")
Back to Journals » Patient Preference and Adherence » Volume 16
Parental Knowledge and Awareness of Childhood Urinary Tract Infections: A Cross Sectional Survey
Authors Almatrafi MA, Sindi L , Alshehri M , Sendi E , Sindi G , Alzahrani G , Alwan J, Salawati E , Alwafi H , Minshawi F , Mosalli R, Samannodi M
Received 6 February 2022
Accepted for publication 1 August 2022
Published 1 September 2022 Volume 2022:16 Pages 2423—2430
DOI https://doi.org/10.2147/PPA.S361313
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Mohammed A Almatrafi,1 Lama Sindi,2 Malak Alshehri,2 Esraa Sendi,2 Ghufran Sindi,2 Ghaida Alzahrani,2 Joud Alwan,2 Emad Salawati,3 Hassan Alwafi,4 Faisal Minshawi,5 Rafat Mosalli,1 Mohammed Samannodi6
1Department of Pediatrics, Umm Al-Qura University, Makkah, Saudi Arabia; 2Medical College of Umm Al-Qura University, Makkah, Saudi Arabia; 3Department of Family Medicine, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 4Department of Pharmacology and Toxicology, Umm Al-Qura University, Makkah, Saudi Arabia; 5Department of Laboratory Medicine, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia; 6Department of Medicine, College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Mohammed Samannodi, Department of Medicine, College of Medicine, Umm Al-Qura University, Makkah, 21955, Saudi Arabia, Tel +966548293937, Fax +966125502188, Email [email protected]
Background: Parent’s misconceptions or lack of knowledge about childhood urinary tract infections (UTIs) can negatively impact their children’s health. Therefore, the present study aimed to determine the childhood urinary tract infections awareness and understanding among parents in Saudi Arabia.
Patients and Methods: An online validated cross-sectional survey of parents in Saudi Arabia was conducted from August to September 2021. Study participants who met the inclusion criteria were selected using a convenience sampling technique. A questionnaire with two domains was used to assess parental awareness of childhood urinary tract infection symptoms, complications, treatment, prevention, epidemiology, and diagnosis. The total childhood urinary tract infections awareness scores were classified into three categories: low awareness, moderate awareness, and high awareness. Descriptive statistics were used to determine the data distribution. A chi-square test was used to evaluate the relationship between parental awareness about urinary tract infections in children and other variables. Statistical significance was established at 0.05.
Results: Of the 1688 parents who completed the survey, 1289 (76.4%) were female, 1581 (93.7%) were married, and 1161 (68.8) had a university degree. Parent’s total awareness scores were high; however, individual domain scores indicate a moderate level of knowledge. Statistically significant relationship were observed between total awareness and gender, occupation, and level of educational level ((P=0.004, P=0.001, P=0.007, respectively). Another statistically significant relationship was noted between the history of urinary tract infections and awareness of disease prevention (P=0.009).
Conclusion: In Saudi Arabia, parental knowledge about childhood urinary tract infections is moderate to high. However, future studies are needed to investigate gender, educational, and occupational variations in childhood UTI knowledge among parents in Saudi Arabia.
Keywords: urinary tract infections, awareness, parents, childhood
Introduction
Urinary tract infections (UTIs) are one of the most common bacterial infections pediatric patients.1 Females, uncircumcised males, and infants are at a higher risk of developing UTIs.2 Childhood UTIs prevalence varies considerably based on gender and age.3 In the first year of life, approximately 0.7% of girls and 2.7% of uncircumcised boys develop UTIs.4,5 However, females older than one year are significantly more likely to develop UTIs than male. In fact, 7.8% of girls and 1.7% of boys typically contract a UTI by the age of seven years.2,6–10
Clinical manifestations of UTIs also vary according to age. Infants and young children under two years old commonly experience nonspecific symptoms, such as unexplained fevers, poor feeding, vomiting, diarrhea, and foul-smelling urine.2 In contrast, older children have more specific UTI symptoms and signs, including fever, suprapubic abdominal pain, and urinary symptoms such as dysuria, urgency, frequency, new-onset nocturnal enuresis, and incontinence.2,11,12 Patients with symptoms and signs suggestive of a UTI should be evaluated with a comprehensive medical assessment, including a detailed medical history, a thorough physical examination and sending urine samples for microscopic and macroscopic urine sample evaluations and a urine culture.1,13
Clinically, UTIs can be classified as uncomplicated or complicated infections. Complicated UTIs are defined by one or more of the following criteria: critical illness (eg, severe urosepsis or shock), recurrent UTIs with underlying anatomical defects in the genitourinary system, nephrogenic abscesses, and the absence of clinical improvement within 48 hours despite appropriate therapy. Uncomplicated UTIs are typically confined to the urinary bladder and occur in healthy individuals with no structural abnormalities.1,14
During acute infections, 5.6% of pediatric patients with UTIs may develop bacteremia.15 Renal scarring may be seen in up to 5% of girls and 13% of boys following their first symptomatic episode of pyelonephritis.16,17 Furthermore, 10% of children with recurrent UTIs are at risk of developing hypertension, which might result in renal scarring and chronic renal failure.2,4,18 UTI recurrence rates range from 30% to 50%, with females disproportionately affected.9,16,19
Parent’s misconceptions about their children’s illnesses can negatively affect their children’s health.20 Given parents’ typically close relationships with their children, they must be provided with information about diagnostic and treatment options so that they can make correct decisions about their children’s health.21 Several studies have revealed that some parents are unaware of UTI symptoms and long-term health sequelae and lack trust in healthcare providers as sources of information regarding UTIs.21,22 They can also be frustrated by diagnostic and treatment delays and a lack of knowledge among healthcare providers regarding UTIs in children.21,22 A good understanding of these factors can help improve strategies for detecting UTIs in general practice.23 Parental understanding of the disease can facilitate their children’s treatment, prevent a recurrence, and resolve behavioral or emotional issues. Moreover, when parents are informed about their children’s health, the treatment process moves more rapidly.20
In Saudi Arabia, there is limited evidence addressing parental awareness of childhood UTIs. Therefore, the present study aimed to assess parental awareness of UTIs in infants and children and associated demographic characteristics in order to improve the quality of life and care of children in Saudi Arabia.
Materials and Methods
Study Design and Study Population
A validated online cross-sectional survey of Saudi Arabian parents was conducted from August to September 2021 to assess parental knowledge and the understanding of UTIs in children. Parents of children under 18 who reside in Saudi Arabia, regardless of the previous history of childhood UTIs were included to participate in the study. Parents with adult children older than 18 years or who did not reside in Saudi Arabia were excluded from this study.
Sampling Strategy
Study participants who meet the inclusion criteria were selected using a convenience sampling technique. A validated survey tool was distributed electronically using social media networks. Numerous reminders were sent in an attempt to boost response rates. Only those participants who met the inclusion criteria and completed the questionnaires were included in the final analysis.
Questionnaire Tool
A questionnaire that had previously been validated was adapted.20 Three independent experts translated the questionnaire into Arabic and validated it using the forward–backward translation technique. The first questionnaire domain includes questions about the demographic data of parents and children and parental awareness of childhood UTIs. The demographic data provides information about the parents (age, gender, region of residence, marital status, educational level, and occupation) and their children (number of children in the family unit, number of children with a history of UTIs or recurrent UTIs).
The second questionnaire domain contains 35 items assessing parental awareness of childhood UTI symptoms, complications, treatment, prevention, epidemiology, and diagnosis. Correct answers to easy questions (1, 5, 6, 9, 16, 21, 27, 35) were worth 1 point, while questions of medium (2–4, 7, 10–15, 18–20, 23–26, 29–31, 33–34) and higher difficultly (8, 17, 22, 28, 32) were worth 2 and 3 points, respectively. Incorrect responses resulted in a score of zero. The total awareness score was divided into three categories: 0–22 (low awareness), 23–45 (moderate awareness), and 46–67 (high awareness).
Sample Size
The sample size was determined using World Health Organization (WHO) guidelines. The target sample size was 385 participants to achieve a 95% confidence interval and a 5% margin of error.
Statistical Analysis
The statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS). Frequencies and percentages were used to report categorical variables. A chi-square test was used to determine the relationship between parental awareness of symptoms, treatment, complications, prevention, diagnosis, and total score and the parent’s age, gender, marital status, occupation, educational level, and child’s UTI history. P-values less than 0.05 were considered significant.
Ethical Statement
The study was approved by the Biomedical Ethics Committee at Umm Al-Qura University. Full consent for enrollment was included in the questionnaire, and all information regarding the study participants was treated with the utmost confidentiality. Each respondent was informed of the study objectives and fully consented to participate. The study was conducted in accordance with the Declaration of Helsinki.
Results
Of the 1688 parents, 76.4% were mothers, and 34.4% were aged 31–40. 84.4% of parents reported no history of UTIs in their children, and 8.2% reported recurrent UTIs. (Table 1). Our study participants’ mean total score for awareness of childhood UTI was 47.3±8.4, indicating a high awareness level. Yet, individual mean scores for each domain of the questionnaire were indicating a moderate to a high level of awareness for all individual domains (Table 2). Regarding the questionnaire, the least correct response was for the item “If you have a history of previous urinary tract infections, you can take the same medicine every time you have a fever without seeing a doctor” (345 participants or 20.4%) (see Supplementary Table 1). The results revealed a statistically significant relationship between parent’s gender, occupation, and educational level with the total score for parental awareness of childhood UTIs (P=0.004, P=0.001, P=0.007, respectively) (Table 3). Males, employed parents, and those with university degrees had a higher number of correct responses in all significant domains (Table 3). However, there was no significant relationship between parent’s age and history of previous UTIs with the total score for parental awareness of childhood UTIs (Table 3).
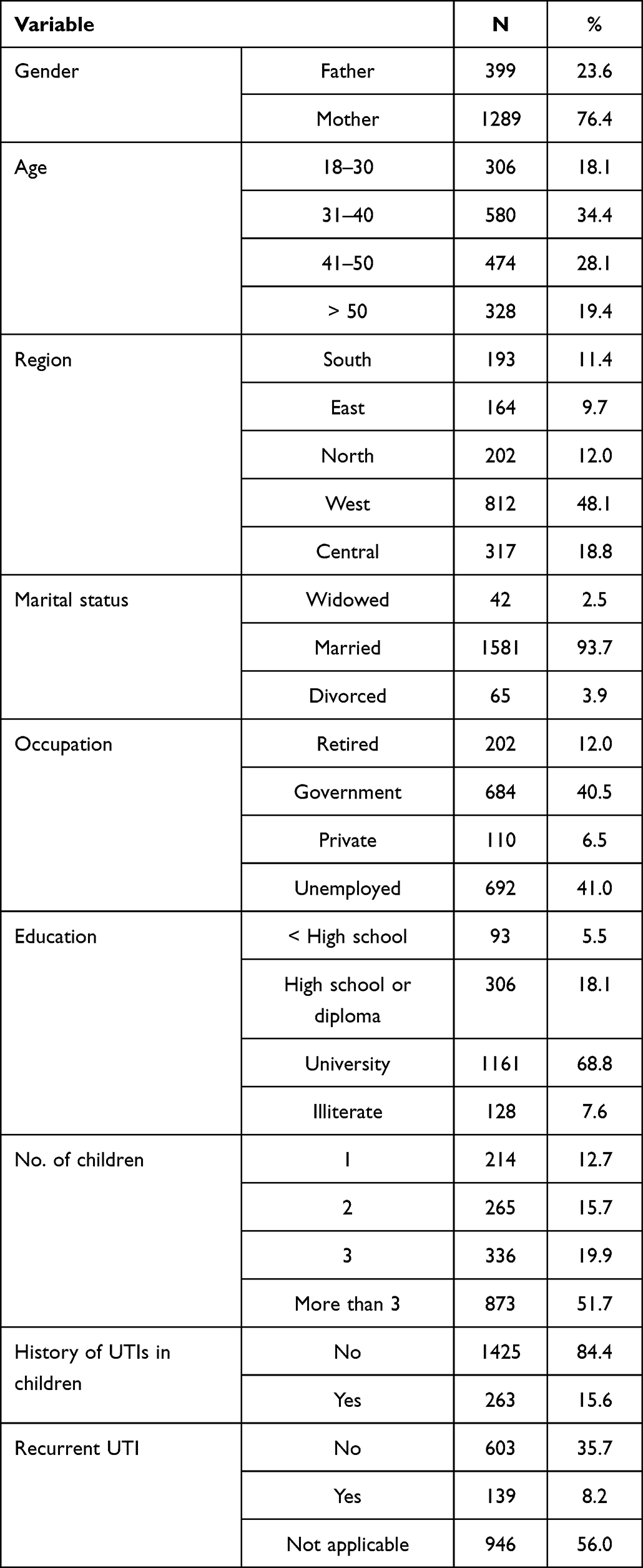 |
Table 1 Participants’ Demographic Data |
 |
Table 2 Scores for Parental Awareness of Childhood UTIs |
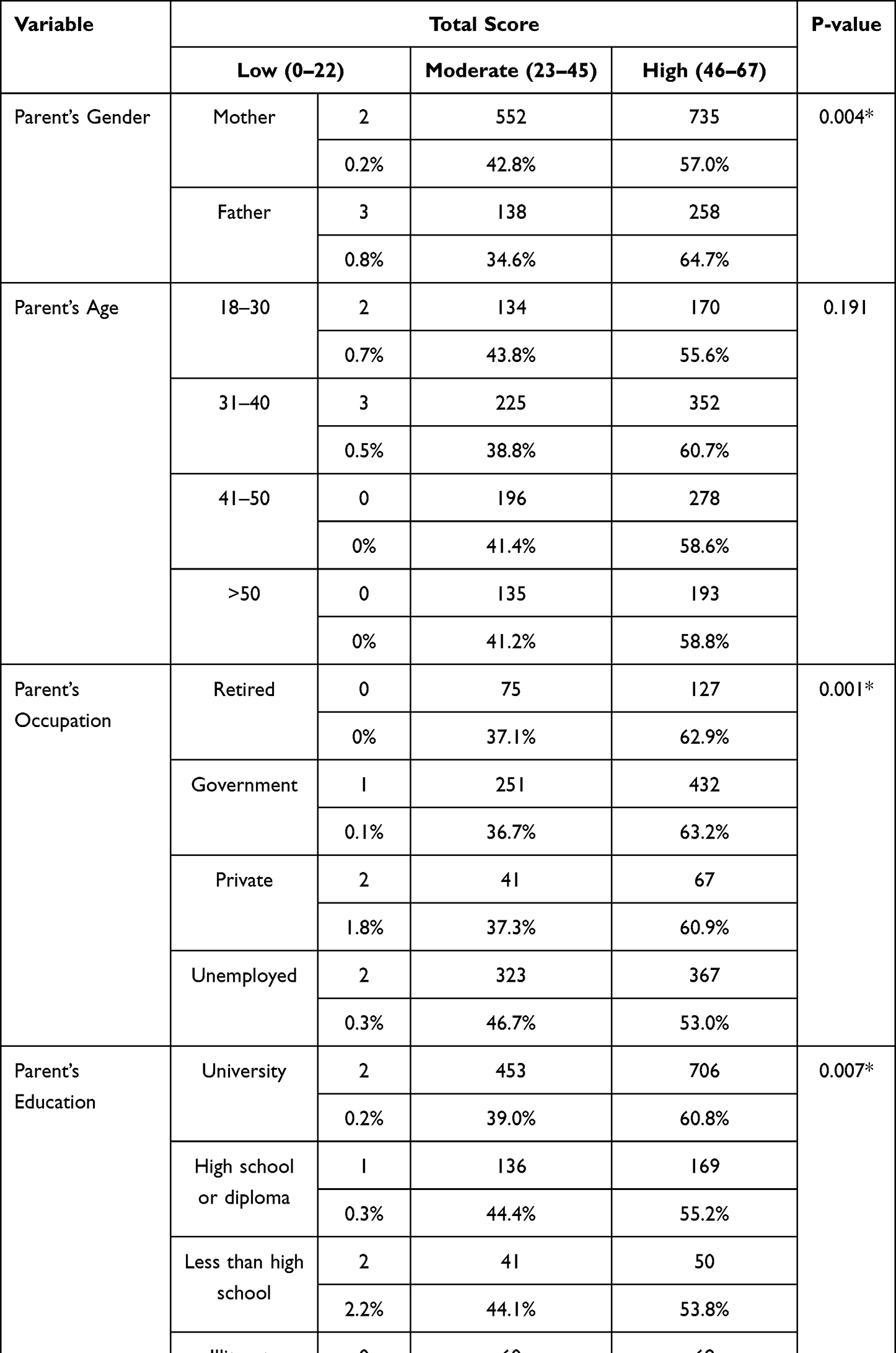 |
Table 3 Predictors Associated with the Total Score for Parental Awareness of Childhood UTIs |
Discussion
This study aimed to determine parent’s awareness and knowledge of childhood UTIs. Most study participants were middle-aged parents who lived in the western and central regions of Saudi Arabia, the areas in the country with the highest population density.24 Our study findings showed that 58.8% of the participants had a high total awareness score regarding childhood UTIs (47.3±8.4). However, previous studies conducted in other countries have reported a moderate to low parental awareness of childhood UTIs.20,23,25
Numerous studies have assessed parental awareness of various health issues, including UTIs, and found that mothers are more knowledgeable than fathers.20,25,26 However, in the present study, fathers (64.7%) had a higher overall awareness of childhood UTIs than mothers (57%). Meanwhile, previous studies have found that a high level of understanding is correlated with a higher level of education.20,25,26 Similarly, in our study, heightened awareness directly corresponded to level of education. Furthermore, even though education can significantly reduce UTI recurrence and complications, financial constraints could negatively influence knowledge due to unsatisfactory educational attainment.27 For instance, this report found that unemployed parents had lower total awareness scores than retired or employed parents.27
Although the participants in the present study had a high overall awareness of UTIs, their level of knowledge about UTI symptoms was moderate. A lower percentage of correct responses was observed for questions about atypical UTI presentation. Likewise, in an interview-based qualitative study, Harmsen et al found that most parents had a lower awareness of atypical UTI symptoms.23 Meanwhile, a systematic review of 2726 parents revealed that most of the participants could not recognize UTI symptoms and lacked adequate information about tests and treatments, resulting in misdiagnoses or noncompliance with treatment.21 These findings could be partly attributed to the fact that a significant percentage of pediatric UTI cases present with atypical symptoms and that parents may overlook the possibility of a UTI as an etiology, thus hampering early recognition.
Campbell et al found that parents whose children have had at least one UTI could recognize the symptoms and signs of childhood UTIs earlier.28 In a study of parents’ opinions about diagnosing UTIs in children, Owen et al found that most of the participants believed that health care providers have low childhood UTI awareness levels and do not promptly investigate the possibility of UTIs in children.22 Practical uncertainties, inadequate knowledge, and financial expenses are health care professionals’ most common obstacles to identifying UTIs.22 Therefore, it is imperative to distribute current guidelines to health care providers and their raise awareness of UTIs.22 Efforts to increase parental and provider awareness of UTI symptoms, particularly regarding children presenting with atypical signs and symptoms, may lead parents to seek prompt medical advice and implement preventative interventions, thereby averting potential consequences.
Potential short-term consequences of recurrent UTIs in children include an increased risk of developing sepsis and infections caused by multidrug-resistant organisms.1 If such infections are not prevented, children can develop renal scarring, hypertension, and chronic kidney disease.2 As mentioned in the literature, uncircumcised boys and children with chronic constipation have a higher risk of recurrent UTIs, thus increasing the risk of complications and morbidity.1 In our study, a considerable percentage of participants gave incorrect responses when asked about the relationship between chronic constipation, circumcision, and UTI occurrence (44.3% and 77.5%, respectively). Therefore, it is crucial to identify parental knowledge gaps regarding childhood UTI prevention and complications during clinical encounters at continuity and well-child clinics.2,29,30
This study has some limitations. First, convenience sampling may present a challenge in terms of sample representation. However, given the increased use of online platforms and social media during the COVID-19 pandemic, an adequate sample representation was assumed. Second, recall bias cannot be ruled out because of the cross-sectional nature of the study. Third, the questionnaire tool was written entirely in Arabic, which impeded those who did not understand the language.
Conclusion
According to our findings, parents in Saudi Arabia have a high level of awareness of childhood UTIs. However, they have a lower awareness of atypical UTI symptoms, which could increase the risk of delayed diagnosis and subsequent complications. Future studies should investigate how gender, educational, and occupational variations affect childhood UTI awareness among parents in Saudi Arabia.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Albarrak M, Alzomor O, Almaghrabi R, et al. Diagnosis and management of community-acquired urinary tract infection in infants and children: clinical guidelines endorsed by the Saudi pediatric infectious diseases society (SPIDS). Int J Pediatr Adolesc Med. 2021;8(2):57–67. doi:10.1016/j.ijpam.2021.03.001
2. Leung AK, Wong AH, Leung AA, Hon KL. Urinary tract infection in children. Recent Pat Inflamm Allergy Drug Discov. 2019;13(1):2–18. doi:10.2174/1872213X13666181228154940
3. Almofarreh M, Alowaa Z, Junainah E, et al. Prevalence of urinary tract infection among children. Int J Contemp Pediatr. 2018;5(6):2356–2359. doi:10.18203/2349-3291.ijcp20183878
4. Chang SL, Shortliffe LD. Pediatric urinary tract infections. Pediatr Clin. 2006;53(3):379–400. doi:10.1016/j.pcl.2006.02.011
5. Simoes e Silva AC, Oliveira EA. Update on the approach of urinary tract infection in childhood. J Pediatr (Rio J). 2015;91:S2–S10. doi:10.1016/j.jped.2015.05.003
6. Radiology ACo. ACR appropriateness criteria: urinary tract infection—child. TractInfectionChildDoc10 aspx. 2010.
7. Schlager TA, Mulvey MA, Stapleton AE, Klumpp DJ. Urinary tract infections in infants and children. Microbiol Spectrum. 2016;4(5):
8. Zorc JJ, Kiddoo DA, Shaw KN. Diagnosis and management of pediatric urinary tract infections. Clin Microbiol Rev. 2005;18(2):417–422. doi:10.1128/CMR.18.2.417-422.2005
9. Stephens GM, Akers S, Nguyen H, Woxland H. Evaluation and management of urinary tract infections in the school-aged child. Primary Care. 2015;42(1):33–41. doi:10.1016/j.pop.2014.09.007
10. Larcombe J. Urinary tract infection in children. BMJ Clin Evid. 2010;2010:1173–1175.
11. Majd M, Rushton HG, Jantausch B, Wiedermann BL. Relationship among vesicoureteral reflux, P-fimbriated Escherichia coli, and acute pyelonephritis in children with febrile urinary tract infection. J Pediatr. 1991;119(4):578–585. doi:10.1016/S0022-3476(05)82407-2
12. Winberg J, Andersen H, Bergström T, Jacobsson B, Larson H, Lincoln K. Epidemiology of symptomatic urinary tract infection in childhood. Acta Paediatrica. 1974;63:1–20. doi:10.1111/j.1651-2227.1974.tb05718.x
13. Schmiemann G, Kniehl E, Gebhardt K, Matejczyk MM, Hummers-Pradier E. The diagnosis of urinary tract infection: a systematic review. Deutsches Ärzteblatt Int. 2010;107(21):361. doi:10.3238/arztebl.2010.0361
14. Sabih A, Leslie SW. Complicated urinary tract infections. 2017.
15. Megged O. Bacteremic vs nonbacteremic urinary tract infection in children. Am J Emerg Med. 2017;35(1):36–38. doi:10.1016/j.ajem.2016.09.060
16. Larcombe J. Urinary tract infection in children: recurrent infections. BMJ Clin Evid. 2015;2015:306.
17. Schlager TA. Urinary tract infections in infants and children. Infect Dis Clin. 2003;17(2):353–365. doi:10.1016/s0891-5520(03)00009-6
18. Blumenthal I. Vesicoureteric reflux and urinary tract infection in children. Postgrad Med J. 2006;82(963):31–35. doi:10.1136/pgmj.2005.036327
19. Korbel L, Howell M, Spencer JD. The clinical diagnosis and management of urinary tract infections in children and adolescents. Paediatr Int Child Health. 2017;37(4):273–279. doi:10.1080/20469047.2017.1382046
20. Seyezadeh A, Tohidi MR, Sameni M, Seyedzadeh MS, Hookari S. Assessment of parents’ awareness of Urinary Tract Infections (UTIs) in infants and children and related demographic factors: a cross-sectional study. J Comprehensive Pediatr. 2021;12(1). doi:10.5812/compreped.107529
21. Gates A, Shulhan J, Featherstone R, Scott SD, Hartling L. A systematic review of parents’ experiences and information needs related to their child’s urinary tract infection. Patient Educ Couns. 2018;101(7):1207–1215. doi:10.1016/j.pec.2018.01.014
22. Owen D, Vidal-Alaball J, Mansour M, Bordeaux K, Jones KV, Edwards A. Parent’s opinions on the diagnosis of children under 2 years of age with urinary tract infection. Fam Pract. 2003;20(5):531–537. doi:10.1093/fampra/cmg507
23. Harmsen M, Wensing M, van der Wouden JC, Grol RP. Parents’ awareness of and knowledge about young children’s urinary tract infections. Patient Educ Couns. 2007;66(2):250–255. doi:10.1016/j.pec.2006.12.009
24. Stats.gov.sa. Demographic research bulletin; 2021. Available from: https://www.stats.gov.sa/sites/default/files/en-demographic-research-2016_7.pdf.
25. Baghiani Moghadam M, Shojaeazadeh D, Mohamadloo A, Fallahzadeh H, Ranjbary M. Evaluation of preventive behaviors of UTI based on health belief model (HBM) in mothers with girls younger than 6 years old. Tolooebehdasht. 2013;12(1):78–88.
26. Alharbi MM, Almasri MS, Aldayel AY, Alkhonezan SM. Parental knowledge, attitudes and practices towards paediatric ear infections in Riyadh, Saudi Arabia: a quantitative study. Sultan Qaboos Univ Med J. 2019;19(2):e114–e21. doi:10.18295/squmj.2019.19.02.006
27. Navarro A, Tiongco RE, Bundalian R. Knowledge, attitude, practices, and health beliefs of pregnant women about urinary tract infection and its associated risk factors: a local Filipino community experience. Kesmas. 2019;14(2):82–87.
28. Campbell A, Hartling L, Louie-Poon S, Scott SD. Exploring the experiences and information needs of parents caring for a child with a urinary tract infection: a qualitative study. J Patient Experience. 2021;8:23743735211008299. doi:10.1177/23743735211008299
29. Tullus K, Shaikh N. Urinary tract infections in children. Lancet. 2020;395(10237):1659–1668. doi:10.1016/S0140-6736(20)30676-0
30. Kaufman J, Temple-Smith M, Sanci L. Urinary tract infections in children: an overview of diagnosis and management. BMJ Paediatr Open. 2019;3(1):e000487. doi:10.1136/bmjpo-2019-000487
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.