Back to Journals » Clinical Ophthalmology » Volume 16
Patient Attitudes and Desirability Regarding Immediate Sequential Bilateral Cataract Surgery
Authors Rush SW, Omoruyi F, Rush RB ![]()
Received 20 February 2022
Accepted for publication 20 April 2022
Published 29 April 2022 Volume 2022:16 Pages 1375—1381
DOI https://doi.org/10.2147/OPTH.S363327
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sloan W Rush,1,2 Felix Omoruyi,2 Ryan B Rush2,3
1Rush Eye Associates, Amarillo, TX, 79106, USA; 2Texas Tech University Health Science Center, Amarillo, TX, 79106, USA; 3Southwest Retina Specialists, Amarillo, TX, 79106, USA
Correspondence: Ryan B Rush, Southwest Retina Specialists, 7411 Wallace Blvd, Amarillo, TX, 79106, USA, Tel +1-806 351-1870, Email [email protected]
Purpose: To analyze patient attitudes and desirability regarding routine immediate sequential bilateral cataract surgery (ISBCS).
Methods: This study was conducted as a prospective, consecutive survey-based case series from a single private practice institution serving a mostly rural population. A standardized phone survey assessing patient perspectives on ISBCS was administered to patients before and after routine delayed sequential bilateral cataract surgery (DSBCS) was performed. Subject responses were analyzed, including a subset analysis on patient responses under a variety of circumstances.
Results: There were 61 patients enrolled into the study and 47 completed the surveys before and after routine DSBCS (77.0% completion rate). Thirty-nine (83.0%) of respondents had a favorable outlook of ISBCS preoperatively, whereas 36 (76.6%) had a favorable outlook of ISBCS postoperatively (p> 0.05). On the postoperative questionnaire, twenty-five (53.2%) of respondents were willing to accept additional surgical risk if necessary to receive ISBCS, and this finding was significant between the subgroup of patients with systemic health co-morbidities compared to those without systemic health co-morbidities (p=0.05).
Conclusion: Most patients had a favorable outlook of ISBCS before and after undergoing DSBCS. Patients with underlying systemic health co-morbidities were most likely to accept additional surgical risk if necessary to receive ISBCS. From a patient’s perspective, ISBCS may be an acceptable option to routinely implement when cataract surgery is required for both eyes.
Keywords: bilateral cataract surgery, patient desirability
Introduction
Phacoemulsification with intraocular lens is the most common surgical procedure performed in the USA with an excess of 4 million annually.1 The overwhelming majority of them are conducted in the setting of delayed sequential bilateral cataract surgery (DSBCS).2 Numerous reports over the last 10 years have explored the benefits and risks of immediate sequential bilateral cataract surgery (ISBCS).3–5 ISBCS has already been incorporated into practice in the USA when special circumstances arise such as cases requiring general anesthesia or in pediatric patients,6 but it is not the standard practice for routine cases.7 Most advocates for ISBCS cite the increasing amount of literature that indicate safety and effectiveness when appropriate protocols are used,8–10 whereas opponents of ISBCS cite concerns related to serious complications such as bilateral endophthalmitis11,12 and a lack of high-quality evidence.13,14 Other investigators have described the potential time and cost savings for patients as well as the reduced cost burden for healthcare systems.15–18
In addition to the debate on efficacy and safety as it relates to ISBCS, there are many nonmedical barriers that discourage widespread implementation. These include lack of full physician reimbursement, medicolegal issues, and lack of board/society approval.19–21 Another factor may be patient acceptance and attitudes towards ISBCS. To date, the published literature has limited information on direct inputs from a patient’s perspective. Patient attitudes and desirability regarding ISBCS may help determine circumstances in which ISBCS may be offered as a preferred option in the setting of routine cataract surgery. In this study, we explore patient reported outcome measures under a variety of circumstances to gain insight about ISBCS by scoring and evaluating patient impressions.
Methods
This prospective case series was approved by the SRS Institutional Review Board (IRB00009122) and was conducted on consecutive patients scheduled for routine DSBCS at a single private practice location in Amarillo, TX during the month of April 2021. All components of the study adhered to the principles of the Declaration of Helsinki and were in accordance to human research standards and regulations.
Questionnaire and Patient Recruitment
The questionnaire was administered preoperatively and postoperatively to participating study subjects scheduled for routine DSBCS. Once informed consent was obtained, patients were administered the preoperative component of the survey by phone 7 days (± 2 days) from their scheduled cataract surgery time for the first eye. The postoperative survey was conducted by phone 4 weeks (± 1 week) after cataract surgery for the second eye. All surveys were given by the same examiner (FO).
Data Collection and Statistical Analysis
Questionnaire data was entered into a safe-guarded spreadsheet (MS Excel). The JMP 11 software from the SAS Institute (Cary, NC, USA) was used to generate percentages, means and standard deviations for the survey responses. One-way analysis of the variance was used to compare numerical outcomes, whereas contingency analysis with likelihood ratios was used to compare outcomes between nominal variables. The results were considered statistically significant at the p<0.05 level. Incomplete surveys were excluded from the analysis.
Results
There were 61 patients enrolled into the study, whilst 47 patients completed both the preoperative and postoperative surveys (77.0%) and therefore included in the study’s analysis.
Preoperative Survey Outcomes
Table 1 details patient responses to the preoperative questionnaire. Notably, 74.5% of the survey participants described their living situation as “living alone”. The average one-way distance travel mileage to the eye surgery center was 47.7 (±45.2) with 48.9% of patients traveling 50 miles or greater. There were 83.0% of the respondents that indicated favorable impression for ISBCS with a desirability scaled score of 7.6 (±2.7). There were 3 patients (6.4%) that gave it the lowest rating of “1” and 16 patients (34.0%) that gave it the highest rating of “10”.
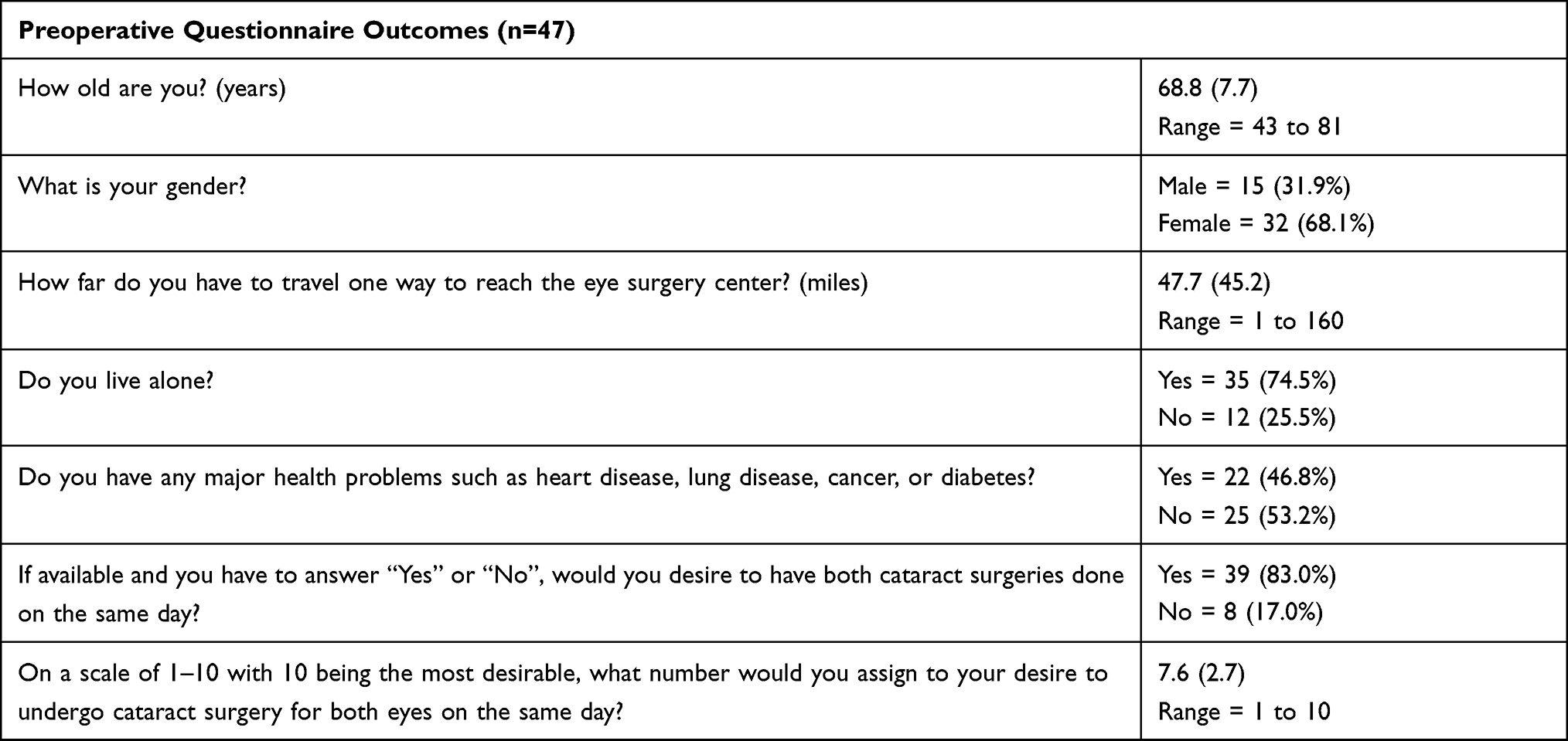 |
Table 1 Preoperative Questionnaire Outcomes. Distributions and Means with (Standard Deviations) |
Postoperative Survey Outcomes
Table 2 details patient responses to the postoperative questionnaire. The average time span between surgery for both eyes was 9.4 (±4.5) days with a range of 9 to 28 days. Having gone through the DSBCS process, survey respondents estimated that their average cost and time savings would have been 89.8 (±120.9) USD and 19.3 (±22.0) hours, respectively, if cataract surgery was performed on both eyes on the same day. Very similar to the preoperative survey outcomes, there were 76.6% of patients that indicated a preference for ISBCS with a desirability scaled score of 7.5 (±2.9). There were 53.2% of patients willing to accept additional surgical risk in order to have ISBCS rather than DSBCS.
 |
Table 2 Postoperative Questionnaire Outcomes. Distributions and Means with (Standard Deviations) |
Comparative Analysis
Patient attitudes and desirability regarding ISBCS remained constant before and after DSBCS and between various cohorts with respect to living arrangements, travel distance, and active systemic health comorbidities (p>0.05 for all). When comparing patients living near (<50 miles or less away from surgery center) versus patients living far (50 miles or more away from surgery center), the far patients revealed more projected cost savings by an average of 73.6 USD (p=0.04) and more time savings by an average of 14.9 hours (p=0.02). Patients with active systemic health comorbidities were more willing to accept increased surgical risk in favor of ISBCS compared to otherwise healthy patients (p=0.05). Table 3 displays this subgroup analysis.
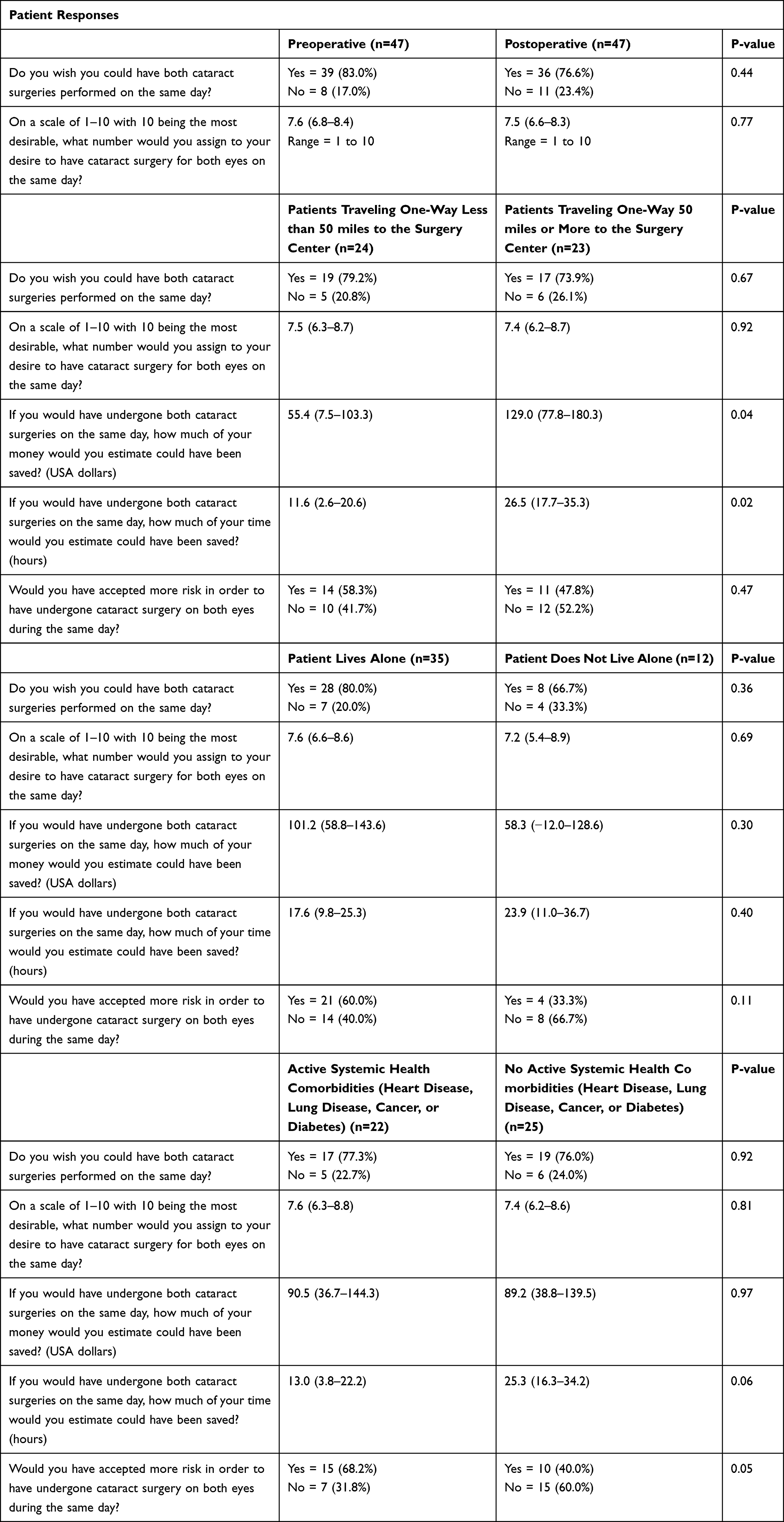 |
Table 3 Comparative Analysis for Patient Responses Regarding ISBCS in Various Scenarios. Distributions and Means with (95% Confidence Intervals) |
Discussion
The questionnaires analyzed in this study shed light on patient preferences for ISBCS. It is noteworthy that patient attitudes and desirability for ISBCS did not change in the postoperative period following DSBCS. Patient impressions also remained consistent postoperatively across a variety of scenarios including patient living arrangements, travel distances, and presence of systemic health co-morbidities. This suggests that a majority of the patients surveyed recognized a potential for decreased physician visits, cost and travel time savings, and other convenience factors with ISBCS, and if given the choice by the physician, would elect for ISBCS over DSBCS.
Common objections to the routine performance of ISBCS relate to safety issues. This can range from non-vision threatening mishaps such as aberrant intraocular lens calculation on the first eye to severe (albeit rare) complications such as bilateral postoperative endophthalmitis. However, Arshinoff et al10 and other study groups8 have demonstrated the effectiveness of ISBCS and report an exceedingly low incidence of severe complications when proper precautions are utilized. Furthermore, the most recent nationwide registry in the US revealed that the rate of endophthalmitis is the same between patients that underwent ISBCS and DSBCS.22 It is revealing that over half of the patients surveyed in this study indicated that they would accept a higher complication risk for the sake of receiving ISBCS. This factor should be considered when determining the most appropriate technique for each patient.
There is data suggesting that improved patient experience with medical care will improve clinical outcomes.23 However, studies evaluating routine medical care have struggled to characterize effective outcome measures that will determine patient satisfaction.24 With specific regards to ISBCS, we have identified certain patient circumstances that will affect patient attitudes and their economic burden. Not surprisingly, patients residing 50 miles or more from the surgery center reported the potential for greater cost and time savings with ISBCS. Average patient projected cost savings of 73.6 USD for this cohort can be accounted for based upon savings on fuel and, in some cases, overnight hotel lodging. Average patient projected time savings of 14.9 hours for this group may be largely tied to time spent on the road, and it results in approximately 2 days of no wages (or loss of vacation) for those still in the workforce. These factors are necessary to consider when offering ISBCS, especially for practices like ours that serve rural populations.
Patients with systemic health co-morbidities may experience greater challenges in making physician appointments when compared to the general population. This may in part explain why this subgroup was more willing to accept a higher complication rate if fewer physician visits would result as with ISBCS. Surprisingly, transportation to-and-from surgery was not an important factor in our survey, and patients living alone were no more likely to have a favorable impression toward ISBCS than those living with family or caretakers. This suggests that rideshare companies, public transportation, and housing facilities offer patients suitable transportation options to-and-from physician appointments.
Weaknesses of this study include its observational design without subject randomization to DSBCS or ISBCS, inclusion of patients from just one isolated geographic area in the USA, and the relatively small number of survey respondents. Strengths of this study include its prospective outlook and the high completion rate of survey respondents. In summary, little data regarding patient perspectives exists for in the setting of cataract surgery. This study reports high desirability for routine ISBCS from a patient perspective, especially in patients with systemic health co-morbidities. When considering the implementation of ISBCS into routine clinical practice, surgeons should question the patient’s desirability on the matter as an important factor when assessing each patient’s suitability for this technique. More research is needed from the perspective of the cataract surgery patient to further elucidate which subjects may be routinely offered ISBCS.
Abbreviations
ISBCS, immediate sequential bilateral cataract surgery; DSBCS, delayed sequential bilateral cataract surgery.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The study was approved by the SRS Institutional Review Board (IRB00009122) in accordance with the Ethical Standards laid down in the Declaration of Helsinki.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. National Eye Institute Cataract Data and Statistics. Available from: https://www.nei.nih.gov/learn-about-eye-health/outreach-campaigns-and-resources/eye-health-data-and-statistics/cataract-data-andAQ6 statistics. Accessed April, 27 2022.
2. American Academy of Ophthalmology Cataract in the Adult Eye Preferred Practice Patterns 2021. Available from: https://www.aao.org/preferred-practice-pattern/cataract-in-adult-eye-ppp-2021-in-press. Accessed April 27, 2022.
3. Malvankar-Mehta MS, Chen YN, Patel S, et al. Immediate versus delayed sequential bilateral cataract surgery: a systematic review and meta-analysis. PLoS One. 2015;10(6):e0131857. doi:10.1371/journal.pone.0131857
4. Herrinton LJ, Liu L, Alexeeff S, et al. Immediate Sequential vs Delayed Sequential Bilateral Cataract Surgery: Retrospective Comparison of Postoperative Visual Outcomes. Ophthalmol. 2017;124(8):1126–1135.
5. Lee E, Balasingam B, Mills EC, Zarei-Ghanavati M, Liu C. A survey exploring ophthalmologists’ attitudes and beliefs in performing immediately sequential bilateral cataract surgery in the United Kingdom. BMC Ophthalmol. 2020;20(1):210. doi:10.1186/s12886-020-01475-0
6. Bhambhwani V, Khalili S, Tehrani N, et al. Outcomes and complications of immediate versus delayed sequential bilateral cataract surgery in children. J AAPOS. 2020;24(3):
7. Singh R, Dohlman TH, Sun G. Immediately sequential bilateral cataract surgery: advantages and disadvantages. Curr Opin Ophthalmol. 2017;28(1):81–86. doi:10.1097/ICU.0000000000000327
8. Serrano-Aguilar P, Ramallo-Fariña Y, Cabrera-Hernández JM, et al. Immediately sequential versus delayed sequential bilateral cataract surgery: safety and effectiveness. J Cataract Refract Surg. 2012;38(10):1734–1742. doi:10.1016/j.jcrs.2012.05.024
9. Arshinoff SA. Same-day cataract surgery should be the standard of care for patients with bilateral visually significant cataract. Surv Ophthalmol. 2012;57(6):574–579. doi:10.1016/j.survophthal.2012.05.002
10. Arshinoff S, Claoue C, Johansson B. iSBCS general principles for excellence in ISBCS 2009. International Society of Bilateral Cataract Surgeons; 2009.
11. Masket S. Same day bilateral cataract surgery-who benefits? Ophthalmology. 2021;128(1):11–12. doi:10.1016/j.ophtha.2020.08.017
12. Henderson BA, Schneider J. Same-day cataract surgery should not be the standard of care for patients with bilateral visually significant cataract. Surv Ophthalmol. 2012;57(6):580–583. doi:10.1016/j.survophthal.2012.05.001
13. Kessel L, Andresen J, Erngaard D, et al. Immediate sequential bilateral cataract surgery: a systematic review and meta-analysis. J Ophthalmol. 2015;2015:912481. doi:10.1155/2015/912481
14. Lansingh VC, Eckert KA, Strauss G. Benefits and risks of immediately sequential bilateral cataract surgery: a literature review. Clin Exp Ophthalmol. 2015;43(7):666–672. doi:10.1111/ceo.12527
15. Rush SW, Gerald AE, Smith JC, Rush JA, Rush RB. Prospective analysis of outcomes and economic factors of same-day bilateral cataract surgery in the United States. J Cataract Refract Surg. 2015;41(4):732–739. doi:10.1016/j.jcrs.2014.07.034
16. Neel ST. A cost-minimization analysis comparing immediate sequential cataract surgery and delayed sequential cataract surgery from the payer, patient, and societal perspectives in the United States. JAMA Ophthalmol. 2014;132:1282–1288. doi:10.1001/jamaophthalmol.2014.2074
17. O’Brart DP, Roberts H, Naderi K, Gormley J. Economic modelling of immediately sequential bilateral cataract surgery (ISBCS) in the national health service based on possible improvements in surgical efficiency. BMJ Open Ophthalmol. 2020;5(1):e000426. doi:10.1136/bmjophth-2019-000426
18. Leivo T, Sarikkola AU, Uusitalo R, Hellstedt T, Ess S-L, Kivelä T. Simultaneous bilateral cataract surgery: economic analysis; Helsinki simultaneous bilateral cataract surgery study report 2. J Cataract Refractive Surg. 2011;37:1003–1008. doi:10.1016/j.jcrs.2010.12.050
19. Amsden LB, Shorstein NH, Fevrier H, et al. Immediate sequential bilateral cataract surgery: surgeon preferences and concerns. Can J Ophthalmol. 2018;53(4):337–341. doi:10.1016/j.jcjo.2017.10.034
20. Mills EC, Zarei-Ghanavati M, Liu CSC. Immediate sequential bilateral cataract surgery: the rationale, implementation, and beliefs of ophthalmic surgeons across Europe. J Cataract Refract Surg. 2019;45(12):1725–1731. doi:10.1016/j.jcrs.2019.07.027
21. Tatham A, Brookes JL. Bilateral same-day cataract surgery should routinely be offered to patients – no. Eye. 2012;26:1033–1035. doi:10.1038/eye.2012.92
22. Lacy M, Kung TH, Owen JP, et al. Endophthalmitis rate in immediately sequential versus delayed sequential bilateral cataract surgery within the Intelligent Research in Sight (IRIS) registry data. Ophthalmology. 2022;129(2):129–138. doi:10.1016/j.ophtha.2021.07.008
23. Navarro S, Ochoa CY, Chan E, Du S, Farias AJ. Will improvements in patient experience with care impact clinical and quality of care outcomes?: a systematic review. Med Care. 2021;59(9):843–856. doi:10.1097/MLR.0000000000001598
24. Black D, Held ML, Skeesick J, Peters T. Measures evaluating patient satisfaction in integrated health care settings: a systematic review. Community Ment Health J. 2021;57(8):1464–1477. doi:10.1007/s10597-020-00760-y
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.