Back to Journals » Breast Cancer: Targets and Therapy » Volume 12
Pathological Complete Response with Neoadjuvant Trastuzumab Combined with Chemotherapy in HER2 Positive Breast Cancer: A Single Institution Retrospective Analysis from Vietnam
Authors Phung HT, Thi Nguyen H, Nguyen TV, Nguyen TV ![]() , Dinh LAT, Nguyen CV
, Dinh LAT, Nguyen CV ![]()
Received 18 June 2020
Accepted for publication 18 August 2020
Published 7 October 2020 Volume 2020:12 Pages 117—122
DOI https://doi.org/10.2147/BCTT.S268369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Huyen Thi Phung,1 Hoa Thi Nguyen,1 Tung Van Nguyen,1 Tai Van Nguyen,2 Lan Anh Thi Dinh,3 Chu Van Nguyen4
1Department of Medical Oncology 6, National Cancer Hospital of Vietnam, Hanoi, Vietnam; 2Department of Medical Oncology 1, National Cancer Hospital of Vietnam, Hanoi, Vietnam; 3Department of Optimal Therapy, Quan Su Campus, National Cancer Hospital of Vietnam, Hanoi, Vietnam; 4Department of Pathology, National Cancer Hospital of Vietnam, Hanoi, Vietnam
Correspondence: Tung Van Nguyen Department of Medical Oncology 6
National Cancer Hospital of Vietnam, 30 Cau Buou, Thanh Tri, Hanoi 134821, Vietnam
Tel +84 912353930
Fax +84 904690818
Email [email protected]
Purpose: Neoadjuvant regimens containing trastuzumab and chemotherapy were widely used in human epidermal growth factor 2 (HER2) positive breast cancer patients. In this article, we report complete pathological response (pCR) rates from a single institution in Vietnam.
Patients and Methods: Medical records of HER2 positive breast cancer patients who received neoadjuvant treatment with trastuzumab combined with chemotherapy were reviewed. Information on patient demographics, breast cancer stage, pathology reports, surgical data, and treatment regimens were collected. Pathological response was evaluated using Chevallier’s criteria, in which complete pathological response was defined as yT0yN0 or yTisN0.
Results: Thirty-nine eligible breast cancer patients treated with chemo-trastuzumab combined regimens in a neoadjuvant setting at Vietnam National Cancer Hospital were included in the analysis. Median age was 47 (range 32– 72 years). Of these 39 patients, 5 (12.8%) were at stage II and 34 (87.2%) were at stage III. Median tumor size was 5.8 cm. There were 22 (56.4%) and 17 (43.6%) patients who had hormone receptor (HR) negative and positive diseases, respectively. Pathological complete response in the breast was demonstrated in 30 out of 39 (76.9%) patients. Of 35 patients with lymph nodal involvement, axillary pCR occurred in 25 (71.4%) patients. Total pathological complete response (tpCR) was achieved in 25 (64.1%) of the evaluated patients. There was no significant association between pathological response rates and age, tumor grade, hormone receptor status, and Ki-67 expression.
Conclusion: Neoadjuvant treatment with trastuzumab and chemotherapy combined in patients with HER2 positive breast cancer yielded a pathological complete response rate of 64.1%.
Keywords: pathological response, neoadjuvant, breast cancer, trastuzumab, chemotherapy
Introduction
The beneficial role of neoadjuvant chemotherapy in locally advanced breast cancer has been demonstrated in many phase III trials.1,2 Traditionally, the benefit of neoadjuvant treatment is to convert inoperable tumors to operable. However, preoperative chemotherapy has been increasingly used in operable breast cancer, especially in patients with unfavorable breast tumors to increase the conservative surgery opportunity, and ultimately increase survival.1 Patients with adverse factors were found to benefit most from neoadjuvant treatment as found in a study conducted by Von Minckwitz et al in 2012.3 Unfavorable features of breast cancer recurrence are HER2 expression, hormone receptor negative (ER and PR negative), and high-grade tumors.
Pathological complete response (pCR) has been used as a surrogate end point for disease-free survival and overall survival in assessing the efficacy of neoadjuvant treatment in breast cancer. In a metanalysis by Mieog and van der Hage in 2007 that included 14 trials comparing neoadjuvant with adjuvant chemotherapy in some 5500 operable breast cancer patients, the risk of death in those who achieved pCR was half of those who did not.4 In 2012, the US Food and Drug Administration (FDA) issued a guideline for approval of neoadjuvant drugs in breast cancer and pCR (ypT0/is, ypN0) was proposed to be used as a surrogate end point for survival.5 The German Breast Group required pCR to be no residual disease in both breast and axilla, including in situ disease (ypT0, ypN0).6 However, there seemed to not be a significant difference between these two criteria, in terms of predictive value of survival benefit.
In the FDA guideline, total pCR was defined as “the absence of invasive disease in the breast and axilla”, meaning “ypT0/is, ypN0” as described by Chevallier’s criteria. This definition was used in subsequent analysis and found to be correlated better with disease-free survival (with HR of 0.48; 95% CI [0.33 to 0.69]) and overall survival (with HR of 0.48; 95% CI [0.37 to 0.63]) when compared with those who had residual disease at pathological examination.4
The benefit of adding an anti-HER2 agent into neoadjuvant treatment protocols for HER2 positive breast cancer has been confirmed in the NOAH trial, which enrolled 235 HER2 positive, locally advanced, or inflammatory breast cancer patients to compare trastuzumab combined with chemotherapy versus chemotherapy alone. At 5.4 years of follow-up, the regimen containing trastuzumab significantly improved EFS when compared with chemotherapy alone with a hazard ratio of 0.64 (95% CI: 0.44–0.93).2
In Vietnam, standard of care regimens for neoadjuvant treatment of HER2 positive breast cancer are AC-TH (4 cycles of dose-dense doxorubicin/cyclophosphamide followed by 12 weeks of paclitaxel/trastuzumab or 4 cycles of taxane/trastuzumab) or TCH (6 cycles of taxane/carboplatin/trastuzumab). These regimens are also endorsed by the National Comprehensive Cancer Network guidelines (NCCN).7 Here, we report the pathological response result of a retrospective analysis of stage II and III HER2 positive Vietnamese breast cancer patients treated with trastuzumab combined with AC-TH or TCH protocols.
Patients and Methods
This retrospective analysis included stage II or III HER2 positive, operable or inoperable breast cancer patients, treated preoperatively with trastuzumab–chemotherapy combined at the National Cancer Hospital of Vietnam, during 5 years from 2013 to 2018. Core needle biopsy was used to confirm malignant diagnosis. Clinical staging was performed by the treating physician at the initial visits using clinical examination of the breast and axillary nodes, in combination with imaging results from ultrasound and mammography. Magnetic resonance imaging was used if the patient initially opted for conservative surgery.
In terms of treatment protocols, we included only patients who were treated with AC-TH or TCH regimens. Patients treated with the AC-TH regimen received 4 cycles of dose-dense AC (60 mg/sqm doxorubicin and 600 mg/sqm cyclophosphamide) every 2 weeks with granulocyte colony-stimulating factor support, followed by weekly paclitaxel 80 mg/sqm+trastuzumab for 12 weeks or docetaxel 100 mg/sqm+trastuzumab every 3 weeks. The patients treated with the TCH protocol received 6 cycles of 175 mg/sqm paclitaxel or docetaxel 75 mg/sqm and AUC 6 carboplatin and trastuzumab every 3 weeks. Trastuzumab was administered with 4 mg/kg loading then 2 mg/kg subsequently in weekly regimen or 8 mg/kg loading then 6 mg/kg subsequently in 3 weeks regimen. After concurrent chemo-trastuzumab administration, all patients received single -gent trastuzumab to complete 12 months while they were on treatments of radiation and/or endocrine therapy.
Pathological assessment was based on a core needle biopsy specimen for pre-surgery, with HE and IHC staining for tumor histology, tumor grade, hormone receptor status, HER2 expression, and Ki-67 index. Hormone receptor positive status was defined as estrogen receptor (ER) positive and/or progesterone receptor (PR) positive, with at least 1% of tumor cells stained positive for ER or PR. Ki-67 index was measured by the percentage of positively stained cells among the total number of tumor cells scored. With data from our laboratory, the cutoff point of 20% was used to define low or high expression of Ki-67. Expression of HER2 antibody measured by IHC was categorized as negative (1+), equivocal (2+), or positive (3+). Samples with equivocal result of HER2 expression on IHC were confirmed by fluorescent in situ hybridization (FISH) test. Postoperation pathology was examined using a surgical residual specimen, including breast tissue and axillary nodes. Pathological response was evaluated by Chevallier’s criteria, in which complete pathological response was defined as yT0yN0 or yTisN0.
Information extracted from the medical records included patient demographics (age, menopausal status) and tumor characteristics (locations, size, histological type, grade, hormone receptor status, Ki-67 and HER2 expression). Available data for pathological features were collected both before and after surgery.
Data were managed and analyzed using the SPSS statistics software. Chi-square and Fisher’s exact tests were used to test the difference of pathological response by clinical and pathological features.
Results
Patients and Treatment
There were 39 patients with stage IIA–IIIC, HER2 positive breast cancer treated from January 2013 to October 2018 at the National Cancer Hospital of Vietnam who met the inclusion criteria and were included in the analysis. Median age was 47 years (range, 32–72 years). Twenty-four (61.5%) patients were menopausal and 15 (38.5%) were pre-menopausal. Median tumor size was 5.8 cm. Of these 39 patients, 9 (25%) patients were operable (T1-3, N0-1, M0). Twenty-two (56.4%) patients had HR negative and 17 (43.6%) patients had HR positive diseases. Patient features are presented in Table 1. Twenty-nine (74.3%) patients were treated with the AC-TH regimen and 10 (25.7%) patients were treated with the TCH regimen.
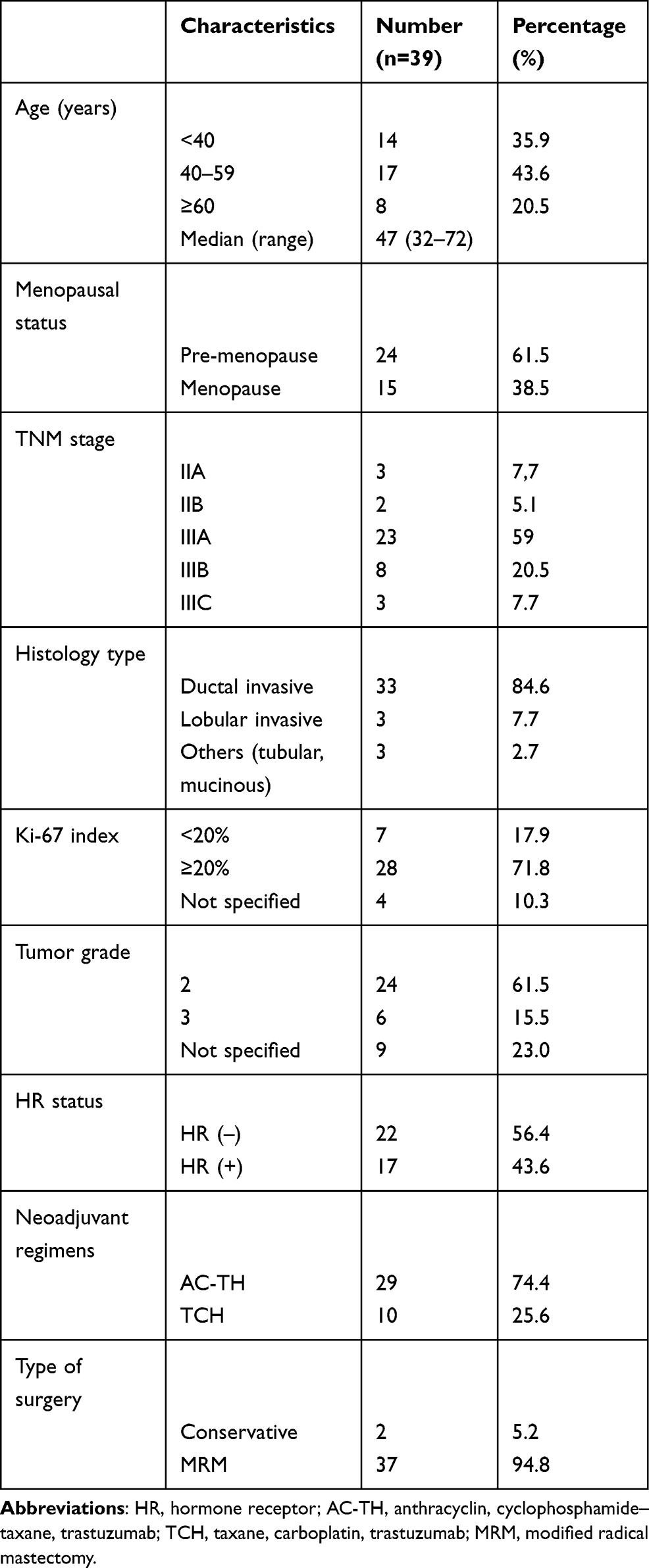 |
Table 1 Patient Demographics |
All (100%) of the patients were assessed to be clinically operable after finishing neoadjuvant chemo-trastuzumab regimens. Of these, 37 (94.8%) patients received modified radical mastectomy and 2 (5.2%) received conservative surgery.
Clinical Response
Synchronous clinical complete response (cCR) in breast and axillary lymph node was achieved in 33.3% of patients (13 out of 39) evaluated by RECIST criteria, with cCR rates of 33.3% (13 out of 39) in breast and 80% (28 out of 35) in node, respectively. There was no case of stable or progression of disease after neoadjuvant treatment. All the 30 inoperable patients were assessed to be operable after the neoadjuvant treatment.
Pathological Response
Rate of pathological complete response (tpCR) in both primary tumor and axillary lymph node was 64.1% (25 cases out of 39). Separately, pCR was achieved in 30 out of 39 patients (76.9%) for breast tumor and in 25 out 35 patients (71.4%) for axillary nodes. Table 2 presents detailed information on response rates in breast and axillary nodes.
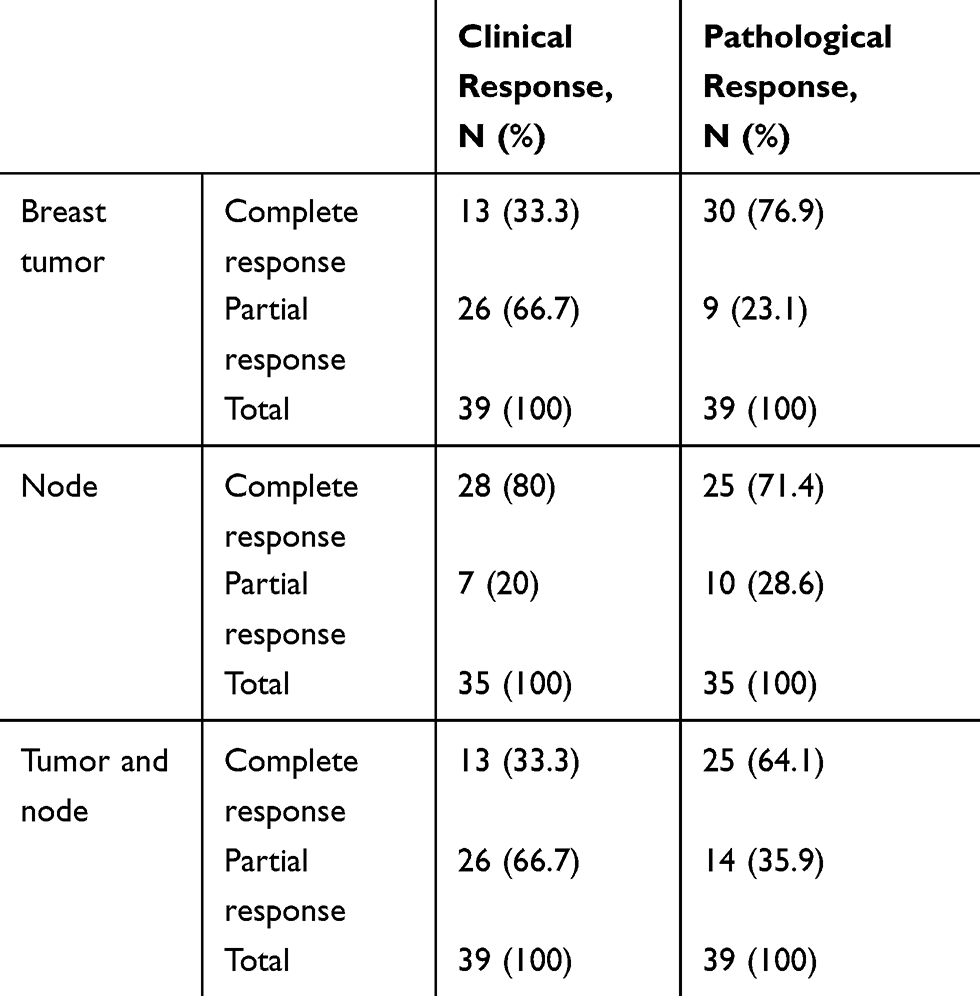 |
Table 2 Clinical and Pathological Response in Tumor and Nodes |
Total pathological complete response occurred in 12/17 (70%) and 13/22 (50%) patients with HR positive and HR negative diseases, respectively (p=0.46). Pertaining to pCR in breast only, 12/17 (70%) patients with HR positive and 18/22 (81%) with HR negative diseases achieved pCR (p=0.33). For pathological response in axillary node, 11/14 (78.6%) and 14/21 (66.7%) patients had HR positive and HR negative diseases, respectively (p=0.36). There were also no associations between pathological response and age (younger and older than 40), tumor grade, and chemotherapy regimens, as detailed in Table 3.
 |
Table 3 Pathological Response by Age and Tumor Biological Features |
Discussion
Our analysis was conducted in HER2 positive breast cancer patients with stage IIA–IIIC, treated with neoadjuvant trastuzumab–chemotherapy combined in the National Cancer Hospital of Vietnam, a specific population not previously included in any other similar trials. The rate of total pathological complete response in both primary breast tumor and axillary lymph node was 64.1%. Separately, 76.9% patients had pCR in breast only and 71.4% patients had pCR in the axillary node only. There was no significant association between pathological response and age, tumor grade, hormone receptor status, and chemotherapy regimens.
Total pathological complete response (tpCR) is one of the main end points in evaluating efficacy of neoadjuvant treatment. In the NOAH trial, the group treated with trastuzumab combined with chemotherapy had a total pCR of 38%, which was significantly higher than those treated with chemotherapy alone. In the study conducted by Buzdar et al8 to assess the role of neoadjuvant chemotherapy combined with trastuzumab, the tumor pCR rate was 65.2% which was significantly higher than the chemotherapy alone group (p=0.016).
One of the main objectives of neoadjuvant treatment in breast cancer is to convert the disease from inoperable to operable. In our study, all the 30 patients who were assessed to be clinically inoperable at baseline (T4, any N; any T, N2-3) were converted to operable after neoadjuvant treatment. This result is clinically meaningful and encouraging as the rates of late diagnosis of breast cancer are still significantly high. According to a report by Van Thuan et al, nearly 50% of breast cancer patients in Vietnam were diagnosed at stage III or IV.9 There were 2 (5.2%) patients who received conservative surgery. This low rate of conservative surgery is explained mainly by patient’s preference.
In our study, we did not find a significant correlation between pathological response and younger age (less than 40 years), tumor grade, hormone receptor status, Ki-67 index, and the chemotherapy regimens. The relative small sample size in our study might have also limited this finding. There has been an endeavor to identify demographic and tumor biology factors that can predict response to neoadjuvant treatment. In the TECHNO10 study, age (younger or older than 40 years), histological type and grade, tumor stage, node stage, and hormone receptor status were analyzed and none of them had significant correlation with the pCR rate. In the Gepar Quattro trial, Untch et al11 noted a significantly higher pCR in the hormone receptor negative group (43.5%) compared to the hormone receptor positive group (23.4%; p<0.001).
In the context of Vietnam as a developing country where affordability to dual HER2 blockade is limited, information on the clinical benefit of trastuzumab combined with chemotherapy in neoadjuvant treatment remains critical and practical. For those patients who could afford HER2 targeted drug, regimens with trastuzumab combined with chemotherapy remain the standard of care. Information from this analysis would therefore be clinically relevant to our daily practice.
Conclusion
Neoadjuvant trastuzumab combined with chemotherapy improved the pathological complete response rate in both tumor and lymph node in HER2 positive breast cancer with a tpCR of 64.1%. Based on this result, we recommend further studies to evaluate the survival benefit of the treatment protocol on this particular group of breast cancer patients.
Ethical Consideration
This study complied with the 1964 Helsinki Declaration and its later amendments. All the data collected from patient file were treated confidentially and in compliance with relevant data privacy policies.
The protocol of this study was approved by the National Cancer Hospital of Vietnam, by the Decision numbered 797/QĐ – BVK in 2018.
Disclosure
The authors declared that they have no conflicts of interest related to this study.
References
1. Asselain B, Barlow W, Bartlett J, Early Breast Cancer Trialists’ Collaborative G. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018;19(1):27–39. doi:10.1016/S1470-2045(17)30777-5
2. Gianni L, Eiermann W, Semiglazov V, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet. 2010;375(9712):377–384. doi:10.1016/S0140-6736(09)61964-4
3. Von Minckwitz G, Untch M, Blohmer JU, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol. 2012;30(15):1796–1804. doi:10.1200/JCO.2011.38.8595
4. Mieog JS, van der Hage JA. Preoperative chemotherapy for women with operable breast cancer. Cochrane Database Syst Rev. 2007;(2):CD005002.
5. Prowell TM, Pazdur R. Pathological complete response and accelerated drug approval in early breast cancer. N Engl J Med. 2012;366(26):2438–2441. doi:10.1056/NEJMp1205737
6. Marchio C, Maletta F, Annaratone L, Sapino A. The perfect pathology report after neoadjuvant therapy. J Natl Cancer Inst Monogr. 2015;2015(51):47–50. doi:10.1093/jncimonographs/lgv016
7. National Comprehensive Cancer Network. Breast cancer; 2018. Available from: https://www.nccn.org.
8. Buzdar AU, Ibrahim NK, Francis D, et al. Significantly higher pathologic complete remission rate after neoadjuvant therapy with trastuzumab, paclitaxel, and epirubicin chemotherapy: results of a randomized trial in human epidermal growth factor receptor 2-positive operable breast cancer. J Clin Oncol. 2005;23(16):3676–3685. doi:10.1200/JCO.2005.07.032
9. Van Thuan T, Anh PT, Van Tu D. Cancer control in Vietnam: where are we now? Cancer Control. 2016;99.
10. Untch M, Fasching PA, Konecny GE, et al. Pathologic complete response after neoadjuvant chemotherapy plus trastuzumab predicts favorable survival in human epidermal growth factor receptor 2-overexpressing breast cancer: results from the TECHNO trial of the AGO and GBG study groups. J Clin Oncol. 2011;29(25):3351–3357. doi:10.1200/JCO.2010.31.4930
11. Untch M, Rezai M, Loibl S, et al. Neoadjuvant treatment with trastuzumab in HER2-positive breast cancer: results from the GeparQuattro study. J Clin Oncol. 2010;28(12):2024–2031. doi:10.1200/JCO.2009.23.8451
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.