Back to Journals » International Journal of Women's Health » Volume 17
Partial Response Achieved in a Case of Metastatic Triple-Negative Breast Cancer Based on the Patient-Derived Tumor Organoids
Received 12 February 2025
Accepted for publication 5 July 2025
Published 31 July 2025 Volume 2025:17 Pages 2395—2400
DOI https://doi.org/10.2147/IJWH.S520867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Yang Liu, Shuai Liang, Jian Li
Department of Breast Surgery, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated to Shanxi Medical University, Taiyuan, 030013, People’s Republic of China
Correspondence: Jian Li, Department of Breast Surgery, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated to Shanxi Medical University, No. 3 Zhigong New Village, Xinghualing District, Taiyuan, 030013, People’s Republic of China, Email [email protected]
Background: The prognosis of triple-negative breast cancer (TNBC) is dismal due to aggressive behaviors. Emergence of patient-derived tumor organoids (PDTOs) allows for biomarker identification and drug screening to identify potential drugs at the patient-specific level. Here, we described a case of metastatic TNBC who obtained partial response in the liver metastatic lesions after treatment with sacituzumab govitecan that was identified highly sensitive by the PDTOs.
Case Presentation: A 50-year-old woman visited our hospital for re-examination due to over 9 years after surgery for the left breast cancer. In February 2024, she experienced liver metastasis. In combination with medical history and immunohistochemistry results, metastatic TNBC was diagnosed. Based on the PDTO drug sensitivity testing, the patient was treated with highly sensitive sacituzumab govitecan. After 6 cycles of treatment, liver metastatic lesions were reduced partially.
Conclusion: In our case of TNBC, partial response is achieved in the liver metastatic lesions after treatment based on the PDTOs, unveiling that the PDTO, a potential companion tool for selection of treatment options, can facilitate the personalized treatment in metastatic TNBC patients to improve the prognosis.
Keywords: triple-negative breast cancer, liver metastasis, sacituzumab govitecan, patient-derived tumor organoids, personalized treatment
Introduction
Breast cancer is the most frequent malignancy in women worldwide, in which triple-negative breast cancer (TNBC) defined by absence of estrogen receptors (ER), progesterone receptors (PR) and human epidermal growth factor receptor-2 (HER2) approximately accounts for 15–20% and is associated with dismal prognosis due to aggressive behaviors like earlier recurrence and metastasis.1,2 Currently, surgery and chemotherapy remain to be the feasible treatment modality for TNBC in the initial stage, but almost ineffective for TNBC at an advanced stage.3 Due to lack of ER, PR, and HER2 expression in TNBC, patients are exempt from any targeted endocrine or HER2 therapies, consequently leading to non-specific cytotoxic chemotherapy as the standard treatment.4 Therefore, it is urgently needed to better understand TNBC biology and to identify more precise druggable targets.
Conventional breast cancer models comprise cell lines and patient-derived xenografts (PDXs). Although cancer cell lines are simple and easy to adjust culture conditions, the genetic features and tumor heterogeneity are difficult to be preserved during passaging.5 PDX models are considered to play an important role in understanding the tumor biology and drug development, but they have high cost and need a long time for establishment.6 Patient-derived tumor organoids (PDTOs), a recently emerging three-dimensional pre-clinical model, are identified to accurately recapitulate the features of original tumors at genetic and molecular levels and have been constructed successfully in multiple cancer types including colorectal cancer, gastric cancer and breast cancer.6–8 For risk assessment and drug development in breast cancer, the PDTOs have been demonstrated to be a valuable model system.9 They are not only predictive of response to neoadjuvant therapy but also contribute to guide the treatment options for advanced breast cancer.10,11 Here, we shared a case of metastatic TNBC who responded well to sacituzumab govitecan that was identified highly sensitive by the PDTOs and achieved good prognosis.
Case Presentation
A 50-year-old woman came to our hospital for re-examination due to over 9 years after surgery for the left breast cancer. At the beginning of 2015, the patient inadvertently palpated a mass with the size of an apricot pit in the left breast, accompanied by tenderness but no nipple discharge. The mass gradually increased without attention. In July 2015, she underwent modified radical resection of left breast cancer under general anesthesia (Figure 1A), and the postoperative pathology showed invasive ductal carcinoma of the left breast, with ER of approximately 80%++, PR of approximately 80%+++, HER-2 of 0, and Ki67 of approximately 40%+. Stage IIA (T2N2M0) breast cancer was diagnosed. Accordingly, adjuvant chemotherapy with Cyclophosphamide (0.9 g), Epirubicin (140 mg), and Docetaxel (140 mg) was administrated for 6 cycles. During December 2015 and January 2016, radiotherapy was performed, with 95% of the prescribed dose of 50 Gy/25 fractions for the planning target volume (PTV1: the left chest wall; PTV2: the left clavicle region). Subsequently, endocrine therapy with Toremifene (60 mg) and Letrozole (2.5 mg) was continuously taken for 4 years.
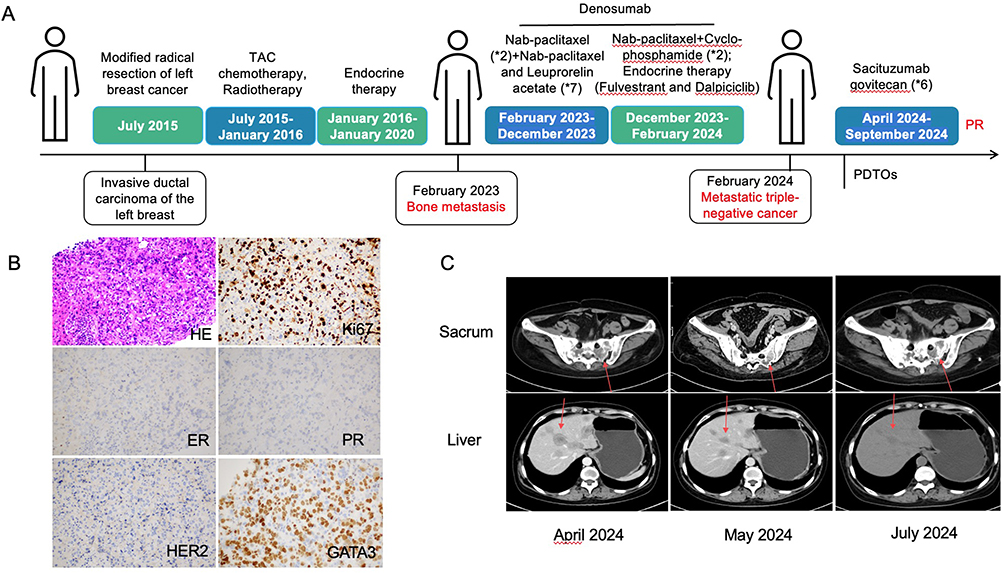 |
Figure 1 The diagram of diagnosis and treatment process of the patient (A), H&E staining and immunobiological results of the liver metastatic lesion (B), and radiological variations during the treatment based on patient-derived breast cancer organoids (C). |
At the beginning of 2023, the patient developed significant low back pain. The computerized tomography (CT) scan showed bone destruction (metastasis) in the right sacroiliac 3 vertebrae, bulging of the intervertebral disc in L3-4, as well as protrusion in L4-5 and L5-Sacrum 1. In February 2023, the patient received 2 cycles of Nab-paclitaxel (400 mg) chemotherapy, followed by 7 cycles of Nab-paclitaxel combined with subcutaneous injection of Leuprorelin acetate (3.75 mg). In December 2023, the treatment regimen was adjusted to 2 cycles of Nab-paclitaxel plus Cyclophosphamide, during which Fulvestrant and Dalpiciclib were used as endocrine therapy. Notably, Denosumab had been continuously administrated against bone metastasis since March 2023. In February 2024, ultrasonic examinations showed multiple solid, low-echo nodules in the liver, suggesting the possibility of metastasis, thus the liver nodule was punctured. In combination with medical history and immunohistochemistry results [ER (-), PR (-), HER-2 (0), CK5 (scattered), Ki67 (approximately 70%+), GATA3 (+), hepatocyte (-); Figure 1B], metastatic cancer was diagnosed, suggesting breast origin. In April 2024, the CT scan showed postoperative changes in the breast malignancy, significantly relieved thickening near the sternum of the left chest wall, newly increased scattered patches and irregular nodules in both lungs, abnormal density in bilateral ribs, vertebral bodies, appendages, sacrum and the hip bone, as well as multiple liver nodules and masses, suggesting metastasis (Figure 1C).
After the patient was informed consent, the needle biopsy tissue from liver nodules was collected and immediately transported to the laboratory (Kingbio Medical [Chongqing] Co., Ltd., China) on ice for organoid culture and drug sensitivity testing. Briefly, the tissue was first rinsed, and then minced and digested. Through centrifugation, the cell pellet was obtained. Subsequently, Matrigel was added, and cells and Matrigel suspension were both inoculated onto 6-well plates (2 mL per well) using pipettes, which were placed in a 37°C incubator for 15 min. Once the droplets solidified, Jiabili culture medium (Kingbio Medical [Chongqing] Co., Ltd., China) was added, which was then cultured at 37°C, 5% CO2. The culture medium was changed every 2–3 days. When the organoid presented typical saccular, solid spherical or dispersive base form (Figure 2A–C), drug sensitivity testing was performed. It could be observed that the PDTOs were highly sensitive to the targeted drug sacituzumab govitecan, except for chemotherapy drugs (Figure 2D). Thus, the patient was treated with sacituzumab govitecan (3 mg/kg) for 6 cycles. In May 2024, the CT scan indicated slightly thickening near the sternum of the left chest wall, decreased small patches in both lungs, increased density shadows in bilateral ribs, vertebral bodies, appendages, sacrum and the hip bone, as well as multiple slightly low-density nodules and mass shadows in the liver parenchyma, with the largest being about 4.3*2.8 cm, some of which were reduced compared with before (Figure 1C). In July 2024, the CT scan further revealed that the thickening near the sternum of the left chest wall was consistent with the postoperative changes; scattered small patches and cord-like shadows are similar to before; most of the multiple slightly low-density nodules and mass shadows in the liver parenchyma were lessened than before, with the largest being about 3.5*2.3 cm, which all suggested shrunken liver nodules (Figure 1C). So far, the patient still receives sacituzumab govitecan for further treatment.
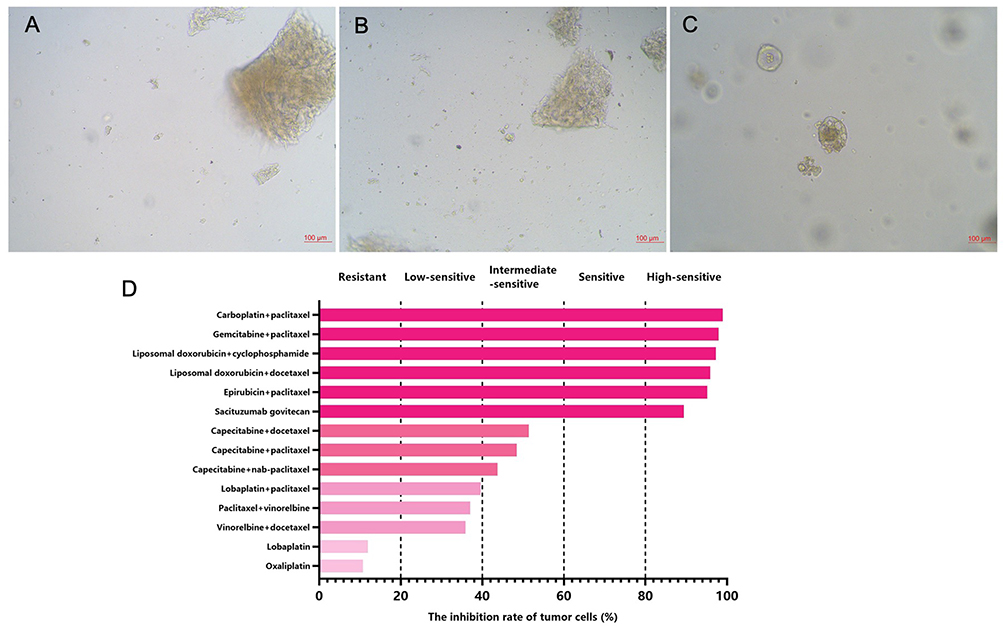 |
Figure 2 The growth changes of patient-derived triple-negative breast cancer organoids including prior to inoculation of Matrigel (A), organoid formation (B) and prior to drug sensitivity testing (C), as well as drug sensitivity testing results (D). |
Discussion
Metastatic TNBC patients have poor survival outcomes. Although immunotherapy shows promising in the first-line treatment, single-agent chemotherapy is still the standard for previously treated (beyond first-line) metastatic TNBC.12 Nevertheless, chemotherapy is found to have poor response rates and survival outcomes.13 For metastatic breast cancer, this poor clinical outcome underlines the demand for dependable personalized oncology and importance of models that can preserve the features of metastatic breast cancer.14 In this study, we adjusted the chemotherapy regimens into the single agent sacituzumab govitecan for treatment based on the drug sensitivity testing results from PDTOs and found that the metastatic lesions in the liver gradually reduced. Sacituzumab govitecan, an antibody-drug conjugate for treating solid tumors, has recently received accelerated approval for adult patients with metastatic TNBC who are previously treated with at least two therapies for metastatic disease, with significantly longer progression-free survival and overall survival than single-agent chemotherapy in metastatic TNBC.15,16
The pre-clinical research of breast cancer has always depended on various cell lines as an in-vitro representation of a heterogeneous disease over the decades, but these cell lines do not completely capture the spectrum of breast cancer despite feasible high‐throughput screening. Although patient-derived xenograft models can effectively capture tumor heterogeneity, they have low success rates, long time, and high cost in establishment.17 Tumor organoids with high success rates are the 3D cultures of cancer cells based on a single patient, which can not only recapitulate the biological characteristics of cancer cells but also assess the drug efficacy and toxicity.18 They can guide clinical decision-making at the patient-specific level by offering a mechanism for faithfully testing the drug sensitivity and a half-maximal inhibitory concentration value.19
In recent years, PDTOs have been identified to be a superior pre-clinical model for drug screening and treatment responses.20 Shu et al established a living organoid biobank to predict the response to neoadjuvant chemotherapy in breast cancer, and the results showed that the PDTOs could not only predict the response to neoadjuvant chemotherapy in vitro but also contribute to screening the drugs with diverse functions on different patients.8 By culturing the PDTOs from different breast cancer subtypes, Campaner et al demonstrated the feasibility of PDTOs in testing the efficacy of the standard treatment.21 Notably, in a previous study of advanced breast cancer, the patients receiving at least one drug that was indicated sensitive by the PDTO obtained good response,11 which supported our findings that the patient achieved partial response in liver metastatic lesions after use of the PDTO-highly sensitive drug sacituzumab govitecan.
To the best of our knowledge, this was the first study to describe a case of breast cancer with liver metastasis responding to sacituzumab govitecan that was shown highly sensitive by the PDTOs, highlighting that PDTOs could be used to test the response to monotherapy in advanced breast cancer patients previously receiving therapies. However, several limitations should be concerned. First, this was only a single case, largely affecting the generalization of the results. Second, a post-treatment tissue biopsy was missing. Additionally, the long-term outcomes were also absent due to a short follow-up period. In the future, a large-scale study with a long follow-up period should be conducted to further verify our findings.
Conclusion
In our case of TNBC, partial response is achieved in the liver metastatic lesions during the follow-up period after treatment with sacituzumab govitecan based on the PDTOs, unveiling that the PDTO, a potential companion tool for selection of treatment options, can facilitate the personalized treatment in metastatic TNBC patients to improve the prognosis.
Data Sharing Statement
The data generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
Written informed consent was obtained from the patient for publication of the health information in anonymised form. Institutional review board approval was not required, given the patient provided written consent.
Consent for Publication
The patient provided consent for publication of the case report and images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Harbeck N, Gnant M. Breast cancer. Lancet. 2017;389:1134–1150. doi:10.1016/S0140-6736(16)31891-8
2. Keenan TE, Tolaney SM. Role of immunotherapy in triple-negative breast cancer. J Natl Compr Canc Netw. 2020;18:479–489. doi:10.6004/jnccn.2020.7554
3. Yang R, Li Y, Wang H, et al. Therapeutic progress and challenges for triple negative breast cancer: targeted therapy and immunotherapy. Mol Biomed. 2022;3(1):8. doi:10.1186/s43556-022-00071-6
4. Bhatia S, Kramer M, Russo S, et al. Patient-derived triple-negative breast cancer organoids provide robust model systems that recapitulate tumor intrinsic characteristics. Cancer Res. 2022;82:1174–1192. doi:10.1158/0008-5472.CAN-21-2807
5. Yu J, Huang W. The progress and clinical application of breast cancer organoids. Int J Stem Cells. 2020;13:295–304. doi:10.15283/ijsc20082
6. Vargo-Gogola T, Rosen JM. Modelling breast cancer: one size does not fit all. Nat Rev Cancer. 2007;7:659–672. doi:10.1038/nrc2193
7. Hsu KS, Adileh M, Martin ML, et al. Colorectal cancer develops inherent radiosensitivity that can be predicted using patient-derived organoids. Cancer Res. 2022;82:2298–2312. doi:10.1158/0008-5472.CAN-21-4128
8. Vlachogiannis G, Hedayat S, Vatsiou A, et al. Patient-derived organoids model treatment response of metastatic gastrointestinal cancers. Science. 2018;359:920–926. doi:10.1126/science.aao2774
9. Rosenbluth JM, Schackmann RCJ, Gray GK, et al. Organoid cultures from normal and cancer-prone human breast tissues preserve complex epithelial lineages. Nat Commun. 2020;11:1711. doi:10.1038/s41467-020-15548-7
10. Shu D, Shen M, Li K, et al. Organoids from patient biopsy samples can predict the response of BC patients to neoadjuvant chemotherapy. Ann Med. 2022;54:2581–2597. doi:10.1080/07853890.2022.2122550
11. Chen P, Zhang X, Ding R, et al. Patient-derived organoids can guide personalized-therapies for patients with advanced breast cancer. Adv Sci. 2021;8:e2101176.
12. Gradishar WJ, Anderson BO, Abraham J, et al. Breast cancer, version 3.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2020;18:452–478. doi:10.6004/jnccn.2020.0016
13. Park IH, Im SA, Jung KH, et al. Randomized open label Phase III trial of irinotecan plus capecitabine versus capecitabine monotherapy in patients with metastatic breast cancer previously treated with anthracycline and taxane: PROCEED Trial (KCSG BR 11-01). Cancer Res Treat. 2019;51:43–52. doi:10.4143/crt.2017.562
14. Pasha N, Turner NC. Understanding and overcoming tumor heterogeneity in metastatic breast cancer treatment. Nat Cancer. 2021;2:680–692. doi:10.1038/s43018-021-00229-1
15. Syed YY. Sacituzumab Govitecan: first Approval. Drugs. 2020;80:1019–1025. doi:10.1007/s40265-020-01337-5
16. Bardia A, Hurvitz SA, Tolaney SM, et al. Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. 2021;384:1529–1541. doi:10.1056/NEJMoa2028485
17. Yang L, Liu B, Chen H, et al. Progress in the application of organoids to breast cancer research. J Cell Mol Med. 2020;24:5420–5427. doi:10.1111/jcmm.15216
18. Weeber F, Ooft SN, Dijkstra KK, et al. Tumor organoids as a pre-clinical cancer model for drug discovery. Cell Chem Biol. 2017;24(9):1092–1100. doi:10.1016/j.chembiol.2017.06.012
19. Mauri G, Durinikova E, Amatu A, et al. Empowering clinical decision making in oligometastatic colorectal cancer: the potential role of drug screening of patient-derived organoids. JCO Precis Oncol. 2021;5:
20. Psilopatis I, Mantzari A, Vrettou K, et al. The role of patient-derived organoids in triple-negative breast cancer drug screening. Biomedicines. 2023;11(3):773. doi:10.3390/biomedicines11030773
21. Campaner E, Zannini A, Santorsola M, et al. Breast cancer organoids model patient-specific response to drug treatment. Cancers. 2020;12:3869. doi:10.3390/cancers12123869
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.