Back to Journals » Patient Related Outcome Measures » Volume 16
Patient Acceptable Symptom State for the Oxford Elbow Score After Primary Elbow Arthroplasty Due to Acute Distal Humeral Fracture
Authors Nielsen AF ![]() , Nyring MRK, Al-Hamdani A, Thillemann TM, Rasmussen JV, Olsen BS
, Nyring MRK, Al-Hamdani A, Thillemann TM, Rasmussen JV, Olsen BS
Received 12 August 2025
Accepted for publication 6 December 2025
Published 20 December 2025 Volume 2025:16 Pages 215—224
DOI https://doi.org/10.2147/PROM.S547814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Lynne Nemeth
Andreas Falkenberg Nielsen,1,2 Marc Randall Kristensen Nyring,1 Ali Al-Hamdani,1 Theis Muncholm Thillemann,3,4 Jeppe Vejlgaard Rasmussen,1,2 Bo Sanderhoff Olsen1,2
1Shoulder and Elbow Surgery, Herlev and Gentofte Hospital, Hellerup, Denmark; 2Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark; 3Department of Orthopedic Surgery, Aarhus University Hospital, Aarhus, Denmark; 4Department of Clinical Medicine, Aarhus University, Aarhus, Denmark
Correspondence: Andreas Falkenberg Nielsen, Shoulder and Elbow Surgery, Herlev and Gentofte Hospital, Hellerup, Denmark, Email [email protected]; [email protected]
Background: Patient Acceptable Symptom State (PASS) describes the highest level of symptom beyond which patients consider themselves well. PASS can be used to establish what patients’ view as an acceptable outcome after surgery. The Oxford Elbow Score (OES) is one of the most used elbow-specific patient-reported outcome measure (PROM), but a PASS-value has not yet been established for the OES after elbow arthroplasty. The primary purpose of this study was to determine the PASS for the OES after primary elbow arthroplasty due to acute distal humeral fracture.
Methods: This is a retrospective multi-center cohort study. All nationwide patients treated with elbow arthroplasty due to acute distal humeral fracture from January 1, 2008, until December 1, 2021, were invited to participate. Data were collected retrospectively using electronic health records. Study participants answered the OES, and a PASS-anchor question was used to assess if patients were in an acceptable state at follow-up. Logistic modelling was used to determine the PASS-value, defined as the value of OES needed to achieve an acceptable postoperative result with at least 95% probability. A PASS-value was estimated for the total population, for patients with < 5 years of follow-up, and patients with ≥ 5 years of follow-up.
Results: The OES and PASS-anchor was answered by 159 (62%) patients. Median OES was 41 (0– 48) in the total population. One hundred and thirty-nine patients (87%) reported an acceptable result. The 95% PASS-value for the OES was 33 (95% CI 29.6– 38.5) in the total population.
Conclusion: The PASS-value for the OES after elbow arthroplasty due to acute distal humeral fracture was 33 for the total population and similar for patients with short-term and long-term follow-up. We recommend using the PASS-value to aid in interpretation of clinical trials and registry-based studies as well as identifying clinical failures in registries.
Keywords: elbow joint replacement, elbow trauma, fracture management, patient related outcome measures, patient reported outcome measures
Introduction
Patient Reported Outcome Measures (PROMs) are widely used in the assessment of surgical procedures, as they can be used to evaluate and report the subjective experiences of patients undergoing surgery on both the population level, and for individual patients. The Oxford Elbow Score (OES) is an elbow-specific PROM developed to assess outcomes of elbow surgery.1 Although it has not yet been validated in a population of exclusively elbow-trauma patients, it is one of the most widely used elbow-specific PROMs available.2
The Minimal Clinically Important Difference (MCID) is frequently used to define clinically relevant differences in outcome measures when comparing results of surgical treatment in different patient groups.3–5 However, the MCID is difficult to use when preoperative assessment is unavailable, which is usually the case with acute trauma patients. Therefore, when conducting cross-sectional studies with only a single assessment, the Patient Acceptable Symptom State (PASS) might be more appropriate.
The PASS describes the highest level of symptom beyond which patients consider themselves well.6 It defines a threshold score in a PROM, beyond which patients view their condition as acceptable.6,7 This PASS-value can be a valuable aid for researchers and clinicians when interpreting the results of clinical studies, as it helps to identify the level of symptom improvement that provides an acceptable result to patients.6–8 It can also be helpful for clinicians to know the PASS-value for specific conditions and PROM-instruments, when making informed decisions about treatment goals and patient satisfaction. PASS is a concept with emphasis on the current state of the patient, and it can be estimated by use of an anchor question asking the patient if they feel they are in an acceptable state or not.6–8
National clinical registries have shown that the use of total elbow arthroplasty in acute trauma care increased by 15%, when comparing the periods 2000–2009 and 2010–2017,9 but reporting and interpretation of outcomes are not consistent, and no objective threshold for a successful outcome has yet been established. Recent studies have reported long-term revision rates of 13–20%,10,11 which could indicate a tendency for outcomes to deteriorate, leading to inferior long-term results and consequently different PASS-values for patients with short- and long-term follow-up.
The primary purpose of this study was to determine the PASS for the OES in patients having primary elbow arthroplasty due to acute distal humeral fracture. Additionally, we investigated the PASS values at both short- and long-term follow-up.
Methods
The study was developed, conducted, and reported in accordance with the RECORD statement12 (Reporting of studies Conducted using Observational Routinely collected health data).
The study was a national multi-center cross-sectional cohort study. Data were collected retrospectively from the period January 1, 2008, to December 1, 2021. OES and the PASS anchor-question was collected prospectively in the period April 1, 2023, to August 31, 2024.
Inclusion criteria were patients treated in Denmark with primary total elbow arthroplasty (TEA) or hemiarthroplasty (EHA) due to acute distal humeral fracture that cannot be reconstructed with open reduction and internal fixation (ORIF), who had surgery within six weeks of injury. This includes patients who were initially treated with ORIF or non-operatively but had elbow arthroplasty within six weeks of injury. All age-groups were included.
Exclusion criteria were revision in the study period, which was defined as removal, exchange or addition of any arthroplasty component, and isolated radial head arthroplasties, Figure 1. Bilateral arthroplasties were also excluded to avoid issues with dependency when determining the PASS-values.
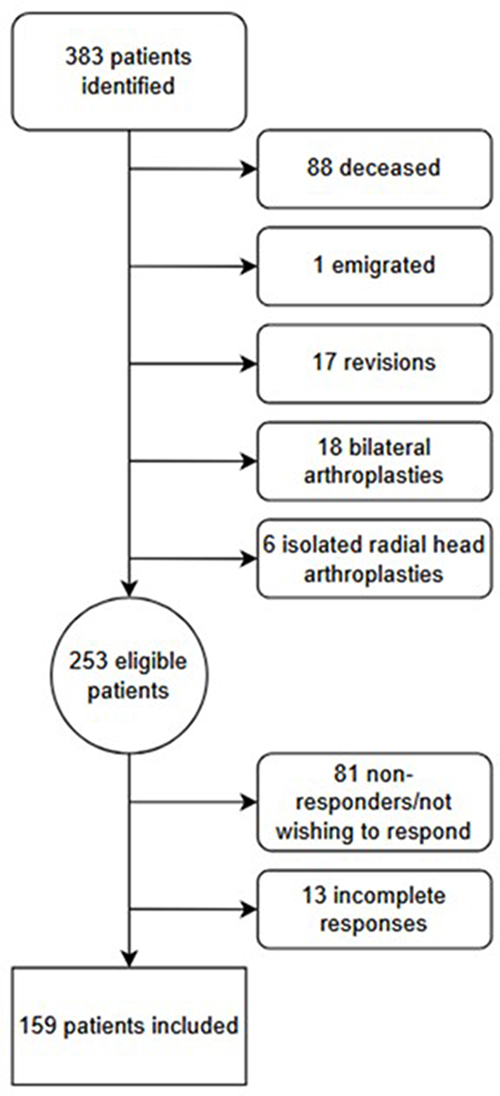 |
Figure 1 Inclusion flowchart. |
Patients were not excluded based on neurological or psychological comorbidities.
Data Collection and Ethical Considerations
In the study period, elbow arthroplasty surgery was exclusively performed at three public university hospitals due to §208 of the 2008 Danish Health Care Act. This made it possible to identify all patients on a national level and to collect data by reviewing individual patient records from these three hospitals.
In the Danish Healthcare System, all surgical procedures are coded using the Danish version of the NOMESCO Classification of Surgical Procedures13 (NCSP). All Danish patients are assigned a unique social security number, which is used to store all health-related information in an electronic health record for all admissions and out-patient contacts. Primary and revision procedures can therefore be linked, regardless of where the procedures were performed. We used the NCSP procedure codes to identify patients who were treated with an elbow arthroplasty. Individual patient health records were then reviewed, and the relevant data were extracted.
Invitations to answer the OES questionnaire and the PASS-anchor question were sent to eligible patients by mail. Patients who did not answer were contacted by telephone to ensure the invitation had been received. Patients accepted the invitation to participate in the study by answering and returning the questionnaire and anchor-question. The questionnaire and anchor-question were completed by the patients without involving surgeons or any other persons with relation to the study.
Ethical review and permission to conduct the study was obtained from the Center for Regional Development in the Capital Region of Denmark, on behalf of The Regional Counsel (journal number R-22028272), as specified in §46, sect. 2 of The Danish Health Act. All procedures were conducted in accordance with the Declaration of Helsinki and Danish regulations for research on human subjects.
License to use the Danish version of the OES14 was obtained from Clinical Outcomes at Oxford University Innovation.
The REDcap15 software was used to create a database hosted at the Capital Region of Denmark, where data were stored and managed in accordance with the General Data Protection Regulation.
Baseline Data and Classification
Data were collected on sex, age, body mass index (BMI), American Society of Anesthesiologists (ASA) score (0–6), time to surgery (days from date of injury), elbow arthroplasty type (TEA or EHA), and elbow arthroplasty brand, Table 1.
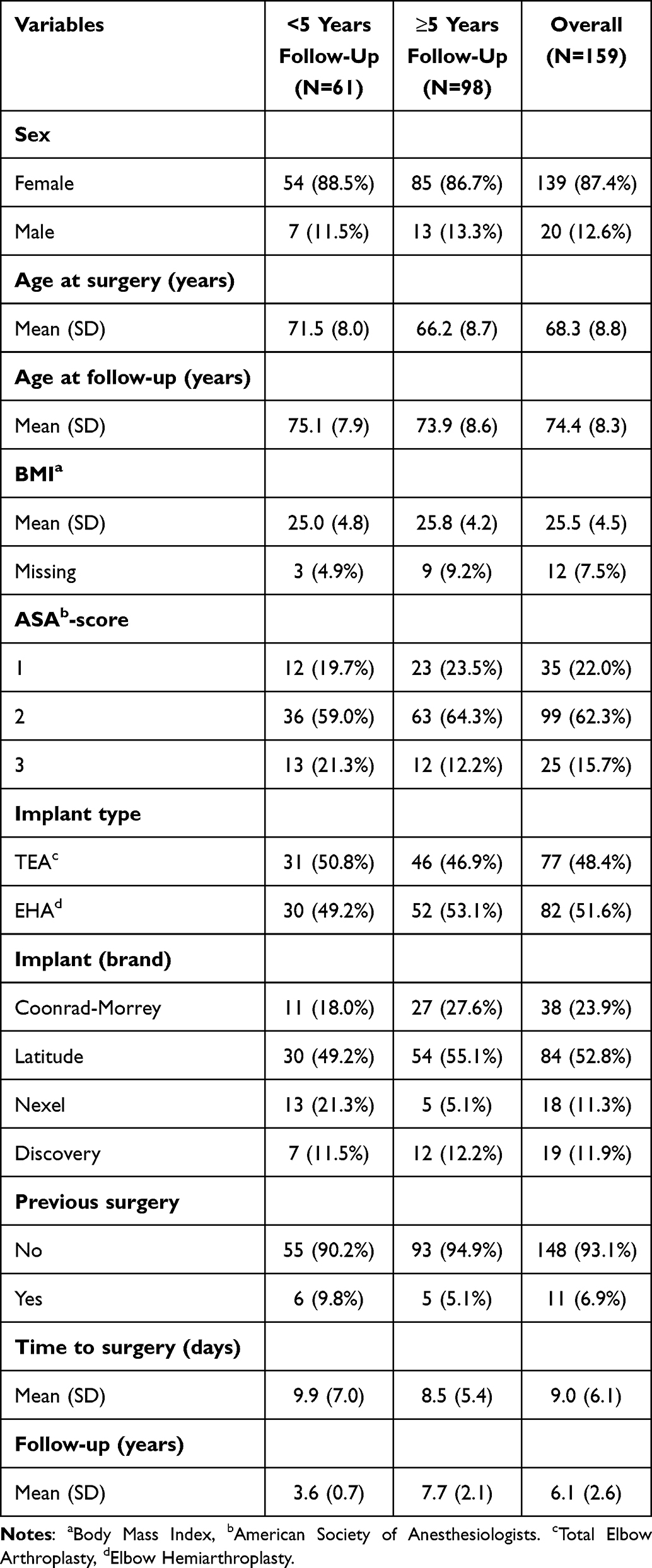 |
Table 1 Baseline Patient Characteristics |
Time to follow-up was defined as the time from surgery to answering the questionnaire.
Outcomes and Statistical Analysis
Patients were grouped as having either < or ≥5 years of follow-up. This was done to both report PASS-values in patients who have not had an elbow arthroplasty for many years (short-term group), and in patients who have had an arthroplasty long enough to reach steady-state and adjust their daily lives to the arthroplasty (long-term group).
The Oxford Elbow Score1 is one of the only PROMs developed specifically for assessing the results of surgery in the elbow.2 It consists of 12 questions equally distributed into three domains: Elbow pain, elbow function, and social-psychological. Patients answer each question from 0 to 4, with 0 representing the worst score. The result is a score from 0 to 48 points, with 48 points representing a fully functioning and pain-free elbow joint.
Tubach et al proposed the following PASS anchor-question:
Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?8
We used a modified version of the anchor-question:
Taking into account all the activities you have during your daily life, your level of pain, and also the functional impairment of your elbow, do you consider that your current state is satisfactory?
It was modified to focus on the elbow and translated to Danish for the purpose of the study. The translation was done by the first author, and reviewed and accepted by the other authors. All authors are fluent in Danish and English. A pilot evaluation of the questionnaire and anchor-question was not done, as this required a degree of patient contact that was not possible in the study.
The 95% PASS-value was defined as the specific value of OES, at which the probability of the patient having answered “yes” on the PASS anchor question was 95%.
A cutoff of 95% probability for PASS was chosen, as 95% significance is the generally accepted cut-off for statistical significance in clinical research.
Logistic modelling was used to determine the 95% PASS for the OES in the total population, and for patients < or ≥5 years of follow-up.
The PASS anchor of yes or no (acceptable or not acceptable result) was used as a binary dependent variable in the logistic models, with the OES as a continuous independent variable.
The cutoff for OES with a 95% probability of being in PASS (the 95% PASS) was then estimated using the logistic regression equation  , with P(Y=1) = 0.95, to estimate the corresponding value of X. This value was then rounded to the nearest integer, representing the OES with at least 95% probability of being in PASS.
, with P(Y=1) = 0.95, to estimate the corresponding value of X. This value was then rounded to the nearest integer, representing the OES with at least 95% probability of being in PASS.
Bootstrap confidence intervals (CI) were then estimated for the PASS-values, with 2000 resamples.
Figures 2–4 visually illustrate the logistic relationship between the PASS anchor-question and the OES for the total population, patients with short-term follow-up, and patients with long-term follow-up.
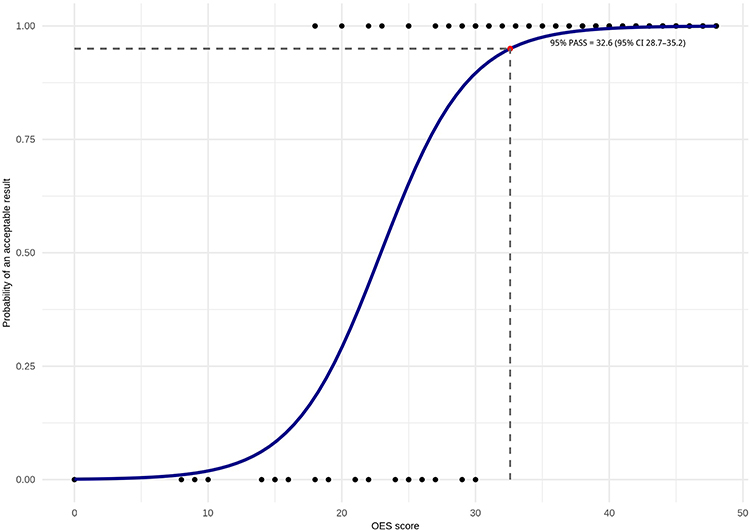 |
Figure 2 Patient acceptable symptom state for the Oxford Elbow Score. All patients with primary elbow arthroplasty due to acute distal humeral fracture. The Y-axis shows the probability of the patient having answered yes (acceptable result) on the PASS anchor-question. The X-axis shows continuous values of the OES. The black dots in the bottom show answered values for patients having answered no (unacceptable result) on the PASS anchor-question. Black dots in the top show answered values for patients having answered yes (acceptable result) on the PASS anchor-question. The blue line represents the logistical regression curve. The red dot (95% PASS) represents the cutoff for PASS where the probability of patients having achieved an acceptable result is at least 95%. |
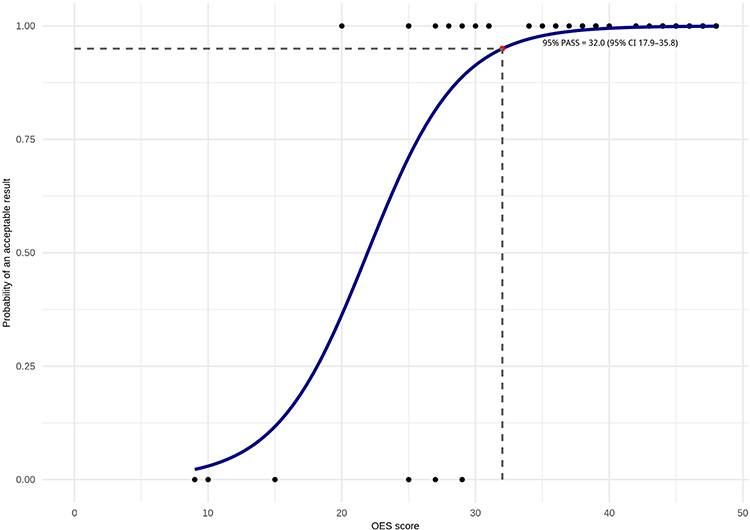 |
Figure 3 Patient acceptable symptom state for the Oxford Elbow Score. Primary elbow arthroplasty due to acute distal humeral fracture - < 5 years follow-up. The Y-axis shows the probability of the patient having answered yes (acceptable result) on the PASS anchor-question. The X-axis shows continuous values of the OES. The black dots in the bottom show answered values for patients having answered no (unacceptable result) on the PASS anchor-question. Black dots in the top show answered values for patients having answered yes (acceptable result) on the PASS anchor-question. The blue line represents the logistical regression curve. The red dot (95% PASS) represents the cutoff for PASS where the probability of patients having achieved an acceptable result is at least 95%. |
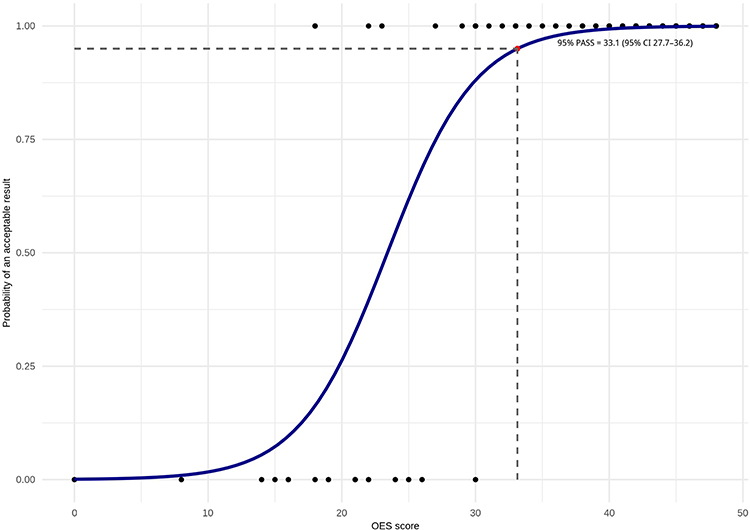 |
Figure 4 Patient acceptable symptom state for the Oxford Elbow Score. Primary elbow arthroplasty due to acute distal humeral fracture - ≥ 5 years follow-up. The Y-axis shows the probability of the patient having answered yes (acceptable result) on the PASS anchor-question. The X-axis shows continuous values of the OES. The black dots in the bottom show answered values for patients having answered no (unacceptable result) on the PASS anchor-question. Black dots in the top show answered values for patients having answered yes (acceptable result) on the PASS anchor-question. The blue line represents the logistical regression curve. The red dot (95% PASS) represents the cutoff for PASS where the probability of patients having achieved an acceptable result is at least 95%. |
The level of significance was set at p = 0.05, and results were reported with confidence intervals.
Statistical analysis was performed in R version 4.4.1.16
Results
Baseline patient characteristics are reported in Table 1. Age at surgery was higher in the short-term follow-up group (Table 1). As the Nexel arthroplasty was introduced in Denmark more recently compared to the other arthroplasties, there were fewer Nexel arthroplasties in the group with long-term follow-up (Table 1). The distribution of TEA and EHA were similar in the two follow-up groups (Table 1).
PASS-Values
The 95% PASS-value for the OES in the total population was 33 (95% CI 28.7–35.2, Figure 2). This indicates that patients with a primary elbow arthroplasty due to acute fracture, who have not had revision surgery, needed an OES of at least 33 to achieve PASS, with 95% certainty. Patients with <5 years of follow-up needed an OES of 32 (95% CI 17.9–35.8, Figure 3) to achieve 95% PASS, and patients with ≥5 years of follow-up needed an OES of 33 (95% CI 27.7–36.2, Figure 4) to achieve 95% PASS.
OES & Acceptable results
OES and acceptability grouped by follow-up are presented in Table 2.
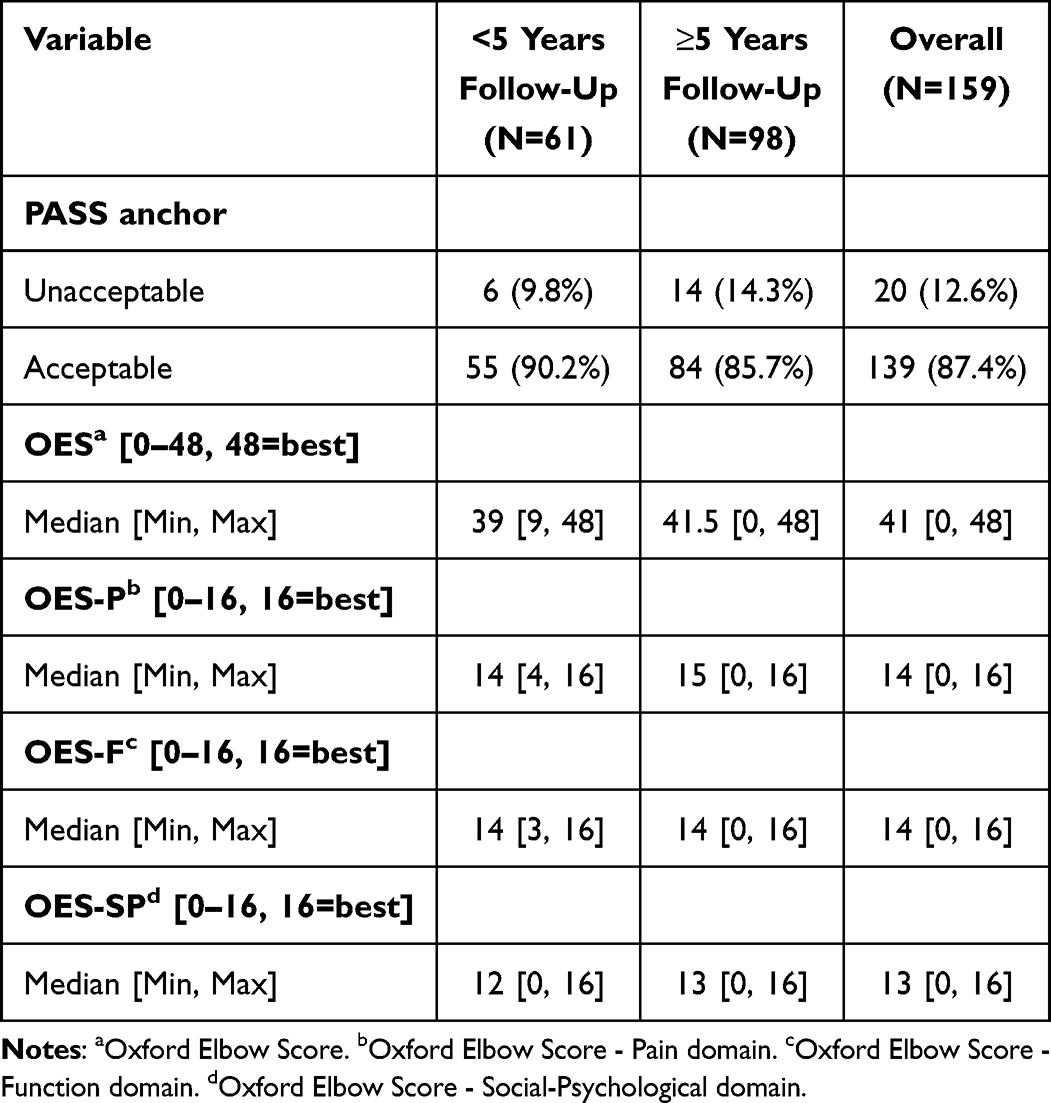 |
Table 2 OES & Acceptable Results Grouped by Follow-Up |
In the total population, 139 patients (87%) answered they had achieved an acceptable result at follow-up.
OES was not normally distributed but skewed towards higher scores and is presented with median and range. Median OES was 41 [0–48] in the total population, 39 [9–48] in the population with <5 years of follow-up, and 42 [0–48] in the population with ≥5 years of follow-up.
OES grouped by acceptable and unacceptable results are presented in Table 3.
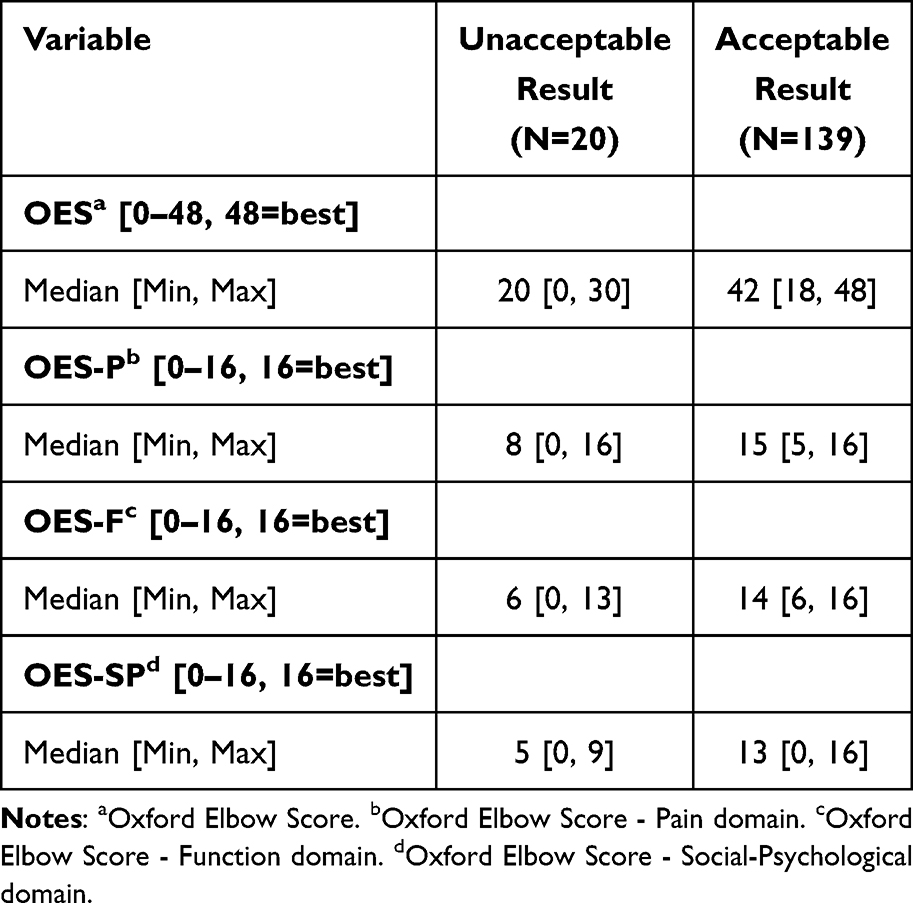 |
Table 3 OES Grouped by Acceptable or Unacceptable Result |
Patients who reported an acceptable result at follow-up had a median OES of 42 [18, 48], whereas patients who reported an unacceptable result had a median OES of 20 [0, 30].
Discussion
The overall PASS-value for the OES in patients with elbow arthroplasty due to acute distal humeral fracture was 33 (95% CI 28.7–35.2). The PASS-values were similar in the short-term and long-term follow-up groups.
To our knowledge, the present study is the only available study reporting a PASS-value for the OES after elbow arthroplasty, and the only available study reporting a PASS-value for the OES using an anchor-based method. The only other available study reporting PASS-values for the OES is based on a population of patients with surgical or non-surgical treatment of lateral epicondylitis.17 The PASS-values were estimated using the 75th-percentile method and Receiver Operating Characteristics (ROC), and the authors report PASS-values for the OES of 81% and 80% of the maximum possible score, corresponding to 38 points on the 0–48 OES. The estimated PASS-value in the present study is five points lower, but the populations and method of estimating the PASS-values are different, which makes comparison difficult. The PASS clinimetric is not commonly used in studies of upper extremity pathologies, and there is currently no consensus on the best method of estimating PASS-values.7,8,18,19 Additional studies reporting PASS-values, and a consensus on the most suitable method would be valuable in future studies to increase comparability.
By modelling the PASS-value based on an anchor-question, the subjective experience of the patient is considered, resulting in a more patient-centered PASS-value. As shown in Table 3, the OES was as low as 18 in the group of patients who reported an acceptable result. This indicates that there is a high degree of subjectivity in patients’ perceptions of an acceptable outcome. The PASS-value can be used to determine the proportion of patients achieving an acceptable outcome when comparing groups of patients. It can also be helpful when assessing the risk of an unacceptable outcome. In registries and cross-sectional studies, the PASS-value can be used as a benchmark for clinical failure or success. In clinical trials, it can be used to interpret the clinical value of the results, as a difference in effect between two treatments might not be clinically relevant, if neither of the treatments succeed in making the patient achieve PASS. The PASS-value might also be used to guide informed decision making and align expectations of treatment in the clinical setting, when considering elbow arthroplasty for an acute distal humeral fracture.
The PASS-value does not quantify the effect size of treatment but provides a threshold for what patients view as an acceptable outcome.7,8 It also has the benefit of not needing a preoperative assessment, which is difficult to obtain for acute fractures. Asking patients to rate their current elbow between injury and surgery to obtain a preoperative score seems unreliable and introduces recall bias, especially for patients with a pre-injury normal elbow function, and when conducting mid- or long-term follow-up. These limitations can be eliminated by focusing on the current state and whether this is acceptable for the patient, as is the case with PASS.
In this study, the PASS-values for the OES were similar for patients with short- and long-term follow-up. This indicates that patients need approximately the same OES to achieve an acceptable result, regardless of follow-up time. The result was acceptable for 87% and unacceptable for 13%, but the proportion of patients with unacceptable outcomes may be higher, as this study does not include revision patients. As shown in Figure 1, 17 (4%) of the 383 identified patients were excluded due to revision surgery. It is currently unclear if revision arthroplasty leads to inferior results compared to primary elbow arthroplasty, but the identified amount of revision arthroplasty patients was too small for a separate analysis.
Strengths and Limitations
This study reports the first PASS-value for the OES after elbow arthroplasty due to acute fracture, in a large population of patients with both short-term and long-term follow-up. There are no established gold-standard for estimating PASS-values, and to our knowledge the PASS-concept is not widely used. It is therefore debatable which method for estimating PASS-values is the most appropriate, and only using an anchor-based method for estimating the PASS-value might be a limitation of the study. The anchor-based PASS-value reported in this study is estimated by logistic modelling of the anchor-question and the OES. This method is patient-centered and based on statistical modelling, and therefore not relying on the judgement of clinicians or researchers to determine the cut-off for PASS, but it also makes adjusting for confounding or interaction of other variables difficult, as the estimated PASS-value changes with the number of coefficients in the model. When additional β-coefficients are added to the regression equation, the resulting value of X, which represents the PASS-value, changes (see Methods section). This would make interpretation of the output difficult and is a limitation. Additionally, a pilot evaluation of the questionnaire and anchor-question was not practically possible, as this would require a degree of patient contact, which was not possible in the present study. This is also a limitation of the study, as feedback from relevant patients could provide valuable information regarding the precision and comprehensibility of the questionnaire and PASS anchor-question.
Conclusion
The PASS-value for the OES after elbow arthroplasty due to acute distal humeral fracture was 33 for the total population and similar for patients with short-term and long-term follow-up. We recommend using the PASS-value to aid in interpretation of clinical trials and registry-based studies as well as identifying clinical failures in registries, and in aligning the expectations of patient and surgeon when considering elbow arthroplasty for acute distal humeral fracture.
Disclosure
Dr Nielsen, Dr Nyring, Dr Al-Hamdani, and Dr Thillemann: These authors, their immediate family, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article.
Dr Rasmussen reports the following:
Research support from Depuy/Synthes, Johnson and Johnson, and Zimmer/Biomet.
All of the declarations are without relation to the submitted work.
Dr Olsen reports the following:
Research support from Depuy/Synthes and Zimmer/Biomet.
Speaker fee from Swemac.
All of the declarations are without relation to the submitted work.
References
1. Dawson J, Doll H, Boller I, et al. The development and validation of a patient-reported questionnaire to assess outcomes of elbow surgery. J Bone Joint Surg B. 2008;90(4):466–473. doi:10.1302/0301-620X.90B4.20290
2. Buchanan TR, Lamprecht CB, Bindi VE, et al. Reported outcome measures in total elbow arthroplasty: a systematic review. Semin Arthroplasty. 2025;35:263–269. doi:10.1053/j.sart.2025.03.007
3. Docter S, Fathalla Z, Lukacs MJ, et al. Interpreting patient-reported outcome measures in orthopaedic surgery. J Bone Joint Surg. 2021;103(2):185–190. doi:10.2106/JBJS.20.00474
4. Jeyaraman N, Jeyaraman M, Ramasubramanian S, Balaji S, Muthu S. Beyond statistical significance: embracing minimal clinically important difference for better patient care. World J Methodol. 2025;15(1):97814. doi:10.5662/WJM.V15.I1.97814
5. Jaeschke R, Singer J, Guyatt GH. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989;10:407–415. doi:10.1016/0197-2456(89)90005-6
6. Kvien TK, Heiberg T, Hagen KB. Minimal clinically important improvement/difference (MCII/MCID) and patient acceptable symptom state (PASS): what do these concepts mean? Ann Rheum Dis. 2007;66(SUPPL. 3):40–42. doi:10.1136/ard.2007.079798
7. Pham T, Tubach F. Patient acceptable symptomatic state (PASS). Joint Bone Spine. 2009;76(4):321–323. doi:10.1016/j.jbspin.2009.03.008
8. Tubach F, Dougados M, Falissard B, Baron G, Logeart I, Ravaud P. Feeling good rather than feeling better matters more to patients. Arthritis Care Res. 2006;55(4):526–530. doi:10.1002/ART.22110
9. Macken AA, Prkic A, Kodde IF, Lans J, Chen NC, Eygendaal D. Global trends in indications for total elbow arthroplasty: a systematic review of national registries. EFORT Open Rev. 2020;5(4):215–220. doi:10.1302/2058-5241.5.190036
10. Nielsen AF, Thillemann TM, Al-Hamdani A, Jacobsen PK, Rasmussen JV, Olsen BS. Total elbow arthroplasty versus hemiarthroplasty for acute distal humeral fractures: a retrospective cohort study of revision rates in 366 consecutive patients. J Shoulder Elbow Surg. 2025;34:2596–2603. doi:10.1016/J.JSE.2025.02.034
11. Taylor F, Page R, Wheeler J, et al. Distal humeral hemiarthroplasty compared to total elbow replacement for distal humeral fractures: a registry analysis of 906 procedures. J Shoulder Elbow Surg. 2023:1–10. doi:10.1016/j.jse.2023.08.001
12. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):1–22. doi:10.1371/journal.pmed.1001885
13. Nordic Medico-Statistical Committee. NOMESCO classification of surgical procedures. 1.16. Nordic Centre for Classifications in Health Care; 2011.
14. Plaschke HC, Jørgensen A, Thillemann TM, Brorson S, Olsen BS. Validation of the Danish version of the Oxford elbow score. Dan Med J. 2013;60(10):2–5.
15. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019:95. doi:10.1016/j.jbi.2019.103208
16. R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing; 2024. Available from: https://www.r-project.org/.
17. Karjalainen T, Lähdeoja T, Salmela M, et al. Minimal important difference, patient acceptable symptom state and longitudinal validity of Oxford elbow score and the quickDASH in patients with tennis elbow. BMC Med Res Methodol. 2023;23(1). doi:10.1186/s12874-023-01934-4
18. Tubach F, Wells GA, Ravaud P, Dougados M. Minimal clinically important difference, low disease activity state, and patient acceptable symptom state: methodological issues. J Rheumatol. 2005;32(10):2025–2029.
19. Terle PM, Peebles LA, Verma A, Kraeutler MJ. Minimal clinically important difference, substantial clinical benefit, and patient acceptable symptom state values after hip arthroscopy for femoroacetabular impingement are highly dependent on their study population and calculation methods: a systematic review. Arthroscopy. 2025;41(6):2105–2113. doi:10.1016/j.arthro.2024.07.032
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.