")
Back to Journals » International Medical Case Reports Journal » Volume 16
Partial Obstruction of the Endotracheal Tube by a Part of the Metallic Stylet; Case Report and Review of the Literature
Authors Assiri AM , Alhelali A, AL-Benhassan I, Abo Hamed S, Alkathiri A, Miskeen E , Alqarny M
Received 27 March 2023
Accepted for publication 17 August 2023
Published 24 August 2023 Volume 2023:16 Pages 485—489
DOI https://doi.org/10.2147/IMCRJ.S414298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdullah M Assiri,1 Abdullah Alhelali,2 Ibrahim AL-Benhassan,3 Saeed Abo Hamed,3 Assaf Alkathiri,2 Elhadi Miskeen,4 Mohammed Alqarny5
1Department of Surgery, College of Medicine, Najran University, Najran, Saudi Arabia; 2Otolaryngology Department, Abha Children Hospital & Aseer Central Hospital, Abha, Saudi Arabia; 3Pediatric Critical Care Unit, Abha Maternity and Children Hospital, Abha, Saudi Arabia; 4Department of Obstetrics and Gynecology, College of Medicine, University of Bisha, Bisha, Saudi Arabia; 5Otolaryngology Head and Neck Surgery, Department of Surgery, College of Medicine, University of Bisha, Bisha, Saudi Arabia
Correspondence: Mohammed Alqarny, Department of Surgery, College of Medicine, University of Bisha, P.O. Box 0011, Bisha, Asir, 61922, Saudi Arabia, Email [email protected]
Abstract: Endotracheal intubation is common in the emergency department, intensive care units, and operating rooms. It involves the insertion of an endotracheal tube (ETT) through the mouth or nose into the trachea to maintain a patent airway and facilitate mechanical ventilation. Using a stylet during intubation can guide the ETT through the vocal cords. However, complications can arise when the stylet is not removed after successful intubation. Herewith, we reported a patient who was two years old and suffered from respiratory failure. However, in the first 12 hours, we observed a foreign body in the trachea, a small end of a metal stylet immediately removed by bronchoscope. This case demonstrates that multiple uses of a stylet, especially by a single user, can result in impaction of the stylet in the ETT during intubation, requiring force when the stylet is withdrawn after intubation, which can result in breakage, shearing, and retention of the stylet or plastic sheath in the lumen of the ETT.
Keywords: stylet, foreign body, Saudi Arabia
Introduction
Partial obstruction of the endotracheal tube by a metallic stylet is a rare and potentially life-threatening complication encountered during intubation procedures.1 The endotracheal tube is a critical device to secure the airway and facilitate mechanical ventilation in patients undergoing anesthesia or those requiring respiratory support.2 While endotracheal intubation is a routine and essential procedure in various medical settings, complications associated with using adjunct devices, such as the metallic stylet, can pose unique challenges to healthcare professionals.3
The metallic stylet is a rigid and flexible instrument commonly employed to aid intubation. Its purpose is to guide the endotracheal tube smoothly into the trachea, ensuring proper placement and effective ventilation.4 However, in rare instances, the metallic stylet can become dislodged or mispositioned inside the endotracheal tube, leading to partial airway obstruction.5
Difficult airways are commonly encountered in clinical practice, especially in emergencies. Difficulty airway is estimated as 20%, with about 1% failure. Many devices have been used and known in current practice, including the metallic stylet, to facilitate managing the difficult airway and for routine intubation.5,6
Because this complication is rare and unpredictable, healthcare professionals may not be familiar with its presentation or diagnosis.7 Recognizing the signs and symptoms early is crucial for prompt intervention and avoiding adverse outcomes.8,9
In acute respiratory status deterioration in the pediatric intensive care unit, equipment failure is among the most common causes.10,11 An obstructed endotracheal tube (ETT) is a common cause of ventilatory or oxygen delivery failure.12 It is common for the ETT to become obstructed by secretions. Nevertheless, we present a case in which part of the metal stylet obstructs the ETT’s lumen during intubation.13
Several case reports and retrospective studies have documented partial obstruction of the endotracheal tube due to the metallic stylet becoming dislodged or malpositioned inside the tube.14–16 These reports underscore the importance of vigilance during intubation and the need to recognize this rare but critical complication early.
In a study conducted by Sahin et al in 2020, they reported a case of partial endotracheal tube obstruction. Using endotracheal tubes in sick infants may lead to potentially life-threatening airway obstruction. Therefore, inspecting these tubes before use17 carefully is imperative.
In another study by Kim et al, a series of cases of partial airway obstruction due to dislodged stylets was reviewed. The authors highlighted the unpredictability of this complication and recommended increased awareness among healthcare providers to diagnose and manage it18 promptly.
Management of partial endotracheal tube obstruction caused by a metallic stylet involves immediate recognition and prompt intervention. O’Connor et al reported the successful resolution of a case by carefully withdrawing the metallic stylet under bronchoscopic guidance, restoring adequate airway patency.9 In contrast, Akins et al discussed a case where delayed complication recognition led to severe hypoxemia and necessitated emergent reintubation. The report highlights the importance of regular monitoring and vigilant post-intubation assessments.19
The significance of this case report lies in its potential to raise awareness among clinicians, anesthesiologists, and critical care teams about the risks associated with using metallic stylets during intubation. Through an in-depth examination of the literature and a critical analysis of similar reported cases, this report aims to contribute to the existing knowledge on this subject and emphasize the importance of vigilant airway management practices.
Herewith, we document the successful treatment of a pediatric patient with respiratory failure due to partial obstruction of the endotracheal tube by a portion of the metal stylet.
Case Report
A two-year-old boy presented with respiratory failure due to covid-19. The patient needed intubation, so he was intubated with a 4.5cc ETT. Intubation was performed in the second attending and with a metal stylet during both attendings. However, we noticed difficulty in removing the stylet. After intubation, the patient maintained his oxygen saturation and had good air entry into both sides of the lungs. Unfortunately, we did not notice that the stylet was slightly short after removal. In the first 6 hours, unexplained short desaturations occurred repeatedly. After intubation, radiography was performed, and it was suspected that there was a remnant in the trachea at the level of the bifurcation. The patient developed pneumothorax, and a chest tube was placed. Then we observed an accumulation of CO2 in the VBGs in the first 6 hours. Suction was performed, and we had difficulty aspirating the endotracheal tube. A chest radiograph showed a foreign body (Stylet’s part) in the tube and trachea (see Figures 1 and 2). We checked the intubation kits and found that a stylet was booked at the end.
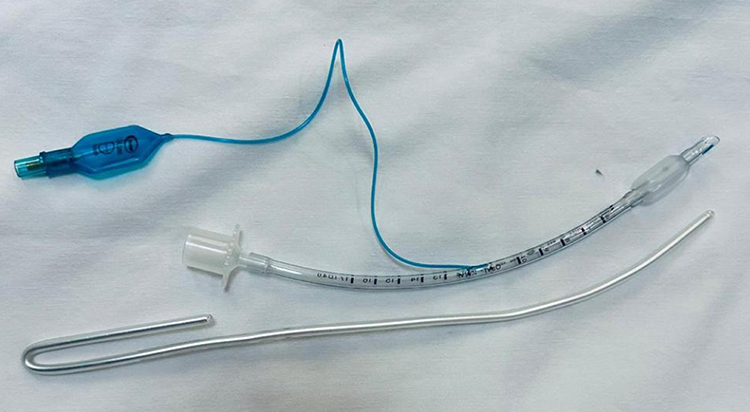 |
Figure 1 Stylet. |
 |
Figure 2 Shows a foreign body (Stylet’s part) in the tube and trachea. |
The otolaryngology team was called in. The flexible endoscope shows the stylet tip in the trachea. The endotracheal tube was removed, and a rigid bronchoscopy was performed. A stylet was retrieved with telescopic forceps. The patient was easily reintubated after the procedure. After removing that part, the patient’s condition improved regarding ventilation with the same oxygenation issue. After removal, there was an immediate improvement in tidal volumes and peak airway pressures.
Discussion
Partial obstruction of an ETT can lead to significant respiratory compromise and requires prompt intervention to prevent hypoxia and hypercapnia. Using a stylet during intubation can aid in guiding the ETT through the vocal cords, but it should be removed after successful intubation to prevent complications.
Airway obstruction due to a foreign body should be regularly reported. However, medical device involvement is common and results in severe respiratory morbidities.15–17
Any stylet can lead to such a problem. Either multiple used metallic stylet or coated stylet with plastic. Also, offering stylet can contribute to this problem, or using a single used one for multiple users specifically with lousy quality. Although, few cases were reported with blocked ETT tubes by stylet or any part.18,19
An earlier report described a child intubated with a stylet at 24 weeks gestational age on the 16th day of life. It required considerable effort by the physician to remove the stylet after intubation. After removing the plastic stylet, the infant’s condition improved dramatically.20 One month after the repair of a bilateral inguinal hernia, an infant experienced the removal of the plastic tip of the stylet, and the stylet was released. There was a case of two large plastic fragments detaching from a stylet when he was intubated at age 27 after trauma. A few hours later, a piece was removed from the endotracheal tube, and the result was satisfactory.21,22
Multiple other factors can increase these events, like firmly holding the ETT the clinician during the removal of the stylet after intubation or quickly and firmly pulling the stylet out.23–27 In our case, the cause of this event was using multiple used stylet and a single user.
Increased awareness among healthcare providers is vital to promptly diagnose and manage this complication. The case report and literature review serve as valuable educational tools for healthcare professionals, highlighting the importance of recognizing early signs of airway obstruction and employing appropriate interventions.
Conclusion
A metallic object’s partial obstruction of an ETT can lead to significant respiratory compromise and requires prompt intervention. Using a stylet during intubation can aid in guiding the ETT through the vocal cords, but it should be removed after successful intubation to prevent complications. Proper technique should be used during removal to prevent dislodgement and equipment migration into the ETT lumen.
This case demonstrates that multiple uses of a stylet, especially by a single user, can result in impaction of the stylet in the ETT during intubation, such that an effort to pull the stylet out after intubation can result in breakage, shearing, and entrapment of the stylet or plastic sheath in the lumen of the ETT. Also, checking the equipment before and after intubation, not in quantity base also in quality, it’s important and can prevent this from happening or at least quickly discover it after happening.
Abbreviations
ETT, Endotracheal tube; O2, oxygen; Co2, carbon dioxide.
Ethical Cosideration
We confirming that written informed consent has been provided by the parents to have the case details and accompanying images published. The IRB from University of Bisha, college of medicine was approved the case for publication after revised the informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, execution, acquisition of data, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
No conflict of interest was reported.
References
1. Xia M. Complications associated with anesthesia: in oral and maxillofacial surgery. In: Anesthesia for Oral and Maxillofacial Surgery. Singapore: Springer Nature Singapore;2023:125–144. doi:10.1007/978-981-19-7287-4_9
2. Chavez CL, Macias AM, Bárcenas CD, Molina AI, Villalobos MP. Special considerations in pediatrics for rapid intubation sequence. Int J Med Sci Clin Res Stud. 2023;3(06):1067–1071. doi:10.47191/ijmscrs/v3-i6-06
3. Hansel J, Law JA, Chrimes N, et al. Clinical tests for confirming tracheal intubation or excluding oesophageal intubation: a diagnostic test accuracy systematic review and meta‐analysis. Anaesthesia. 2023;78(8):1020–1030. doi:10.1111/anae.16059
4. Pirotte A, Panchananam V, Finley M, et al. Current considerations in emergency airway management. Curr Emerg Hosp Med Rep. 2022;10(4):73–86. doi:10.1007/s40138-022-00255-y
5. Ito M, Watanabe N, Sawado Y, et al. An unusual foreign body in the oral cavity: a case report from a patient safety point of view and literature review. J Anesth. 2022;36(4):564–571. doi:10.1007/s00540-022-03087-y
6. Sagarin MJ, Barton ED, Chng YM, Walls RM; National Emergency Airway Registry (NEAR) Investigators. Airway management by US and Canadian emergency medicine residents: a multicenter analysis of more than 6000 endotracheal intubation attempts. Ann Emerg Med. 2005;46(4):328–336. doi:10.1016/j.annemergmed.2005.01.009
7. Gambato M, Scotti N, Borsari G, et al. Chest X-ray interpretation: detecting devices and device-related complications. Diagnostics. 2023;13(4):599. doi:10.3390/diagnostics13040599
8. Williamson E, Ratnasabapathy U. Anaesthesia for maxillofacial surgery. Anaesth Intens Care Med. 2023;24(8):455–460. doi:10.1016/j.mpaic.2023.05.010
9. Kostyk P, Francois K, Salik I. Airway anesthesia for awake tracheal intubation: a review of the literature. Cureus. 2021;13:7. doi:10.7759/cureus.16315
10. Riphagen S, Bird R, von Ungern‐Sternberg B. Ventilatory management of critically ill children in the emergency setting, during transport and retrieval. Pediatric Anesth. 2022;32(2):330–339. doi:10.1111/pan.14358
11. Nishisaki A, Ferry S, Colborn S, et al. Characterization of tracheal intubation process of care and safety outcomes in a tertiary pediatric intensive care unit. Pediatric Crit Care Med. 2012;13(1):e5–e10. doi:10.1097/PCC.0b013e3181fe472d
12. Vivas Fernández FJ, Sánchez Segovia J, Martel Bravo I, et al. Res (Uhu) rge: a low cost and fully functional ventilator indicated for application in COVID-19 patients. Sensors. 2020;20(23):6774.
13. Patil VP, Trivedi BD, Desai MD. Double lumen tubes and bronchial blockers. In: Understanding Anesthetic Equipment & Procedures: A Practical Approach. Jaypee Brothers Medical Publishers; 2021:184. Available from: https://books.google.com.sa/.
14. Lee Y-H, Su C-H, Lin C-Y, et al. Endoscopic and image analysis of the airway in patients with mucopolysaccharidosis type IVA. J Personal Med. 2023;13(3):494. doi:10.3390/jpm13030494
15. Shafeeq A, Imad HA, Azhad A, et al. A fatal case of native valve endocarditis with multiple embolic phenomena and invasive methicillin-resistant Staphylococcus aureus bacteremia: a Case Report from the Maldives. Trop Med Infect Dis. 2023;8(1):53. doi:10.3390/tropicalmed8010053
16. Roy S, Santosh KC. Analyzing overlaid foreign objects in chest X-rays—clinical significance and artificial intelligence tools. In: Healthcare. MDPI; 2023:308. doi:10.3390/healthcare11030308
17. Evren Sahin K, Salman Onemli C. Difficult ventilation in an infant after successful intubation. Turkish J Anaesthesiol Reanim. 2022;50(4):303–305. doi:10.5152/TJAR.2021.21191
18. Kim CY, Cho S, Ryoo S-H. Anesthetic management for emergency tracheostomy in patients with head and neck cancer: a case series. J Dental Anesth Pain Med. 2022;22(6):457. doi:10.17245/jdapm.2022.22.6.457
19. Akins PT, Ledgerwood LG, Duong HT. Early and late complications after open and endoscopic neurosurgery for complex skull base and craniofacial pathology: case series, illustrative cases, and review. Interdiscipl Neurosurg. 2022;29:101552. doi:10.1016/j.inat.2022.101552
20. Shapiro NL, Kaselonis GL. Tracheobronchial foreign body management in an acutely ill neonate. Int J Pediatr Otorhinolaryngol. 2000;52(1):75–77. doi:10.1016/S0165-5876(99)00294-3
21. Garcia-Aparicio L, Castanon M, Tarrado X, Rodriguez L, Iriondo M, Morales L. Bronchial complication of a closed-tube endotracheal suction catheter. J Pediatr Surg. 2002;37(10):1483–1484. doi:10.1053/jpsu.2002.35422
22. Nurkin S, Waisman D, Davkin O, Kessel I, Vinograd I, Rotschild A. A rare complication of the closed tracheal suction system. J Pediatr. 2004;145(6):858. doi:10.1016/j.jpeds.2004.06.048
23. Chalhoub V, Richa F, El-Rassi I, Dagher C, Yazbeck P. Pulmonary migration of a fragment of plastic coating sheared from a stylet. J Emerg Med. 2013;44(6):1097–1100. doi:10.1016/j.jemermed.2012.11.004
24. Bhargava M, Pothula SNM, Joshi S. The obstruction of an endotracheal tube by the plastic coating sheared from a stylet: a revisit. Anesthesiology. 1998;88(2):548–549. doi:10.1097/00000542-199802000-00043
25. Das A, Chagalamarri S, Saridakis K. Partial obstruction of the endotracheal tube by the plastic coating sheared from a stylet. Case Rep Pediatr. 2016;2016:2. doi:10.1155/2016/4373207
26. Kemper M, Imach S, Buehler PK, Thomas J, Dave M, Weiss M. Tube tip and cuff position using different strategies for placement of currently available paediatric tracheal tubes. Br J Anaesth. 2018;121(2):490–495. doi:10.1016/j.bja.2018.05.002
27. Dillier CM, Trachsel D, Baulig W, Gysin C, Gerber AC, Weiss M. Laryngeal damage due to an unexpectedly large and inappropriately designed cuffed pediatric tracheal tube in a 13-month-old child. Can J Anesth. 2004;51(1):72–75. doi:10.1007/BF03018551
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.