Back to Journals » International Journal of General Medicine » Volume 19
Patient Educational Needs and Communication Barriers in Dermatology Clinics in Saudi Arabia: A Cross-Sectional Survey
Authors Alshammarie FF, Alhobera A ![]() , Alshammari M
, Alshammari M
Received 12 February 2026
Accepted for publication 14 May 2026
Published 19 May 2026 Volume 2026:19 603039
DOI https://doi.org/10.2147/IJGM.S603039
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Fawwaz Freih Alshammarie,1 Aala Alhobera,2 Maryam Alshammari3
1Dermatology Department, University of Hail, Ministry of Education, Hail, Saudi Arabia; 2Pediatric Dermatology Division of Medical Pediatrics Department, Maternity and Children Hospital, Ministry of Health, Hail, 55432, Saudi Arabia; 3Family Medicine Department, Hail Health Cluster, Ministry of Health, Hail, Saudi Arabia
Correspondence: Aala Alhobera, Pediatric Dermatology Division of Medical Pediatrics Department, Maternity and Children Hospital, Ministry of Health, Hail, 55432, Saudi Arabia, Email [email protected]
Purpose: Understanding patient perspectives is essential to improving quality and satisfaction of care in dermatology clinics. In Saudi Arabia, limited national data exist on patients’ educational needs and communication barriers. This study aimed to assess patient satisfaction, identify educational gaps, and explore communication challenges in dermatology clinics across Saudi Arabia.
Patients and Methods: A national cross-sectional survey was conducted among 976 dermatology patients. A structured questionnaire evaluated demographics, perceived knowledge, satisfaction with information provided, communication barriers, and preferred educational methods. Descriptive statistics and chi-square tests were used for analysis.
Results: Among participants who had attended dermatology clinics (n = 795), 61.6% reported frequent or occasional confusion about their condition, and only 45.4% demonstrated high self-reported knowledge. Overall satisfaction was moderate, with 58.3% satisfied or very satisfied, while 9.9% reported dissatisfaction. The most reported communication barriers were limited consultation time (25.2%) and patient anxiety about asking questions (15.3%). Patients felt least informed about treatment options (22.6%), diagnosis (20.3%), and potential side effects (19.3%). Most participants (70.6%) preferred language communication to be in Arabic, and 78% favored face-to-face education consultation. Patient knowledge, barriers and preferences significantly differed with age, gender, and condition complexity (p < 0.05).
Conclusion: Dermatology patients in Saudi Arabia report moderate satisfaction with substantial educational needs and communication barriers. Addressing consultation time constraints, fostering supportive communication environments, and providing patient-centered, language-appropriate education; particularly through face-to-face interactions will aid to enhance understanding, satisfaction, and engagement in for overall better provider-patient dermatologic care.
Keywords: healthcare communication, health literacy, patient-centered care, consultation time, knowledge gaps, Healthcare communication, cross-sectional survey, Saudi Arabia
Introduction
Patient education is an essential component of dermatologic care and plays a critical role in improving treatment adherence, patient satisfaction, and clinical outcomes. In this study, patient education refers to the process of providing patients with clear, relevant, and understandable information regarding their condition, treatment options, and self-care, with the aim of improving understanding, adherence, and health outcomes.1 Effective education by healthcare providers enables patients to understand their conditions, apply treatments correctly, and engage in self-management behaviors that support long-term disease control. Evidence from chronic dermatologic conditions, including atopic dermatitis, demonstrates that structured educational interventions improve patient comprehension, engagement, and adherence to medical recommendations.2 Despite these benefits, many dermatology patients report gaps in the clarity, accessibility, or adequacy of the information they receive in clinical settings.3
Variability in the delivery of patient education is influenced by consultation time constraints, diverse patient learning preferences, and differences in health literacy. Studies highlight that many standard patient education materials are not fully adapted to patient needs, and personalization, such as tailoring communication to language, preferred format, and cultural context, enhances satisfaction and understanding.4–6 Patients’ preferred methods for receiving information often vary; while digital resources are increasingly available, face-to-face interactions remain the most valued approach, providing reassurance, clarity, and opportunities for questions.6–8 Health literacy levels in Saudi Arabia vary, with evidence suggesting that a considerable proportion of the population has limited health literacy, which may affect patients’ ability to understand medical information and follow treatment recommendations.9
Patient comprehension is also shaped by individual and condition-related factors, including age, gender, prior confusion, and the complexity of the skin condition. For example, confusion or anxiety can negatively affect understanding, whereas patients with less complex conditions often demonstrate higher knowledge.2,6,7 Additionally, patients frequently seek supplemental information outside clinical encounters, commonly via the internet, underscoring the importance of providing reliable, clinic-based educational resources to prevent misinformation.8
In the Kingdom of Saudi Arabia, dermatology services are delivered through both public and private healthcare sectors. Public services are typically accessed through primary care referrals, while private clinics allow more direct access to specialists. This structure may influence consultation time, continuity of care, and the delivery of patient education.10 Despite this, only limited research has explored dermatology patient education from the patients’ perspective.
This study is conceptually guided by principles of the Patient-Centered Care model, which emphasizes effective communication, patient engagement, and shared decision-making as core elements of quality healthcare11 The present cross-sectional survey aims to provide an overview of patient education in dermatology clinics in Saudi Arabia, examining formats, content, perceived adequacy, and preferred educational methods. By identifying unmet needs, the study seeks to inform strategies that enhance understanding, satisfaction, and patient involvement in dermatologic care.
Material and Methods
Study Design and Participants
A cross-sectional survey was conducted across various regions of Saudi Arabia using a convenience sampling approach. The sample size was calculated using a standard formula for cross-sectional studies, assuming a 50% prevalence, 95% confidence level, and 5% margin of error, yielding a minimum required sample of 384 participants. To enhance representativeness, a larger sample was targeted. A total of 976 participants were included in the final analysis. Eligible participants were Saudi adults, aged 18 years and above, of both female and male gender, with a history of at least one prior visit to a dermatology clinic. Participants who were non-Saudi, younger than 18 years, or had no prior history of dermatology clinic visits were excluded from the analysis.
Survey Method and Data
Data were collected using a structured, anonymous questionnaire designed to obtain both quantitative and qualitative information. The questionnaire was developed by the research team based on a review of relevant literature to ensure coverage of key aspects of patient education and communication in dermatology settings. The questionnaire was pilot tested on 20 participants to assess clarity and comprehension of both the Arabic and English versions, and a retest was conducted after two weeks on the same group to evaluate response consistency. The questionnaire included demographic variables such as age, gender, educational level, and region of residence. Clinical-related information included history and frequency of dermatology clinic visits and the type of skin condition followed. It also assessed provider-patient communication, patient educational needs, perceived knowledge gaps, barriers to understanding, and preferred methods to improve comprehension. The full questionnaire is provided in Supplementary Figure 1.
Period and Data Collection
Data collection was carried out over a two-month period, from 1 January to 28 February 2025. Participants were recruited by data collectors encompassing of medical students and interns through online and in-person channels. Online recruitment was conducted via widely used social media platforms, including WhatsApp, Instagram, and X, through dissemination of the survey link. In addition, participants were recruited in public locations such as malls, parks, and university campuses. Participation was voluntary and anonymous. No personally identifiable information was collected, ensuring full confidentiality of responses.
Statistical Analysis
Data were analyzed using Statistical Package for Social Studies for Windows, Version 26 (SPSS; Released 2019; IBM Corp., Armonk, NY, USA). Descriptive statistics, including frequencies and percentages, were employed to summarize the demographic and clinical characteristics of the study population. Categorical variables were analyzed using the Chi-square test to evaluate associations and identify statistically significant relationships between variables. When the expected cell count was <5 in 20% or more of the cells, Fisher’s exact test was applied to ensure the accuracy of the results. Statistical significance was determined at a p-value threshold of <0.05.
Results
Demographic and Clinical Characteristics
Table 1 presents the demographic and clinical characteristics of the study participants. A total of 976 individuals were included, with females representing the majority at 786 (80.5%) and males accounting for 190 (19.5%). The largest age group was 20–30 years, comprising 445 participants (45.6%), followed by 151 participants between 40–50 years (15.5%), 137 participants were 18 to less than 20 years (14.0%), 134 participants between 30–40 years (13.7%), 85 participants between 50–60 years (8.7%), and those aged 60 years and above representing about 24 (2.5%). Regarding education, 582 participants held a bachelor’s degree (59.6%), while high school education was reported by 275 (28.2%), 56 participants held a master’s degree (5.7%), 44 participants reported secondary education (4.5%), and primary education was reported by 19 (1.9%). Geographically, participants were predominantly from the northern region 495 (50.7%), followed by the western region 185 (19.0%), middle region 178 (18.2%), eastern region 96 (9.8%), and southern region 22 (2.3%). Most participants had previously visited a dermatology clinic 795 (81.5%), while 181 (18.5%) had not and were therefore excluded from the study. Among those who had visited a clinic, with 318 (40.0%) reporting only one visit, 232 (29.2%) visiting once a year, 157 (19.7%) visiting 2–3 times a year, and 88 (11.1%) visiting more than three times annually. Regarding skin conditions, acne was the most common 427 (53.2%), followed by eczema 184 (22.9%), skin infections 63 (7.9%), rosacea 47 (5.9%), warts 33 (4.1%), psoriasis 18 (2.2%), and other conditions 30 (3.7%), with multiple responses allowed.
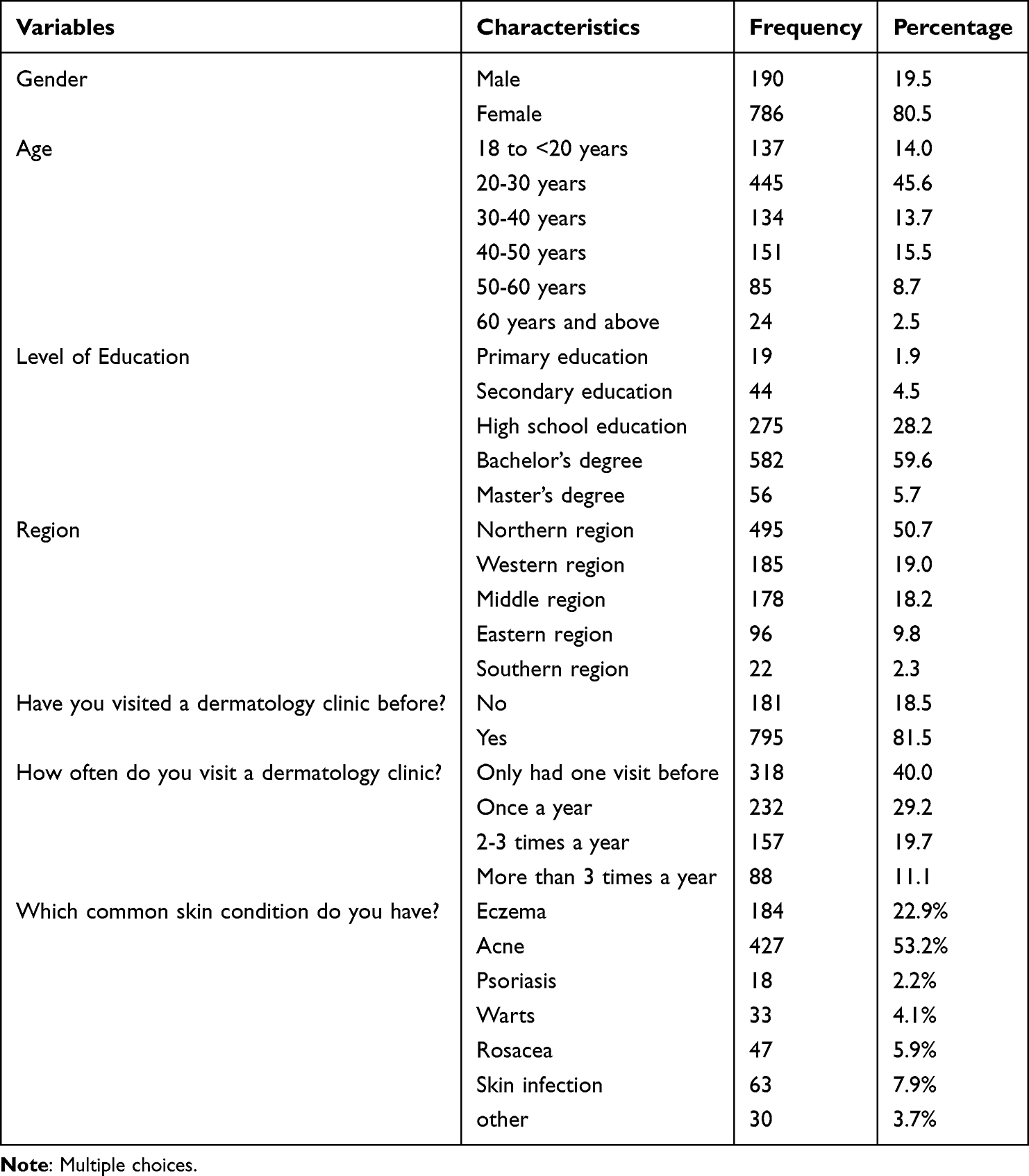 |
Table 1 Demographic and Clinical Characteristics |
Patients’ Knowledge Gaps Regarding Their Skin Conditions
Table 2 depicts an overview of patients’ knowledge gaps regarding their skin conditions. Among participants ((N = 795), 133 (16.7%) of respondents reported often being confused or misunderstanding information about their skin condition, 357 (44.9%) experienced some confusion, 170 (21.4%) rarely felt confused, and 135 (17.0%) never felt confused. When asked how much general knowledge they felt they had about their condition at the current time, 161 (20.3%) reported low knowledge, 273 (34.3%) reported moderate knowledge, and 361 (45.4%) reported high knowledge. Regarding the complexity of the dermatology skin condition role in understanding their condition, 443 (55.7%) believed their understanding was not affected, 122 (15.3%) thought complexity affected their understanding, and 230 (28.9%) were neutral regarding this aspect. When asked if they were satisfied with the information provided by their dermatologist, 152 (19.1%) were very satisfied, 312 (39.2%) were satisfied, 252 (31.7%) were neutral, 56 (7.0%) were not satisfied, and 23 (2.9%) were not satisfied at all. Patients shared many barriers that impeded their understanding at their clinic visit including: not having enough time with their provider at 313 (25.2%) of patients, feeling anxious or scared to ask their questions at 190 (15.3%) of patients, thinking the provider was too busy at 121 (9.8%) of patients, caregivers at the visit could not communicate in the same language as doctor at 59 (4.8%) of patients, having medical terminology that was impossible to understand at 66 (5.3%), other barriers at 52 (4.2%) of patients, and finally, 439 (35.4%) of patients did not have barriers. Regarding medical aspects about which patients felt least informed, 248 (20.3%) indicated diagnosis, 80 (6.6%) causes and risk factors, 276 (22.6%) treatment options, 159 (13.0%) medication usage, 200 (16.4%) prevention and lifestyle measures, 235 (19.3%) potential side effects or complications, and only 22 (1.8%) felt fully informed.
 |
Table 2 Patients’ Knowledge Gaps Regarding Their Skin Conditions |
Patients’ Preferences for Receiving Information
Table 3 presents an overview of patients’ preferences for receiving information about their skin conditions. The majority of participants (70.6%) preferred to communicate with their provider in Arabic as they understood it better, while 5.7% preferred English since most information online and names of skin conditions are in English, and 23.8% expressed no preference for either language. When asked if they had ever sought information outside of their clinic visits because they felt confused or that the information provided was not enough, most respondents (72.2%) reported doing so, whereas 27.8% had not. Among those who sought additional information, online sources such as social media and websites were the most common (57.1%), followed by advice from family and friends (25.6%), support groups either in person or online (10.8%), and books or pamphlets (6.4%).
 |
Table 3 Patients’ Preferences for Receiving Information About Their Skin Conditions |
Figure 1 presents participants’ preferred methods of receiving information about their skin condition, face-to-face consultations were overwhelmingly favored as the first choice by 620 participants (78%), with smaller proportions selecting it as their second 84 (10.6%), third 45 (5.7%), or fourth choice 24 (3%), and only 11 participants (1.4%) ranking it fifth or sixth. Digital written sources, such as websites and Twitter, were chosen as the first preference by 202 participants (25.4%) and were most commonly selected as the second choice 245 (30.8%). Video platforms like YouTube and TikTok were preferred as the first choice by 220 respondents (27.7%), followed closely by group sessions, chosen as the first choice by 141 participants (17.7%) but more frequently ranked in the fourth to sixth positions. Printed materials were less frequently selected as the first choice 99 (12.5%) but gained higher preference in the second and third positions (181; 22.8% and 169; 21.3%, respectively). Finally, other methods were selected as the first choice by 192 participants (24.2%), though the majority favored them as a sixth choice 268 (33.7%). Overall, face-to-face consultations clearly dominated participants’ preferences, while digital, video, and group-based methods showed more varied rankings across the sample.
 |
Figure 1 Preferred Methods of Receiving Information (N = 795). |
Table 4 presents an overview of patients’ perceptions regarding factors that improve understanding of their skin condition and their engagement with educational resources. Among participants (N = 795), step-by-step guides for managing their condition were considered the most helpful by 795 (35.0%), followed by closure summaries provided by the doctor at the end of the visit by 264 (11.6%), visual aids in the clinic such as 3D skin models or diagrams by 231 (10.2%), more time spent with the dermatologist during each visit by 224 (9.9%), patients’ success stories or case study examples (219, 9.6%), contact information for additional support like nurse hotlines or support groups by 203 (8.9%), research updates and new treatment options by 182 (8.0%), and availability of a patient educator to provide further explanations and support by 153 (6.7%). Regarding whether participants felt their dermatologist took enough time to answer questions and explain their condition, 257 (32.3%) reported “yes, always,” 297 (37.4%) stated “yes, most times,” and 241 (30.3%) reported “sometimes.” When asked about how often they would like updates about their skin condition, 406 (51.1%) preferred updates at every visit, 93 (11.7%) once a month, 86 (10.8%) every three months, 170 (21.4%) only when there were significant changes, and 40 (5.0%) did not care to be informed. Regarding participation in educational workshops or webinars hosted by the clinic to help other patients and improve awareness, 342 (43.0%) expressed interest, 275 (34.6%) were unsure, and 178 (22.4%) were not interested. Finally, when asked if they would be willing to provide feedback on educational materials to improve them, 501 (63.0%) answered yes, while 294 (37.0%) declined.
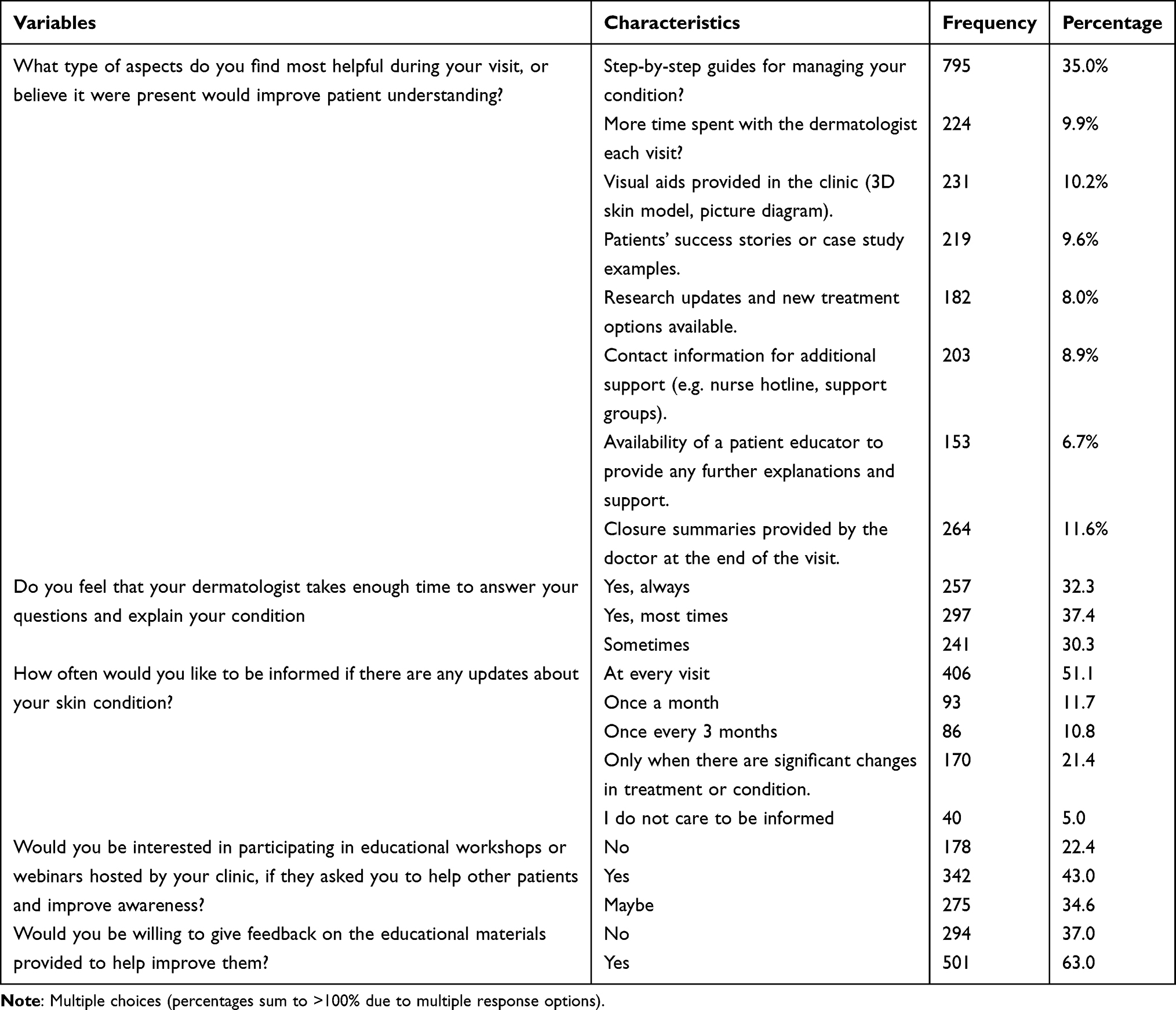 |
Table 4 Patients’ Perceptions Regarding Factors That Improve Understanding of Their Skin Condition |
The results presented in Table 5 illustrate the associations between participants’ characteristics and their knowledge about their skin condition. Male participants were slightly more likely to have high knowledge 72 (49.0%) compared with females 289 (44.6%) (χ2 = 6.446, p = 0.040). Age also showed a significant association, with participants aged 40–50 years demonstrating the highest proportion of high knowledge 75 (57.3%), while those 18 to <20 years had the lowest 42 (43.3%) (χ2 = 19.959, p = 0.030). Although education level appeared related to knowledge, the association was not statistically significant; participants with a master’s degree had the highest proportion of high knowledge 27 (56.3%) compared with those with primary education 8 (44.4%) (χ2 = 7.033, p = 0.533). Regarding misunderstandings about their condition, those who reported rarely and never being confused had markedly greater in high knowledge levels 102 (60.0%) and 97 (71.9%), respectively, compared with participants who often experienced confusion 40 (30.1%) (χ2 = 95.993, p < 0.001). The complexity of the skin condition was strongly associated with knowledge: participants without complex conditions were more likely to have high knowledge 238 (53.7%) than those with complex conditions 29 (23.8%) (χ2 = 70.793, p < 0.001). These findings emphasize that age, gender, prior confusion, and condition complexity significantly influence patients’ understanding of their skin health.
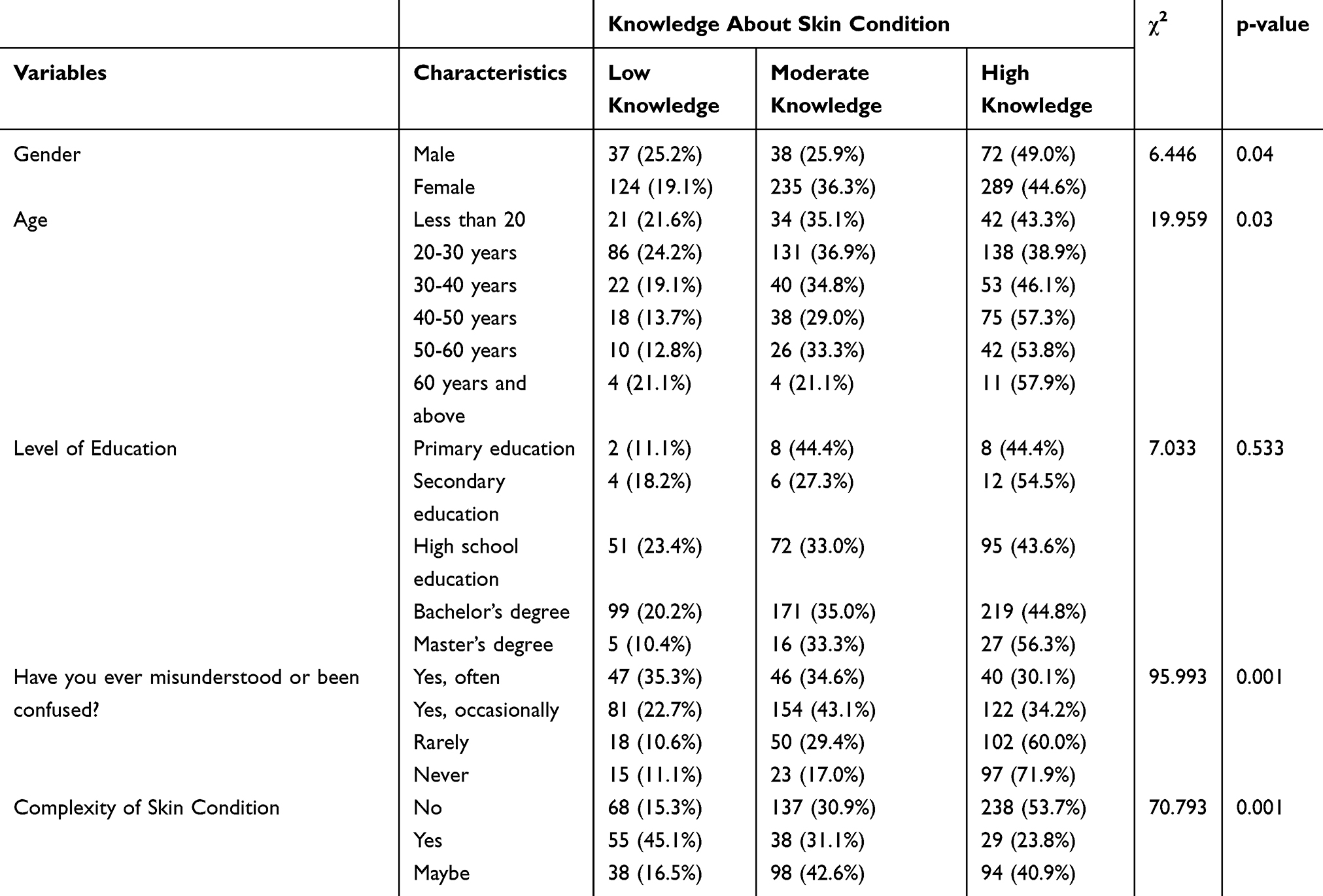 |
Table 5 Associations Between Participants’ Characteristics and Their Knowledge About Their Skin Condition |
Participants were asked what improvements they would suggest to enhance patient education in dermatology clinics. Based on their responses, five key suggestions were identified to improve patient education in dermatology clinics. The first suggestion is to provide ample time for each patient with in-depth explanation of the patient’s condition, treatment options, potential side effects, and preventative care. The second suggestion is to improve communication by using straightforward, unambiguous language, visuals, and interactive resources so patients better understand their diagnosis and clinical care plan. The third suggestion is to provide patients with personalized educational materials at numerous levels, and some follow-up support such as digital resources, virtual consultations, and reminders during support group meetings. The fourth suggestion is to ensure physicians show empathy, active listening, and psychological support to patients, and create a supportive environment for patients to feel they have some agency in asking questions and sharing concerns. The fifth suggestion is to improve accessibility and cost-effectiveness of services for dermatology patients by providing additional appointments, making that care more reasonably available, or even advising on feasible and economical treatments.
Discussion
This study evaluates the importance of patient education in medical settings in the Kingdom of Saudi Arabia by looking from the patients’ perspectives, asking for suggested improvements, and considering the feasibility of measuring education effectiveness. There were evident knowledge gaps between patients and their skin condition. Almost 490 (62%) of participants indicated some confusion about their condition, and less than half 361 (45.4%) identified having high knowledge. Whereas the majority of patients were of the opinion their condition did not complicate understanding their diagnosis, the level of satisfaction with the information received was moderate, with 252 (31.7%) neutral, and only 152 (19.1%) of patients identifying being very satisfied with the education they received. A frequent barrier to understanding the medical education provided was limited time with a medical provider (313 (25.2%)) and anxiety about asking questions (190 (15.3%)). Patients identified feeling least informed about their management options (276 (22.6%)), the diagnosis itself (248 (20.3%)), and possible treatment side-effects (235 (19.3%)). These represent important opportunities where medical education could be improved. Ultimately, study findings suggest that improved patient education strategies and communication with patients will address important knowledge gaps and support improved patient understanding, satisfaction, and involvement in their treatment and management of their skin condition. The findings of this study corroborate previous literature that highlights the significance of patient education in dermatology. A recent study12 reported that barriers to understanding, poor recall, and the physician’s delivery are some of the main barriers to effective patient education, similar to the confusion and moderate satisfaction reported in our study. Another study13 found that, even with regular follow-ups, there were significant knowledge gaps in disease management and treatment misconceptions, reinforcing the need for targeted education. Clearly, the topics in which patients felt least informed included treatment options like the use of micrographic surgery (MoHs), diagnosis, and possible side effects, which are typical areas of deficiencies reported in dermatology populations and requires systematic educational strategies to enhance knowledge, patient satisfaction, and active engagement in self-care. The study results identified patient preference for communication in Arabic (562, 70.6%) and noted that it was common for patients to seek additional information beyond their visits (574, 72.2%) - primarily the internet as a source (454, 57.1%). Additionally, close to 80% (620, 78.0%) of participants indicated that face-to-face encounters was the most preferred way to receive information, while “digitally”, “video”, or “group” orientated methods tended to be more variable in responses. Overall, the findings suggest that in-person interaction continues to be the most valued approach to patient education, despite the existence of alternative information sources. This preference for direct, in-person interactions echoes study,14 which reported that patients valued access to dermatology clinic notes and felt it enhanced understanding and involvement in care. Additionally, a study15 highlighted that while social media can provide curated educational content, it may also spread misinformation, which could explain patients’ reliance on direct consultations despite the availability of online sources. The findings suggest that patient education strategies must balance the convenience of digital resources with the personalized reassurance of face-to-face interactions to maximize comprehension and trust.
The findings indicate that participants’ knowledge about their skin condition is significantly influenced by age, gender, prior confusion, and the complexity of their condition. Males showed slightly higher knowledge than females. The studies13 and16 report the opposite, with females demonstrating significantly higher dermatology knowledge than males.
Moreover, the results show that participants aged 40–50 years had the highest knowledge levels, whereas those 18 to <20 years had the lowest. Importantly, participants who rarely or never experienced confusion about their condition demonstrated substantially higher knowledge compared with those who were often confused. The study17 highlighted that psychological factors, including confusion, anxiety, or psychiatric comorbidities, can negatively affect patient comprehension.
Additionally, individuals with non-complex skin conditions have markedly higher knowledge than those with complex conditions. While education level appeared related to knowledge, this association was not statistically significant. Overall, these results highlight that patient understanding is shaped more by experiential and condition-related factors than formal education. Finally, while the study addresses key factors to improve dermatology patient education, additional studies are required to develop, implement and evaluate approaches that improve patient understanding.
Limitations
This study has several limitations. The use of convenience sampling may introduce selection bias, with an overrepresentation of female participants and individuals from the Northern region, which may limit generalizability. In addition, the reliance on self-reported data introduces the possibility of recall and reporting bias, including social desirability bias. Furthermore, the cross-sectional design limits the ability to establish causal relationships between variables.
Conclusion
The present study highlights the importance of patient education in dermatology within the Kingdom of Saudi Arabia and identifies notable gaps in patients’ understanding of their skin conditions. A considerable proportion of participants reported confusion, and less than half indicated a high level of understanding of their condition. The main factors associated with confusion included limited consultation time and hesitation to ask questions. Participants demonstrated the lowest understanding regarding treatment options, diagnosis, and potential treatment side effects. These findings underscore the need for structured and targeted educational strategies to improve patient knowledge, satisfaction, and engagement in self-management. Face-to-face consultations were the most preferred method for receiving information, highlighting the continued importance of direct patient-physician interaction despite the increasing availability of digital resources. Patient knowledge was also influenced by factors such as age, gender, prior confusion, and condition complexity.
Recommendations
Based on the findings, several practical recommendations can be made. Dermatology clinics should consider allocating additional time for patient consultations, particularly for newly diagnosed patients, to allow adequate explanation of diagnosis, treatment options, and potential side effects. The use of standardized Arabic-language visual educational materials may further enhance patient understanding. In addition, implementing brief structured education points during consultations and providing verified clinic-based or digital educational resources may help reduce reliance on non-medical sources and improve consistency of patient education delivery.
Final Statement
Overall, the study emphasizes that effective patient education in dermatology requires clear communication strategies tailored to individual patient needs and characteristics. Strengthening these approaches can improve patient understanding, enhance satisfaction, and support better long-term disease management and outcomes.
Ethics Approval and Informed Consent
A waived informed consent in written format was obtained from all participants prior to completing an anonymous questionnaire, confirmed by either answering agree to participate or do not agree to participate in the study. The study has been reviewed and approved by the Research Ethics Committee (REC) at University of Hail, College of Medicine. Dated: 02/12/2024 with the reference number of H-2024-507. The study complied with ethical standards outlined in the Declaration of Helsinki.
Acknowledgment
This paper has been uploaded to Medrxiv, the preprint server for health science as a preprint: https://www.medrxiv.org/content/10.64898/2026.03.11.26348118v1.full.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Regional Office for Europe. Therapeutic patient education: continuing education programmes for health care providers in the field of prevention of chronic diseases: report of a WHO working group. World Health Organization. Regional Office for Europe; 1998. Available from: https://iris.who.int/handle/10665/108151.
2. Wilken B, Zaman M, Asai Y. Patient education in atopic dermatitis: a scoping review. Allergy Asthma Clin Immunol. 2023;19(89). doi:10.1186/s13223-023-00844-w
3. Martínez-García E, Affleck A, Rakvit P, Arias-Santiago S, Buendía-Eisman A. Exploring patients’ insight, concerns, and expectations at dermatology clinic: an observational study in 2 centers in Scotland and Spain. J Patient Experience. 2020;7(6):1197–11. doi:10.1177/2374373520912085
4. Prabhu AV, Gupta R, Kim C, et al. Patient education materials in dermatology: addressing the health literacy needs of patients. JAMA Dermatol. 2016;152(8):946–947. doi:10.1001/jamadermatol.2016.1135
5. Alagheband SJ, Miller JJ, Clarke JT. Individualizing patient education for greater patient satisfaction. Cutis. 2015;95(5):291–292. PMID: 26057507.
6. AlHilali SM, AlMuammar AM, AlKahtani E, Khandekar R, AlJasser AA. Preferred method of education among patients in ophthalmic care in Saudi Arabia. Middle East Afr J Ophthalmol. 2016;23(2):168–171. PMID: 27162447; PMCID: PMC4845613. doi:10.4103/0974-9233.171780
7. Tak H, Ruhnke GW, Shih YC. The association between patient-centered attributes of care and patient satisfaction. Patient. 2015;8(2):187–197. PMID: 25011683. doi:10.1007/s40271-014-0073-0
8. Orgaz-Molina J, Cotugno M, Girón-Prieto MS, et al. A study of Internet searches for medical information in dermatology patients: the patient-physician relationship. Actas Dermosifiliogr. 2015;106(6):493–499. [English, Spanish]. PMID: 25805250. doi:10.1016/j.ad.2015.01.011
9. Almubark R, Basyouni M, Alghanem A, et al. Health literacy in Saudi Arabia: implications for public health and healthcare access. Pharmacol Res Perspect. 2019;7(4):e00514. PMID: 31397117; PMCID: PMC6687660. doi:10.1002/prp2.514
10. Almalki M, Fitzgerald G, Clark M. Health care system in Saudi Arabia: an overview. East Mediterr Health J. 2011;17(10):784–793. PMID: 22256414. doi:10.26719/2011.17.10.784
11. Epstein RM, Street RL. The values and value of patient-centered care. Ann Fam Med. 2011;9(2):100–103. PMID: 21403134; PMCID: PMC3056855. doi:10.1370/afm.1239
12. Zirwas MJ, Holder JL. Patient education strategies in dermatology: part 1: benefits and challenges. J Clin Aesthetic Dermatol. 2009;2(12):24–27. PMID: 20725581; PMCID: PMC2923943.
13. AlOrbani AM, El-Komy MHM, Mourad A, Amer MA. Psoriasis knowledge gaps and misconceptions in the Middle East and North Africa (MENA) regions: patients’ survey-based study. Int J Dermatol. 2024;63(12):1748–1754. doi:10.1111/ijd.17255
14. Yang K, Lau CB, Lau WC, Nambudiri VE, Watson AJ. Patient perspectives on clinic note transparency within dermatology. JAMA Dermatol. 2023;159(4):456–458. doi:10.1001/jamadermatol.2023.0086
15. Wojtara MS. Use of social media for patient education in dermatology: narrative review. JMIR Dermatol. 2023;6:e42609. doi:10.2196/42609
16. Sampogna F, Samela T, Abeni D, et al. A cross-sectional study on gender differences in body dysmorphic concerns in patients with skin conditions in relation to sociodemographic, clinical and psychological variables. J Eur Acad Dermatol Venereol. 2025;39(4):823–832. doi:10.1111/jdv.20247
17. Kelly KA, Balogh EA, Kaplan SG, Feldman SR. Skin disease in children: effects on quality of life, stigmatization, bullying, and suicide risk in pediatric acne, atopic dermatitis, and psoriasis patients. Children. 2021;8(11):1057. doi:10.3390/children8111057
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.