HCPs actively checked for understanding and ensured shared meaning.
It means a lot that HCP checks what we have talked about, that I have understood it correctly. That I don’t leave the room with a completely different perception than what was actually said. Patient 3, interview.
The power dynamic between HCPs and patients was acknowledged as a potential barrier to reassurance. Patients described feeling hesitant to ask questions due to perceived authority.
Doctors embody authority. Even though I am an expert on my health, asking naive questions makes me feel unwise, Patient 2, workshop.
Patients believed that balancing this power dynamic requires treating patients as equal partners through repeated invitations to ask questions, by emphasizing that there are no foolish questions, and recognizing patients as experts in their own health. Patients who feel empowered to engage openly were described as more likely to achieve reassurance and, consequently, adhere to their medication.
Healthcare Professional as a Fellow Human and Expert
To enable person-centered communication that supports long-term medication adherence, a synergistic combination of human connection and professional competence is needed.
“Meet Me as a Person” in the Adherence Communication
Meeting the patient as a person, acknowledging their experiences, feelings, and needs that extend beyond the disease and treatment itself, is essential to enable patients to engage in adherence communication. Participants valued HCPs who demonstrated empathy and presence, creating a relationship in which the patient is treated as an equal partner.
We should be empathetic pharmacists with a curious mindset, not strict and dedicated, Pharmacist 5, workshop.
Patients appreciated when HCPs were genuine and honest, even in situations of uncertainty, and avoided hiding behind medical jargon. An autonomy-supportive attitude was also seen as essential, recognizing that medication use is ultimately a voluntary act and that adherence should be framed as a collaborative choice, not a moral judgment.
It does not make sense to talk about poor or good adherence. The patient is autonomous and can, in fact, choose whether to take the medication or not, Pharmacist 1, interview.
It is not something I do just because the doctor says so. I understand the function and the need Patient 3, interview.
“Know Your Stuff but Speak My Language”: Translating Expertise Into Trust
HCPs need to apply clinical knowledge and expertise in a manner that is meaningful and relevant to the patient. Participants expected HCPs to act in accordance with laws, professional standards, and ethical guidelines.
It is important to know that the doctor has taken into account weight, kidney function, interactions when choosing the drug and dosage. what the doctor has said to the patient, whether the doctor has considered the latest guidelines, Pharmacist 4, workshop
Beyond technical competence and providing instructions, participants highlighted the value of giving the patient a basis for making their own decisions.
Exploring the patient’s understanding of their illness and their understanding of medication use, that is a skill one should have. Pharmacist 2, interview.
Demonstrating collaboration, accountability, and continuity also strengthens patients’ adherence. Patients found it reassuring when pharmacists contacted their physician on their behalf or followed up with them over time.
I once experienced … that the pharmacist called the doctor. And I was in such a good mood, I was so grateful both to the doctor who answered the phone and the pharmacist who called. For me, as a patient, this was very reassuring, Patient 2, workshop.
A Reassuring Mindset - Where the Human and Expert Meet
When the human and expert perspectives of the HCP are combined, a reassuring mindset emerges. Patients are met with both empathy and knowledge, and experience genuine involvement in decision-making. This enables a shift away from a paternalistic focus on “good” or “poor” adherence, towards a person-centered approach in which adherence is understood as a collaborative effort.
Such a mindset means that communication is not about “teaching the patient,” but about learning together with the patient:
The conversation should be… of such a nature. that the patient is invited to teach the pharmacist how it is going. Pharmacist 1, interview.
Participants emphasized that human qualities, such as empathy, can be learned and developed in the same way that knowledge in pharmacology can be acquired, and that HCPs need to invest in developing their human qualities, just as they would with other professional skills.
Discussion
This study aimed to explore the perceptions and lived experiences of patients, next of kin, and HCPs regarding medication adherence. Using person-centered methodology, the findings revealed that reassurance is a central enabler of engagement in adherence communication, emerging through relational, communicative, and professional interactions. The results illustrate that reassurance is not a singular act, but a multidimensional, co-constructed process shaped by empathy, trust, clinical competence, and continuity of care.
Reassurance in the context of medication adherence has received little attention in the research literature. Existing studies have primarily focused on patients with unexplained medical symptoms rather than individuals using medication for chronic conditions.32,33 Akyirem et al describe reassurance as a complex construct that involves the use of interpersonal skills to establish and sustain emotional connections with patients and their families.33 In the present study, reassurance in adherence communication can be understood as a process of providing patients with a sense of treatment safety, both physiologically, by ensuring that the medication is appropriate and safe, and psychologically, by addressing concerns and fostering trust in both the treatment and the HCP.
The insights generated in this study can be linked to the WHO`s five dimensions of adherence.1 Within this framework, reassurance can be understood as a cross-cutting process influencing all five dimensions, highlighting the need for adherence communication that addresses multiple, interrelated factors. This interpretation aligns with broader adherence literature emphasizing the importance of multidimensional interventions.23,34 Our findings suggest that such an approach can be operationalized by applying reassurance strategies to actively engage patients in adherence-related consultations.
Our findings align with prior studies, which show that communication about medication use extends beyond simple information transfer and requires comprehension, compassion, and flexibility.18,19 Patients in our study emphasized that they must first trust the HCP and feel reassured before they can commit to engaging in a medication use dialog. This aligns with research showing that reassurance is the most critical action providers can take to build trust early in the therapeutic relationship.35
This dynamic, where reassurance precedes commitment, can be further understood through the SDT perspective. Reassurance fosters a sense of connection, fulfilling the need for relatedness. When delivered through open and respectful dialogue, it supports autonomy by making patients feel valued and trusted to make their own decisions. Furthermore, when reassurance includes clear and relevant information, it builds competence by equipping patients to understand and manage their health. Together, these aspects of reassurance support intrinsic motivation, which has been shown to facilitate long-term medication adherence.13
The reassurance model proposed by Pincus et al (2013) distinguishes between affective reassurance, defined as showing empathy, comfort, and care, and cognitive reassurance, which involves providing clear information about collaborative treatment planning.36 This model aligns with our findings, in which participants emphasized that patients expect HCPs to demonstrate both professional expertise and compassion; a reassuring mindset. This mindset facilitates person-centered adherence communication by, for example, demonstrating empathy. Jubrai and co-authors have critically discussed the need for pharmacists to underpin medication consultations with empathy, as patients want HCP to demonstrate clinical empathy.37 Several studies have demonstrated that empathy is not only an innate trait but also a skill that can be taught and developed through targeted training.38,39 The results of our study suggest that empathy and communication skills should be acquired and maintained alongside clinical knowledge to ensure person-centered adherence communication.
Implications
To aid long-term medication adherence, a positive relationship and effective communication between patients and HCPs are essential. Based on the results of this study, we argue that reassurance plays a central role in enabling patient engagement in adherence communication. Moreover, the results presented can serve as a guide for developing communication strategies and HCP skills in adherence communication to establish partnerships in adherence. Skills in person-centered communication and a reassurance-oriented mindset are essential for HCPs delivering adherence services. Yet in Norway, undergraduate curricula for pharmacists (and likely other HCPs) rarely include structured training in these areas, leaving many HCPs without a clear understanding of why these skills matter and how to apply them in practice. Embedding such competencies in both undergraduate curricula and continuing professional development would represent a meaningful step toward improving consultation quality and, ultimately, adherence outcomes. Future adherence services should be designed with this in mind, ensuring that those who deliver them are adequately equipped. Hence, further research is needed to explore how reassurance can be effectively used in person-centered medication adherence consultation interventions and assess its impact on achieving medication treatment goals.
Strength and Limitations
A strength is the use of design thinking, which emphasizes empathy and understanding of the end user’s needs. Furthermore, the active involvement of a non-academic co-researcher is a strength of this study. Data analysis was conducted in multiple stages, and all authors were involved. However, our study has limitations. Self-reporting by participants and group dynamics in workshops could lead to bias. Human-centeredness in design thinking could also introduce biases and overshadow the need for theoretical exploration. The iterative nature of design thinking can also be more time-consuming, and the time used to conduct our research could be inappropriate for collecting enough data. Therefore, while our study provides in-depth insights into specific contexts or challenges, findings may not always apply to broader populations or settings.
Conclusion
This study highlights reassurance as a foundational element of patient-centered communication about medication adherence and extends existing theoretical perspectives by framing reassurance as an enabling factor that operates across multiple dimensions of adherence. Reassurance emerges in adherence consultations through an active, co-constructed relationship between HCPs and patients. HCP characteristics, being a fellow human and expert, can strengthen patient reassurance and, consequently, medication adherence.
Data Sharing Statement
The datasets analyzed during the current study are not publicly available due to ethical and privacy reasons.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. The Regional Committee for Medical and Health Research Ethics (REK, reference: 542227) concluded that the study did not require formal ethical approval. The study was approved by the Norwegian Agency for Shared Services in Education and Research (SIKT, reference: 548839) for data protection compliance. Participants were informed of the study’s aims, methods, and potential risks. Written consent was obtained for workshops, verbal consent for interviews, and surveys were anonymous. All data were de-identified and are securely stored with access restricted to researchers HS, TK, and HMD.
Consent for Publication
All study participants provided their consent to participate, including publication of anonymized responses and quotes.
Acknowledgments
We would like to express our sincere gratitude to the participants in this study for their valuable contributions. We are also grateful to the Norwegian Pharmacy Foundation for its financial support, which made this research possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was conducted as part of TK’s PhD project, which is funded by the Norwegian Pharmacy Foundation (grant dated 21.04.2022). No additional funding was received from public, commercial, or not-for-profit sectors.
Disclosure
TK and HMD: working at Aalesund Hospital Pharmacy, Central Norway Pharmaceutical Trust. The authors report no other conflicts of interest in this work.
References
1. Sabaté E. Adherence to Long-Term Therapies: evidence for Action. 2003. Available from: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf.
2. Abegaz TM, Shehab A, Gebreyohannes EA, Bhagavathula AS, Elnour AA. Nonadherence to antihypertensive drugs: a systematic review and meta-analysis. Medicine. 2017;96(4):e5641. doi:10.1097/md.0000000000005641
3. Zhang J, Gong Y, Zhao Y, Jiang N, Wang J, Yin X. Post-stroke medication adherence and persistence rates: a meta-analysis of observational studies. J Neurol. 2021;268(6):2090–11. doi:10.1007/s00415-019-09660-y
4. Ozaki AF, Choi AS, Le QT, et al. Real-world adherence and persistence to direct oral anticoagulants in patients with atrial fibrillation: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2020;13(3):e005969. doi:10.1161/circoutcomes.119.005969
5. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. 2018;8(1):e016982. doi:10.1136/bmjopen-2017-016982
6. Mennini FS, Marcellusi A, von der Schulenburg JM, et al. Cost of poor adherence to anti-hypertensive therapy in five European countries. Eur J Health Econ. 2015;16(1):65–72. doi:10.1007/s10198-013-0554-4
7. Chapman SCE, Chan AHY. Medication nonadherence - definition, measurement, prevalence, and causes: reflecting on the past 20 years and looking forwards. Front Pharmacol. 2025;16:1465059. doi:10.3389/fphar.2025.1465059
8. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4:91. doi:10.3389/fphar.2013.00091
9. Amico KR, Mugavero M, Krousel-Wood MA, Bosworth HB, Merlin JS. Advantages to using social-behavioral models of medication adherence in research and practice. J Gen Intern Med. 2018;33(2):207–215. doi:10.1007/s11606-017-4197-5
10. Ryan RM, Patrick H, Deci EL, Williams GC. Facilitating health behaviour change and its maintenance: interventions based on self-determination theory. Eur Health Psychol. 2008;10(1):2–5.
11. Kennedy S, Goggin K, Nollen N. Adherence to HIV medications: utility of the theory of self-determination. Cogn Ther Res. 2004;28(5):611–628. doi:10.1023/B:COTR.0000045568.95219.e2
12. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68–78. doi:10.1037/0003-066X.55.1.68
13. Williams GC, Rodin GC, Ryan RM, Grolnick WS, Deci EL. Autonomous regulation and long-term medication adherence in adult outpatients. Health Psychol. 1998;17(3):269–276. doi:10.1037/0278-6133.17.3.269
14. Marupuru S, Roether A, Guimond AJ, Stanley C, Pesqueira T, Axon DR. A systematic review of clinical outcomes from pharmacist provided Medication Therapy Management (MTM) among patients with diabetes, hypertension, or dyslipidemia. Healthcare. 2022;10(7):1207. doi:10.3390/healthcare10071207
15. Stewart D, Whittlesea C, Dhital R, Newbould L, McCambridge J. Community pharmacist led medication reviews in the UK: a scoping review of the medicines use review and the new medicine service literatures. Res Social Adm Pharm. 2020;16(2):111–122. doi:10.1016/j.sapharm.2019.04.010
16. Latif A, Pollock K, Boardman HF. The contribution of the medicines use review (MUR) consultation to counseling practice in community pharmacies. Patient Educ Couns. 2011;83(3):336–344. doi:10.1016/j.pec.2011.05.007
17. Boyd M, Waring J, Barber N, et al. Protocol for the New Medicine Service Study: a randomized controlled trial and economic evaluation with qualitative appraisal comparing the effectiveness and cost effectiveness of the New Medicine Service in community pharmacies in England. Trials. 2013;14(1):411. doi:10.1186/1745-6215-14-411
18. Latif A. Community pharmacy medicines use review: current challenges. Integr Pharm Res Pract. 2018;7:83–92. doi:10.2147/iprp.S148765
19. Rendrayani F, Alfian SD, Wahyudin W, Puspitasari IM. Pharmacists’ knowledge, attitude, and practice of Medication Therapy Management: a systematic review. Healthcare. 2022;10(12):2513. doi:10.3390/healthcare10122513
20. Qudah B, Thakur T, Chewning B. Factors influencing patient participation in medication counseling at the community pharmacy: a systematic review. Res Social Adm Pharm. 2021;17(11):1863–1876. doi:10.1016/j.sapharm.2021.03.005
21. Brundisini F, Vanstone M, Hulan D, DeJean D, Giacomini M. Type 2 diabetes patients’ and providers’ differing perspectives on medication nonadherence: a qualitative meta-synthesis. BMC Health Serv Res. 2015;15:516. doi:10.1186/s12913-015-1174-8
22. McMullen CK, Safford MM, Bosworth HB, et al. Patient-centered priorities for improving medication management and adherence. Patient Educ Couns. 2015;98(1):102–110. doi:10.1016/j.pec.2014.09.015
23. Conn VS, Ruppar TM, Maithe Enriquez RN, Cooper PS. Patient-centered outcomes of medication adherence interventions: systematic review and meta-analysis. Value Health. 2016;19(2):277–285. doi:10.1016/j.jval.2015.12.001
24. Kuntz JL, Safford MM, Singh JA, et al. Patient-centered interventions to improve medication management and adherence: a qualitative review of research findings. Patient Educ Couns. 2014;97(3):310–326. doi:10.1016/j.pec.2014.08.021
25. Ruud KW, Rønningen SW, Faksvåg PK, Ariansen H, Hovland R. Evaluation of a structured pharmacist-led inhalation technique assessment service for patients with asthma and COPD in Norwegian pharmacies. Patient Educ Couns. 2018;101(10):1828–1837. doi:10.1016/j.pec.2018.05.018
26. Hovland R, Bremer S, Frigaard C, et al. Effect of a pharmacist-led intervention on adherence among patients with a first-time prescription for a cardiovascular medicine: a randomized controlled trial in Norwegian pharmacies. Int J Pharm Pract. 2020;28(4):337–345. doi:10.1111/ijpp.12598
27. Plattner H. An Introduction to Design Thinking Process Guide. 2010. Available from: https://web.stanford.edu/~mshanks/MichaelShanks/files/509554.pdf.
28. Altman M, Huang TTK, Breland JY. Design Thinking in Health Care. Prev Chronic Dis. 2018;15:E117. doi:10.5888/pcd15.180128
29. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
30. Braun V, Clarke V. Thematic Analysis: A Practical Guide. 2021.
31. Braun V, Clarke V. Conceptual and design thinking for thematic analysis. Qual Psychol. 2022;9(1):3–26. doi:10.1037/qup0000196
32. Giroldi E, Veldhuijzen W, Leijten C, et al. ‘No need to worry’: an exploration of general practitioners’ reassuring strategies. BMC Fam Pract. 2014;15(1):133. doi:10.1186/1471-2296-15-133
33. Akyirem S, Salifu Y, Bayuo J, Duodu PA, Bossman IF, Abboah-Offei M. An integrative review of the use of the concept of reassurance in clinical practice. Nurs Open. 2022;9(3):1515–1535. doi:10.1002/nop2.1102
34. Cross AJ, Elliott RA, Petrie K, Kuruvilla L, George J. Interventions for improving medication-taking ability and adherence in older adults prescribed multiple medications. Cochrane Database Syst Rev. 2020;5:CD012419. doi:10.1002/14651858.CD012419.pub2
35. Dang BN, Westbrook RA, Njue SM, Giordano TP. Building trust and rapport early in the new doctor-patient relationship: a longitudinal qualitative study. BMC Med Educ. 2017;17(1):32. doi:10.1186/s12909-017-0868-5
36. Pincus T, Holt N, Vogel S, et al. Cognitive and affective reassurance and patient outcomes in primary care: a systematic review. Pain. 2013;154(11):2407–2416. doi:10.1016/j.pain.2013.07.019
37. Jubraj B, Barnett NL, Grimes L, Varia S, Chater A, Auyeung V. Why we should understand the patient experience: clinical empathy and medicines optimisation. Int J Pharm Pract. 2016;24(5):367–370. doi:10.1111/ijpp.12268
38. Sarkis DJ, Lucchetti G, Mattos Martins MDC, et al. Effectiveness of different strategies to teach empathy among medical students: a randomized controlled study. Patient Educ Couns. 2025;130:108468. doi:10.1016/j.pec.2024.108468
39. Riess H, Kelley JM, Bailey RW, Dunn EJ, Phillips M. Empathy training for resident physicians: a randomized controlled trial of a neuroscience-informed curriculum. J Gen Intern Med. 2012;27(10):1280–1286. doi:10.1007/s11606-012-2063-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.