Back to Journals » International Journal of General Medicine » Volume 17
Pathological Changes and Pregnancy Outcomes in Cervical Intraepithelial Neoplasia Patients After Cold Knife Conization
Authors Cui N, Li X, Wen X, Xu JJ, Chen L ![]()
Received 2 January 2024
Accepted for publication 19 June 2024
Published 22 August 2024 Volume 2024:17 Pages 3641—3648
DOI https://doi.org/10.2147/IJGM.S457614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniele Castellani
Na Cui,1 Xue Li,1 Xin Wen,1 JingJing Xu,2 Li Chen1
1Department of Obstetrics and Gynecology, Baoding No.1 Central Hospital, Baoding City, Hebei Province, 071000, People’s Republic of China; 2Department of Ultrasound, Baoding No.1 Central Hospital, Baoding City, Hebei Province, 071000, People’s Republic of China
Correspondence: Li Chen, Department of Obstetrics and Gynecology, Baoding No.1 Central Hospital, No. 320 Changcheng North Street, Baoding City, Hebei Province, 071000, People’s Republic of China, Email [email protected]
Objective: Analyze women treated with underwent cold knife conization (CKC) to remove advanced squamous intraepithelial lesions (CIN) of the cervix. The histopathological upgrading of the lesions previously detected on vaginal biopsy and postoperative pregnancy outcomes of were investigated, to identify high-risk subgroups in women.
Methods: A retrospective study was conducted at the First Central Hospital of Baoding City from June 2019 to December 2022 to analyze confirmed cases of Cervical Intraepithelial Neoplasia CIN-II and CIN-III. Investigation of pathological changes in postoperative pathological tissues, and to perform binary logistic analysis to identify risk factors for histopathological escalation in postoperative lesions. We analyze the effects of CKC surgery on pregnancy outcomes in patients by comparing against a control group of healthy pregnant women.
Results: Out of the 176 patients diagnosed with CIN-II who underwent cervical biopsy, 39 (22.16%) were found to have a final specimen diagnosis of CIN-III, while 7 (3.98%) were downgraded to CIN-I. Among the 108 patients diagnosed with CIN-III who underwent cervical biopsy, 7 cases (6.48%) were ultimately confirmed to have CIN-III. Ki67-positive, p16-positive (OR = 1.13, 95% CI 1.01– 1.15), and colposcopy biopsy for CIN-II (OR = 1.59, 95% CI 1.33– 3.6) were independent risk factors for pathological upgrade after CKC. Compared with healthy pregnant women, CIN patients had higher rates of premature birth (14.4%), premature rupture of the fetal membrane (13.6%), and cesarean section (37.5%) (P < 0.05). The mode of conception, abortion rate, ectopic pregnancy rate, and postpartum hemorrhage were not different between healthy pregnant women and CIN patients (P > 0.05).
Conclusion: Following cervical multi-point biopsy or CKC, along with pathological examination, the accurate diagnosis of cervical lesions is crucial as it allows for more precise identification of such lesions. Additionally, CKC increases the risk of premature birth, premature rupture of membranes, and the need for cesarean section.
Keywords: cervical intraepithelial neoplasia, cold knife conization, pregnant women, colposcopy biopsy
Introduction
Globally, cervical cancer (CC) is the fourth most common malignancy in women, and it is the first or second most common cancer in poor countries.1 The number of new cases of CC is as high as 530,000 each year, while the number of deaths due to CC is close to 270,000.2,3 Genital infection with high-risk HPV increases the risk of developing precancerous lesions, such as cervical intraepithelial neoplasia (CIN).4,5 In addition, high-risk subtypes of HPV, such as HPV16/18, are associated with CC initiation, and persistent infection leads to CIN and eventually CC.6 The main diagnostic methods for CIN include cervical cytology, colposcopy, and histopathology.7,8 A small amount of uterine tissue guided by colposcopy for pathological examination before surgery can further diagnose diseases.9 However, due to the limited sampling scope and tissue size, the accuracy of biopsy pathological examination is limited.10 It has been noted that the incidence of CIN-II peaks between 25 and 29 years of age.11 The treatment methods for CIN include laser ablation, laser photocoagulation, loop electrosurgical excision procedure, and cold knife conization (CKC). A correct diagnosis of CIN is essential for selecting the right treatment method and achieving a significant improvement in treatment effect.
CKC is increasingly common among young patients with cervical lesions. In light of the delay in women’s reproductive function, preserving reproductive function is of particular importance in treatment. Cervical coning has not yet been conclusively demonstrated to affect fertility, delivery mode, or pregnancy outcome. Accordingly, assessing CKC’s impact on pregnancy outcomes may allow patients to postpone surgery or conservative treatment depending on their fertility needs.
Therefore, the purpose of this retrospective study was to understand the accuracy of colposcopy biopsy in the diagnosis of CIN before surgery and to analyze the risk factors for the upgrade of histopathologic examination after surgery. The second objective was to analyze the impact of CKC on pregnancy outcomes and provide research-based recommendations for patients with cervical lesions who have reproductive needs.
Materials and Methods
Research Data
This retrospective case study involved the selection of patients from the Obstetrics and Gynecology Center of Baoding No.1 Central Hospital between June 2019 and June 2022. The methods employed in this study adhered to the principles outlined in the Helsinki Declaration and relevant guidelines and regulations. This study has been approved by the Ethical Committee of Baoding No.1 Central Hospital (No. 201812BD-09). Inclusion criteria: (1) women diagnosed with moderate or advanced CIN by colposcopy biopsy and those who received CKC; (2) women aged 25–40 years; (3) No adverse obstetric history or pregnancy contraindications; (4) pregnancy after surgery; (5) Complete clinical data; (6) Regular re-examination of HR-HPV after treatment according to norms. Exclusion criteria: (1) women with postoperative pathological grades exceeding stage Ia1; (2) women with a history of infertility or known factors that may cause infertility; (3) women with clear contraindications to natural delivery before pregnancy; (4) women suffering from serious complications such as heart disease and blood disease; (5) Immune system diseases, HIV infection, etc. Finally, 284 patients were included as the study subjects. Patients ranged in age from 25 to 39 years, with an average age of 32.3 ± 4.2 years. All subjects were found to be CIN by colposcopy biopsy, and high-risk HPV was detected positive by polymerase chain reaction (PCR) and hybrid capture II (HC-II), including 176 cases of CIN-II and 108 cases of CINI-III. In addition, under the premise of age, pregnancy period, and delivery order, pregnant women who have experienced normal delivery in our hospital during the same period without obstetric complications, cervical lesions or developmental abnormalities, chronic diseases, and negative HPV tests were selected as the control group.
Data Collection and Grouping
Retrieve the patient’s demographic information, including age, body mass index (BMI), smoking status, human papillomavirus (HPV) DNA viral load, pathological grade of cervical lesions, fertility status, and pregnancy outcomes from clinical documentation during the screening process. Utilize the International Federation of Obstetrics and Gynecology (FIGO) 2018 staging criteria for cervical intraepithelial neoplasia (CIN) classification. Specifically, CIN staging criteria categorize CIN I as mild squamous dysplasia, koilocytosis, and basal cell hyperplasia; CIN-II stage: There is cell pleomorphism, the arrangement is disordered, and there are abnormal proliferating cells occupying more than two-thirds of the cortex; CIN-III stage: Epithelium with severe atypical hyperplasia has pleomorphism, loss of polarity, and abnormal proliferative cells extending to almost about two-thirds of the epithelium, or almost all of it, which is difficult to distinguish from carcinoma in situ.
Colposcopic Biopsy
The patient underwent a preoperative colposcopic biopsy. The patient emptied the bladder in the cystotomy position and underwent routine sterilization and toweling. A speculum was placed to dilate the vagina, fully exposing the cervix and sterilizing the vaginal and cervical areas. A colposcope was inserted into the patient’s vagina to visualize the cervix and vaginal walls. The surface of the cervix was rubbed with a 3% to 5% acetic acid cotton ball for 1 min to localize the suspected lesion area by the color change. A portion of the cervical tissue was extracted using biopsy forceps in the uncolored area. The biopsies were fixed and subsequently histopathologically examined and diagnosed by 2 experienced pathologists in the Department of Pathology according to the same criteria.
CKC
The procedure was performed 3–7 days after the end of menstruation, and the patient was asked to abstain from sexual intercourse for 1 week before the procedure. Before the operation, the patient should empty the bladder, take the cystotomy position, and perform the operation after routine anesthesia. The cervix was fully visualized and rubbed with Lugol’s iodine to clarify the area of the lesion and show the scope of the lesion and its boundaries. A low concentration of adrenaline was injected into the cervix to constrict the peripheral tissues of the cervix and capillaries, so as to reduce bleeding. For patients with small lesions, a circular incision can be made 0.5–1 cm from the outer edge of the lesion, while patients with larger lesions need to resect the non-stained area as much as possible, with the cervical canal as the axis, and resect the lesion into a cone shape, with a cone height of 2.0–2.5 cm.
Gauze compression was used to stop bleeding, and vaginal gauze was placed to prevent adhesions to the cervical canal and removed 48 hours after surgery. The removed tissues were immediately sent to the Department of Pathology for independent review by two or more intermediate pathologists, and all pathological diagnoses were reviewed and published by senior pathologists. Hemostatic drugs were routinely used, and perioperative infection prevention and care were given. Patients were observed for postoperative complications such as vaginal bleeding and infection, and appropriate therapeutic measures were given. Sexual intercourse was prohibited for 3 months after surgery.
Second Generation Hybridization Capture Method (HC-II)
Patients were sampled during the preoperative non-menstrual period, and vaginal medication and sexual intercourse were prohibited for the first 3 days. The HC-II method was used to detect HR-HPV viral load and quantify the content of 13 types of HPV-DNA (including HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68). The main test reagents and the main experimental instruments, gene hybridization signal amplifier DML2000, were purchased from Digene Corporation, USA. All specimens were taken by a professional obstetrician and gynecologist.
Sampling brush was conducted in the cervical opening through counterclockwise 3 turns to take the squamous columnar epithelial junction secretion. The sample was transferred to the STM preservation solution. The specific test was strictly in accordance with the instructions of the reagents, and the results were obtained on the DML2000 microtiter plate reader. HPV-DNA sample RLU/standard positive control RLU ≥ 1 means ≥ 1 pg of HPV-DNA per milliliter of specimen.
Reverse Transcription Amplification (Aptima-mRNA) Assay
For samples that test positive for high-risk HPV, HPV16, 18 mRNA within liquid cervical specimens were detected using Aptima 16 18/45 assay (Gen-Probe Inc., San Diego, CA). Briefly, a 1 mL aliquot of PreservCyt sample was pipetted into 2.9 mL of buffered clean solution, and a 400 uL aliquot of the mixture was assayed on a fully automated Panther system.
Immunohistochemical Staining
Wax blocks of the most heavily lesioned tissue were taken for P16 and Ki-67 immunohistochemistry. The biopsies were paraffin-embedded and sectioned (thickness 4 μm). Sections were dewaxed and incubated with 3% H2O2 for 5–10 minutes at room temperature to eliminate endogenous peroxidase activity, followed by antigen repair as needed. The slices were incubated with primary antibody (P16, dilution 1:100, Ki-67 dilution 1:50) at 37°C for 2 hours. The slices were incubated with biotin-labeled secondary antibody at 37°C for 30 minutes, freshly prepared 100 μL of diaminobenzidine solution was added to the slices, and the color development was observed under the microscope. The primary antibody was replaced by acid buffer as negative control; cervical cancer tissues were used as positive control for P16 and Ki-67.
Statistical Analysis
Continuous data were expressed as the median (interquartile interval, IQR). Enumeration data were expressed as n (percentage, %). Measurement data were in line with the normal distribution and homogeneity of variance and were analyzed by student t test. When the normal distribution is not satisfied, Mann–Whitney U-test was performed. Enumerations were compared by Chi-square test and Fisher's exact test. A two-tailed test was used to assess statistical significance, and a P-value < 0.05 was considered to indicate statistical significance. Statistical tests were performed using SPSS version 22.0, and graphs were produced using GraphPad Prism 9.0.
Results
Preoperative Data of CIN-II and CIN-III Patients
A total of 284 patients were included in our study, with colposcopy biopsy of CIN-II in 176 patients and CIN-III in 108 patients. As shown in Table 1, there were no statistical differences in age (P = 0.537), BMI (P = 0.622) and smoking history (P = 0.783) between CIN-II and CIN-III patients. The positive rates of Ki67 and p16 were as high as 96.8% and 91.9%, among which the positive rates of Ki67 and p16 were 94.9% and 85.2% in CIN-II patients, and 100% and 95.4% in CIN-III patients, respectively (P = 0.015, P = 0.008). The proportion of patients with HPV 16/18 subtype positive did not differ significantly between CIN-II and CIN-III patients (P = 0.218). However, HPV-DNA viral load was higher in CIN-III patients (P < 0.001).
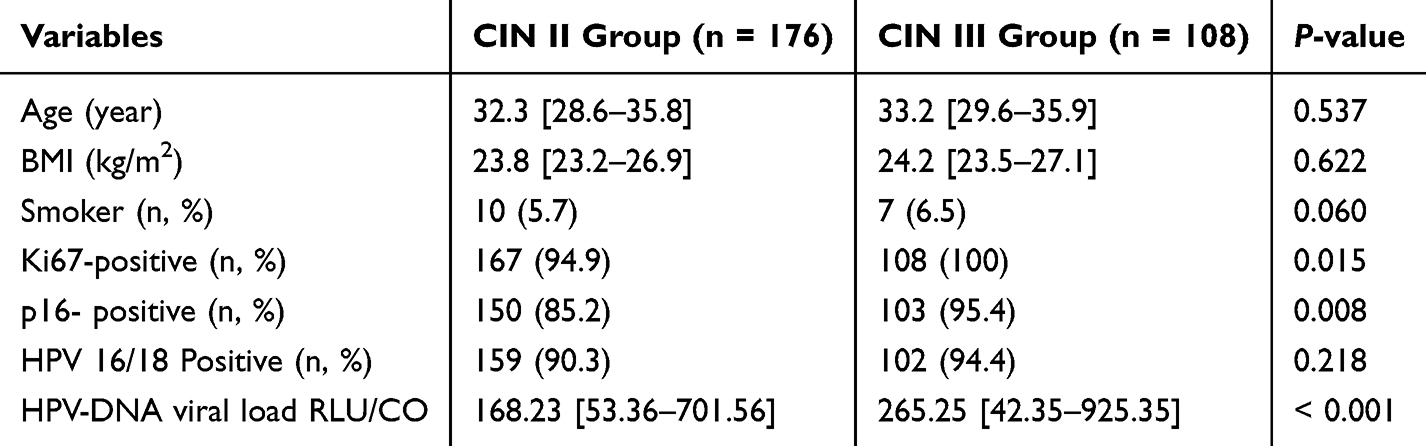 |
Table 1 Preoperative Data Comparison of Patients |
Univariate/Multivariable Logistic Regression of Risk Factors for Histopathological Upgrading of the Lesions Previously Detected on Vaginal Biopsy
As shown in Table 2, postoperative histopathological examination showed 7 cases of CIN-I, 135 cases of CIN-II, 135 cases of CIN-III, and 7 cases of invasive cervical squamous cell carcinoma stage Ia1. Preoperative colposcopy biopsy and postoperative histopathological examination were consistent in 226 cases, and 12 cases downgraded, and 46 cases upgraded. For CIN-II patients, the rates of preoperative and postoperative pathological consistent, downgrade and upgrade were 73.86%, 3.98% and 22.16%, respectively, while 88.89%, 4.63% and 6.48%, respectively, for CIN-III patients. There was a statistical difference between the two groups (P = 0.002, Table 2). Those with CIN-II in biopsy were more likely to experience CIN upgrading after CKC than those with CIN-III.
 |
Table 2 Comparison of Preoperative Colposcopy-Guided Biopsy and Postoperative Pathological Grade of CKC |
Next, the risk factors of postoperative pathological upgrade were analyzed by binary logistic analysis. As shown in Table 3, univariate analysis showed that Ki67-positive (OR = 1.12, 95% CI 1.03–3.58, P < 0.001), p16-positive (OR = 1.68, 95% CI 1.18–4.25, P < 0.001), HPV-DNA viral load (OR = 1.82, 95% CI 1.34–2.62, P = 0.033), and colposcopy biopsy for CIN-III (OR = 2.85, 95% CI 2.03–5.76, P < 0.001) were risk factors for pathological upgrade after CKC. After multivariate analysis correction, Ki67-positive (OR = 1.06, 95% CI 1.01–1.41, P < 0.001), p16-positive (OR = 1.13, 95% CI 1.01–1.15, P = 0.010), and colposcopy biopsy for CIN-II (OR = 1.59, 95% CI 1.33–3.60, P = 0.001) were independent risk factors for pathological upgrade after CKC.
 |
Table 3 Univariate/Multivariable Logistic Regression of Risk Factors for Histopathological Upgrading of the Lesions Previously Detected on Vaginal Biopsy |
Effect of CKC on Pregnancy Outcome
Further, we analyzed the effect of CKC on pregnancy outcomes. Table 4 shows that the mean gestation week of patients undergoing CKC surgery was 37.7 weeks [IOR, 36.9–38.2 weeks] and 38.4 weeks [IOR, 37.7–39.4 weeks] in the control group (P = 0.001). In addition, there was a statistical difference in the number of deliveries between the two groups (P < 0.001). The CKC group had higher rates of premature birth, premature rupture of membranes, and cesarean section, accounting for 14.4%, 13.6% and 37.5%, respectively, which were much higher than the control group (P = 0.011, P = 0.023, P < 0.001). Age (P = 0.787), BMI (P = 0.852), number of pregnancies (P = 0.124), smoking history (P = 0.167), mode of conception (P = 0.702), abortion rate (P = 0.172), ectopic pregnancy rate (P = 0.286), and postpartum hemorrhage (P = 0.720) were not different between the two groups.
 |
Table 4 Comparison of General Data and Pregnancy Outcomes Between CKC Group and Control Group |
Discussion
With the widespread promotion of cervical cancer screenings such as cervical cytology examinations and HPV tests over recent years, health awareness has improved significantly, and CC and precancerous lesions are more frequently detected and screened.12 At present, the main clinical treatment for high-grade CIN is CKC.13 This method has a complete specimen resection, no damage to the specimen margins, and is more conducive to the pathological definition of the lesion range.14,15 In recent years, clinicians have begun to pay attention to the effects of CKC on pregnancy. In this retrospective study, we found that after CKC surgery, the accuracy of pathological grades of CIN-II and CIN-III was 73.9% and 88.9%, and that pregnancy after CKC was more likely to have adverse outcomes. Our study may contribute to understanding the accuracy of the pathological grade of preoperative colposcopy biopsy and the impact of CKC on pregnancy.
CIN becomes precancerous lesions of CC, but not all CIN will develop into CC. In the process of screening and preliminary diagnosis of CIN, colposcopy biopsy is accurate and effective. However, in non-pregnant women, CKC is superior to Large Loop Excision of the Transformation Zone due to the lower positive rate of margins or residual lesions.16 Despite this, underdiagnosis persists. According to the study of Souza et al, the incidence of postoperative histopathological examination with CIN-II or worse lesions was 19% (15/80), and 1 woman showed stage I-a low-proliferation malignant tumor, which was not found by colposcopy or previous biopsy.17 In addition, the total coincidence rate between cervical biopsy pathological results and surgical results is only 57.29%, and the rate of postoperative CIN II lesions is 27.27%.18 Over- or under-treatment can be avoided by giving CKC treatment and follow-up based on colposcopic biopsy in patients with high-grade CIN. The results of this study showed that 176 cases of cervical biopsy guided by a colposcope before surgery were CIN-II and 108 cases were CIN-III. Ki67 and p16 in cervical smear for the auxiliary diagnosis of CIN have been clinically recognized.19,20 Ki67 and p16 are useful in identifying lesions at high risk for progressive CIN.21 In addition, positivity of Ki67 and p16 proteins is associated with disease progression.22 In our study, CIN-III patients had a higher positive rate of Ki67 and p16, which were independent risk factors for postoperative pathological upgrade. It is well known that persistent HPV16/18 infection is a risk factor for cervical-related lesions.23 We observed that high-risk HPV-DNA viral load was associated with disease severity but was not a risk factor for postoperative pathological upgrade. It is worth noting that colposcopic biopsy diagnosis of CIN-II is a risk factor for pathological upgrade. We believe that the reason for the increase in the examination grade may be related to the coexistence and multi-centricity of cervical lesions. Stoler et al also showed in a multicenter study that same-day biopsy, multiple biopsies and multi-point sampling were correlated with pathological accuracy.24 There is no clear conclusion on the effect of CKC on pregnancy outcomes. Aleman et al’s study showed that CKC was associated with serious adverse pregnancy outcomes.25 A meta-analysis also showed that CKC increased the risk of preterm birth, premature rupture of membranes, and low birth weight.26 CKC excites part of the mucus-secreting tissue, resulting in reduced secretion of cervical mucous containing antibacterial substances and easy invasion of pathogenic microorganisms, which makes pregnant women prone to subclinical infection, thereby increasing the risk of abortion, premature rupture of membranes, and premature delivery.27 Similar results were found in our study, where CKC influenced increased rates of preterm birth and premature rupture of membranes. Another literature concluded through meta-analysis that the risk of cesarean section in patients undergoing CKC is increased.28 In our analysis, the number of women who delivered by cesarean section after CKC increased by 37.5%.
Limitation
This study assessed the pregnancy outcomes of patients who underwent CKC, excluding those who underwent histopathological examination of postoperative lesion specimens and advanced beyond stage Ia1 of cervical squamous cell carcinoma, despite the rarity of such cases in clinical practice. At present, the impact of CKC on postoperative fertility and pregnancy outcomes of CIN patients has not been uniformly concluded, which may be related to the single-center study and retrospective analysis, and the prospect of multi-center and larger sample sizes is still needed. In addition, based on the results of this study, we can design a prospective study to subcompositionally measure the height, transverse diameter, and volume of the cone to obtain the optimal critical level and analyze the ability of these critical levels to predict adverse pregnancy outcomes to guide clinical practice.
Conclusion
Accurate diagnosis of cervical lesions following cervical multi-point biopsy, CKC, and pathological examination is imperative, as it enables more precise identification of such lesions. Those with CIN-II in biopsy were more likely to experience CIN upgrading after CKC than those with CIN-III. Furthermore, CKC increases the risk of adverse pregnancy outcomes, including premature birth, premature rupture of membranes, and the need for cesarean section.
Data Sharing Statement
Data is available from the corresponding author on request.
Ethics Approval
The present study was approved by the Ethics Committee of Baoding No.1 Central Hospital (No. 201812BD-09) and written informed consent was provided by all patients prior to the start of the study. All procedures were performed in accordance with the ethical standards of the Institutional Review Board and The Declaration of Helsinki, and its later amendments or comparable ethical standards.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Munoz N, Bravo LE. Epidemiology of cervical cancer in Colombia. Salud Publica Mex. 2014;56(5):431–439. doi:10.21149/spm.v56i5.7368
2. Miao J, Regenstein JM, Xu D, et al. The roles of microRNA in human cervical cancer. Arch Biochem Biophys. 2020;690:108480. doi:10.1016/j.abb.2020.108480
3. Bhat S, Kabekkodu SP, Noronha A, et al. Biological implications and therapeutic significance of DNA methylation regulated genes in cervical cancer. Biochimie. 2016;121:298–311. doi:10.1016/j.biochi.2015.12.018
4. Lazare C, Xiao S, Meng Y, et al. Evaluation of cervical intraepithelial neoplasia occurrence following the recorded onset of persistent high-risk human papillomavirus infection: a retrospective study on infection duration. Front Oncol. 2019;9:976. doi:10.3389/fonc.2019.00976
5. Spinillo A, Gardella B, Roccio M, et al. Untypable human papillomavirus infection and risk of cervical intraepithelial neoplasia among women with abnormal cervical cytology. J Med Virol. 2014;86(7):1145–1152. doi:10.1002/jmv.23938
6. Liao S, Deng D, Zhang W, et al. Human papillomavirus 16/18 E5 promotes cervical cancer cell proliferation, migration and invasion in vitro and accelerates tumor growth in vivo. Oncol Rep. 2013;29(1):95–102. doi:10.3892/or.2012.2106
7. Muller K, Soergel P, Hillemanns P, et al. Accuracy of colposcopically guided diagnostic methods for the detection of cervical intraepithelial neoplasia. Geburtshilfe Frauenheilkd. 2016;76(2):182–187. doi:10.1055/s-0041-111504
8. Wright VC. Cervical intraepithelial neoplasia: new developments in diagnosis and treatment. Can Fam Physician. 1980;26:729–736.
9. Bifulco G, De Rosa N, Lavitola G, et al. A prospective randomized study on limits of colposcopy and histology: the skill of colposcopist and colposcopy-guided biopsy in diagnosis of cervical intraepithelial lesions. Infect Agent Cancer. 2015;10(1):47. doi:10.1186/s13027-015-0042-9
10. van der Marel J, van Baars R, Rodriguez A, et al. The increased detection of cervical intraepithelial neoplasia when using a second biopsy at colposcopy. Gynecol Oncol. 2014;135(2):201–207. doi:10.1016/j.ygyno.2014.08.040
11. Wilkinson TM, Sykes PHH, Simcock B, et al. Recurrence of high-grade cervical abnormalities following conservative management of cervical intraepithelial neoplasia grade 2. Am J Obstet Gynecol. 2015;212(6):769 e1–7. doi:10.1016/j.ajog.2015.01.010
12. Bhatla N, Singhal S. Primary HPV screening for cervical cancer. Best Pract Res Clin Obstet Gynaecol. 2020;65:98–108. doi:10.1016/j.bpobgyn.2020.02.008
13. Xiang L, Li J, Yang W, et al. Conization using an electrosurgical knife for cervical intraepithelial neoplasia and microinvasive carcinoma. PLoS One. 2015;10(7):e0131790. doi:10.1371/journal.pone.0131790
14. Sand FL, Kjaer SK, Frederiksen K, et al. Risk of cervical intraepithelial neoplasia grade 2 or worse after conization in relation to HPV vaccination status. Int, J, Cancer. 2020;147(3):641–647. doi:10.1002/ijc.32752
15. Liu Y, Qiu HF, Tang Y, et al. Pregnancy outcome after the treatment of loop electrosurgical excision procedure or cold-knife conization for cervical intraepithelial neoplasia. Gynecol Obstet Invest. 2014;77(4):240–244. doi:10.1159/000360538
16. Nam K, Chung S, Kwak J, et al. Random biopsy after colposcopy-directed biopsy improves the diagnosis of cervical intraepithelial neoplasia grade 2 or worse. J Low Genit Tract Dis. 2010;14(4):346–351. doi:10.1097/LGT.0b013e3181e9635b
17. Souza CA, Discacciati MG, d’Otavianno MG, et al. Underdiagnosis of cervical intraepithelial neoplasia (CIN) 2 or worse lesion in women with a previous colposcopy-guided biopsy showing CIN 1. Rev Bras Ginecol Obstet. 2017;39(3):123–127. doi:10.1055/s-0037-1599071
18. Kabaca C, Koleli I, Sariibrahim B, et al. Is cervical punch biopsy enough for the management of low-grade cervical intraepithelial neoplasia? J Low Genit Tract Dis. 2014;18(3):240–245. doi:10.1097/LGT.0b013e3182aa08f6
19. Bergeron C, Ikenberg H, Sideri M, et al. Prospective evaluation of p16/Ki-67 dual-stained cytology for managing women with abnormal Papanicolaou cytology: PALMS study results. Cancer Cytopathol. 2015;123(6):373–381. doi:10.1002/cncy.21542
20. Gustinucci D, Passamonti B, Cesarini E, et al. Role of p16(INK4a) cytology testing as an adjunct to enhance the diagnostic specificity and accuracy in human papillomavirus-positive women within an organized cervical cancer screening program. Acta Cytol. 2012;56(5):506–514. doi:10.1159/000338979
21. Simionescu C, Mărgăritescu C, Stepan A, et al. The utility of p16, E-cadherin and Ki67 in cervical squamous intraepithelial lesions diagnosis. Rom J Morphol Embryol. 2010;51(4):621–626.
22. Kanthiya K, Khunnarong J, Tangjitgamol S, et al. Expression of the p16 and Ki67 in Cervical Squamous Intraepithelial Lesions and Cancer. Asian Pac J Cancer Prev. 2016;17(7):3201–3206.
23. Sierra MS, Tsang SH, Hu S, et al. Risk factors for non-human papillomavirus (HPV) Type 16/18 cervical infections and associated lesions among HPV DNA-negative women vaccinated against HPV-16/18 in the Costa Rica vaccine trial. J Infect Dis. 2021;224(3):503–516. doi:10.1093/infdis/jiaa768
24. Wentzensen N, Walker JL, Gold MA, et al. Multiple biopsies and detection of cervical cancer precursors at colposcopy. J Clin Oncol. 2015;33(1):83–89. doi:10.1200/JCO.2014.55.9948
25. Aleman JM, Arlien F, Tjalma WAA. The impact of conisation on pregnancy outcome. Eur J Gynaecol Oncol. 2016;37(6):786–791.
26. Zhuang H, Hong S, Zheng L, et al. Effects of cervical conisation on pregnancy outcome: a meta-analysis. J Obstet Gynaecol. 2019;39(1):74–81. doi:10.1080/01443615.2018.1463206
27. Selcuk I, Ersak B, Umaroğlu M, et al. The impact of Loop Electrosurgical Excision Procedure and cold-knife conization training model on the surgical skills and confidence level. Turk J Obstet Gynecol. 2020;17(2):133–138. doi:10.4274/tjod.galenos.2020.25675
28. Kyrgiou M, Athanasiou A, Kalliala IEJ, et al. Obstetric outcomes after conservative treatment for cervical intraepithelial lesions and early invasive disease. Cochrane Database Syst Rev. 2017;11(11):CD012847. doi:10.1002/14651858.CD012847
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.