Back to Journals » Patient Preference and Adherence » Volume 16
Patient and Provider Perspectives on Medication Non-adherence Among Patients with Depression and/or Diabetes in Diverse Community Settings – A Qualitative Analysis
Authors Hamilton JE, Blanco E, Selek S, Wirfel KL, Bernstam EV, Velligan D ![]() , Gudala M
, Gudala M ![]() , Roberts K
, Roberts K
Received 27 July 2021
Accepted for publication 15 October 2021
Published 30 June 2022 Volume 2022:16 Pages 1581—1594
DOI https://doi.org/10.2147/PPA.S328785
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jane E Hamilton,1 Eduardo Blanco,2 Salih Selek,1 Kelly L Wirfel,3 Elmer V Bernstam,3,4 Dawn Velligan,5 Meghana Gudala,4 Kirk Roberts4
1The University of Texas Health Science Center at Houston, McGovern Medical School, Louis Faillace Department of Psychiatry and Behavioral Sciences, Houston, TX, USA; 2Arizona State University, School of Computing and Augmented Intelligence, Tempe, AZ, USA; 3The University of Texas Health Science Center at Houston, McGovern Medical School, Department of Internal Medicine, Houston, TX, USA; 4The University of Texas Health Science Center at Houston, School of Biomedical Informatics, Houston, TX, USA; 5The University of Texas Health Science Center at San Antonio, Long School of Medicine, Department of Psychiatry, San Antonio, TX, USA
Correspondence: Jane E Hamilton, The University of Texas Health Science Center at Houston, McGovern Medical School, Louis A. Faillace, MD, Department of Psychiatry and Behavioral Sciences, 1941 East Road, BBSB 1204, Houston, TX, 77054, USA, Tel +1 713-486-2858, Email [email protected]
Background: Diabetes and depression affect a significant percentage of the world’s total population, and the management of these conditions is critical for reducing the global burden of disease. Medication adherence is crucial for improving diabetes and depression outcomes, and research is needed to elucidate barriers to medication adherence, including the intentionality of non-adherence, to intervene effectively. The purpose of this study was to explore the perspectives of patients and health care providers on intentional and unintentional medication adherence among patients with depression and diabetes through a series of focus groups conducted across clinical settings in a large urban area.
Methods: This qualitative study utilized a grounded theory approach to thematically analyze qualitative data using the framework method. Four focus groups in total were conducted, two with patients and two with providers, over a one-year period using a semi-structured facilitation instrument containing open-ended questions about experiences, perceptions and beliefs about medication adherence.
Results: Across the focus groups, communication difficulties between patients and providers resulting in medication non-adherence was a primary theme that emerged. Concerns about medication side effects and beliefs about medication effectiveness were identified as perceptual barriers related to intentional medication non-adherence. Practical barriers to medication adherence, including medication costs, forgetting to take medications and polypharmacy, emerged as themes related to unintentional medication non-adherence.
Conclusion: The study findings contribute to a growing body of research suggesting health system changes are needed to improve provider education and implement multicomponent interventions to improve medication adherence among patients with depression and/or diabetes, both chronic illnesses accounting for significant disease burden globally.
Keywords: medication adherence, patient and provider preferences, intentional versus unintentional nonadherence
Background
Medication adherence refers to the extent to which taking medication corresponds with the agreement between patients and providers based on prescribed medications.1 Studies have consistently shown that 20% to 30% of medication prescriptions are never filled and that approximately 50% of medications for chronic illnesses are not taken as prescribed.2,3 Further, medication non-adherence is a significant barrier to successful treatment, estimated to cause at least 100,000 preventable deaths and $100 billion in preventable medical costs per year.1 Medication non-adherence for patients with one or more chronic illnesses is extremely common, especially among patients who are prescribed medications for the management of chronic conditions such as diabetes and/or depression.4–7 Medication non-adherence may be reduced by improving the quality of the patient-provider relationship8 and improving understanding of adherence barriers. Accordingly, evidence supports adopting a patient-centered approach for improving medication adherence.9–11 However, the complexity of medication non-adherence among patients with diabetes and/or depression requires a framework that considers the intentionality of non-adherence to develop effective interventions.12–14 Intentional non-adherence refers to non-adherence that is deliberate and largely associated with patient motivation whereas unintentional non-adherence is largely driven by a lack of capacity or resources to take medications.15 There is also overlap between these categories making it difficult to elucidate factors contributing to intentional versus unintentional medication non-adherence.16 While research has led to theories of medication adherence,17–20 there is limited literature exploring intentional and unintentional adherence among patients with chronic illnesses such as depression and diabetes, especially from the perspectives of patients and health care providers.21 While previous qualitative research has conducted semi-structured interviews with patients and providers to understand barriers to medication adherence among patients with uncontrolled diabetes,22 qualitative research has not utilized a conceptual framework to guide the data collection process or analysis among patients with diabetes and/or depression. In particular, qualitative research is needed to obtain in depth information on patient and provider perspectives on intentional and unintentional medication adherence for diabetes and/or depression.13 This study fills a gap in current qualitative research by explicitly seeking participant perceptions on medication non-adherence using the conceptual framework as it relates to depression and diabetes.
Methods
This qualitative study utilized a grounded theory approach.23,24 Two patient and two provider focus groups (four in total) were conducted over a one-year period to obtain patient and provider-reported information to develop a theoretical model of medication adherence for individuals with depression and/or diabetes. In line with recommendations for conducting qualitative research on health service use, focus group participants who shared key characteristics pertinent to the study were recruited for each focus group that comprised between five and nine participants.25 One focus group was conducted with patients with a primary diagnosis of diabetes and one focus group was conducted with patients with a primary diagnosis of depression to ensure participants would have similar enough experiences to feel safe to share openly and honestly about issues related to their medical conditions and barriers they may be facing adhering to prescribed medication.26 Patient participants were selected based on their clinical diagnoses, and patients were excluded if they did not have a primary diagnosis of diabetes and/or depression. Healthcare providers who were currently treating patients diagnosed with diabetes and/or depression were recruited for the provider focus groups. A description of each focus group is as follows:
- Focus Group One: Patients diagnosed with depression being treated in an inpatient psychiatric hospital (n=9 participants)
- Focus Group Two: Mental health providers (psychiatrists, psychologists, and clinical social workers) treating patients diagnosed with depression (n=7 participants)
- Focus Group Three: Participants in a community wellness program for individuals of Hispanic ethnicity diagnosed with diabetes (n=7 participants)
- Focus Group Four: Diabetes providers (attending and resident physicians) at an academic medical center serving diverse populations. (n=5 participants).
Focus Group Participants
Depression patients and providers were recruited from a regional academic psychiatric safety-net hospital in a large urban area serving approximately 9000 low-income and uninsured patients per year. Depression patients were recruited from an inpatient depression unit at the hospital, and depression providers included inpatient psychiatrists, clinical psychologists and social workers. Diabetes patients were recruited from a diabetes self-management program administered by the local health department in a low-income community. Diabetes providers were recruited from the primary care practice group of an academic medical center and through a safety-net hospital general medicine unit.
Study Funding
Research reported in this article was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (ME-2018C1-10963). The statements in this article are solely the responsibility of the authors and do not necessarily represent the views of PCORI, its Board of Governors or Methodology Committee.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki and received ethics approval from the University of Texas Health Science Center Houston Institutional Review Board (IRB#HSC-SBMI-19-0196).
Informed Consent
Prior to beginning each focus group, informed consent was obtained for each participant, who was informed that anything they said during the focus group would be held in the strictest confidence and they would not be quoted directly. Participants were told that if they chose not to participate in the focus group, their decision not to participate would not be disclosed to anyone. Participants were given the opportunity to ask questions or voice concerns prior to each focus group.
Data Collection
Data were collected during each focus group using a semi-structured facilitation instrument. One instrument was developed for patient participants and one instrument was developed for provider participants to guide the discussion in each focus group. Each facilitation instrument contained eight open-ended questions. The patient focus group facilitation instrument (Table 1) was designed to obtain detailed information across the following domains including:
- Patient experiences taking prescription medications, and specifically adhering to a medication regimen
- Intentional medication non-adherence
- Unintentional medication non-adherence
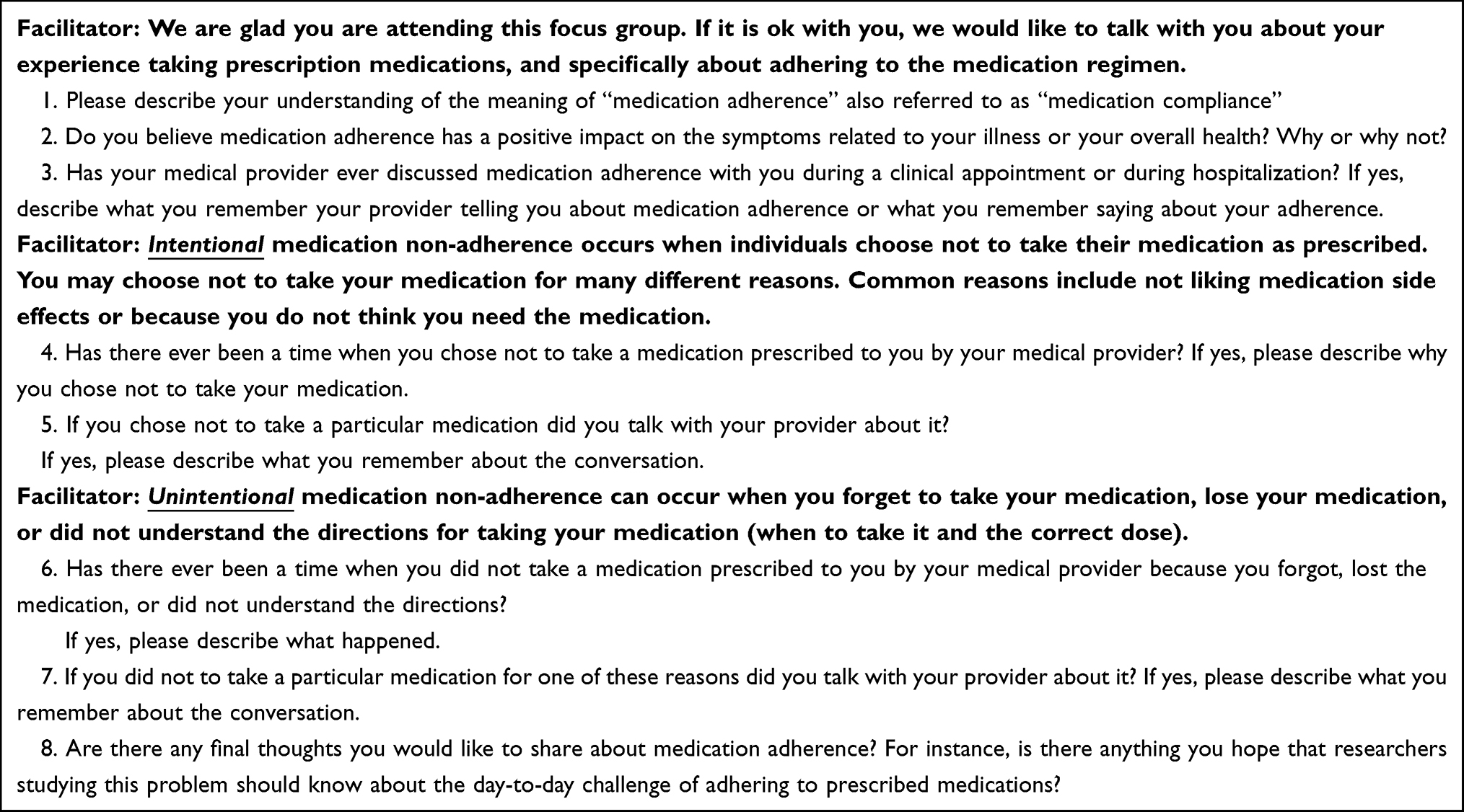 |
Table 1 Patient Focus Group Questions |
The provider focus group focus group facilitation instrument (Table 2) was designed to obtain detailed information across the following domains including:
- Provider experiences interacting with patients who are on prescription medications, and specifically about those patients adhering to the medication regimen
- Intentional medication non-adherence
- Unintentional medication non-adherence
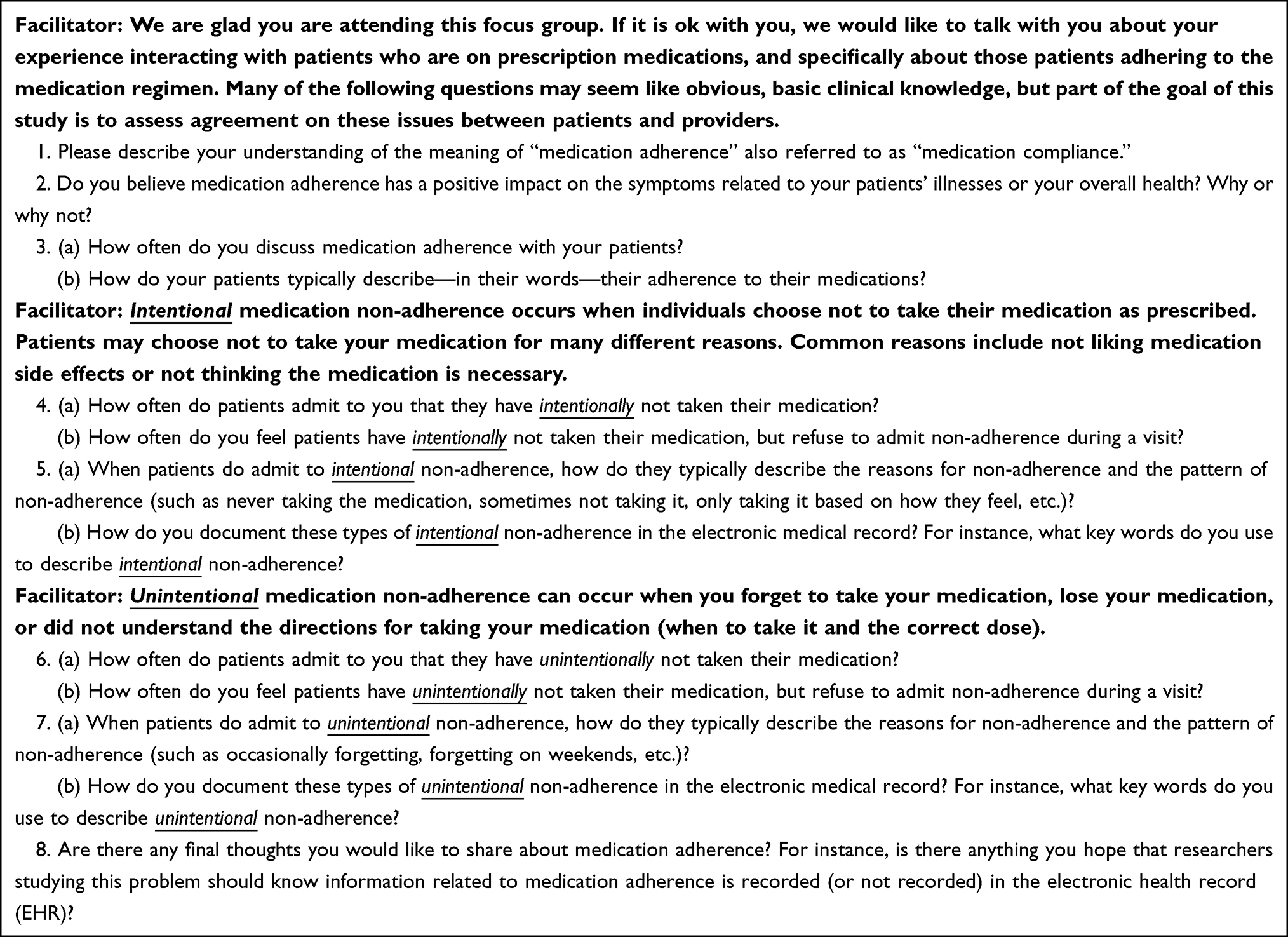 |
Table 2 Provider Focus Group Questions |
The focus group discussions were facilitated by a moderator (a co-investigator with prior experience facilitating focus groups) and co-moderator (principal investigator) who encouraged participants to share their perceptions and points of view about medication non-adherence. A graduate research assistant assisted with the key informant interviews by observing the interviews and taking notes. All focus groups were audio recorded and transcribed verbatim.
Data Analysis
To conduct thematic analysis guided by a grounded theory approach, a coding rubric was developed to code the transcribed data. Two of the investigators (J.H. and K.R.) used an iterative open coding approach to identify major themes in the focus group data.27 Each investigator worked independently when coding the interview data and was blinded to the coding used by the other investigator until the coding process was completed. The inter-coder agreement for two coders using Krippendorff’s alpha was 70.8% for n = 65 cases (46 agreements, 19 disagreements). Disagreements in coding were resolved through negotiated consensus, refining, and finalizing the coding structure. During the indexing process, the coders documented how many times a particular concern was raised by a participant to identify themes and underlying theoretical constructs. The final indexed text providing a listing and frequency of the codes mentioned in the focus group text (overall, within each interview, and across interviews) is presented in Tables 3–6. Focus group analyses identified common and contrasting themes emerging:
- Within each focus group
- Across patient focus groups
- Across provider focus groups
- Across all four focus groups
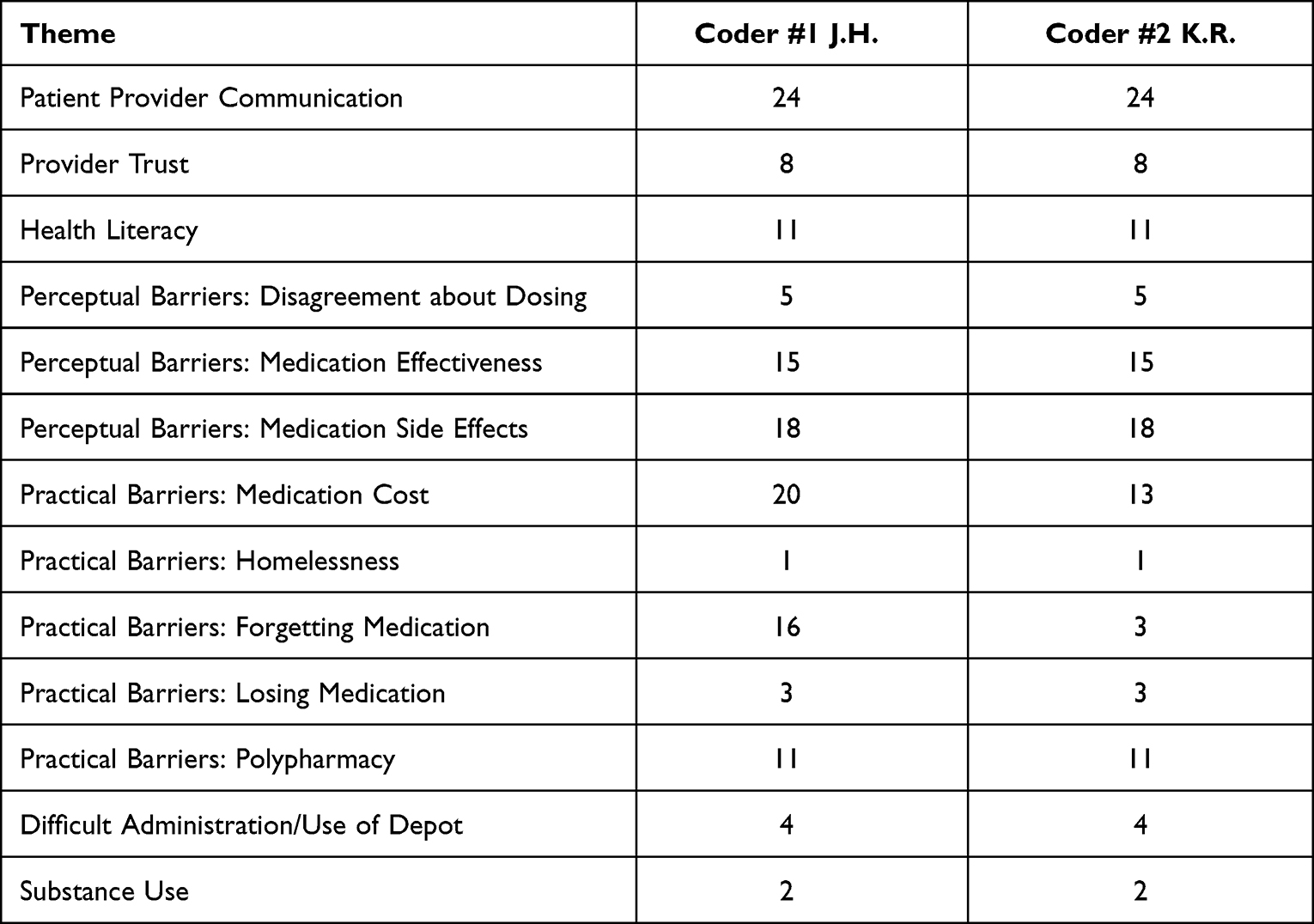 |
Table 3 Focus Group One |
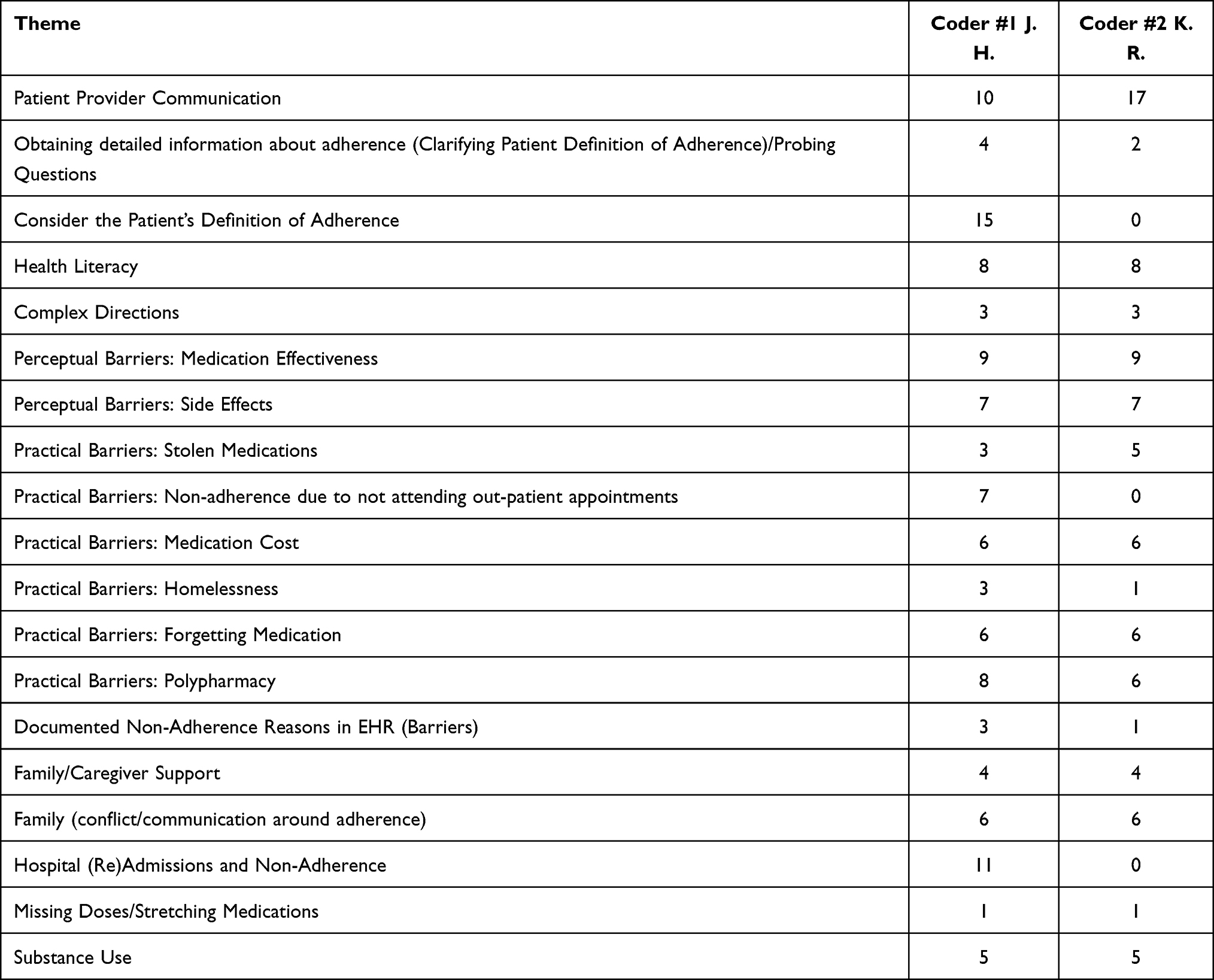 |
Table 4 Focus Group Two |
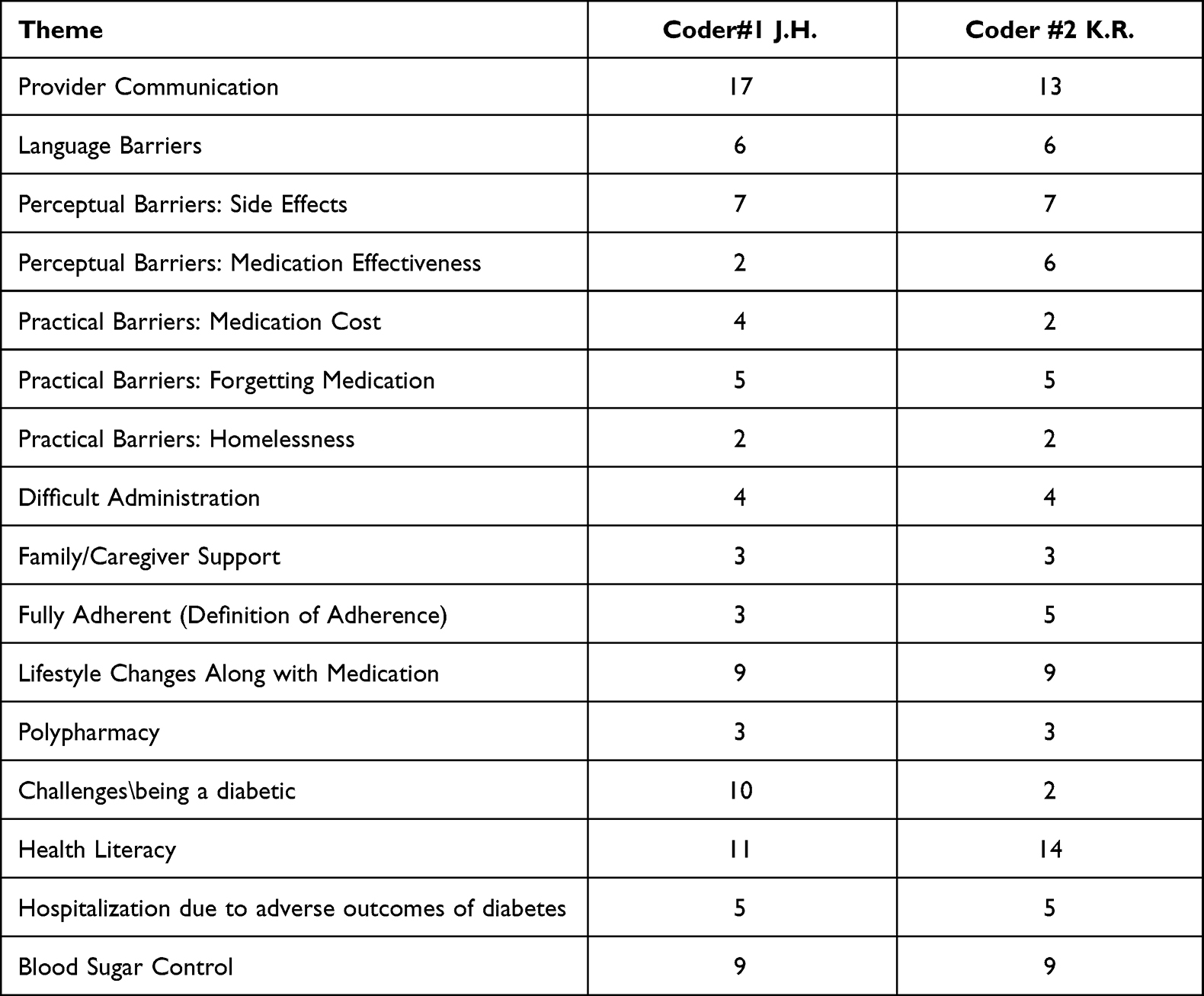 |
Table 5 Focus Group Three |
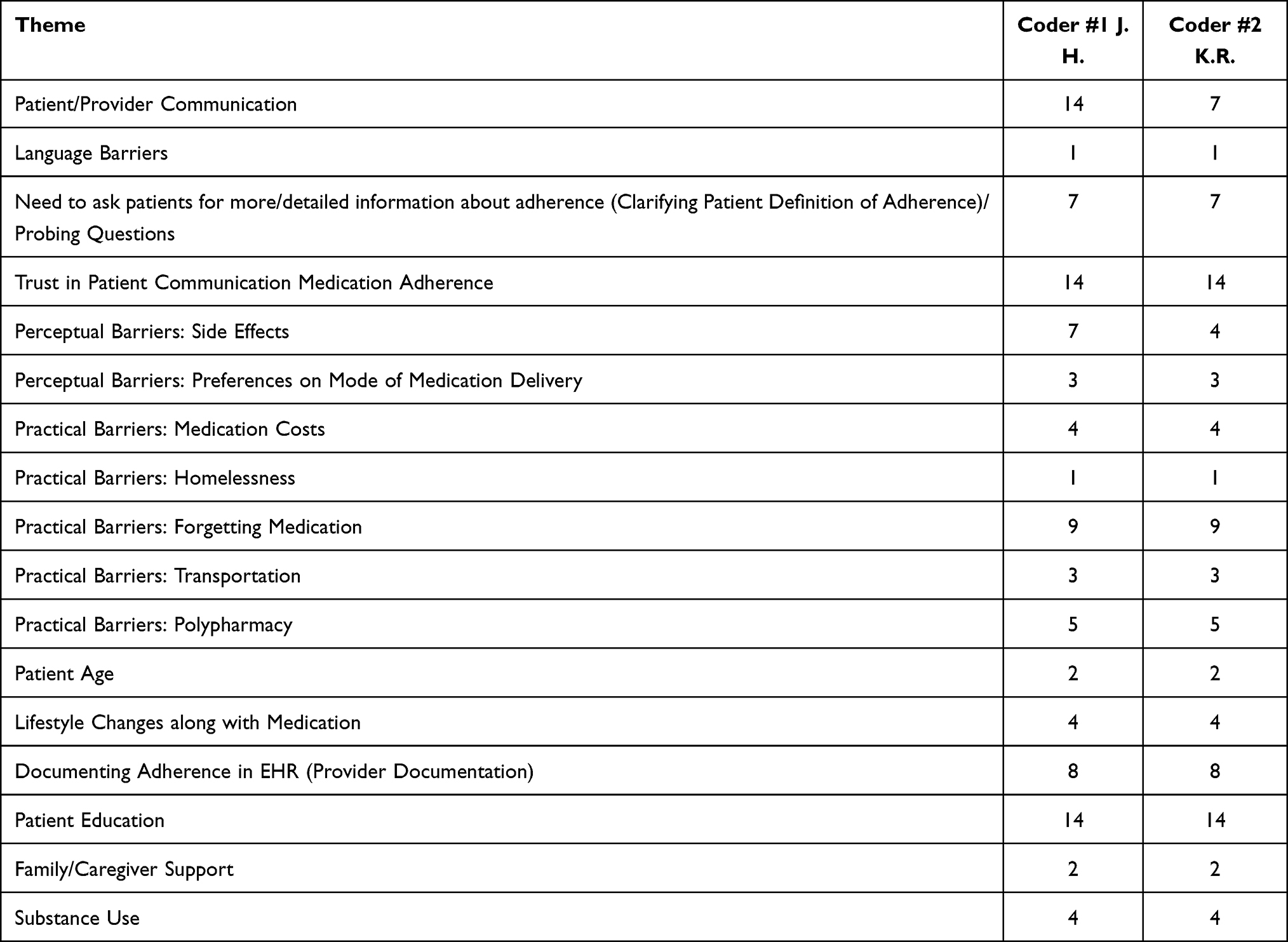 |
Table 6 Focus Group Four |
Across focus groups, if a particular comment was made only once, then the comment was not included as a theme. Codes were tallied and stratified with the most frequently emerging codes reported as major themes. All codes were thematically analyzed using the framework method28 to organize the data into categories to develop the model of medication adherence (Figure 1). The framework method was used to create a new structure for the data to summarize and reduce the data across focus groups in order to develop the theoretical model. During the analysis process, codes were grouped into clusters around similar and interrelated ideas or concepts (Tables 4–6) to start the process of abstraction of the data (i.e., towards the general rather than the specific or anecdotal).28 Using grounded theory to guide the termination of the data analysis, saturation was defined as the point at which no new codes were occurring in the data and as the point at which a complete range of theoretical constructs was fully represented by the data (Figure 1). Member checking, also known as participant or respondent validation, is a technique for exploring the credibility of qualitative analysis results.29 Member checking was conducted by including stakeholder advisory board members, three healthcare providers (K.W., E.B., and S.S.), as study co-authors to improve the quality of the interpretation of the qualitative analyses as they are working in clinical settings where the study was conducted and also participated in the provider focus groups. PCORI Stakeholder Advisory Board members commented on study design and qualitative analysis.
 |
Figure 1 Model medication non-adherence. |
Results
Across focus groups, participants acknowledged medication non-adherence to be a complex problem in depression and/or diabetes. Emerging themes fell into three categories: Patient-Provider Communication, Intentional Medication Non-Adherence (Perceptual Barriers), and Unintentional Medication Non-Adherence (Practical Barriers). Emerging themes are presented across patient focus groups, provider focus groups, and all focus groups.
Patient Focus Groups
Across the patient focus groups, participants discussed how communication difficulties with their providers resulted in medication non-adherence. The need for more culturally competent and collaborative communication about adherence to their prescribed medications emerged as a theme. In particular, participants explained that more instructions on how to take prescribed medication and education on what to expect would help them be adherent. A Spanish-speaking only participant in the diabetes patient focus group reported “not every doctor can explain, can sit down and ask you what is bothering you, is everything ok?” Further, patient participants report that their providers are not talking with them about the need to be adherent to prescribed medications. One participant reported “I have been to multiple mental health hospitals due to major depression and suicide and only providers at one hospital actually talked to me about adherence to medications … they were the ones who actually sat down and talked to me about the importance of the medication and if it’s not working, to talk to the doctor about it or take it on time or if you miss a dose, when to take it next and everything.” Another participant reported “communication is big … if you really want me to take it … how are you going to take something if you do not trust what you are taking.” Beliefs about medication ineffectiveness emerged as a theme, especially among depression focus group participants who voiced concerns about the length of time for depression medication to become effective and the inability of the medication to relieve depression symptoms, were given as a reason for intentional medication non-adherence. Across the depression and diabetes patient focus groups, a theme emerged that intentional non-adherence was related to medication side effects. A depression focus group participant reported “me, I’m afraid of side effects –you know, everyone they say, what I have now and then prepare for something else because of what I’m taking now, because bam boom I got another thing due to taking medicine.” Across the diabetes and depression patient focus groups, participants reported that they do not trust the medication they are taking due to concerns about side effects, but have a difficult time communicating with their providers about their concerns. One participant in the depression focus group reported “So how you gonna take something that you don’t trust what you are taking?” Multiple patient participants reported being unintentionally non-adherent to depression medications primarily due to practical barriers accessing prescribed medication. Practical barriers reported by patient participants in the depression focus group were related to social determinants of health (SDoH) including not being able to afford the medication due to lacking income or being uninsured (n=11 comments) and/or not having transportation to pick up medication from the pharmacy. In the diabetes patient focus group, participants reported not taking all their medications as prescribed to make them last longer. One participant discussed that medication non-adherence occurring “usually because they don’t have money to buy so they make it last longer. I have seen that a lot here.” Practical barriers reported by patient participants also included forgetting to take medication as prescribed. In the diabetes patient focus group, one participant reported “I had a long day … yesterday … so, I forgot them in the morning.” The theme of polypharmacy (involving the administration of five or more medicines for the treatment of one or more medical conditions), emerged among focus group participants as a practical barrier resulting in unintentional medication non-adherence. A participant from the depression focus group reported “I’m on several different medications and they all have to be taken at different times, none of them are taken together. So, it’s really hard for me to stay complaint, especially when I’m trying to go to a job and I have to take my medication during the day and I have to remember too, because I will be working and I forget about it or if I’m like off on a weekend trip or something it is also hard to remember to take it during the day and throughout multiple times during the day.”
Provider Focus Groups
As with the patient focus groups, communication difficulties between patients and providers was a primary theme emerging during the provider focus groups. The need to consider the patient’s definition of medication adherence was a primary theme emerging in the depression provider focus group (n=15 comments). A major concern emerging among multiple providers was the need for patients to take their prescribed medications more consistently. Multiple providers reported that while they view medication adherence as consistently taking medications as prescribed, many patients will report being adherent even if they are not taking their medication consistently. A diabetes provider reported that “some patients can be taking it as prescribed, but then they forget one or two times a week so it’s also hard to know how consistent they are with taking it as prescribed.” Across the diabetes and depression provider focus groups, participants reported needing to assess the patient’s beliefs about their medications to address perceptual barriers to medication adherence. One depression provider reported “facilitating discussions about patient beliefs about medications to see if they need any education … or when they [patients] try to do experiments by themselves not taking meds for few days and see if that works. Education that may be needed in that scenario.” Additionally, providers reported a lack of patient understanding of chronic illness self-management is largely driven by limited health literacy. Providers reported that understanding and addressing the patient beliefs about medication effectiveness is especially important when communicating with patients about medication adherence. Further, intentional non-adherence was reported by participants as being related to patient perceptual barriers including negative patient views about insulin. A diabetes provider reported “practically speaking it [diabetes self-management] takes a lot of work, it takes time, it’s not like giving them a shot of insulin and your sugar comes down.” A depression provider reported that because depression medications take a while to become fully effective, patients become frustrated and intentionally non-adherent. One provider reported “I frequently teach patients that of all the things that we treat in psychiatry – depression tends to get better the slowest. They [patients] sometimes seem frustrated because they see patients who come into the hospital looking a whole lot sicker than they are, get better much faster and do not stay as long. Hence, we have to talk about unfortunately slow road to recovery with depression.” Providers reported that it is also necessary to inquire about concerns about side effects when discussing the medication adherence to address intentional medication non-adherence. A psychiatrist in the depression provider focus group reported “one of the reasons that patients stop medications is because of unwanted side-effects, so I would say that I ask every patient every day if they have any problems with the medication which is a larger question than just the side effects. That’s kind of a little bit of an assessment about how they think about compliance.” A theme emerged among providers across the focus groups about needing to also discuss practical barriers to medication adherence such as forgetting to take prescribed medications, to understand the patient’s definition of medication adherence and to prevent unintentional non-adherence. Across provider focus groups, participants expressed concerns about the impact of polypharmacy on unintentional medication non-adherence. A depression provider reported “I also feel like it’s a failure on our part too to not start to remove medications to combat polypharmacy … because … I feel like we are many times too quick to throw another medication on top of somebody who is complaining of this symptom or illness or this or that, rather than doing more investigation of what could be causing that.” SDoH were also identified by providers as drivers of unintentional medication non-adherence. The primary SDoH identified across provider focus groups as barriers to medication adherence included medication costs and lack of transportation. A diabetes provider reported that adherence is related to “the cost of medication, certain patients can’t get them [medications] from the pharmacy and they don’t pick them up … they’ll show up four months later. then [provider asks] why didn’t you call us and let us know … was it a side-effect for which you didn’t get it? so I think that [SDoH] plays big into [non-adherence] and of course their high blood sugar four months later is still high, because they didn’t follow or at least contact us and let us know that they couldn’t get those things.”
Across All Focus Groups
Across focus groups, patient and provider communication difficulties emerged as a primary barrier to medication adherence. Depression providers suggested several corrective measures for reducing communication barriers including engaging in positive communication with patients using the patient’s own words, obtaining detailed information about patient medication use, and avoiding being accusatory during adherence discussions. Additional themes emerging across focus groups were related to a perceived link between poor health literacy and medication non-adherence and the need for better patient education. Multiple patient participants suggested a shared decision-making approach is needed that explains the benefits and risks of treatment and includes education on how to take prescribed medication and what to expect. Another major theme that emerged was a lack of understanding of how medication adherence is defined, with multiple participants in the patient focus groups reporting that they were not fully adherent with medication, with some patients reporting they would skip doses to save money. While medication adherence is defined in research as taking 80% or more of the prescribed medication doses,21 focus group participants were not able to agree on a way to quantify medication adherence. Concerns about medication side effects were described across focus groups as a perceptual barrier resulting in intentional medication non-adherence. Both patients and providers discussed practical barriers to medication adherence driven by SDoH resulting in unintentional medication non-adherence, including medication costs and housing instability. Additional practical barriers related to forgetting to take medications and polypharmacy also emerged as major themes associated with unintentional medication non-adherence. The combined focus group results are shown in Figure 1.
Contrasting Themes
Several contrasting themes emerged between the focus groups. Among diabetes patients and providers, the need to incorporate healthy lifestyle changes such as diet and exercise along with medication adherence emerged as a theme but was not mentioned the depression patient and provider focus groups. Additionally, among patients with diabetes and diabetes providers, discussions around the need to address patient-provider language barriers also emerged. Interestingly, patient-provider trust emerged as a theme among patients diagnosed with depression and diabetes providers. Disagreements about medication dosing emerged as a theme among patients diagnosed with depression, but did not emerge as a theme among patients with diabetes. While symptom control emerged as a theme among patients with diabetes, this theme did not emerge among patients diagnosed with depression. While perceptual barriers related to concerns about medication effectiveness were themes emerging among patients diagnosed with depression and diabetes, as well as depression providers, this theme did not emerge among diabetes providers.
Discussion
A major theme emerging from the focus group data was the need for improving patient - provider communication to reduce medication non-adherence, which is consistent with prior research.30–33 A major theme emerging across patient focus groups was related to health literacy barriers, specifically not understanding their doctors’ instructions on how to take their medications as prescribed, not understanding how long it would take for medications to become effective, or not knowing what side effects to expect from the medication. Health literacy, or the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions, has been associated with worse glycemic control and complications in patients with type 2 diabetes.34,35 Research has also found poorer antidepressant adherence among adults with diabetes and shown that health literacy limitations may jeopardize the continuation and maintenance phases of depression pharmacotherapy.36 Multiple participants in the provider focus groups reported that evidence-based patient education approaches such as Teach Back are needed to improve medication adherence,33 which underscores the importance of efforts to address health literacy and simplify health communications regarding treatment options.36 Across focus groups, a theme also emerged indicating a lack of agreement as to how partial adherence is conceptualized by patients or providers, which may have made discussions and documentation of adherence difficult. Depression providers in particular suggested a need for providers to consider the patient’s definition of medication adherence and use a more consistent, patient-centered communication strategy to better address medication non-adherence.
Intentional Non-Adherence
Across focus groups, medication ineffectiveness was a major theme that emerged related to intentional medication non-adherence. As pointed out by depression providers, this finding may be related to the longer length of time required for depression medication to become effective. Another major theme reported across the patient focus groups was concerns about medication side effects, which according to patients, results in intentional medication non-adherence. Medication side effects (or the fear of side effects) have been shown to be a major treatment related barrier to medication adherence,21 and participants across the patient focus groups reported that their providers were not adequately explaining the benefits versus side effects of different treatment options. This is a particularly salient finding as healthcare operates with a high degree of information asymmetry, where patients often lack knowledge to evaluate the benefits and side effects of treatment.37 Research has found that shared decision making (SDM), a model of interaction between providers and patients in which both participants contribute to the medical decision-making process, and the provider explains the benefits and risks of each treatment option, improves medication adherence.38 Further, qualitative research has found that patient education efforts, physician training in interpersonal skills, and efforts to engage patients in SDM may positively impact mistrust of physicians in racial/ethnic minority populations and help improve medication adherence and diabetes outcomes.39 Among diabetes providers, intentional non-adherence was reported as being related to patient perceptual barriers including negative patient views about insulin. Perceptual factors refer to factors arising primarily from internal cognitive processes, such as motivation, emotions, or patient perceptions and beliefs of the illness and treatment,40 and have been quantified through the use of the Beliefs about Medicines questionnaire.41 A systematic review and meta-analysis showed medication non-adherence was predicted by doubts about the necessity for treatment (necessity beliefs) and concerns about adverse effects (concerns).20 Hence, given that perceptual barriers are important factors influencing intentional non-adherence, provider communication using a SDM framework should address patient beliefs about the necessity for long-term medication as well as concerns about potential side effects.40
Unintentional Non-Adherence
Across the patient focus groups, practical adherence barriers emerged as major themes both among patients and providers. Research has shown that even if patients intend to take their medication as prescribed, they may be prevented from doing so by limitations in capacity or resources such as deficiencies in memory or access to medicines.42,43 Among practical barriers, forgetfulness emerged as a reason for unintentional medication non-adherence across patient and provider focus groups, which has been consistently found to be one of the most common reasons for non-adherence.44–47 Research supports the use of individually tailored environmental supports such as signs, alarms, calendars, checklists, and notebooks to record questions for their prescriber, organization of belongings, and pill containers to improve medication adherence.48 Research also supports the use of devices such as the Med-eMonitor (MM), where treatment consists of an MM therapist programming prescribing information into MM device, setting up the device in the home to fit into the patient’s routine (eg, set alarm to take medication about 30min after waking, place in a location where he/she is likely to hear the alarm, etc.), assisting the patient in accurately filling the device, training the patient how to use the device and providing ongoing trouble shooting.48–51 Practical barriers related to SDoH, including the cost of medications and housing instability, also emerged as themes related to unintentional medication non-adherence. Accordingly, addressing SDoH may be a particularly important strategy for improving medication adherence among patients with depression and/or diabetes who are medically underserved. Polypharmacy, a prescribing issue linked to increasing rates of medication non-adherence and patient confusion due to the high pill burden and complex administration requirements,52 was identified across focus groups as a risk factor for unintentional medication non-adherence. This finding has important implications as prior research has associated unintentional medication non-adherence with the receipt of higher numbers of medications among community dwelling people with type 2 diabetes.53 Innovative methods are needed to reduce polypharmacy to improve medication adherence among patients with chronic conditions such as depression and/or diabetes. For example, the feasibility of a novel stereolithographic (SLA) 3D printing method has been established for fabricating multi-layer constructs (polypills) to reduce polypharmacy.54 The findings of this study elucidate multiple practical barriers to medication adherence among patients with depression and/or diabetes. While adherence research has primarily focused on perceptual factors, the identification of practical factors driving medication non-adherence is increasingly being recognized as important for targeted interventions as practical factors are often more easily amenable to changes in the physical environment compared to perceptual barriers.40
Clinical and Policy Implications
A major theme emerging from the focus groups was the need to improve patient-provider communication to address medication non-adherence, which has clinical and policy implications for improving healthcare practice and policy. Training physicians in communication skills has been shown to result in substantial and significant improvements in patient adherence such that with physician communication training, the odds of patient adherence are 1.62 times higher than when a physician receives no training.30 Accordingly, this study provides support for providing communication training for physicians and other healthcare providers to improve medication adherence. Both the perceptual and practical barriers to medication adherence identified in the study point to a need for a need for tailored, multi-component interventions, which may require both healthcare and reimbursement system changes.
Strengths and Limitations
A strength of this study includes the diverse group of focus group participants and settings. Additionally, the use of intentional and unintentional medication non-adherence as a comprehensive framework for examining patient and provider perspectives is another strength of this study, as it expands current research in this area. A possible limitation includes the inclusion of focus group facilitators and participants as study co-authors. However, we believe this approach allowed for member checking to ensure focus group themes were adequately identified and interpreted. Additionally, an international medication adherence expert, D.V., and PCORI study co-investigator, E.B., were included as manuscript co-authors (who did not participate in the focus groups) to independently review the focus group transcripts and interpret and provide feedback on the qualitative findings.
Conclusion
Across focus groups, perceptual and practical barriers to medication adherence as well as patient and provider communication difficulties were major themes that emerged. The findings from this study contribute to a long line of research showing improved communication to be highly correlated with better patient medication adherence, suggesting health care systems should prioritize improving patient-provider communication. Additionally, perceptual barriers resulting in intentional medication non-adherence included beliefs about medication effectiveness and concerns about side effects. The study findings point to a need to better address SDoH to reduce multiple practical barriers to medication adherence. Participants suggested important targets for adherence interventions to reduce practical barriers faced by underserved populations including medication costs and transportation. The study findings also suggest a need for innovative, multi-component interventions to address additional practical barriers to medication adherence that are common among persons with depression and/or diabetes including forgetting to take prescribed medication and polypharmacy.
Disclosure
Dr Eduardo Blanco reports grants from Patient-Centered Outcomes Research Institute, during the conduct of the study. Dr Dawn Velligan reports personal fees from Otsuka Pharmaceuticals, personal fees from Janssen Pharmaceuticals, personal fees from Teva Pharmaceuticals, personal fees from Alkermes, personal fees from Lyndra Pharmaceuticals, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
2. Peterson AM, Takiya L, Finley R. Meta-analysis of trials of interventions to improve medication adherence. Am J Health Syst Pharm. 2003;60:657–665. doi:10.1093/ajhp/60.7.657
3. Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2008;2008:CD000011.
4. Viswanathan M, Golin CE, Jones CD, et al. Interventions to improve adherence to self-administered medications for chronic diseases in the United States: a systematic review. Ann Intern Med. 2012;157(11):785–795. doi:10.7326/0003-4819-157-11-201212040-00538
5. Cramer JA. A systematic review of adherence with medications for diabetes. Diabetes Care. 2004;27(5):1218–1224. doi:10.2337/diacare.27.5.1218
6. Aronson BD, Sittner KJ, Walls ML. The mediating role of diabetes distress and depressive symptoms in type 2 diabetes medication adherence gender differences. Health Educ Behav. 2020;47(3):474–482. doi:10.1177/1090198119885416
7. Gonzalez JS, Peyrot M, McCarl LA, et al. Depression and diabetes treatment nonadherence: a meta-analysis. Diabetes Care. 2008;31(12):2398–2403. doi:10.2337/dc08-1341
8. Edward A, Campbell B, Manase F, Appel LJ. Patient and healthcare provider perspectives on adherence with antihypertensive medications: an exploratory qualitative study in Tanzania. BMC Health Serv Res. 2021;21(1):834. doi:10.1186/s12913-021-06858-7
9. van Boven JF, Stuurman-Bieze AG, Hiddink EG, Postma MJ, Vegter S. Medication monitoring and optimization: a targeted pharmacist program for effective and cost-effective improvement of chronic therapy adherence. J Manag Care Pharm. 2014;20(8):786–792. doi:10.18553/jmcp.2014.20.8.786
10. Kangovi S, Mitra N, Grande D, et al. Patient-centered community health worker intervention to improve posthospital outcomes: a randomized clinical trial. JAMA Intern Med. 2014;174(4):535–543. doi:10.1001/jamainternmed.2013.14327
11. Bosworth HB, Fortmann SP, Kuntz J, et al. Recommendations for providers on person-centered approaches to assess and improve medication adherence. J Gen Intern Med. 2017;32(1):93–100. doi:10.1007/s11606-016-3851-7
12. Hodges JR, Phillips SM, Norell S, et al. Intentional and unintentional nonadherence to hydroxyurea among people with sickle cell disease: a qualitative study [published correction appears in Blood Adv. 2020 Oct 13;4(19):4822]. Blood Adv. 2020;4(18):4463–4473. doi:10.1182/bloodadvances.2020001701
13. Lehane E, McCarthy G. Intentional and unintentional medication non-adherence: a comprehensive framework for clinical research and practice? A discussion paper. Int J Nurs Stud. 2007;44(8):1468–1477. doi:10.1016/j.ijnurstu.2006.07.010
14. Fan JH, Lyons SA, Goodman MS, Blanchard MS, Kaphingst KA. Relationship between health literacy and unintentional and intentional medication nonadherence in medically underserved patients with type 2 diabetes. Diabetes Educ. 2016;42(2):199–208. doi:10.1177/0145721715624969
15. Clifford S, Barber N, Horne R. Understanding different beliefs held by adherers, unintentional non-adherence, and intentional non-adherers: application of the necessity–concerns framework. J Psychosom Res. 2008;64:41–46. doi:10.1016/j.jpsychores.2007.05.004
16. Lowry KP, Dudley TK, Oddone EZ, Bosworth HB. Intentional and unintentional nonadherence to antihypertensive medication. Ann Pharmacother. 2005;39(7–8):1198–1203. doi:10.1345/aph.1E594
17. DiMatteo MR. Variations in patients’ adherence to medical recommendations: a quantitative review of 50 years of research. Med Care. 2004;42(3):200–209. doi:10.1097/01.mlr.0000114908.90348.f9
18. DiMatteo MR, Haskard-Zolnierek KB, Martin LR. Improving patient adherence: a three-factor model to guide practice. Health Psychol Rev. 2012;6:74–91.
19. French DP, Wade AN, Farmer AJ. Predicting self-care behaviours of patients with type 2 diabetes: the importance of beliefs about behaviour, not just beliefs about illness. J Psychosom Res. 2013;74:327–333. doi:10.1016/j.jpsychores.2012.12.008
20. Horne R, Chapman SC, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity–concerns framework. PLoS One. 2013;8:e80633.
21. Kleinsinger F. The unmet challenge of medication nonadherence. Perm J. 2018;22:18–033. doi:10.7812/TPP/18-033
22. Jaam M, Hadi MA, Kheir N, et al. A qualitative exploration of barriers to medication adherence among patients with uncontrolled diabetes in Qatar: integrating perspectives of patients and health care providers. Patient Prefer Adherence. 2018;12:2205–2216. doi:10.2147/PPA.S174652
23. Glaser BG, Strauss AL. The Discovery of Grounded Theory. Strategies for Qualitative Research. Chicago: Aldine; 1967.
24. Glaser BG. Doing Grounded Theory: Issues and Discussions. Mill Valley, CA: Sociology Press; 1998.
25. Powell RA, Single HM. Focus groups. Int J Qual Health Care. 1996;8(5):499–504. doi:10.1093/intqhc/8.5.499
26. Wong LP. Focus group discussion: a tool for health and medical research. Singapore Med J. 2008;49(3):
27. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. doi:10.1191/1478088706qp063oa
28. Gale NK, Heath G, Cameron E, et al. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13:117. doi:10.1186/1471-2288-13-117
29. Birt L, Scott S, Cavers D, Campbell C, Walter F. Member checking: a tool to enhance trustworthiness or merely a nod to validation? Qual Health Res. 2016;26(13):1802–1811. doi:10.1177/1049732316654870
30. Zolnierek KB, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47(8):826–834. doi:10.1097/MLR.0b013e31819a5acc
31. Jolles EP, Clark AM, Braam B. Getting the message across: opportunities and obstacles in effective communication in hypertension care. J Hypertens. 2012;30(8):1500–1510. doi:10.1097/HJH.0b013e32835476e1
32. Roter DL, Hall JA, Aoki Y. Physician gender effects in medical communication: a meta-analytic review. JAMA. 2002;288(6):756–764.
33. Yen PH, Leasure AR. Use and effectiveness of the teach-back method in patient education and health outcomes. Federal Practition. 2019;36(6):284–289.
34. Schillinger D. Association of health literacy with diabetes outcomes. JAMA. 2002;288(4):475. doi:10.1001/jama.288.4.475
35. Nielsen-Bohlman L, editor. Institute of Medicine (U.S.) Health Literacy: A Prescription to End Confusion. Washington, D.C: National Academies Press; 2004.
36. Bauer AM, Schillinger D, Parker MM, et al. Health literacy and antidepressant medication adherence among adults with diabetes: the diabetes study of Northern California (DISTANCE). J Gen Intern Med. 2013;28(9):1181–1187. doi:10.1007/s11606-013-2402-8
37. Upadhyai R, Jain AK, Roy H, Pant V. Participants’ perspectives on healthcare service quality in multispecialty hospitals: a qualitative approach. J Health Manag. 2020;22(3):446–465. doi:10.1177/0972063420938471
38. Hopwood M. The shared decision-making process in the pharmacological management of depression. Patient. 2020;13(1):23–30. doi:10.1007/s40271-019-00383-w
39. Peek ME, Gorawara-Bhat R, Quinn MT, Odoms-Young A, Wilson SC, Chin MH. Patient trust in physicians and shared decision-making among African-Americans with diabetes. Health Commun. 2013;28(6):616–623. doi:10.1080/10410236.2012.710873
40. Chan AHY, Cooper V, Lycett H, Horne R. Practical barriers to medication adherence: what do current self- or observer-reported instruments assess? Front Pharmacol. 2020;11:572. doi:10.3389/fphar.2020.00572
41. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
42. Briesacher BA, Gurwitz JH, Soumerai SB. Patients at-risk for cost-related medication nonadherence: a review of the literature. J Gen Intern Med. 2007;22(6):864–871. doi:10.1007/s11606-007-0180-x
43. Garfield S, Clifford S, Eliasson L, Barber N, Willson A. Suitability of measures of self-reported medication adherence for routine clinical use: a systematic review. BMC Med Res Methodol. 2011;11:149. doi:10.1186/1471-2288-11-149
44. Taylor SA, Galbraith SM, Mills RP. Causes of non-compliance with drug regimens in glaucoma patients: a qualitative study. J Ocul Pharmacol Ther. 2002;18(5):401–409. doi:10.1089/10807680260362687
45. Martin LR, Williams SL, Haskard KB, Dimatteo MR. The challenge of patient adherence. Ther Clin Risk Manag. 2005;1(3):189–199.
46. Shubber Z, Mills EJ, Nachega JB, et al. Patient-reported barriers to adherence to antiretroviral therapy: a systematic review and meta-analysis. PLoS Med. 2016;13(11):e1002183. doi:10.1371/journal.pmed.1002183
47. Jamison J, Sutton S, Mant J, De Simoni A. Barriers and facilitators to adherence to secondary stroke prevention medications after stroke: analysis of survivors and caregivers views from an online stroke forum. BMJ Open. 2017;7(7):e016814. doi:10.1136/bmjopen-2017-016814
48. Velligan DI, Diamond PM, Mintz J, et al. The use of individually tailored environmental supports to improve medication adherence and outcomes in schizophrenia. Schizophr Bull. 2008;34(3):483–493. doi:10.1093/schbul/sbm111
49. Velligan DI, Bow-Thomas CC, Huntzinger C, et al. Randomized controlled trial of the use of compensatory strategies to enhance adaptive functioning in outpatients with schizophrenia. Am J Psychiatry. 2000;157(8):1317–1323. doi:10.1176/appi.ajp.157.8.1317
50. Velligan DI, Prihoda TJ, Ritch JL, Maples N, Bow-Thomas CC, Dassori A. A randomized single-blind pilot study of compensatory strategies in schizophrenia outpatients. Schizophr Bull. 2002;28(2):283–292. doi:10.1093/oxfordjournals.schbul.a006938
51. Velligan DI, Gonzalez JM. Rehabilitation and recovery in schizophrenia. Psychiatr Clin North Am. 2007;30(3):535–548. doi:10.1016/j.psc.2007.05.001
52. Payne RA, Avery AJ. Polypharmacy: one of the greatest prescribing challenges in general practice. Br J Gen Pract. 2011;61(583):83–84. doi:10.3399/bjgp11X556146
53. Stack RJ, Bundy CE, Elliott RA, New JP, Gibson M, Noyce PR. Intentional and unintentional non-adherence in community dwelling people with type 2 diabetes: the effect of varying numbers of medicines. Br J Diabetes Vasc Dis. 2010;10(3):148–152. doi:10.1177/1474651409357034
54. Robles-Martinez P, Xu X, Trenfield SJ, et al. 3D printing of a multi-layered polypill containing six drugs using a novel stereolithographic method. Pharmaceutics. 2019;11(6):274. doi:10.3390/pharmaceutics11060274
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.