Back to Journals » Medical Devices: Evidence and Research » Volume 18
Passive, Active, or Both—What Hemostats Do Surgeons Choose in the Real World, and Should We Rethink It?
Authors Knapp K, Armento IG, Parreno R, Martinez NP, Tippit R, Chovanes J
Received 24 June 2025
Accepted for publication 14 October 2025
Published 4 November 2025 Volume 2025:18 Pages 545—551
DOI https://doi.org/10.2147/MDER.S549147
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kristen Knapp,1 Isabella G Armento,1 Rhea Parreno,2 Natalia Peres Martinez,2 Rory Tippit,2 John Chovanes1
1Department of Surgery, Cooper University Hospital, Camden, NJ, USA; 2Baxter Healthcare Corporation, Deerfield, IL, USA
Correspondence: Rory Tippit, Baxter Healthcare Corporation, One Baxter Parkway, Deerfield, IL, 60015, USA, Tel +1 (224) 254 1246, Email [email protected]
Background: This study evaluates the association between the type of topical haemostatic agents used during surgery—categorized as active, passive, or a combination of both—and their relationship with intraoperative blood loss and bleeding-related postoperative outcomes.
Methods: A retrospective analysis was conducted at Cooper Health System, Camden, New Jersey, US, using patient records to compare the clinical performance of three haemostatic strategies: active agents, passive agents, and a combined approach.
Results: A total of 149 patients were included in the analysis: 51 treated with passive agents, 51 with active agents, and 47 with both. The mean age at admission was 55.9 years (SD ± 16.3). General surgery was the most frequently represented specialty (24.8%), followed by spine (22.1%), neurosurgery (16.8%), and solid organ procedures (16.1%). The combination group showed the highest estimated blood loss (EBL) at 521.3 mL (SD ± 1456.83; 95% CI: 93.5– 949.0), compared to 390.7 mL (SD ± 1004.81; CI: 108.1– 673.3) in the active group and 301.5 mL (SD ± 295.78; CI: 218.3– 384.7) in the passive group. However, ANCOVA results showed no statistically significant difference in adjusted mean EBL between groups (p = 0.309). Notably, patients in the combination group experienced longer operative times, extended ICU stays, and higher mortality.
Conclusion: Numerical trends suggest greater bleeding and more complex postoperative courses in patients treated with the combination of active and passive haemostats. The use of standardized, validated measures of intraoperative bleeding, paired with a strategic approach that anticipates and manages bleeding complications, may support improved clinical outcomes.
Keywords: bleeding, hemostat, patient blood management, hemostasis, trauma surgery
Introduction
Maintaining a fine balance between bleeding and clotting during surgery is imperative to surgical success and patient outcomes. This is achieved by ensuring adequate perfusion of tissue at the surgical site and avoiding excessive blood loss. Excessive intraoperative bleeding prompts several complications, such as prolonged operating time, obscured surgical field, and increased risk of hemodynamic instability. Intraoperative blood loss may also necessitate transfusion with blood products a limited resource with associated costs and risks.1,2
A wide range of hemostatic products have been developed and are available for use in surgical procedures. Two main product categories exist based on their mechanism of action: passive and active hemostatic products.
Passive hemostatic products like oxidized regenerated cellulose (ORC),3,4 gelatin-based passive hemostatic products2 and collagen-based passive hemostatic products2,5 are generally considered effective for small amounts of bleeding, such as those classified as grade I on the VIBe Scale,6 and act by forming a physical structure around which platelets can aggregate to rapidly form a clot. Their mode of action is dependent on an intact or functioning coagulation cascade. Therefore, the efficacy of passive products is reduced in patients treated with anticoagulant or antiplatelet medications, or in those with other coagulation disorders.
Active hemostatic products, such as thrombin, fibrin sealants and advanced patches act biologically at the end of the coagulation cascade, accelerating the natural clotting process.7 Active hemostatic products are effective regardless of whether patients have received anticoagulant/antiplatelet therapies or not, and function in the setting of both inherited and acquired coagulopathies. This is due to their mode of action which is effective independently of the state of the upstream coagulation cascade. Active products are also effective over a broader spectrum of bleeding, possibly ranging from VIBe grade I to VIBe grade III bleeds. Further, active hemostatic products can be a cost-effective option in some patients by lowering the risk of hemostatic failure and shortening operative and recovery times.8
The objective of this retrospective study was to describe the relationship and possible trends of hemostatic class choice on intraoperative bleeding, and its impact on postoperative bleeding-related outcomes.
The list of active and passive hemostatic/sealant products recorded from patient charts selected for this study is provided in Table 1.
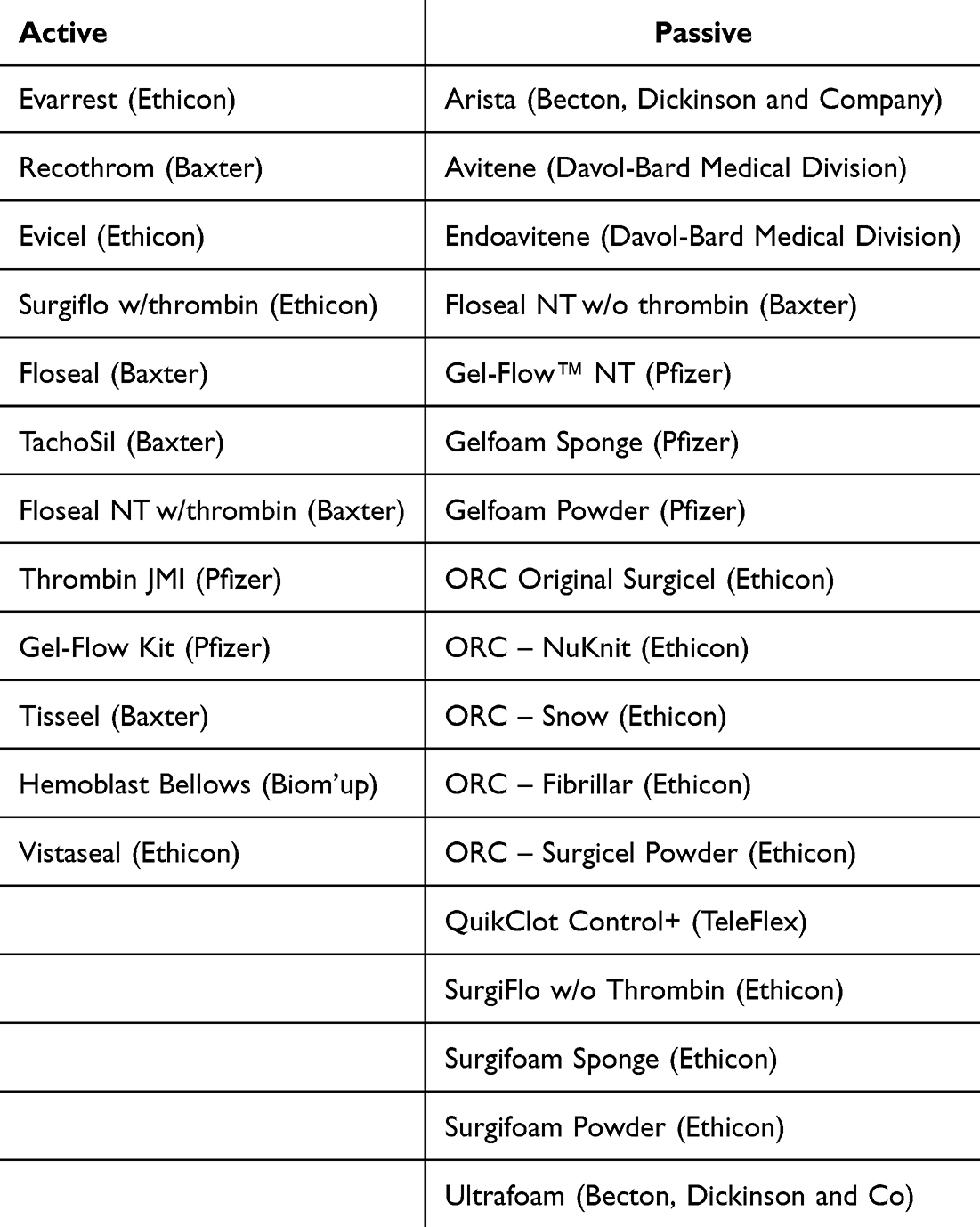 |
Table 1 Brand Names of Haemostatic Products/Sealants Recorded |
Methods
This was a single-center retrospective study in Cooper Health System, Camden, New Jersey, US. Retrospective data on intraoperative adjunctive topical hemostatic product usage from 149 consecutive patients across 3 cohorts (51 patients for whom passive hemostatic products were used, 51 patients for whom active hemostatic products were used, and 47 patients for whom combinations of active and passive hemostatic products were used) were sought. Data were collected from medical charts of adult patients who underwent a single inpatient surgery of interest (ie, cardiac, vascular, non cardiac thoracic, solid organ, general, reproductive organ, spine, or neurosurgery), between 01 September 2017 and 30 September 2020.
The primary endpoint was the intraoperative EBL in each cohort. Secondary endpoints included postoperative bleeding up to 48 hours, transfusion amount of blood products during intra- and postoperative period, incidence of re-intervention (surgical or radiological) for bleeding, preoperative and postoperative use of anticoagulant/antiplatelet agents, length-of-stay (including intensive care unit [ICU] days), OR time, number of hemostatic products used, all-cause mortality, and death due to uncontrollable bleeding.
This study was conducted in compliance with the requirements of the Code of Federal Regulations (21 CFR), the International Conference on Harmonization (ICH), Guideline for Good Clinical Practice (GCP) E6, ISO 14155:2020 and the ethical principles within the Declaration of Helsinki. The protocol was approved by the Cooper Health System Institutional Review Board, which granted a waiver of consent for the retrospective review of medical records.
Variables were analysed descriptively and presented using summary statistics. Differences in EBL between active, passive and a combination of these adjunctive topical hemostatic products were further assessed using ANCOVA, controlling for age, gender, antiplatelet/anticoagulant use prior to admission, and surgical procedure. Data on certain potential confounders (eg, surgeon experience) were unavailable; thus, residual confounding cannot be excluded. Given that this study was not formally powered, all p-values from the ANCOVA were used for descriptive purposes only.
Results
A total of 158 patients were identified for inclusion in the study, but 9 patients (5.7%) underwent more than one surgical procedure and therefore were not included in the analysis, as outlined in Figure 1. The patient population was evenly split, 76 (51.0%) patients were male while 73 (49%) were female. Table 2 shows a mean patient age (SD) of 55.9 (± 16.3) years. Surgical procedures by frequency were as follows: general surgery (24.8%), followed by spine surgery (22.2%), neurosurgery (16.8%), and solid organ surgery (16.1%), reproductive organ surgery (11.4%), vascular surgery (6.7%), cardiac surgery (1,3%) and non-cardiac thoracic surgery (0.7%). In terms of surgical approach, 119 (79.9%) patients underwent an open surgery while the remaining 30 (20.1%) underwent a minimally invasive/robotic procedure. The percentage of patients in whom anticoagulants/antiplatelets were used preoperatively was higher in the combination cohort (11 [23.4%]) than in the passive (5 [9.8%]) and active (9 [17.6%]) cohort.
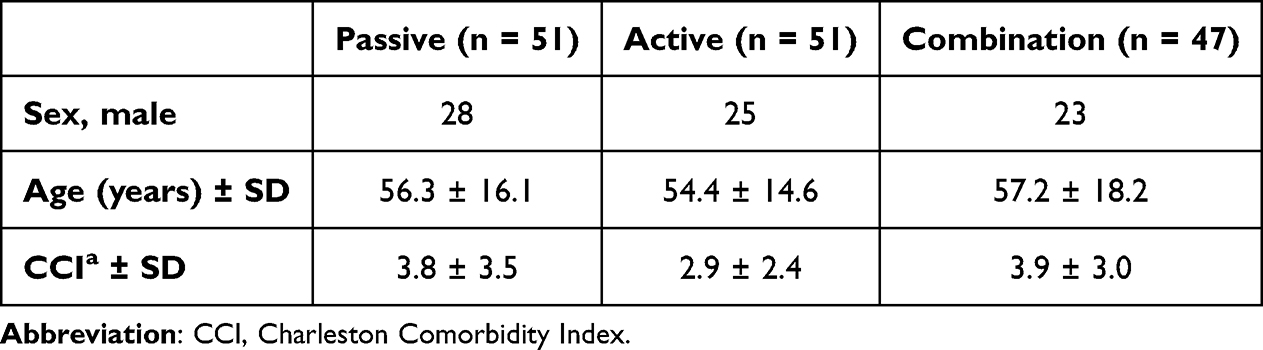 |
Table 2 Population Characteristics |
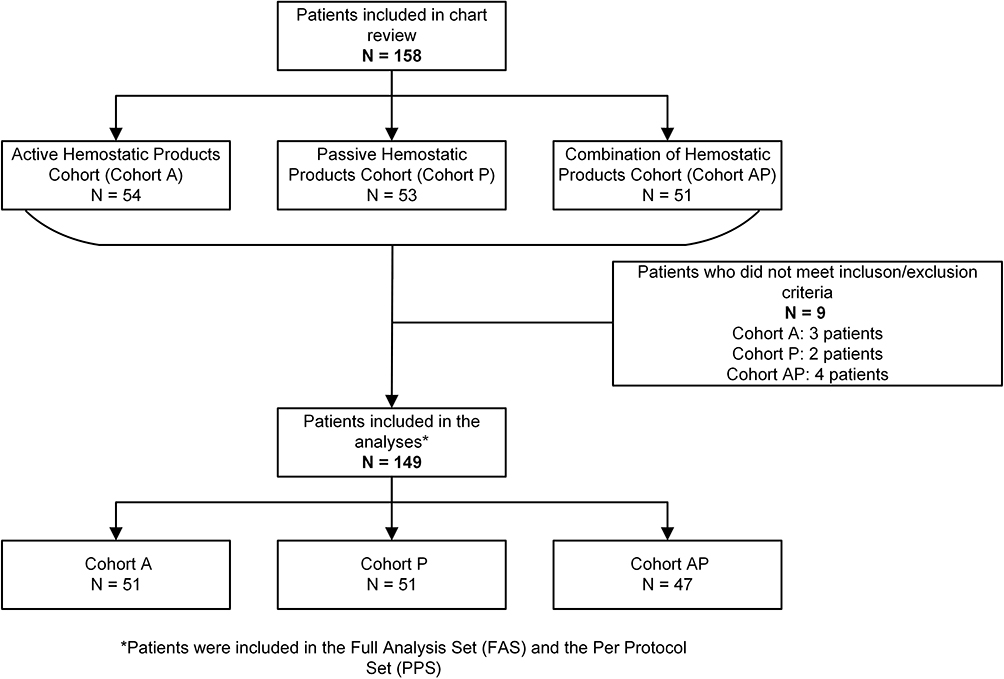 |
Figure 1 Patient Disposition Flowchart. Note: Figure prepared using Visio. *Patients were included in the Full Analysis Set (FAS) and per Protocol Set (PPS). Nine patients underwent more than one surgical procedure and were therefore excluded from the analysis. |
Table 3 shows that the mean intraoperative EBL was highest in the combination cohort (mean [SD; 95% CI]: 521.3 mL [±1456.8 mL; 93.5‑949.0 mL]), followed by the active cohort (390.7 mL [±1004.8 mL; 108.1673.3 mL]) and passive cohort (301.5 mL [±295.8 mL; 218.3‑384.7 mL]). ANCOVA results showed no differences in adjusted mean (SE) EBL among the groups (p = 0.309). The percentage of patients receiving intraoperative transfusion was 11.8% in the passive group, 9.8% in the active group, and 38.3% in the combination group, with comparable percentages postoperatively (11.8% in the passive group, 7.8% in the active group and 21.3% in the combination group). The combination group had the highest rate of postoperative bleeding within 48 hours of the procedure (10.6%), of which 60% required intervention for hemostasis compared to the passive group and active group (both 2.9%). Operating room time was longest for patients in the combination cohort (mean [SD]: 222.7 [± 98.13] minutes), followed by patients in the active cohort (212.5 [± 116.54] minutes) and patients in the passive cohort (195.1 [± 93.82] minutes). Similarly, the mean ICU stay was longer for the combination group (2.9 days), and shorter for the passive group (1.1 days) and active group (0.7 days). Differences were noted in the percentage of mortality between the 3 groups, with the highest mortality rate (10.6%) and mortality due to hemorrhage (6.4%) featuring in the combination group.
 |
Table 3 Primary and Secondary Endpoints |
Discussion
This study compared the individual use with combined use of passive and active agents.
During the intraoperative period, patients in the combination cohort lost more blood than those in the passive and active cohorts, although the significance of this difference is unknown due to the study’s descriptive nature. Training, product knowledge, and type of procedure are factors that affect hemostatic product selection which may, in turn, explain this trend. The most common surgery types assessed were general, spinal, or neurosurgical; all of which are procedures in highly vascularized areas and are associated with high bleeding rates. Operating room time was longest for the combination cohort. While procedure length is dependent among other factors, on surgical site and complexity, OR time for the combination cohort may have been further increased by the surgeon failing to choose the correct hemostatic product to begin with. For significant bleeding (VIBe grade II and III) as well as lower grade bleeding in patients with acquired or inherited coagulopathy, primary use of active products is recommended. Use of passive products in this setting will not control bleeding, and as such, the use of a situationally ineffective product only wastes time and increases OR costs. Further, the presence of passive agents in the surgical field can reduce the effectiveness of secondarily applied active agents. For example, passive products containing oxidated regenerated cellulose have a low pH, and when combined with active products, the acidic environment may result in denaturation of thrombin, the active ingredient, and renders the active hemostatic ineffective. As a result, an active product, such as Floseal, applied into a surgical field contaminated with a passive product, such as Surgicel, may be rendered useless.
We cannot retrospectively judge surgical decision making or determine the chain of intraoperative events which led to the combined use of passive and active products in 30.5% of our study population. As such, it is impossible to rule out scenarios where a passive agent was used appropriately for a VIBe grade I bleed, which subsequently worsened to a grade II or III bleed, requiring an active product. We can, however, with certainty assert that use of a passive product in a patient with known coagulopathy, either inherited or acquired, is ineffective and inappropriate. The percentage of patients with known preoperative anticoagulant/antiplatelet use and in whom a passive agent was utilized alone was 9.8% and 23.4% in the combination cohort, corroborating this hypothesis. This identifies an important and actionable shortcoming in surgical education. If knowledge of the ineffectiveness of passive hemostatic use is made commonplace among clinicians, then patients could be spared the repercussions of delayed bleeding control due to inappropriate product selection. Delayed bleeding control contributes to increased blood loss, transfusion requirement, and operative time – all of which exacerbate the metabolic derangement experienced by patients, which worsens with every minute on a cold OR table under anesthesia.
Blood transfusion is critical in maintaining hemostasis, correcting abnormal coagulation, and ensuring adequate tissue perfusion and oxygenation. However, blood transfusion comes with associated costs and risks. Primarily, banked blood is a limited and costly resource. Second, blood transfusion comes with associated risks of transfusion reaction, infection, and development of antibodies.
While there were no substantial increases in intraoperative blood loss when a combination of hemostatic agents was used, there were significantly more cases requiring transfusions. Of the minority of patients who required administration of blood, more patients received transfusions intraoperatively than postoperatively, with the combination cohort showing the highest requirement during both periods. According to clinical practice guidelines regarding the indications for intraoperative blood transfusions, most of the cases in this study did not meet the criteria for requiring a transfusion based on their EBL alone.9,10 This suggests that additional factors, such as pre-admission blood loss in trauma patients, the type and acuity of the procedure, the rate of blood loss, repeated hemoglobin and hematocrit monitoring, and signs of hemodynamic instability or end-organ damage were all taken into consideration. It is also important to note that anticoagulant/antiplatelet use increases the risk of bleeding, thus their higher percentage of use in the combination cohort may have contributed to the higher incidence of intraoperative and postoperative bleeding within the same cohort. Considering this, intraoperative bleeding was controlled with both active and passive agents before EBL became significant, but intraoperative blood transfusion was still indicated for reasons other than the volume of blood lost.
We also observed a rise in ICU length of stay and overall mortality in patients who received a combination of hemostatic agents. Prior literature has shown that increased ICU lengths of stay have been associated with higher mortality rates11,12 and therefore, it is reasonable to observe that these two share a direct relationship. Several major factors influence a patient’s ICU length of stay, such as undergoing emergent surgery versus an elective procedure, low scores on the Glasgow Coma Scale (GCS), high preoperative surgical risk, and hemodynamic instability.12,13 This suggests that the relationship between combination use of hemostatic agents and ICU length of stay is confounded by additional factors, primarily with respect to the acuity of the surgery, and the stability of the patient. Several hypotheses can be proposed from this, but the most likely is that combination agents are more frequently utilized in settings where blood loss is not controlled by the primary agent and hemodynamic stability is compromised, hypothetically forcing the surgeon to choose a more adequate (potent) hemostatic adjuvant. A validated bleeding severity assessment tool, such as the VIBe Scale, can help to gauge the severity of a bleed in open surgical procedures across surgical specialties and ultimately guide the surgeon to select an appropriate hemostatic product.14,15 The use of such a scale in combination with a treatment approach that considers bleeding-related complications may overall help improve patient outcomes.
Although the evidence supports the efficacy of these adjunctive topical agents in helping to achieve hemostasis, there are several limitations that can be identified. The evidence put forth by this study is inherently limited by the study design. Prospective and multicenter exploration is warranted to provide further validity for the use of these agents. The increased requirement for intraoperative blood transfusion is not based on EBL alone. Signs of hemodynamic instability and longer ICU lengths-of-stay can be impacted by the type of procedure and indication for it, both of which were variables unexamined in this study. Lastly, the trend observed in overall mortalities can simply reflect the direct relationship it has with ICU length of stay. Further investigations should be controlled for these confounders to strengthen the current evidence supporting the efficacy of these hemostatic agents.
Conclusions
Numerical trends suggest greater bleeding and more complex postoperative courses in patients treated with the combination of active and passive haemostats when compared to patients who received either active or passive hemostatic products. While this investigation shows promising insight into the use of these agents and alludes the importance of selecting the right hemostatic product when considering the risks and benefits to the individual patient, further research is warranted. These hypothesis-generating findings support prospective, adequately powered studies that should incorporate standardized, validated measures of intraoperative bleeding severity to guide severity-based selection of hemostatic agents.
Ethical Requirements
The protocol was approved by the Institutional Review Board, which granted a waiver of consent for the retrospective review of medical records.
Acknowledgments
We would like to acknowledge Denise Saliba and Jessica Svatek from Baxter Healthcare for their assistance with writing this manuscript.
Funding
This study was funded by Baxter Healthcare Corporation.
Disclosure
This study was funded by Baxter Healthcare Corporation, which produces active and passive hemostatic products and also funds educational opportunities for Cooper University Hospital, where this study was conducted. Additionally, some of the authors are employees of Baxter Healthcare Corporation. The authors report no other conflicts of interest in this work.
References
1. Renkens KL, Payner TD, Leipzig TJ, et al. A multicenter, prospective, randomized trial evaluating a new hemostatic agent for spinal surgery. Spine. 2001;26(15):1645–1650. doi:10.1097/00007632-200108010-00002
2. Sabel M, Stummer W. The use of local agents: surgicel and Surgifoam. Eur Spine J. 2004;13 Suppl 1:S97–101. doi:10.1007/s00586-004-0735-z
3. Koea JB, Batiller J, Aguirre N, et al. A multicentre, prospective, randomized, controlled trial comparing EVARRESTTM fibrin sealant patch to standard of care in controlling bleeding following elective hepatectomy: anatomic versus non-anatomic resection. HPB. 2016;18(3):221–228. doi:10.1016/j.hpb.2015.12.006
4. Schuhmacher C, Pratschke J, Weiss S, et al. Safety and effectiveness of a synthetic hemostatic patch for intraoperative soft tissue bleeding. Med Devices. 2015;8:167–174. doi:10.2147/MDER.S79556
5. Lawson JH. The clinical use and immunologic impact of thrombin in surgery. Semin Thromb Hemost. 2006;32 Suppl 1:98–110. doi:10.1055/s-2006-939559
6. Lewis KM, Li Q, Jones DS, et al. Development and validation of an intraoperative bleeding severity scale for use in clinical studies of hemostatic agents. Surgery. 2017;161(3):771–781. doi:10.1016/j.surg.2016.09.022
7. Slezak P, Keibl C, Labahn D, et al. A comparative efficacy evaluation of recombinant topical thrombin (RECOTHROM®) with a gelatin sponge carrier versus topical oxidized regenerated cellulose (TABOTAMP®/SURGICEL®) in a porcine liver bleeding model. J Invest Surg. 2020;34:1–7.
8. Nasso G, Piancone F, Bonifazi R, et al. Prospective, randomized clinical trial of the FloSeal matrix sealant in cardiac surgery. Ann Thorac Surg. 2009;88(5):1520–1526. doi:10.1016/j.athoracsur.2009.07.014
9. American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an updated report by the American society of anesthesiologists task force on perioperative blood transfusion and adjuvant therapies. Anesthesiology. 2006;105(1):198–208. doi:10.1097/00000542-200607000-00030
10. Baker L, Park L, Gilbert R, et al. Intraoperative red blood cell transfusion decision-making: a systematic review of guidelines. Ann Surg. 2021;274(1):86–96. doi:10.1097/SLA.0000000000004710
11. Moitra VK, Guerra C, Linde-Zwirble WT, et al. Relationship between ICU length of stay and long-term mortality for elderly ICU survivors. Crit Care Med. 2016;44(4):655–662. doi:10.1097/CCM.0000000000001480
12. Uzman S, Yilmaz Y, Toptas M, et al. A retrospective analysis of postoperative patients admitted to the intensive care unit. Hippokratia. 2016;20(1):38–43.
13. Böhmer AB, Just KS, Lefering R, et al. Factors influencing lengths of stay in the intensive care unit for surviving trauma patients: a retrospective analysis of 30,157 cases. Critical Care. 2014;18(4):R143. doi:10.1186/cc13976
14. Tibi PR, A D Jr, Leung SK, et al. Global observational survey verifying surgeon utilization of the validated intraoperative bleeding (VIBe) scale for use in clinical practice. Surg Pract Sci. 2022;12:100123. doi:10.1016/j.sipas.2022.100123
15. Rabello G, Monteiro R, Meneghini B, Jatene FB. When innovation meets patient blood management - a new way to see bleeding. Hematol Transfus Cell Ther. 2025;47(1). doi:10.1016/j.htct.2024.07.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Safety and Performance of Hemostatic Powders
Szymanski L, Gołaszewska K, Małkowska J, Kaczyńska J, Gołębiewska M, Gromadka B, Matak D
Medical Devices: Evidence and Research 2023, 16:133-144
Published Date: 8 June 2023