Back to Journals » Journal of Pain Research » Volume 12
Patient-controlled intravenous tramadol versus patient-controlled intravenous hydromorphone for analgesia after secondary cesarean delivery: a randomized controlled trial to compare analgesic, anti-anxiety and anti-depression effects
Authors Duan G, Bao X, Yang G ![]() , Peng J, Wu Z
, Peng J, Wu Z ![]() , Zhao P
, Zhao P ![]() , Zuo Z, Li H
, Zuo Z, Li H ![]()
Received 21 August 2018
Accepted for publication 22 November 2018
Published 18 December 2018 Volume 2019:12 Pages 49—59
DOI https://doi.org/10.2147/JPR.S184782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Guangyou Duan,1,* Xiaohang Bao,1,* Guiying Yang,1 Jing Peng,1 Zhuoxi Wu,1 Peng Zhao,1 Zhiyi Zuo,2 Hong Li1
1Department of Anesthesiology, Xinqiao Hospital, Third Military Medical University, Chongqing 400037, China; 2Department of Anesthesiology, University of Virginia, Charlottesville, VA, USA
*These authors contributed equally to this work
Introduction: This study aimed to compare the postoperative analgesic effects of tramadol and hydromorphone for secondary cesarean delivery (CD) as well as their anti-anxiety and anti-depression properties.
Methods: A total of 106 patients receiving secondary CD under spinal anesthesia were randomly allocated to the tramadol group (n=53) and the hydromorphone group (n=53). Each group received patient-controlled intravenous analgesia using flurbiprofen 4 mg/kg combined with tramadol (4 mg/kg) or hydromorphone (0.04 mg/kg) immediately after the surgery. Postoperative pain numerical rating scale (NRS) for incision and visceral pain, hospital anxiety and depression scale (HADS), early walking time and length of hospital stay were assessed.
Results: Patients in the tramadol and hydromorphone groups exhibited equivalent incision pain NRS at different time points (P>0.05). Visceral pain in the tramadol group was higher than that in the hydromorphone group at postoperative 4 hours (2.9 [1.2] vs 2.3 [1.4], P=0.011) and 8 hours (2.4 [1.1] vs 1.8 [1.1], P=0.028). One week after the surgery, the patients in the tramadol group, as compared to the hydromorphone group, had lower anxiety scores (1.9 [3.5] vs 3.6 [4.1], P=0.033) and depression scores (0.8 [1.3] vs 2.7 [4.1], P=0.023). In addition, early walking time (25.3 [7.0] hours vs 29.3 [9.6] hours, P=0.016) and length of hospital stay (2.9 [0.8] days vs 3.3 [0.8] days, P= 0.008) after the surgery in the tramadol group were less than those in the hydromorphone group.
Conclusion: Postoperative intravenous analgesia with tramadol or hydromorphone for secondary CD provides comparable analgesic effects on incision pain. Tramadol is less effective in controlling visceral pain compared to hydromorphone. However, tramadol can help to alleviate anxiety and depression in the early postpartum period, improve patients’ early mobilization and shorten their hospital stay.
Clinical trial number and registry URL: No: ChiCTR-IIR-17011043; URL: www.chictr.org.cn.
Keywords: anxiety, caesarean section, depression, postoperative pain, tramadol
Introduction
Although numerous measures have been developed, the incidence of inadequate postoperative pain treatment for cesarean delivery (CD) remains high.1,2 With the implementation of new national two-child policy in China, a great proportion of patients are scheduled for secondary CD.3,4 A new clinical challenge for postoperative pain treatment after CD has emerged. It was reported that the proportion of women who received secondary CD has increased from 9.8% in 2012 to 17.7% in 2016.5 Because of severe adhesions induced by previous surgery, it is often inevitable to encounter more operative difficulties.6,7 In addition, previous surgery history may increase the patients’ pain sensitivity for secondary CD8,9 and has been identified as a risk factor for experiencing postoperative inadequate pain treatment.10 Therefore, as secondary CD becomes more common in China, it is important but challenging to provide satisfactory postoperative analgesia.
Patient-controlled intravenous analgesia (PCIA) with opioid analgesics, eg, hydromorphone, is one of the most commonly used methods to treat post-CD pain in China.11–13 Tramadol is an effective and well-tolerated agent for post-cesarean section analgesia14 and may have fewer adverse effects as compared to strong opioids.15,16 Previous studies have demonstrated that tramadol administration via PCIA or intermittent intravenous infusion provides effective postoperative analgesia for patients after CD.17–19 Furthermore, a recent study found that for primiparas following CD, PCIA with tramadol may be an excellent strategy due to less pain at mobilization, higher quality of recovery and earlier lactation than using sufentanil.12 However, the studies exploring tramadol as post-CD analgesic for multipara are limited currently.
In addition, women receiving CD often accompany with symptoms of anxiety and depression,20,21 and these mental symptoms, especially depression, is one of the most common complications for puerpera.22,23 The incidence of peripartum anxiety ranges from 15.8% to 17.1%24 and that of peripartum depression ranges from 13.7% to 15.7%.25,26 Although there was no human clinical evidence, previous animal studies have demonstrated that tramadol could reduce anxiety-related and depression-associated behaviors in rats.27,28 Tramadol has an inhibitory effect on the reuptake of norepinephrine and serotonin, which is the underlying mechanism of commonly used drugs for treatment anxiety and depression.29,30 Therefore, we hypothesized that PCIA with tramadol may provide satisfying analgesic effect as strong opioid analgesics and also provide anti-anxiety and anti-depression effects. This prospective randomized controlled trial aimed to compare the post-operative analgesic, anti-anxiety and anti-depression effects of PCIA with tramadol vs PCIA with hydromorphone in a small population of women having second CD.
Methods
Study design
This study was designed as a 1:1 parallel, randomized, controlled and double-blind study according to the CONSORT guidelines. This study was conducted in accordance with the Declaration of Helsinki. This study was approved by the institutional ethics committee of Xinqiao Hospital, Third Military Medical University, Chongqing, China, on December 24, 2016, and written informed consent was obtained from all participating subjects. The trial was registered prior to patient enrollment at Chinese Clinical Trial Registry (www.chictr.org.cn, ChiCTR-IIR-17011043). No change was made to the study methods after trial commencement. The study was performed at Xinqiao Hospital of Third Military Medical University. The full protocol and all the deidentified participant data can be acquired from the corresponding author HL by request.
Patients
All patients were first screened in the obstetric ward and were recruited according to the inclusion and exclusion criteria 1 day before the surgery. A total of 106 Chinese patients, aged 20–40 years, who previously had CD and were scheduled to receive elective CD this time, were recruited into this study (from April to August 2017; Figure 1). The eligible patients were determined according to the obstetrician’s judge based on patient’s individual condition and patient’s personal willingness. Patients who had an uncomplicated and singleton pregnancy with a transverse incision, a gestational age of 37–40 weeks and the American Society of Anesthesiology physical status I–II were eligible to participate in the study. Exclusion criteria included history of pain disorder, chronic opioid use or substance abuse, history of more than one CD, heavy smoking or alcohol dependence, existence of absolute or relative contraindication to subarachnoid space block anesthesia, psychiatric diseases and incapability of communication.
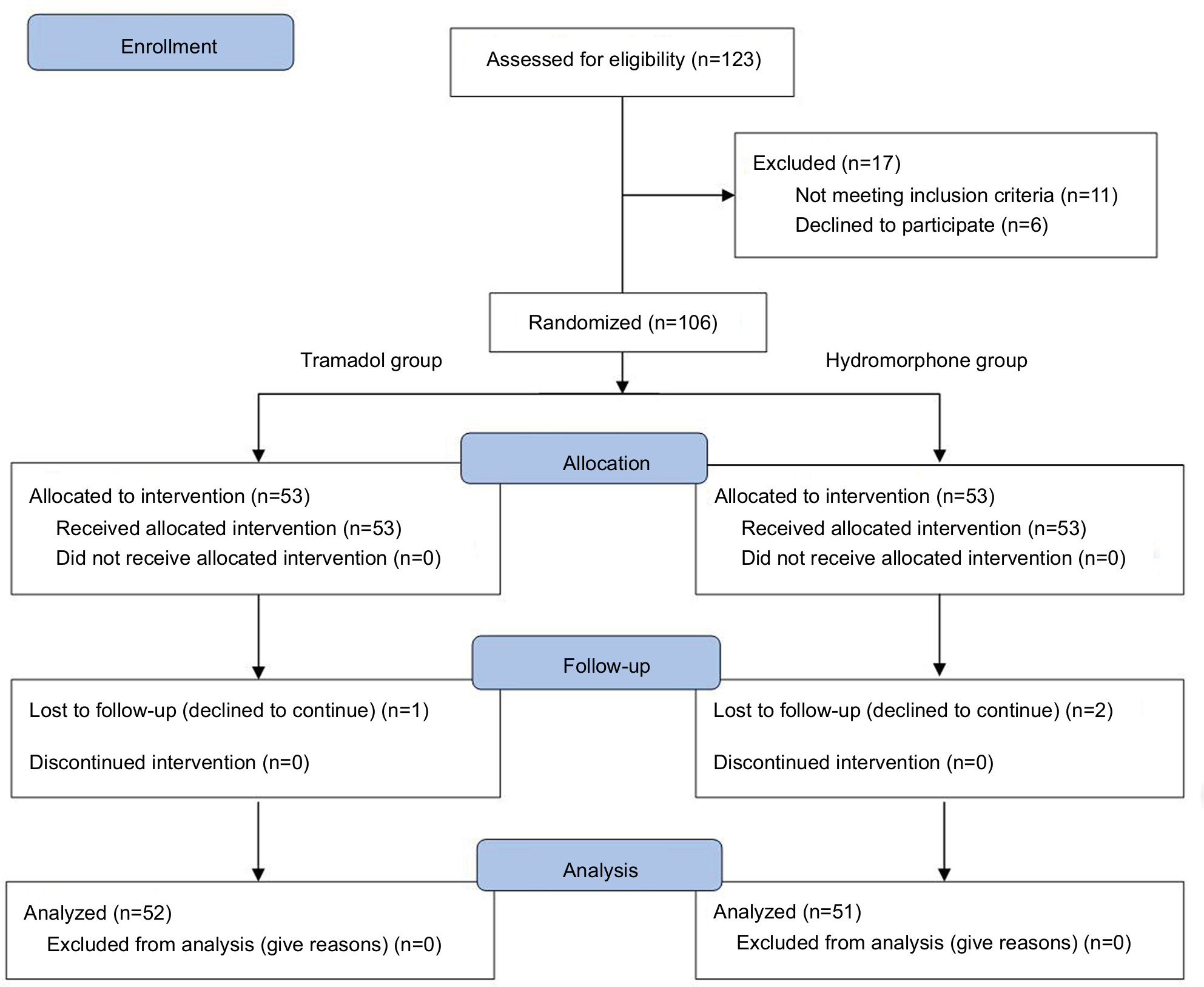 | Figure 1 CONSORT flow diagram of the study. |
Anesthetic and analgesia techniques
Electrocardiography, blood pressure and pulse oxygen saturation were monitored after the patients entered into the operating room. Standardized subarachnoid block anesthesia at L3–4 interspace was performed with isobaric 0.66% ropivacaine 20 mg but without any intrathecal opioids. Operations were conducted by an experienced surgical team, who had successfully completed >1,000 CDs, using a standardized technique. After fetal delivery, and once a day in obstetric ward after the surgery, oxytocin 20 units in 500 mL of saline were routinely given. The amount of intraoperative blood loss and surgery duration were recorded. Patients were monitored for 6 hours in the post-anesthesia care unit before returning to the obstetric ward.
PCIA was started immediately after surgery using a controlled infusion pump. PCIA with tramadol or hydromorphone was applied to patients in the respective groups according to the sealed random numbers. For the patients in the tramadol group, tramadol (Grunenthal Co, Ltd, Aachen, Germany) 4 mg/kg and flurbiprofen 4 mg/kg mixed with 0.9% saline to a volume of 150 mL were placed in a PCIA pump, whereas hydromorphone (Humanwell Pharmaceutical Co, Ltd, Yichang, China) 0.04 mg/kg and flurbiprofen 4 mg/kg were used for the patients of the hydromorphone group. The PCIA pump (150 mL) was programmed to have a background infusion at 2.0 mL/h, a PCIA dose of 1 mL and a lockout period of 15 minutes. The PCIA consumption in 48 hours after surgery was recorded. The postoperative follow-up for pain intensity was carried out by the study investigators. When a patient presented pain numerical rating scale (NRS) >4 and demanded extra analgesia, the pain clinicians were informed. Then, extra analgesic treatment using a single dose of tramadol 50 mg (tramadol group) or hydromorphone 0.5 mg (hydromorphone group) under monitoring was decided and given by the pain clinicians according to the group allocation. The extra analgesia treatment with different analgesic was administered using the same injection syringe by the pain clinicians and were also blinded to patients and study investigators. To prevent intraoperative and postoperative nausea and vomiting (PONV), metoclopramide 10 mg and dexamethasone 10 mg were given before the surgery.
Randomization and masking
Simple randomization was performed in the study, and the random numbers were generated using an online random number generator by an independent assistant who was not involved in any data collection or analysis. The assistant prepared the allocation sequence and hid the numbers in opaque, numbered and sealed envelopes. Patients were randomly allocated into two groups with postoperative analgesic strategy using either tramadol or hydromorphone according to the random number in envelope in the operation room after CD. Then, the envelopes were closed, sealed again and stored at the site of investigation until the end of the study.
Different analgesic strategies were performed using the same type of controlled infusion pump by specialized pain clinicians. In the study, all patients and researchers, including those involved in surgery, were unaware of their group allocation and analgesic strategies during treatment. The pain clinicians who need to make experimental intervention knew the patients’ group allocation. Both the assistant and the pain clinicians were not involved in data collection and independent of the final data analysis. Preoperative and intraoperative data collection, postoperative follow-up during hospitalization period and long-term telephone interview were performed by trained investigators who were blinded to the group allocation.
Outcome measures
Pain intensity during the postoperative 48 hours was determined through NRS of pain (0–10, 0 was defined as no pain and 10 as intolerable pain) at postoperative 4, 8, 12, 24 and 48 hours. In this study, abdominal incision pain NRS at mobilization (on attempting to sit forward in bed) was considered as the primary outcome. The secondary outcomes were incision pain NRS at rest and visceral pain NRS induced by uterine contraction during the 48 hours after CD, and hospital anxiety and depression scale (HADS) 1 week after the surgery. HADS included 14 items assessing symptoms of anxiety and depression (seven items scored 0–3 for anxiety and depression, respectively, yielding a range of 0–21). A score of 8 or above indicates possible anxiety or depression.31,32 The Chinese translation version of HADS has been validated in several previous studies,33,34 and it has been licensed for usage. HADS has been found to be satisfactory for assessing the severity of anxiety and depression for puerpera and has been validated in previous Chinese studies.35–38 The HADS at 1 week after CD was evaluated by an investigator, who was trained by a professional psychologist, through telephone interview.
Except these outcomes, the other critical outcomes included early walking time (the time point when patients could ambulate independently) and length of hospital stay after CD, which was decided by the responsible surgeons according to patients’ ability to active, incision recovery, recovery from postoperative complications, etc.
In addition, the time period when patients started to feel pain after CD, the Ramsay sedation score and vital signs during the postoperative 48 hours, self-reported sleep quality (rated as good or poor) on the day of surgery and 1 day after CD and postoperative adverse events, including nausea, vomiting and pruritus, were recorded. The maximum pain NRS from 3 to 7 days after the surgery was uniformly evaluated by telephone follow-up. Patients were interviewed by telephone for 4 weeks after the surgery to ask the following questions: existing pain or no pain and its effects on sleep.
Statistical analyses
Based on our pilot observation, the mean pain NRS during mobilization at postoperative 4 hours was 3.1 (SD, 1.3) points when receiving a hydromorphone PCIA. The current study was designed as an equivalence test for the primary outcome. We hypothesized that tramadol (experimental group) can provide analgesic effect comparable to hydromorphone (control group), ie, there is no NRS difference between PCIA with tramadol and hydromorphone. We set the equivalence limit as 0.8 points. Therefore, based on a significance level of 0.05, power of 0.8 and considering about 15% loss of follow-up, the required minimum sample size was 53 for each group.
Data were analyzed according to the per-group principle and following a pre-established analysis plan. Statistical analysis was performed using SPSS for Windows version 19.0 (IBM Corporation, Armonk, NY, USA). A two-tailed P-value <0.05 was considered statistically significant. Standard descriptive statistics, such as mean (SD) and number of patients (frequency), were used to summarize the variables. Normal-distributed continuous data including age, height, weight, surgery duration, blood loss, pain NRS, early walking time, hospital stays and PCIA consumption between the hydromorphone group and the tramadol group were compared using independent-sample t-test. Because of abnormal distribution, time of starting to feel pain, HADS anxiety (HADS-A) and HADS depression (HADS-D) scales were compared using the Mann–Whitney U test. Categorical data were analyzed using the chi-squared test, and the rate difference with 95% CI between two groups was calculated. Two-way repeated ANOVA was applied to analyze the mean arterial pressure, heart rate, respiratory rate and Ramsay sedation score at different time points.
Results
A total of 123 patients were assessed for eligibility, and 106 patients (53 patients in each group) were recruited in the study (Figure 1). Because 3 patients (1 patient in the tramadol group and 2 patients in the hydromorphone group) declined to be followed up, 103 patients completed the study and were included in the final analysis. Preoperative baseline characteristics and intraoperative data of the two groups of patients are shown in Table 1, and no significant differences in any of the parameters were found between the two groups (P>0.05).
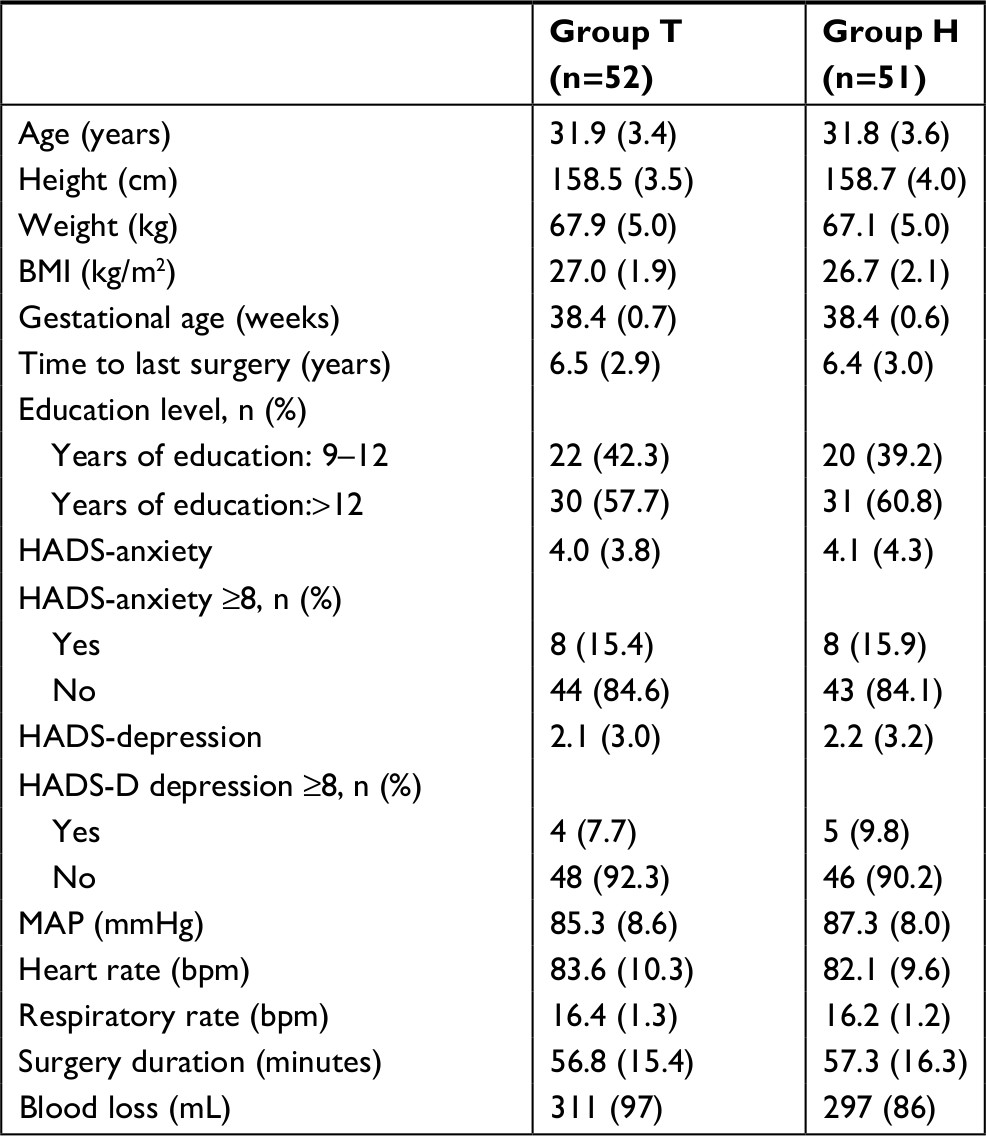 | Table 1 Baseline and intraoperative data Note: Data were presented as mean (SD) or n (%). Abbreviations: BMI, body mass index; HADS, hospital anxiety and depression scale; MAP, mean arterial pressure. |
As shown in Figure 2A and B, the two groups exhibited equivalent incision pain NRS either at rest or mobilization at different time points. Visceral pain NRS at postoperative 4 hours in the tramadol group was significantly higher than in the hydromorphone group (2.9 [1.2] vs 2.3 [1.4], P=0.011) and 8 hours (2.4 [1.1] vs 1.8 [1.1], P=0.028). The mean differences between the two groups were 0.7 (95% CI: 0.2–1.2) and 0.5 (95% CI: 0.1–1.0), respectively (Figure 2C). There was no significant difference in time for patients to start to feel pain, extra analgesia demand, sleep quality and PCIA consumption during the postoperative period between the two groups (Table 2).
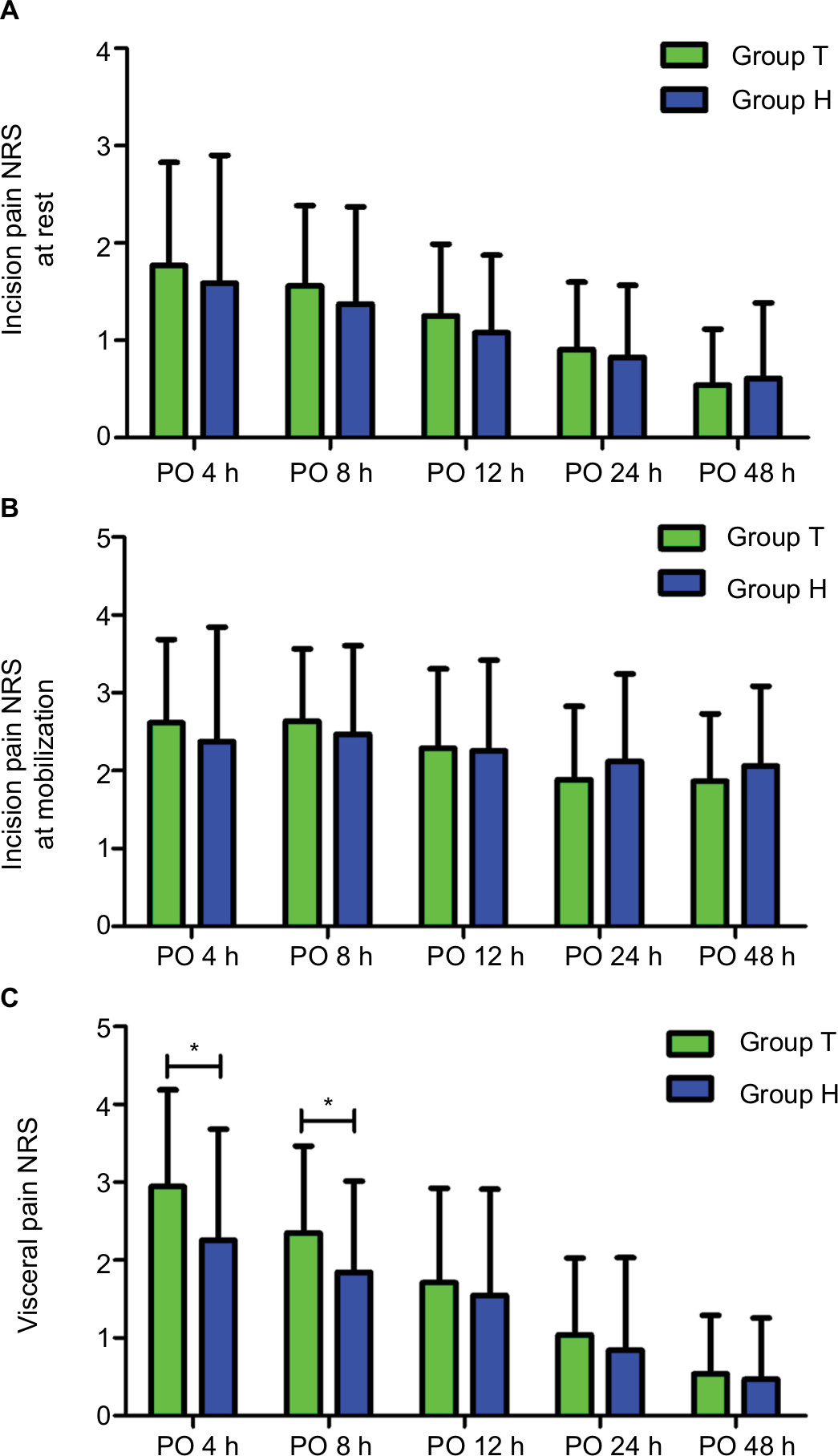 | Figure 2 PO pain NRS including incision pain at rest (A), incision pain at mobilization (B) and visceral pain (C) during the PO 48-hour follow-up. Note: *P<0.05. Abbreviations: h, hours; NRS , numerical rating scale; PO , postoperative. |
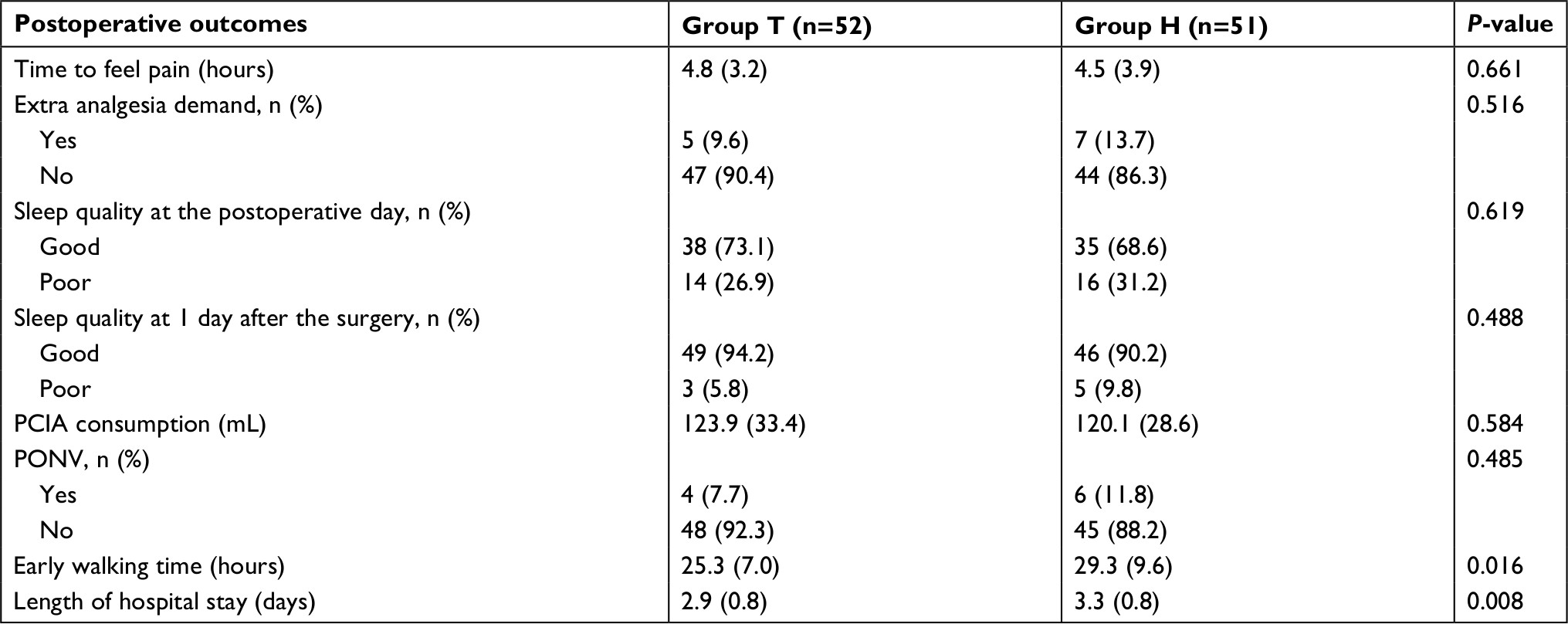 | Table 2 Comparisons of postoperative outcomes between two groups during hospitalization Abbreviations: PCIA, patient-controlled intravenous analgesia; PONV, postoperative nausea and vomiting. |
Postoperative HADS evaluation showed that the anxiety scores of HADS for the patients of the tramadol group were significantly lower than those of the patients who received hydromorphone analgesia (1.9 [3.5] vs 3.6 [4.1], P=0.033; Table 3). The depression scores in the tramadol group were significantly lower than those in the hydromorphone group (0.8 [1.3] vs 2.7 [4.1], P=0.023; Table 3). The HADS-A and HADS-D scores for the two groups before and after the surgery are shown in Figure 3. As shown in Table 3, the percentage of patients in the tramadol group who had a HADS-A of ≥8 and a HADS-D of ≥8 during the postoperative period were significantly lower than those in the hydromorphone group (HADS-A: 1.9% [1/52] vs 13.7% [7/51], P=0.023; HADS-D: 0.0% [0/52] vs 13.7% [7/51], P=0.006). The differences for HADS-A and HADS-D between two groups were 11.8% (95% CI: 2.4%–21.2%) and 13.7% (95% CI: 4.3%–23.1%), respectively.
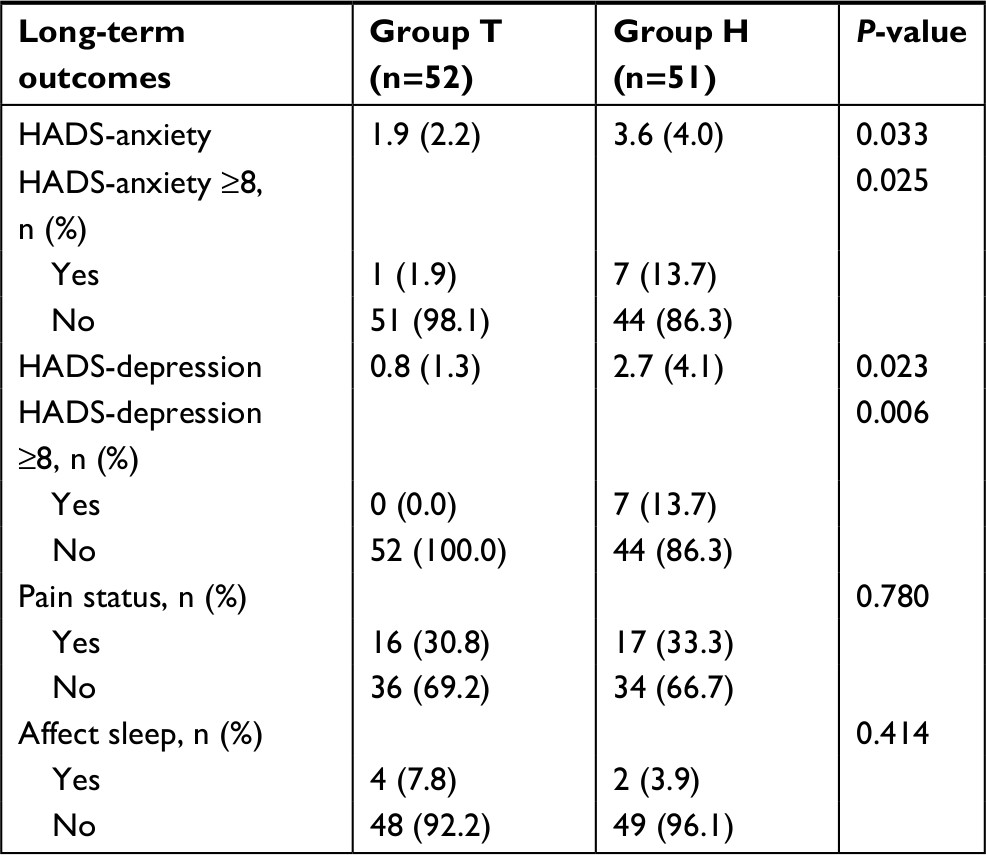 | Table 3 Comparisons of long-term outcomes between two groups Note: Data were presented as mean (SD) or number (percentage). Abbreviation: HADS, hospital anxiety and depression scale. |
 | Figure 3 The HADS-A scores (A) and HADS-D scores (B) before and after the surgery. Note: *P<0.05. Abbreviation: HADS , hospital anxiety and depression scale; HADS-A, HADS anxiety; HADS-D, HADS depression. |
As shown in Table 2, the early walking time in the tramadol group was significantly shorter than that in the hydromorphone group (25.3 [7.0] hours vs 29.3 [9.6] hours, P=0.016), and the mean difference between the two groups was 4.0 (95% CI: 0.8–7.3). Furthermore, the length of hospital stay after the surgery in the tramadol group was also significantly shorter than that in the hydromorphone group (2.9 [0.8] days vs 3.3 [0.8] days, P=0.008), and the mean difference between the two groups was 0.4 (95% CI: 0.1–0.7).
Two-way repeated ANOVA showed that there was no significant difference in mean arterial pressure, heart rate, respiratory rate and Ramsay scale between the tramadol group and the hydromorphone group (Figure 4). No respiratory depression, pruritus, excessive sedation or agitation or other intraoperative and postoperative complications were noted in this study. PONV occurred to four patients (4/52, 7.7%) in the tramadol group and six patients (6/51, 11.8%) in the hydromorphone group during the 48-hour follow-up. All these observed adverse effects were tolerable after treatment and were not significant between the two groups (P=0.485).
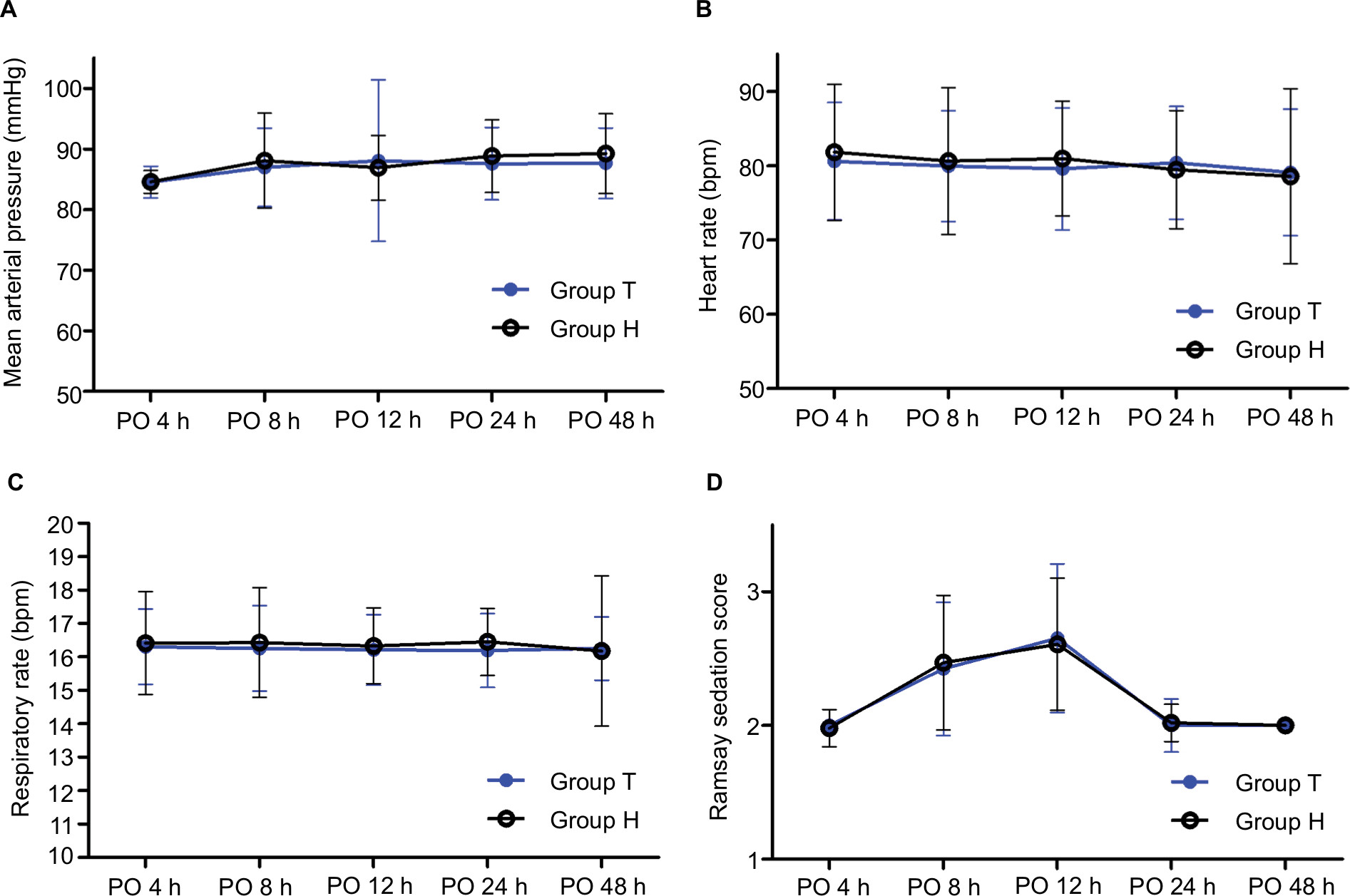 | Figure 4 PO parameters of vital signs (A) mean arterial pressure, (B) heart rate, (C) respiratory rate and Ramsay scores (D) during the PO 48-hour follow-up.PO. Abbreviations: h, hours; PO, postoperative. |
Additionally, the results of telephone interview regarding the maximum pain NRS from 3 to 7 days after the surgery showed no difference between two groups (Figure 5). The pain status 1 month after the surgery showed that a total of 32.0% (33/103) patients experienced postoperative pain, and 18.2% (6/33) of the patients’ sleep quality was affected by the pain. No significant difference in pain status was found between the two groups.
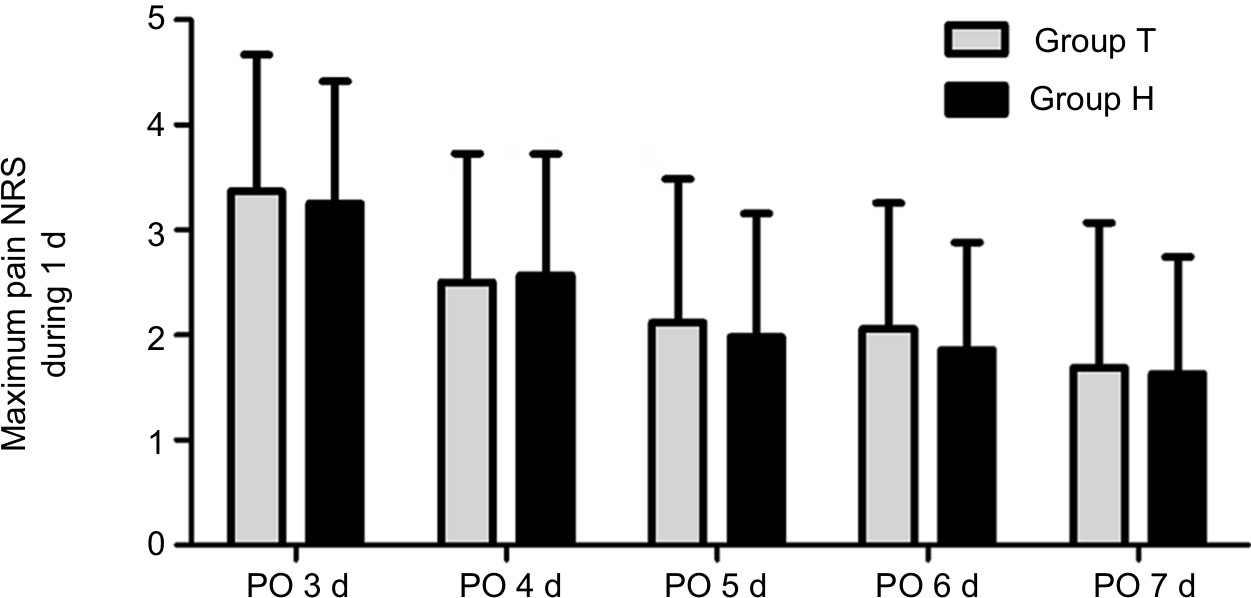 | Figure 5 Pain NRS during the postoperative follow-up from 3 to 7 days after the surgery. Abbreviations: d, days; NRS, numerical rating scale; PO, postoperative. |
Discussion
This study found that, for the patients who received secondary CD, the analgesic effect of PCIA with tramadol on visceral pain at 4 and 8 hours after the surgery was less effective than that of PCIA with hydromorphone. However, the postoperative HADS-A and HADS-D scores at 1 week after CD of the patients who received tramadol analgesia were significantly lower than those who received hydromorphone analgesia. Furthermore, early walking time and the length of hospital stay after the surgery of the patients received tramadol analgesia were significantly shorter than those who received hydromorphone analgesia.
Previous studies have demonstrated that 10 mg of tramadol was equipotent to 1 mg morphine,39 and 1 mg morphine was equipotent to about 0.1–0.15 mg hydromorphone.40,41 A recent study has found that the combination of hydromorphone and intravenous NSAID produced a strong synergistic analgesia on postoperative pain.42 Studies regarding post-CD analgesia management also emphasized the important role of use of NSAID.19,43 Therefore, in this study, we used the combination of NSAID and tramadol or NSAID and hydromorphone to treat surgical pain after CD. According to the equivalent dose (10,000:1.5), a recent study by Chi et al12 found that the PCIA using 10 mg/mL tramadol was more effective than using 1.5 µg/mL sufentanil for CD. Unlike the previous study, the current results showed that the analgesia effect of tramadol on incision pain was not better than that of hydromorphone. On the contrary, the effect of tramadol on visceral pain at early time points (4 hours and 8 hours after the surgery) was worse than hydromorphone. Furthermore, other pain outcomes between two analgesics, including time to feel pain, the total incidences of extra analgesia requirement during the postoperative analgesia period and pain intensity at 3–7 days after the surgery, were also comparable. All patients in this study were multipara patients who had a history of one CD, whereas only primipara patients were included in Chi’s study. Thus, the difference induced by surgery history between multipara and primipara may contribute to the diverse response to surgery and analgesics.
Nevertheless, the current results indicated that the analgesic effect of tramadol was not better than hydromorphone. It is known that effective postoperative pain control can improve patient outcomes including rehabilitation and length of hospital stay.44,45 Thus, the outcomes of patients in the tramadol group may not be as good as those in the hydromorphone group. However, the current results demonstrated an unexpected finding that patients who received tramadol analgesia can independently get out of bed at an earlier time point, and, more importantly, had shorter hospital stays than those who received hydromorphone analgesia. The reason for this observation is not known. We speculate that the different effects of tramadol and hydromorphone on anxiety and depression may contribute to the abovementioned phenomenon.
Except for the postoperative pain, the presence of depression and anxiety is associated with delayed recovery after surgery.46,47 The current results showed that, compared to hydromorphone, intravenous tramadol can significantly decrease the HADS-A and HADS-D scores even 1 week after CD (about 5 days after PCIA treatment). The incidences of positive anxiety and depression based on the cutoff value of HADS after PCIA with tramadol were also lower compared to PCIA with hydromorphone. The rate differences for possible anxiety and depression between two groups reached 11.8% (95% CI: 2.4%–21.2%) and 13.7% (95% CI: 4.3%–23.1%), respectively. Although the patients in the tramadol group showed higher visceral pain intensity at 4 hours and 8 hours after the surgery, no difference was found at later time points or on other pain outcomes. Better mental status may have accelerated patients’ independent activity and decreased the length of hospital stay.
To our knowledge, these results demonstrated for the first time that the use of PCIA with tramadol and flurbiprofen may help to reduce the levels of anxiety and depression in the early postpartum period for women undergoing CD. Postpartum anxiety and depression are known to be associated with reduced level of serotonin and norepinephrine. Selective serotonin reuptake inhibitor or serotonin norepinephrine reuptake inhibitors were commonly used for the treatment of postpartum anxiety and depression.29,30,48–50 Tramadol acts as a weak agonist at μ-opioid receptors, inhibits the re-uptake of both serotonin and noradrenaline and thereby increases their concentrations in descending inhibitory pathways involved in antinociception.15,51 On the other hand, hydromorphone produces analgesic effect mainly because it is an agonist at μ-opioid receptors. This might explain the current finding regarding why the two analgesics have different psychological effects. In addition, previous studies have demonstrated that significant change in serotonin and norepinephrine levels is present at postpartum 48 hours in the patients with postpartum depression, matching the time of postoperative analgesia.48,52 These previous findings further support and explain the current finding that postoperative 48 hours PCIA with tramadol have the potential to reduce postpartum anxiety and depression in the early postpartum period.
Postpartum mental disorders, especially depression, can cause harm to the health of the woman and infant. The estimated prevalence of postpartum depression ranges from 6.5% to 12.9%53,54 and are higher in patients undergoing CD.55,56 Recent data showed that in 2014 >1.2 million patients were scheduled to receive CD in USA.57 In China, this number reached 5.2 million.58 The potential strategy using intravenous tramadol may help to prevent postpartum depression and anxiety during postoperative analgesia period for patients undergoing CD, which may produce huge social benefits.
Several limitations should be considered in this study. First, this was a small study in women who had undergone a second CD, and hence false-positive results are possible. Larger studies looking at the same and other postpartum populations are needed to further investigate the potential beneficial effects of PCIA with tramadol. Second, the study was not designed to evaluate degree of anxiety and depression separately. Further study using more sensitive depression scale, such as Edinburgh postnatal depression scale, should be carried out. In addition, because HADS scoring was done after being discharged from hospital, social factors and living conditions at home may influence the patients’ HADS scores. A direct randomized controlled study with a larger sample size using postpartum depression or anxiety level as the primary outcome is needed to determine the anti-anxiety and anti-depression effects of tramadol for CD patients in the future.
Conclusion
Although the PCIA with tramadol did not provide better analgesic effects than PCIA with hydromorphone, we found that it reduced depression and anxiety in the early postpartum period for patients undergoing secondary CD. Also, postoperative analgesia using tramadol can enhance patients’ mobilization and shorten their hospital stays. Further work is needed to validate and assess these findings in greater detail.
Acknowledgment
The study was supported by Clinical Research Projects of Xinqiao Hospital, Third Military Medical University (No. 2015YLC09, HL, and No. 2016YLC10, GD).
Disclosure
The authors report no conflicts of interest in this work.
References
Gerbershagen HJ, Aduckathil S, van Wijck AJ, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118(4):934–944. | ||
Patel R, Carvalho JC, Downey K, Kanczuk M, Bernstein P, Siddiqui N. Intraperitoneal instillation of lidocaine improves postoperative analgesia at cesarean delivery: a randomized, double-blind, placebo-controlled trial. Anesth Analg. 2017;124(2):554–559. | ||
Wang L, Xu X, Baker P, et al. Factors associated with intention to have caesarean delivery in pregnant women in China: a cross-sectional analysis. Lancet. 2016;388(Suppl 1):S2. | ||
Zeng Y, Hesketh T. The effects of China’s universal two-child policy. Lancet. 2016;388(10054):1930–1938. | ||
Zhang Y, Gu N, Wang Z, Zheng M, Hu Y, Dai Y. Use of the 10-Group Classification System to analyze how the population control policy change in China has affected cesarean delivery. Int J Gynaecol Obstet. 2017;138(2):158–163. | ||
Tulandi T, Agdi M, Zarei A, Miner L, Sikirica V. Adhesion development and morbidity after repeat cesarean delivery. Am J Obstet Gynecol. 2009;201(1):56.e1–e6. | ||
Arlier S, Seyfettinog˘lu S, Yilmaz E, et al. Incidence of adhesions and maternal and neonatal morbidity after repeat cesarean section. Arch Gynecol Obstet. 2017;295(2):303–311. | ||
Valdes AM, Suokas AK, Doherty SA, Jenkins W, Doherty M. History of knee surgery is associated with higher prevalence of neuropathic pain-like symptoms in patients with severe osteoarthritis of the knee. Semin Arthritis Rheum. 2014;43(5):588–592. | ||
Plesh O, Gansky SA, Curtis DA, Pogrel MA. The relationship between chronic facial pain and a history of trauma and surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88(1):16–21. | ||
Duan G, Guo S, Zhang Y, et al. Effects of epidemiological factors and pressure pain measurements in predicting postoperative pain: a prospective survey of 1,002 Chinese patients. Pain Physician. 2017;20(6):E903–E914. | ||
Lei B, Wang L, He S. Postoperative analgesic effect of hydromorphone hydrochloride in patients with scar uterus cesarean section. J China. 2016;30(3):150–152. | ||
Chi X, Li M, Mei W, Liao M. Comparison of patient-controlled intravenous analgesia with sufentanil versus tramadol in post-cesarean section pain management and lactation after general anesthesia – a prospective, randomized, double-blind, controlled study. J Pain Res. 2017;10:1521–1527. | ||
Nie JJ, Sun S, Huang SQ. Effect of oxycodone patient-controlled intravenous analgesia after cesarean section: a randomized controlled study. J Pain Res. 2017;10:2649–2655. | ||
Verstraete S, Van de Velde M. Post-cesarean section analgesia. Acta Anaesthesiol Belg. 2012;63(4):147–167. | ||
Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43(13):879–923. | ||
Scott LJ, Perry CM. Tramadol: a review of its use in perioperative pain. Drugs. 2000;60(1):139–176. | ||
Demirel I, Ozer AB, Atilgan R, Kavak BS, Unlu S, Bayar MK, Sapmaz E. Comparison of patient-controlled analgesia versus continuous infusion of tramadol in post-cesarean section pain management. J Obstet Gynaecol Res. 2014;40(2):392–398. | ||
Kanazi GE, Aouad MT, Abdallah FW, Khatib MI, Adham AM, Harfoush DW, Siddik-Sayyid SM. The analgesic efficacy of subarachnoid morphine in comparison with ultrasound-guided transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg. 2010;111(2):475–481. | ||
Mitra S, Khandelwal P, Sehgal A. Diclofenac-tramadol vs. diclofenac-acetaminophen combinations for pain relief after caesarean section. Acta Anaesthesiol Scand. 2012;56(6):706–711. | ||
Olieman RM, Siemonsma F, Bartens MA, Garthus-Niegel S, Scheele F, Honig A. The effect of an elective cesarean section on maternal request on peripartum anxiety and depression in women with childbirth fear: a systematic review. BMC Pregnancy Childbirth. 2017;17(1):195. | ||
Togher KL, Treacy E, O’Keeffe GW, Kenny LC. Maternal distress in late pregnancy alters obstetric outcomes and the expression of genes important for placental glucocorticoid signalling. Psychiatry Res. 2017;255:17–26. | ||
Howard LM, Molyneaux E, Dennis CL, Rochat T, Stein A, Milgrom J. Non-psychotic mental disorders in the perinatal period. Lancet. 2014;384(9956):1775–1788. | ||
Wu YM, McArthur E, Dixon S, Dirk JS, Welk BK. Association between intrapartum epidural use and maternal postpartum depression presenting for medical care: a population-based, matched cohort study. Int J Obstet Anesth. 2018;35:10–16. | ||
Fairbrother N, Janssen P, Antony MM, Tucker E, Young AH. Perinatal anxiety disorder prevalence and incidence. J Affect Disord. 2016;200:148–155. | ||
Wang SY, Jiang XY, Jan WC, Chen CH. A comparative study of postnatal depression and its predictors in Taiwan and mainland China. Am J Obstet Gynecol. 2003;189(5):1407–1412. | ||
Wisner KL, Sit DK, McShea MC, et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry. 2013;70(5):490–498. | ||
Szkutnik-Fiedler D, Kus K, Balcerkiewicz M, et al. Concomitant use of tramadol and venlafaxine – evaluation of antidepressant-like activity and other behavioral effects in rats. Pharmacol Rep. 2012;64(6):1350–1358. | ||
Caspani O, Reitz MC, Ceci A, Kremer A, Treede RD. Tramadol reduces anxiety-related and depression-associated behaviors presumably induced by pain in the chronic constriction injury model of neuropathic pain in rats. Pharmacol Biochem Behav. 2014;124:290–296. | ||
Roth CK, Hering SL, Campos S. Serotonin syndrome in pregnancy. Nurs Womens Health. 2015;19(4):345–349. | ||
Sekiyama T, Nakatani Y, Yu X, Seki Y, Sato-Suzuki I, Arita H. Increased blood serotonin concentrations are correlated with reduced tension/anxiety in healthy postpartum lactating women. Psychiatry Res. 2013;209(3):560–565. | ||
de Miranda S, Pochard F, Chaize M, et al. Postintensive care unit psychological burden in patients with chronic obstructive pulmonary disease and informal caregivers: a multicenter study. Crit Care Med. 2011;39(1):112–118. | ||
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. | ||
Leung CM, Ho S, Kan CS, Hung CH, Chen CN. Evaluation of the Chinese version of the hospital anxiety and depression scale. a cross-cultural perspective. Int J Psychosom. 1993;40(1–4):29–34. | ||
Li Q, Lin Y, Hu C, Xu Y, Zhou H, Yang L, Xu Y. The Chinese version of hospital anxiety and depression scale: psychometric properties in Chinese cancer patients and their family caregivers. Eur J Oncol Nurs. 2016;25:16–23. | ||
Wang W, Chair SY, Thompson DR, Twinn SF. A psychometric evaluation of the Chinese version of the Hospital Anxiety and Depression Scale in patients with coronary heart disease. J Clin Nurs. 2009;18(13):1908–1915. | ||
Wang LJ, Chen SW, Chen CK, et al. Treatment-emergent depression and anxiety between peginterferon alpha-2a versus alpha-2b plus ribavirin for chronic hepatitis C. BMC Psychiatry. 2016;16(1):424. | ||
Rubertsson C, Hellström J, Cross M, Sydsjö G. Anxiety in early pregnancy: prevalence and contributing factors. Arch Womens Ment Health. 2014;17(3):221–228. | ||
Tam WH, Lee DT, Chiu HF, Ma KC, Lee A, Chung TK. A randomised controlled trial of educational counselling on the management of women who have suffered suboptimal outcomes in pregnancy. BJOG. 2003;110(9):853–859. | ||
Unlugenc H, Ozalevli M, Gunes Y, Guler T, Isik G. Pre-emptive analgesic efficacy of tramadol compared with morphine after major abdominal surgery. Br J Anaesth. 2003;91(2):209–213. | ||
Hill JL, Zacny JP. Comparing the subjective, psychomotor, and physiological effects of intravenous hydromorphone and morphine in healthy volunteers. Psychopharmacology. 2000;152(1):31–39. | ||
Chang AK, Bijur PE, Davitt M, Gallagher EJ. Randomized clinical trial of an intravenous hydromorphone titration protocol versus usual care for management of acute pain in older emergency department patients. Drugs Aging. 2013;30(9):747–754. | ||
Oh E, Ahn HJ, Sim WS, Lee JY. Synergistic effect of intravenous ibuprofen and hydromorphone for postoperative pain: prospective randomized controlled trial. Pain Physician. 2016;19(6):341–348. | ||
Wilder-Smith CH, Hill L, Dyer RA, Torr G, Coetzee E. Postoperative sensitization and pain after cesarean delivery and the effects of single im doses of tramadol and diclofenac alone and in combination. Anesth Analg. 2003;97(2):526–533. | ||
Wu CL, Raja SN. Treatment of acute postoperative pain. Lancet. 2011;377(9784):2215–2225. | ||
Argoff CE. Recent management advances in acute postoperative pain. Pain Pract. 2014;14(5):477–487. | ||
Wilson TJ, Chang KW, Yang LJ. Depression and anxiety in traumatic brachial plexus injury patients are associated with reduced motor outcome after surgical intervention for restoration of elbow flexion. Neurosurgery. 2016;78(6):844–850. | ||
Tully PJ, Baker RA, Turnbull D, Winefield H. The role of depression and anxiety symptoms in hospital readmissions after cardiac surgery. J Behav Med. 2008;31(4):281–290. | ||
Aishwarya S, Rajendiren S, Kattimani S, Dhiman P, Haritha S, Ananthanarayanan PH. Homocysteine and serotonin: association with postpartum depression. Asian J Psychiatr. 2013;6(6):473–477. | ||
Yildiz G, Senturk MB, Yildiz P, Cakmak Y, Budak MS, Cakar E. Serum serotonin, leptin, and adiponectin changes in women with postpartum depression: controlled study. Arch Gynecol Obstet. 2017;295(4):853–858. | ||
Lonstein JS. Regulation of anxiety during the postpartum period. Front Neuroendocrinol. 2007;28(2–3):115–141. | ||
Stevens AJ, Woodman RJ, Owen H. The effect of ondansetron on the efficacy of postoperative tramadol: a systematic review and meta-analysis of a drug interaction. Anaesthesia. 2015;70(2):209–218. | ||
Treadway CR, Kane FJ, Jarrahi-Zadeh A, Lipton MA. A psychoendocrine study of pregnancy and puerperium. Am J Psychiatry. 1969;125(10):1380–1386. | ||
Gaynes BN, Gavin N, Meltzer-Brody S, et al. Perinatal depression: prevalence, screening accuracy, and screening outcomes. Evid Rep Technol Assess (Summ). 2005;119(119):1–8. | ||
Munk-Olsen T, Laursen TM, Pedersen CB, Mors O, Mortensen PB. New parents and mental disorders: a population-based register study. JAMA. 2006;296(21):2582–2589. | ||
Sword W, Landy CK, Thabane L, et al. Is mode of delivery associated with postpartum depression at 6 weeks: a prospective cohort study. BJOG. 2011;118(8):966–977. | ||
Xie RH, Lei J, Wang S, Xie H, Walker M, Wen SW. Cesarean section and postpartum depression in a cohort of Chinese women with a high cesarean delivery rate. J Womens Health (Larchmt). 2011;20(12):1881–1886. | ||
Hamilton BE, Martin JA, Osterman MJ, Curtain SC. Births: preliminary data for 2014. Natl Vital Stat Rep. 2015;64(6):1–19. | ||
Li HT, Luo S, Trasande L, et al. Geographic variations and temporal trends in cesarean delivery rates in China, 2008-2014. JAMA. 2017;317(1):69–76. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.