Back to Journals » Drug Design, Development and Therapy » Volume 20
Patient-Controlled Sedation with Remimazolam Enables More Precise Intraoperative Sedation in Elderly Patients Under Spinal Anesthesia: A Randomized Controlled Trial
Authors Wang M, Wang T, Wu N, Zhang Y ![]() , Jia J, Zhao S
, Jia J, Zhao S ![]() , Yan J
, Yan J ![]() , Wang A
, Wang A ![]() , Yuan D
, Yuan D
Received 12 October 2025
Accepted for publication 15 January 2026
Published 24 January 2026 Volume 2026:20 573714
DOI https://doi.org/10.2147/DDDT.S573714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Yan Zhu
Mei Wang,1,2 Tianqi Wang,1 Nan Wu,2 Yutao Zhang,3,4 Jindi Jia,1 Shengguo Zhao,1,2 Jie Yan,1,2 Airong Wang,1 Dajiang Yuan1,5
1College of Anesthesiology, Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 2Department of Anesthesiology, Second Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 3College of Second Clinical Medical, Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 4Department of Orthopedics, Second Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 5Department of the Party Committee, Shanxi Cardiovascular Hospital, Taiyuan, Shanxi, People’s Republic of China
Correspondence: Dajiang Yuan, Department of the Party Committee, Shanxi Cardiovascular Hospital, Taiyuan, Shanxi, People’s Republic of China, Tel +86-186-3617-1219, Email [email protected]
Purpose: To investigate whether patient-controlled sedation (PCS) with remimazolam provides more precise sedation control and superior overall outcomes compared to conventional sedation (CS) in elderly patients undergoing lower limb surgery under spinal anesthesia.
Patients and Methods: 120 patients aged ≥ 65 years (ASA physical status II~III) were randomized to receive either PCS (n=60) or CS (n=60). PCS received a loading dose (1 mg), background infusion (0.75 mg·h− 1), and patient-demand boluses (0.5 mg; lockout interval 60s). CS received a loading dose (0.05~0.1 mg·kg− 1) followed by a continuous infusion (0.1~0.3 mg·kg− 1·h− 1). The primary outcome was the proportion of patients who maintained optimal sedation, defined as a Ramsay Sedation Scale score of 3~4 with supportive bispectral index (BIS) monitoring. Secondary outcomes included onset/recovery time, hemodynamics, drug consumption, adverse events, and satisfaction.
Results: The proportion maintaining optimal sedation was higher in the PCS group (100% vs 88.3%, P < 0.05). PCS also showed lower total drug use, shorter recovery time (both P < 0.001), and higher scores for comfort, satisfaction, and cooperation (all P < 0.05). Hemodynamic stability was better in the PCS group, with higher mean arterial pressure at T2 through T6 timepoints (mean difference 4.5 mmHg, P = 0.019) and a lower hypotension incidence (10.0% vs 23.3%, P = 0.050).
Conclusion: For elderly patients undergoing lower limb surgery under spinal anesthesia, patient-controlled sedation with remimazolam facilitates more precise sedation control. It ensures a higher proportion of optimal sedation depth while reducing drug consumption, accelerating recovery, and enhancing patient comfort and satisfaction. Under the conditions of this study, this approach constitutes a safe, effective, and individualized sedation strategy.
Keywords: remimazolam, patient-controlled sedation, elderly, spinal anesthesia
Corrigendum for this paper has been published.
Introduction
The global demographic shift toward an aging population has resulted in a rising number of elderly patients undergoing surgical interventions, particularly lower limb procedures such as joint replacements Spinal anesthesia is often the technique of choice for these operations, owing to its effective analgesia and favorable safety profile. However, intraoperative awareness can provoke anxiety and stress, potentially leading to detrimental hemodynamic instability and increased perioperative morbidity—especially in older adults with diminished physiological reserve.1–4 Consequently, adjunct sedation is frequently administered to improve patient comfort and mitigate such stress reactions.5,6
However, safe and effective sedation in the elderly poses distinct clinical challenges. With advancing age, physiological changes such as reduced baroreflex sensitivity, decreased vascular compliance, and diminished hepatic and renal function heighten susceptibility to hemodynamic depression and prolong sedative clearance. Conventional sedation (CS) strategies therefore increase the risk of hypotension and drug accumulation. An approach that achieves more stable plasma drug concentrations and avoids peak-effect fluctuations may offer important hemodynamic safety advantages in this vulnerable population.
An ideal sedative for geriatric patients should exhibit rapid onset, quick recovery, minimal cardiorespiratory depression, and a predictable dose-response relationship. Remimazolam, a novel ultra-short-acting benzodiazepine,7 fulfills many of these requirements. It acts on GABA-A receptors to induce sedation and is rapidly metabolized by tissue esterases into an inactive metabolite, resulting in a short context-sensitive half-life and reduced potential for accumulation.8 These pharmacokinetic characteristics render it particularly suitable for elderly patients. CS typically delivered via clinician-titrated continuous infusion, remains widely used.1,9 However, significant interindividual variability in pharmacodynamics and pharmacokinetics among older adults often complicates drug titration with CS, frequently leading to episodes of undersedation or oversedation.3 The latter is associated with considerable risks, including respiratory depression and hypotension.
Patient-controlled sedation (PCS) offers an innovative alternative that addresses some limitations of CS by enabling patients to self-administer bolus doses within predefined safety limits. This approach promotes autonomy and may allow more precise titration of sedation according to individual needs, potentially reducing total drug consumption and enhancing patient satisfaction.10 Although PCS has been studied with other sedatives such as propofol and dexmedetomidine.10–12 Each of these alternatives carries distinct limitations. Propofol-based PCS is prone to dose-dependent respiratory and circulatory depression, while dexmedetomidine-based PCS often causes bradycardia. In contrast, remimazolam — characterized by its ultra-short-acting metabolism and minimal cardiorespiratory depression — offers a theoretical advantage in circumventing these drawbacks, potentially providing a safer and more controllable pharmacological basis for PCS. The use of PCS with remimazolam remains underexplored. Importantly, robust evidence from randomized controlled trials (RCTs) evaluating the efficacy and safety of remimazolam-based PCS in the vulnerable elderly population under spinal anesthesia is currently scarce.13,14
To address this gap, we conducted a prospective, single-blinded, randomized controlled trial. We hypothesized that for elderly patients undergoing lower limb surgery under spinal anesthesia, remimazolam PCS would be non-inferior to CS in sedation quality and, owing to its patient-controlled nature, would demonstrate superiority in sedation precision, hemodynamic stability, recovery speed, and patient experience. This study was designed to test this hypothesis, with the aim of providing an evidence-based option for personalized sedation in the elderly.
Materials and Methods
Study Design and Ethics
This prospective, randomized controlled trial was conducted at a single center. The study protocol was approved by the Institutional Ethics Committee of the Second Hospital of Shanxi Medical University (Approval No. [2025]YX-080; registered on April 16, 2025) and was registered prior to patient enrollment at https://www.chictr.org.cn (ChiCTR2500102809; registered on May 20, 2025). Written informed consent was obtained from all participants or their legal guardians before any study-related procedures were performed.
The study protocol underwent several refinements after its registration, as outlined below:
Primary outcome: The primary outcome was modified from “drug-related parameters (eg, onset time, total dose, recovery time)” to “the proportion of patients maintaining optimal sedation (Ramsay score 3~4) during surgery”. This change was informed by preliminary data and literature review, which suggested that this composite endpoint more accurately captures the clinical objective of precise sedation control and aligns better with a patient-centered approach.
Sample size: The sample size was recalculated based on the revised primary outcome. Using a two-sided test with 80% power and α = 0.05, 56 patients per group were required. To account for an estimated 10% dropout rate, 126 patients (63 per group) were planned. Ultimately, 123 patients were randomized, and 120 completed the study.
Intervention parameter: The bolus dose for patient-controlled sedation (PCS) was adjusted from 0.25 mg (0.5 mL) to 0.5 mg (1 mL). This adjustment was based on preliminary observations that the original dose sometimes required multiple presses to achieve adequate comfort, which could increase patient anxiety. The modification aimed to enhance titration efficiency and patient experience while preserving a safe lockout interval.
All protocol changes were implemented before the start of the main trial. The study was completed earlier than the conservatively projected timeline in the trial registry, reflecting efficient recruitment and execution without any alterations to the study design.
Patient Population
A total of 126 patients scheduled for elective lower limb surgery under spinal anesthesia between June and August 2025 were assessed for eligibility. Inclusion criteria were: age ≥65 years, American Society of Anesthesiologists (ASA) physical status II or III, and body mass index (BMI) between 18.5 and 27.9 kg·m−2. Exclusion criteria included: psychiatric disorders or cognitive impairment, inability to operate the PCS device, known allergy to remimazolam, severe cardiac, pulmonary, hepatic, or renal dysfunction, chronic use of sedatives or antidepressants, contraindications to neuraxial anesthesia, anticipated difficult airway, and refusal by the patient or their legal guardian to participate in the study. Patients were excluded after randomization if they experienced inadequate spinal anesthesia, required conversion to general anesthesia, or if sedation was discontinued due to adverse events.
Randomization and Blinding
Eligible patients were randomly allocated in a 1:1 ratio to either the PCS group or the CS group using a computer-generated random number sequence. To ensure allocation concealment, each assignment was sealed in an opaque envelope. The envelopes were prepared and kept by independent staff and were opened only after the patient had given written informed consent and entered the operating room. The nature of the intervention precluded blinding of patients, surgeons, and anesthesiologists. Nevertheless, blinding was maintained for the research personnel who collected data and assessed outcomes.
Anesthesia and Sedation Protocol
All patients fasted from solid food for 8 hours and from clear fluids for 2 hours preoperatively. Frailty status was assessed using the FRAIL scale,15 a screening tool consisting of five items: fatigue, resistance (ability to climb one flight of stairs), ambulation (ability to walk one block), illnesses (the presence of ≥5 chronic diseases), and loss of weight (unintentional weight loss). Each item was scored as 1 point for a “yes” response and 0 points for a “no” response. Based on the total score (range 0~5), patients were categorized into three groups: robust (score 0), pre-frail (score 1~2), and frail (score 3~5). Patients received preoperative instruction on using the handheld button. Upon arrival in the operating room, standard monitoring was established, including electrocardiography, non-invasive blood pressure, pulse oximetry, and bispectral index (BIS). Spinal anesthesia was performed at the L3~L4 interspace using 20 mg of ropivacaine hydrochloride (100 mg/10 mL, Qilu Pharmaceutical Co., Ltd., Batch No.: 4C0033C71). Surgery began after achieving a sensory block level reaching approximately T10. Sedation was induced using a 0.5 mg/mL solution of remimazolam besylate (25 mg, Yichang Humanwell Pharmaceutical Co., Ltd., Batch No.: AC5030061). PCS Group: Patients used an electronic infusion pump configured with a bolus dose of 2 mL (equivalent to 1 mg), a background infusion of 1.5 mL/h (equivalent to 0.75 mg·h−1), a rescue bolus of 1 mL (equivalent to 0.5 mg), and a lockout interval of 60 seconds (the minimum time interval allowed between two consecutive effective patient-controlled bolus doses). CS Group: Patients received a loading dose of 0.05–0.1 mg·kg−1 remimazolam over 1 minute, followed by a continuous infusion at 0.1–0.3 mg·kg−1·h−1. “Adequate sedation (sedation onset time)” was defined as the initial point at which a Ramsay Sedation Score of 3–4 coincided with a BIS value below 85. In both groups, sedation was maintained until skin closure. Standardized interventions were defined for hypotension, bradycardia, and hypoxia.
Data Collection and Outcomes
The primary outcome was the proportion of patients who maintained optimal sedation intraoperatively.
Secondary outcomes included the time to sedation onset, recovery time (defined as the interval from discontinuation of sedative infusion to achieving a Ramsay score of 1–2), total dosage of remimazolam consumed, incidence of adverse events, and patient satisfaction scores. For the PCS group, the number of demand attempts and successful deliveries were also recorded. Additionally, we analyzed continuous hemodynamic variables, including mean arterial pressure (MAP), heart rate (HR), and SpO2—as well as sedation variables (BIS and Ramsay score) were documented at baseline (T0), at 5 (T1), 10 (T2), 15 (T3), 30 (T4), and 60 (T5) minutes after sedation initiation, at the end of surgery (T6), and 10 minutes postoperatively (T7).
The depth of sedation was assessed using the Ramsay Sedation Scale,16 which employs the following criteria: a score of 1 indicates an anxious and restless state; 2 signifies a cooperative and tranquil state; 3 reflects responsiveness only to commands; 4 corresponds to a brisk response to a light glabellar tap or a loud auditory stimulus; 5 indicates a sluggish response to such stimuli; and 6 denotes no response. During surgery, the maintenance of a Ramsay score between 3 and 4 was defined as “optimal sedation”.
Sample Size Calculation
The sample size was calculated based on the primary outcome of optimal sedation maintenance. Preliminary data from a pilot study (n=26), which was not included in the formal analysis, showed that 100% (13/13) of the PCS group and 84.6% (11/13) of the CS group maintained optimal sedation. For a conservative estimate in the main trial, the anticipated success rates were set at 99% for PCS and 84.6% for CS. Using a two-sample, two-sided equality test in PASS software (Power Analysis and Sample Size, 2020) with 80% power and a two-sided alpha of 0.05, a minimum of 56 patients per group was required. Accounting for a 10% dropout rate, 126 patients (63 per group) were enrolled.
Statistical Analysis
Data were analyzed using SPSS 30.0 (IBM Corp., Armonk, NY, USA) and GraphPad Prism 10.1.2 (GraphPad Software, San Diego, CA, USA). Normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation (SD) and compared using independent samples t-tests. Repeated-measures analysis of variance (ANOVA) was used to analyze within-group changes over time; Mauchly’s test was applied for sphericity, with Greenhouse-Geisser correction used when needed. Non-normal data were summarized as median (interquartile range) and compared using the Mann–Whitney U-test. Categorical variables were expressed as numbers (percentages) and analyzed with the chi-square or Fisher’s exact test, as appropriate. A two-tailed P-value < 0.05 was considered statistically significant.
Result
Study Population
Among the 126 initially randomized patients, 120 completed the study per protocol and were included in the final analysis. Six patients were excluded: three from the PCS group (one due to an inadequate block and two lost to follow-up) and three from the CS group (one due to conversion to general anesthesia, one due to sedation abandonment, and one lost to follow-up). Consequently, data from 60 patients in each group were analyzed (Figure 1).
 |
Figure 1 Consolidated standards of reporting trials diagram. |
Baseline Patient Characteristics
Patient demographics and clinical characteristics are summarized in Table 1. The mean age was 73.08 ± 2.54 years in the PCS group and 72.73 ± 3.02 years in the CS group (P = 0.493). No statistically significant differences were observed between the two groups regarding gender, height, weight, BMI, ASA status, surgical type, frailty score, anesthesia duration, and surgery duration (all P > 0.05) (Table 1).
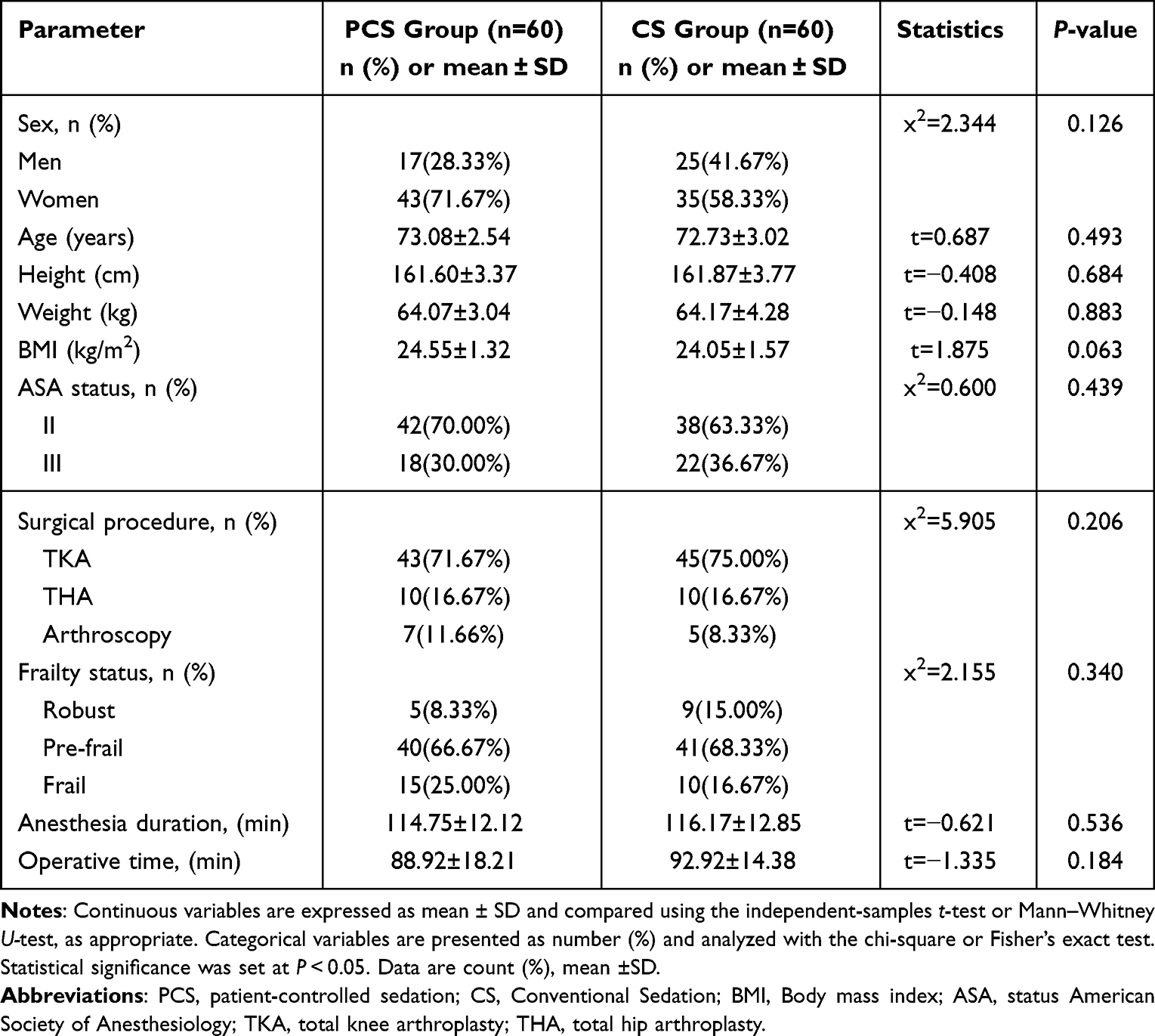 |
Table 1 Patient Demographics and Clinical Characteristics |
Sedation-Related Outcomes
A significantly higher proportion of patients in the PCS group maintained optimal intraoperative sedation compared to the CS group (100% [60/60] vs 88.3% [53/60]; P < 0.05). In the CS group, failure to achieve the target sedation depth was attributed to undersedation in 3 patients and oversedation in 4. Significant differences were observed in the time to sedation onset and recovery between the two groups. The sedation onset time was 9.37 ± 1.39 minutes in the PCS group vs 4.31 ± 1.09 minutes in the CS group (P < 0.001). In contrast, recovery time was significantly shorter in the PCS group (8.28 ± 2.33 minutes) than in the CS group (12.31 ± 1.91 minutes; P < 0.001) (Figure 2).
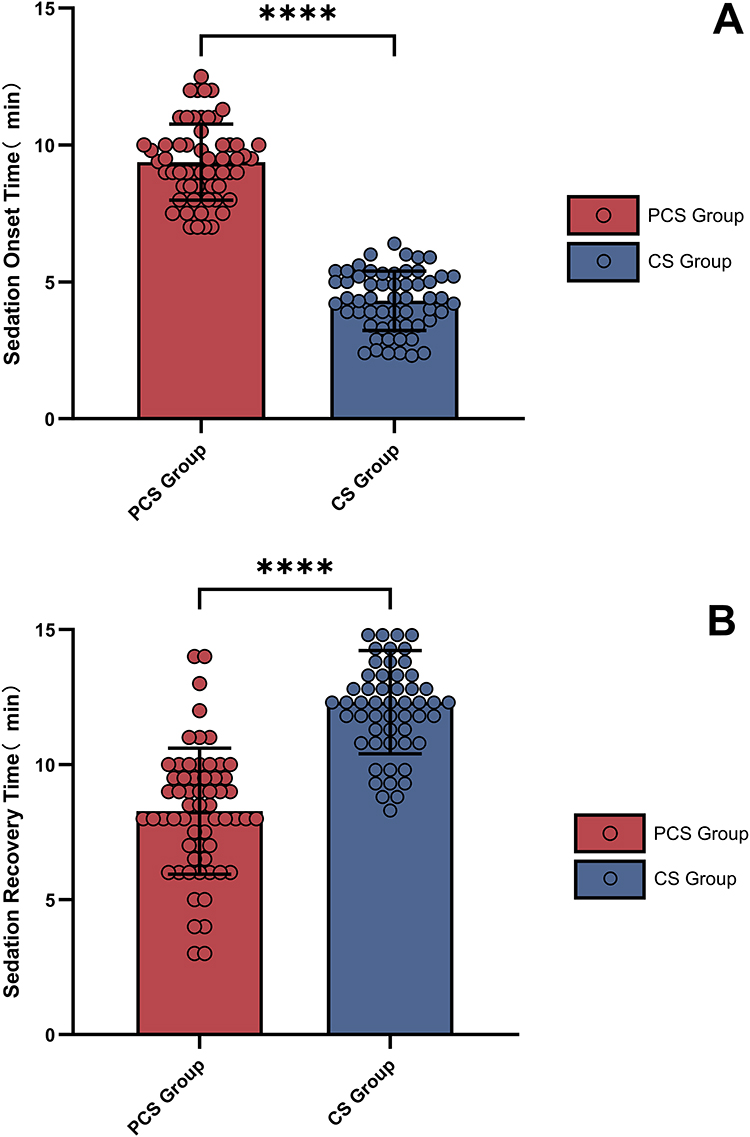 |
Figure 2 (A) Time to sedation onset of remimazolam patient-controlled sedation and conventional sedation. (B) Time to sedation recovery with remimazolam patient-controlled sedation and conventional sedation. Error bars represent standard deviation (SD). ****P < 0.0001 relative to CS Group (n = 60). |
In the PCS group, remimazolam use resulted 11~88 demand attempts (mean ± SD: 25.07 ± 12.74), with 8~20 effective deliveries (12.75 ± 2.94). The total self-administered dose was 10.8~23.7 mL (16.37 ± 3.16 mL) (Figure 3). The sedation onset dose ranged from 2.2 to 6.9 mL (4.64 ± 1.16 mL), achieved within 7.0~12.5 minutes (9.37 ± 1.39 minutes). The number of demands, effective deliveries, and cumulative dosage all showed a time-dependent increase during the procedure. In contrast, the CS group received a total remimazolam dose ranging from 16.0 to 36.8 mL (26.67 ± 3.94 mL), with a sedation onset dose of 5.3 to 12.8 mL (8.41 ± 1.54 mL).
 |
Figure 3 Cumulative demand and dosage of remimazolam in the patient-controlled sedation (PCS) group over time. (A) Cumulative total and valid demands (mean ± SD). (B) Cumulative drug dose (mean ± SD). Measurements were taken at time points T0 to T7. The timeline is divided into two clinical phases: an initial high-demand phase (T0 to T3) and a subsequent stable maintenance-to-recovery phase (T3 to T7). Note: Time points are not equidistant; therefore, the slopes of the lines do not represent actual rates of change. Error bars represent standard deviation (SD). |
Relevant Vital Signs During Sedation
Sedation parameters and vital signs during the procedure are summarized in Figures 3 and 4. Key parameters — including mean arterial pressure (MAP), heart rate (HR), bispectral index (BIS),17 peripheral oxygen saturation (SpO2), Ramsay sedation score — were rigorously monitored in both groups throughout the sedation period.
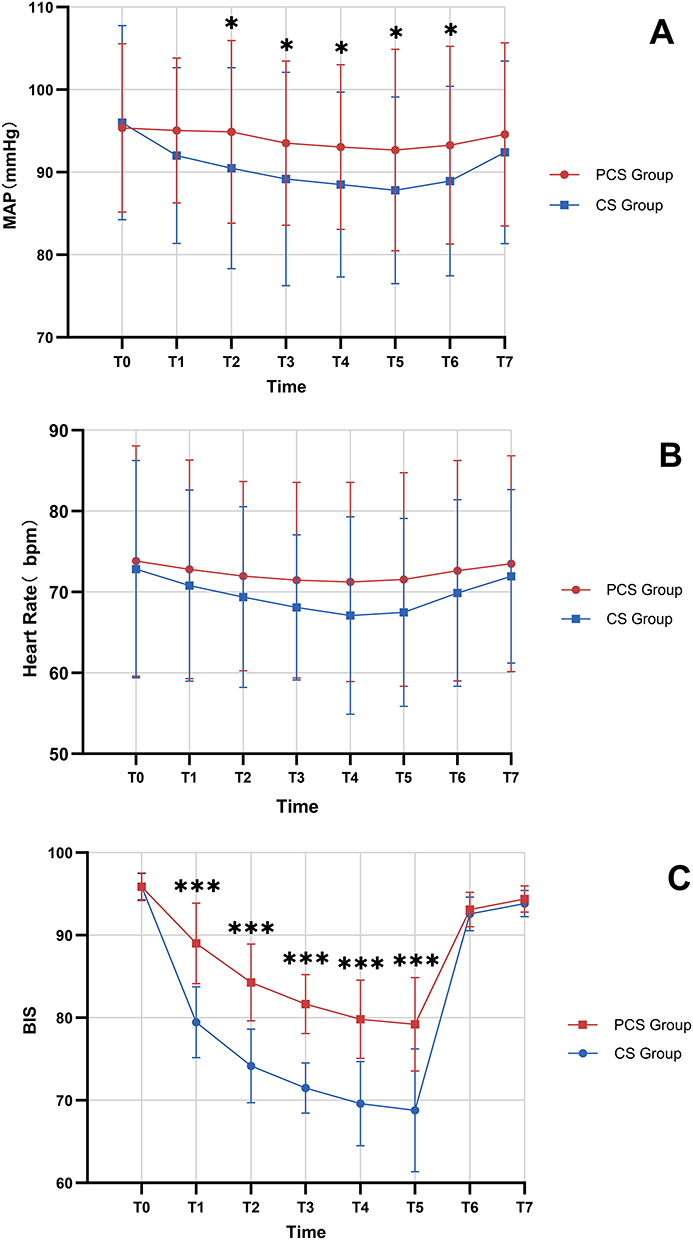 |
Figure 4 Comparison of hemodynamic parameters and sedation depth between patient-controlled and conventional sedation groups over time. (A) Mean arterial pressure (MAP). (B) Heart rate (HR). (C) Bispectral index (BIS) values. Measurements were recorded at predefined time points (T0 to T7). Error bars represent standard deviation (SD). ***P < 0.001, *P < 0.05 relative to CS Group (n = 60). |
No significant differences in HR or SpO2 were detected between the two groups across the eight time points. Statistically significant differences in MAP were observed from T2 to T6, while significant differences in BIS values were noted from T1 to T5. The lowest intraoperative BIS values were 69 in the PCS group and 57 in the CS group (P < 0.001) (Figure 4).
Both groups exhibited gradual increases in Ramsay scores following remimazolam administration, with values returning to near-baseline levels within 10 minutes postoperatively. Before sedation, Ramsay scores of 1 were recorded in 41 patients in the PCS group and 39 patients in the CS group. After drug administration, the number of patients with Ramsay scores of 3~4 at time points T1 through T6 was as follows: in the PCS group —12, 55, 60, 60, 60, and 57; in the CS group — 52, 56, 57, 57, 57, and 53. No patient in either group exhibited a Ramsay score >5 (Figure 5).
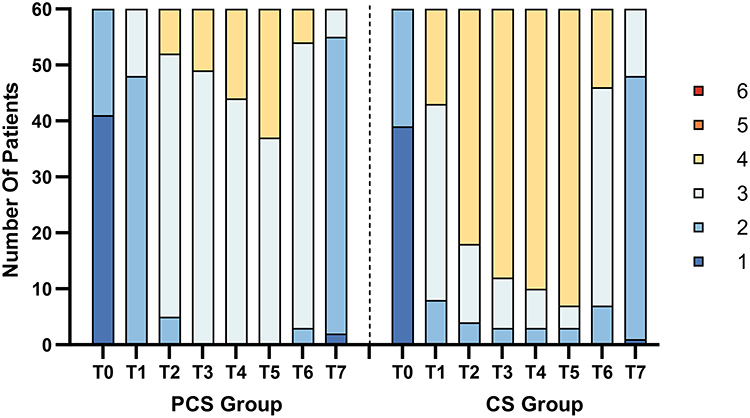 |
Figure 5 Temporal distribution of Ramsay sedation scores comparing remimazolam patient-controlled sedation (PCS) with conventional sedation. The stacked bar chart depicts the proportion of patients at each sedation level (1~6) for all measured time points. |
Adverse Events and Satisfaction with Sedation
The incidence of intraoperative adverse events is summarized in Table 2. Hypotension occurred in 6 patients (10.0%) in the PCS group and 14 (23.3%) in the CS group (P > 0.05); it was managed with ephedrine (6~10 mg) in 2 patients in the PCS group and 8 in the CS group. Hypoxemia (SpO2 < 90%) was observed in 14 patients (23.3%) in the PCS group and 20 (33.3%) in the CS group (P > 0.05). These cases were resolved by increasing the inspired oxygen concentration (14 in PCS group, 19 in CS group) or by jaw-thrust maneuver (1 in CS group). Bradycardia occurred in 1 patient (1.7%) in the PCS group and 3 (5.0%) in the CS group (P > 0.05); one patient in the CS group was treated with atropine (0.5 mg). No significant differences were observed in the overall incidence of intraoperative adverse events between the two groups (P > 0.05). One patient (1.7%) in the CS group developed postoperative delirium within 2 hours. No significant differences were found between the groups in the incidence of postoperative nausea and vomiting, dizziness, headache, somnolence, or delirium within 2 hours after surgery (P > 0.05) (Table 2).
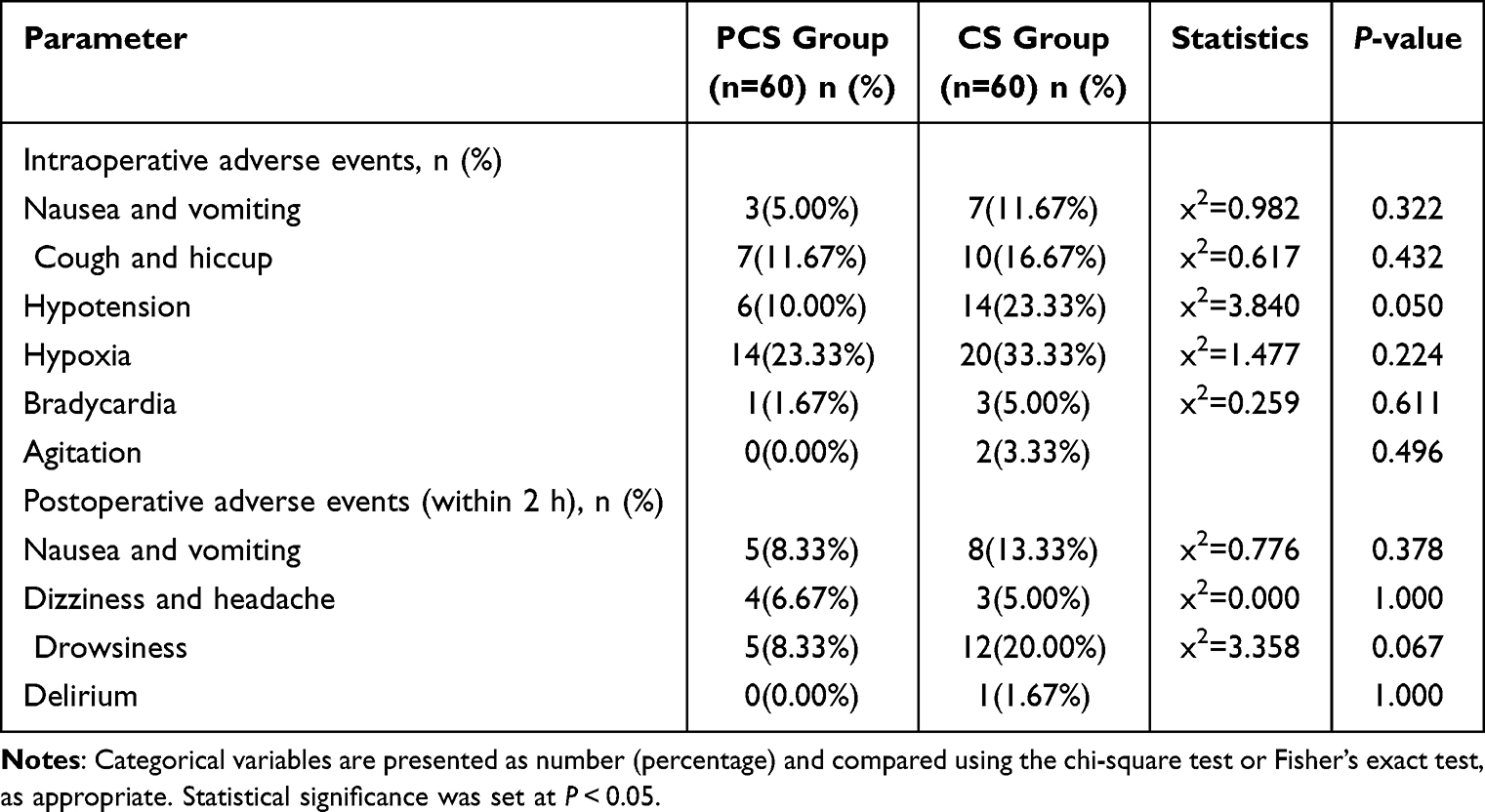 |
Table 2 Perioperative Adverse Events |
Patients in the PCS group reported significantly higher scores for comfort, satisfaction, and cooperation compared to those in the CS group (P < 0.05). Although more patients in the PCS group indicated willingness to choose the same anesthetic method again (50 [83.3%] vs 44 [73.3%] in the CS group), the difference was not statistically significant (P > 0.05). Regarding sedation depth, all 60 patients (100%) in the PCS group achieved adequate sedation (BIS = 65–85). In the CS group, 53 patients (88.3%) were adequately sedated, while 3 (5.0%) had inadequate sedation (BIS > 85) and 4 (6.7%) experienced over-sedation (BIS < 65). These BIS classification criteria for sedation depth are based on the Expert consensus on neurophysiologic monitoring and evaluation of neurocritical care patients (2024 version).18 The difference in sedation adequacy between the two groups was statistically significant (P < 0.05) (Table 3).
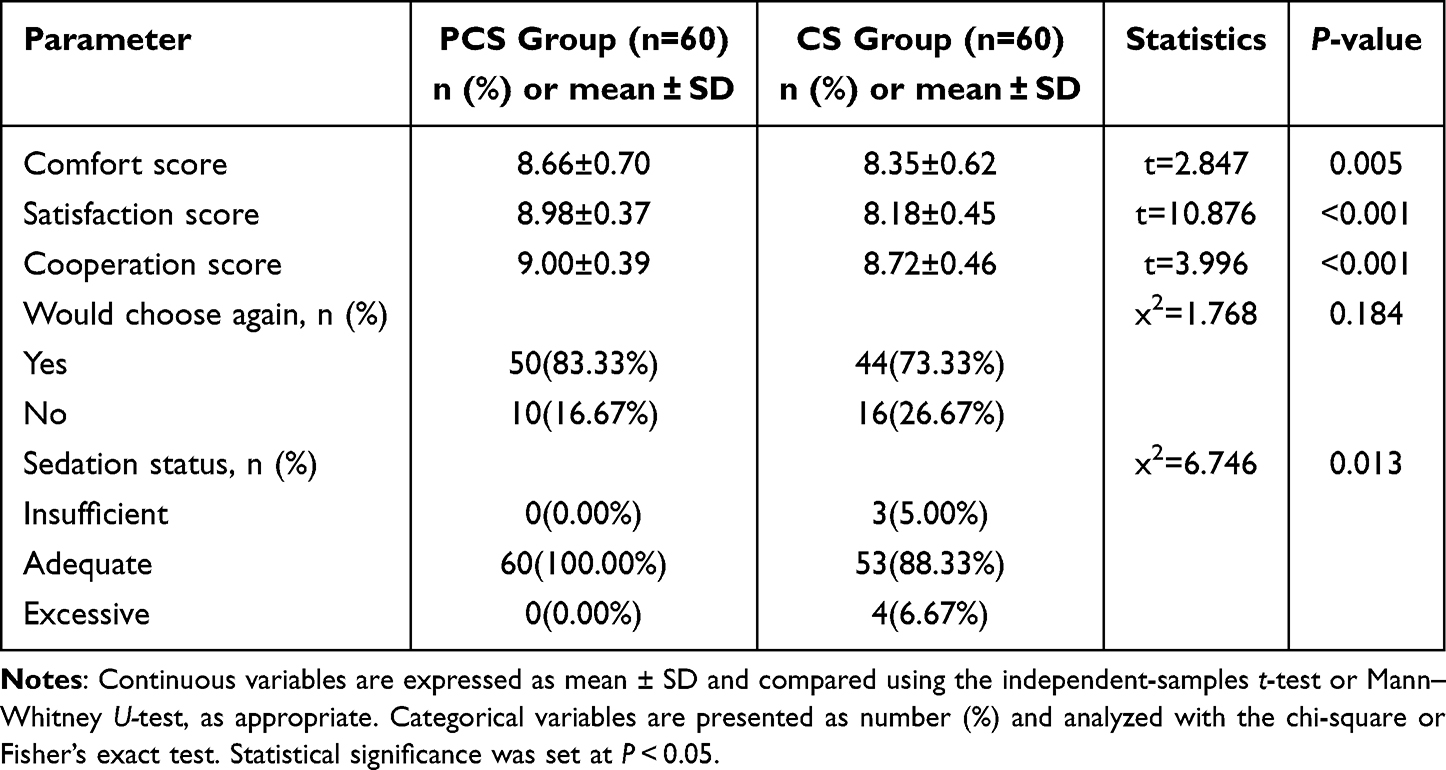 |
Table 3 Evaluation of Sedative Effect |
Discussion
Our results demonstrate that remimazolam PCS enables more precise titration of sedation than CS in elderly patients undergoing lower limb surgery under spinal anesthesia. This superior control is directly evidenced by a perfect rate of optimal intraoperative sedation in the PCS group (100%), significantly higher than the 88.3% observed with CS. This enhanced precision underpins its broader clinical benefits, including greater hemodynamic stability, reduced total drug dosage, and higher patient satisfaction.
The longer sedation onset time observed in the PCS group is an intentional safety feature of the protocol rather than a limitation. The lockout interval, by design, prevents rapid bolus administration and promotes gradual titration, leading to a 39% reduction in total remimazolam consumption compared to the CS group. This lower cumulative dose, together with remimazolam’s favorable pharmacokinetics — characterized by rapid hydrolysis via tissue esterases into an inactive metabolite and a small steady-state volume of distribution —19 was responsible for the significantly shorter recovery time in the PCS group (8.28 ± 2.33 min vs 12.31 ± 1.91 min). This rapid offset is particularly beneficial in geriatric patients, enabling earlier neurological assessment and ambulation, which may shorten PACU stay and align well with Enhanced Recovery After Surgery (ERAS) principles.
This study identified superior hemodynamic stability as a key advantage of remimazolam PCS, evidenced by a clinically significant reduction in the incidence of hypotension compared to CS (10.0% vs 23.3%). This benefit stems from fundamental differences in dosing kinetics between the two regimens. The CS approach, which typically begins with a weight-based bolus, can lead to a rapid peak in plasma drug concentration. This peak may induce a pronounced sympatholytic effect, resulting in a sharp decline in systemic vascular resistance and consequent hypotension. In contrast, the PCS protocol — featuring a low background infusion supplemented by small, patient-titrated boluses — promotes more gradual drug accumulation. This fractionated dosing strategy helps buffer against acute hemodynamic swings, offering a critical safety advantage for elderly patients, who often exhibit reduced cardiovascular reserve and impaired baroreflex compensation.
Notably, the absolute incidence of hypotension in our trial was somewhat higher than that reported in some previous studies.20–23 This discrepancy may be explained by several factors, including patient population characteristics and a deeper exploration of underlying mechanisms. Our cohort included a high proportion of females and pre-frail individuals — groups known to exhibit greater susceptibility to hypotension due to lower baroreflex sensitivity24 and diminished physiological reserve, respectively. Furthermore, beyond its recognized sympathetic inhibitory effect, remimazolam may promote vasodilation through additional pathways. Emerging evidence suggests it could activate G-protein-coupled receptors (GPCRs), potentially increasing intracellular calcium concentration in vascular endothelial cells via the inositol 1,4,5-trisphosphate (IP3) signaling pathway, thereby facilitating vasodilation.25 Age-related pharmacokinetic changes, such as reduced plasma protein binding and smaller volume of distribution, may also lead to higher concentrations of unbound drug, amplifying its hemodynamic impact. Within this context, the fact that the PCS strategy still significantly reduced hypotension risk strongly underscores its protective utility in managing vulnerable geriatric patients.
Our findings further demonstrate the superior ability of remimazolam PCS to accommodate wide inter-individual variability in sedation requirements, enabling more precise control over sedation depth. Although the PCS group exhibited higher BIS values during maintenance, a greater proportion of these patients were consistently maintained within the target Ramsay score range (3~4), with 100% achieving adequate sedation compared to 88.3% in the CS group. This dissociation indicates that effective anxiolysis and patient comfort can be achieved at a lighter hypnotic level — a state closer to the ideal of “cooperative sedation”. This outcome arises from the inherent self-titrating nature of PCS, which establishes a natural feedback loop to maintain sedation within a safer therapeutic window. In contrast, clinician-controlled infusion tends to favor deeper sedation to ensure patient immobility. It should be noted that the dose–response relationship of remimazolam on BIS is less pronounced than that of propofol.4,26 Therefore, our study appropriately used a combination of BIS and Ramsay scores to comprehensively assess sedation depth, although the correlation between the two was not explicitly analyzed. The ability of PCS to reduce the risk of oversedation likely contributed to the lower requirement for airway interventions in this group, further affirming the favorable respiratory safety profile of remimazolam PCS. The respiratory safety profile observed in this study further supports this advantage. Although respiratory depression was not a predefined primary endpoint, the incidence of intraoperative hypoxemia (SpO2 < 90%) was lower in the PCS group (23.3%) than in the CS group (33.3%). All such episodes resolved promptly with simple interventions, such as increasing oxygen delivery, without progressing to severe respiratory depression requiring advanced airway management. Clinically, these findings indicate that remimazolam-based PCS maintains an acceptable and manageable respiratory status in elderly patients.
The comparative profile of remimazolam against other PCS sedatives is of significant clinical importance. While propofol poses a considerable risk of dose-dependent cardiorespiratory depression11,12,27 and dexmedetomidine is frequently linked to bradycardia and prolonged sedation,10,22 remimazolam exhibits a more favorable safety profile. Its key attributes include minimal cardiorespiratory effects and rapid, predictable pharmacokinetics—notably a faster onset and offset than dexmedetomidine.9,28,29 These properties, culminating in a wider therapeutic window and enhanced hemodynamic stability, establish remimazolam-based PCS as a potentially superior and particularly appropriate choice for elderly patients with comorbidities undergoing neuraxial anesthesia. Therefore, by employing remimazolam for PCS in this study, we capitalized on its favorable hemodynamic profile compared with propofol and dexmedetomidine, thereby achieving a higher safety margin in elderly patients.
The significantly higher scores for comfort, satisfaction, and cooperation in the PCS group underscore the critical role of patient autonomy in enhancing the perioperative experience. Granting patients control over their sedation likely reduces anxiety and fosters a more positive subjective experience.
The favorable safety profile of remimazolam was further supported by the absence of serious adverse events in both groups during surgery and the initial 2-hour postoperative period, consistent with previous reports.20,28 Notably, no patient in either group required reversal with flumazenil, affirming the drug’s high therapeutic index. However, our results also indicate that higher doses may be associated with an increased risk of adverse events,30,31 highlighting the inherent safety advantage of the PCS modality, which intrinsically limits total drug exposure.
This study has several limitations. First, due to the nature of the intervention (PCS vs CS), blinding of patients and anesthesia providers was not feasible, which may theoretically introduce performance or detection bias. To mitigate this limitation, outcome assessors were blinded to group allocation, and the study relied primarily on objective measures — including BIS values, hemodynamic parameters, and total drug consumption — as key endpoints. Patient-reported outcomes were also collected using standardized scales to minimize subjective bias. Second, the single-center design and specific patient population may restrict the generalizability of our findings; thus, validation through larger, multi-center trials is warranted. Third, we did not conduct subgroup analysis according to preoperative frailty status, which might have offered valuable insights for personalized dosing in this vulnerable subgroup. Future studies should focus on developing such stratified models. Fourth, the follow-up was limited to the early postoperative period; therefore, longer-term neurocognitive outcomes and patient-reported experiences were not assessed. Future studies should incorporate extended follow-up periods and standardized assessment tools to validate these findings. Furthermore, the generalizability of our conclusions to broader populations (such as in outpatient dental procedures requiring cooperative sedation, or in elderly patients undergoing other surgical types or with higher perioperative risk) remains uncertain and warrants further investigation in prospective trials. Finally, although the PCS parameters used in this study proved effective, they were fixed. Further research is needed to optimize these settings — such as bolus dose and background infusion rate — for specific patient subgroups to refine the sedation protocol.
Conclusion
In conclusion, this study demonstrates that the key advantage of remimazolam patient-controlled sedation is its superior ability to achieve precisely titrated, optimal sedation. This core benefit directly yields significant clinical advantages, including a lower total sedative requirement, faster recovery, and enhanced patient comfort and satisfaction. Building on the positive findings in this specific population, future multicenter trials are warranted to confirm generalizability and evaluate applicability in broader clinical settings. Thus, remimazolam PCS represents a safe, effective, and personalized sedation strategy for elderly patients undergoing spinal anesthesia.
Data Sharing Statement
The datasets for this study are available from the corresponding author (email: [email protected]) upon reasonable request.
Ethical Approval Statement
This study was approved by the Ethics Committee of the Second Hospital of Shanxi Medical University (China; [2025]YX-080; April 2025). Informed consent was obtained from the study participants prior to the commencement of the study.
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff who implemented the intervention and evaluation components of the study.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Kim HJ, Kim H, Park HS, Kim HJ, Ro YJ, Koh WU. Effective remimazolam loading dose for adequate sedation in regional anesthesia. Can J Anesth Can Anesth. 2024;71(6):818–14. doi:10.1007/s12630-024-02698-1
2. Chen Y, Cai Y, Yu G, Zhang X, Hu T, Xue R. Safety and effcacy of remimazolam tosilate for sedation during combined spinal-epidural anesthesia for orthopedic procedures: a randomized controlled trial. BMC Anesthesiol. 2024;24(1):75. doi:10.1186/s12871-024-02451-7
3. Kelliher LJS, Scott M. Modifying the stress response – perioperative considerations and controversies. Anesthesiol Clin. 2022;40(1):23–33. doi:10.1016/j.anclin.2021.11.012
4. Zhao T-Y-M, Chen D, Sun H. Moderate sedation with single-dose remimazolam tosilate in elderly male patients undergoing transurethral resection of the prostate with spinal anesthesia: a prospective, single-arm, single-centre clinical trial. BMC Anesthesiol. 2022;22(1):247. doi:10.1186/s12871-022-01788-1
5. Barry G, Uppal V. Sedation during regional anesthesia: less is more. Can J Anaesth. 2022;69:1453–8. doi:10.1007/s12630-022-02338-6
6. Wang M, Zhao X, Yin P, Bao X, Tang H, Kang X. Profile of remimazolam in anesthesiology: a narrative review of clinical research progress. Drug Des Devel Ther. 2022;16:3431–3444. doi:10.2147/DDDT.S375957
7. Kim KM. Remimazolam: pharmacological characteristics and clinical applications in anesthesiology. Anesth Pain Med. 2022;17(1):1–11. doi:10.17085/apm.21115
8. Hu Q, Liu X, Wen C, Li D, Lei X. Remimazolam: an updated review of a new sedative and anaesthetic. Drug Des Devel Ther. 2022;16:3957–3974. doi:10.2147/DDDT.S384155
9. Hs N, Sh P, Bw K, B S, Hj S. A comparison of the safety and efficacy of remimazolam and dexmedetomidine for sedation in surgical patients under regional anesthesia: a meta-analysis of randomized controlled trials. Med Kaunas Lith. 2025;61(4). doi:10.3390/medicina61040726
10. Rhee SH, Kweon YS, Won DO, Lee SW, Seo KS. Identification of an effective and safe bolus dose and lockout time for patient-controlled sedation (PCS) using dexmedetomidine in dental treatments: a randomized clinical trial. J Dent Anesth Pain Med. 2024;24(1):19. doi:10.17245/jdapm.2024.24.1.19
11. Hewson DW, Worcester F, Sprinks J, et al. Patient-maintained versus anaesthetist-controlled propofol sedation during elective primary lower-limb arthroplasty performed under spinal anaesthesia: a randomised controlled trial. Br J Anaesth. 2022;128(1):186–197. doi:10.1016/j.bja.2021.09.038
12. Kreienbühl L, Elia N, Pfeil-Beun E, Walder B, Tramèr MR. Patient-controlled versus clinician-controlled sedation with propofol: systematic review and meta-analysis with trial sequential analyses. Anesth Analg. 2018;127(4):873–880. doi:10.1213/ANE.0000000000003361
13. Yang WJ, Geng ZL, Chen ZZ. The sedation efficacy of different doses of remimazolam in elderly patients with regional nerve block anaesthesia. Eur J Med Res. 2024;29(1):604. doi:10.1186/s40001-024-02204-9
14. Park KN, Karm MH, Seo KS, Kim HJ, Ryoo SH. Patient-controlled sedation using remimazolam during third molar extraction: a case report. J Dent Anesth Pain Med. 2024;24(1):75. doi:10.17245/jdapm.2024.24.1.75
15. Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. 2012;16(7):601–608. doi:10.1007/s12603-012-0084-2
16. Ramsay MAE, Savege TM, Simpson BRJ, Goodwin R. Controlled sedation with alphaxalone-alphadolone. Br Med J. 1974;2(5920):656–659. doi:10.1136/bmj.2.5920.656
17. Ibrahim AE, Taraday JK, Kharasch ED. Bispectral index monitoring during sedation with sevoflurane, midazolam, and propofol. Anesthesiology. 2001;95(5):1151. doi:10.1097/00000542-200111000-00019
18. Neurophysiological Monitoring Group of the Chinese Medical Doctor Association Neurosurgery Branch, Clinical Neurophysiology Committee of the Chinese Research Hospital Association, Critical Brain Injury Professional Committee of the China Association for Promotion of Health Science and Technology, et al. Expert consensus on neurophysiologic monitoring and evaluation of neurocritical care patients (2024 version). Natl Med J China. 2024;104(23):2113–2122. In Chinese
19. Kim SH, Fechner J. Remimazolam – current knowledge on a new intravenous benzodiazepine anesthetic agent. Korean J Anesthesiol. 2022;75(4):307–315. doi:10.4097/kja.22297
20. Qiao D, Kang JM, Zhang R, et al. The impact of remimazolam sedation during neuraxial anesthesia on perioperative cognitive function in elderly patients: a multicenter randomized controlled study. Front Pharmacol. 2025;16:1504813. doi:10.3389/fphar.2025.1504813
21. Deng CM, Meng ZT, Yang J, et al. Effect of intraoperative remimazolam on postoperative sleep quality in elderly patients after total joint arthroplasty: a randomized control trial. J Anesth. 2023;37(4):511–521. doi:10.1007/s00540-023-03193-5
22. Lee S, Kim M, Kang HY, Choi JH, Kim MK, You AH. Comparison of oxygen reserve index according to the remimazolam or dexmedetomidine for intraoperative sedation under regional anesthesia—A single-blind randomized controlled trial. Front Med. 2023;10:1288243. doi:10.3389/fmed.2023.1288243
23. Lee K, Choi SH, Kim S, Kim HD, Oh H, Kim SH. Comparison of remimazolam and midazolam for preventing intraoperative nausea and vomiting during cesarean section under spinal anesthesia: a randomized controlled trial. Korean J Anesthesiol. 2024;77(6):587–595. doi:10.4097/kja.24311
24. Sex differences in arterial hypertension - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/36136303/.
25. Urabe T, Miyoshi H, Narasaki S, et al. Characterization of intracellular calcium mobilization induced by remimazolam, a newly approved intravenous anesthetic. PLoS One. 2022;17(2):e0263395. doi:10.1371/journal.pone.0263395
26. Yang C, Jiao J, Nie Y, Shao W, Zhang H, Huang S. Comparison of the bispectral indices of patients receiving remimazolam and propofol for general anesthesia: a randomized crossover trial. Anaesth Crit Care Pain Med. 2024;43(3):101377. doi:10.1016/j.accpm.2024.101377
27. Joy PJ, Blanshard HJ. Propofol-remifentanil patient-controlled sedation for endoscopic procedures: a prospective service audit. Can J Anesth Can Anesth. 2023;70(11):1735–1743. doi:10.1007/s12630-023-02593-1
28. Wang D, Liu Z, Zhang W, et al. Comparison of remimazolam versus dexmedetomidine on hemodynamics in older patients under lower extremity orthopedic surgery with spinal anesthesia: a randomized controlled trial. Drug Des Devel Ther. 2025;19:6037–6046. doi:10.2147/DDDT.S504371
29. Hong SW, Park JY, Rhee KY, Kim SH. Comparison emergence of sedation, using dexmedetomidine and remimazolam, in spinal anaesthesia - double blinded randomized controlled trial. Int J Med Sci. 2024;21(8):1552–1558. doi:10.7150/ijms.95736
30. Shi H, Zhang J, Hu Z, et al. The efficacy and safety of remimazolam in painless colonoscopy: a prospective, randomized clinical trial. Front Med. 2024;11:1434767. doi:10.3389/fmed.2024.1434767
31. Chae D, Kim HC, Song Y, Choi YS, Han DW. Pharmacodynamic analysis of intravenous bolus remimazolam for loss of consciousness in patients undergoing general anaesthesia: a randomised, prospective, double-blind study. Br J Anaesth. 2022;129(1):49–57. doi:10.1016/j.bja.2022.02.040
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect-Site Concentration of Remimazolam by Age Groups During Target-Controlled Infusion for Total Intravenous Anesthesia: A Retrospective Comparative Study
Park J, Seo KH, Kwak J, Baek H
Drug Design, Development and Therapy 2024, 18:5149-5159
Published Date: 12 November 2024
Effects of Remimazolam on Intraoperative Frontal Alpha Band Power Spectrum Density and Postoperative Cognitive Function in Older Adults Undergoing Lower Extremity Fractures Surgeries: A Randomized Controlled Trial
Wu H, Tian S, Ma H, Zhou W, Feng S, Meng L, Ou J, Xu F, Zhang Z
Clinical Interventions in Aging 2024, 19:2195-2205
Published Date: 31 December 2024
Comparison of Remimazolam and Sevoflurane on Perioperative Body Temperature Changes in Older Patients Undergoing Transurethral Resection of Prostate or Bladder Tumors Under General Anesthesia: A Randomized Prospective Clinical Trial
Choi J, Park C, Lee KH, Kwak HJ
Clinical Interventions in Aging 2025, 20:1811-1820
Published Date: 25 October 2025