Back to Journals » Psychology Research and Behavior Management » Volume 19
Parental Knowledge, Acceptability, and Involvement in Applied Behavior Analysis for Children with Autism Spectrum Disorder in Jordan: A Cross-Sectional Study
Authors Al-Dwaikat TN, ALMomani RA, Khatatbeh H, Alqarawi N, Alothaim SS, Ali AM, Alasqah I ![]()
Received 30 November 2025
Accepted for publication 18 February 2026
Published 24 February 2026 Volume 2026:19 576856
DOI https://doi.org/10.2147/PRBM.S576856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gabriela Topa
Tariq N Al-Dwaikat,1 Rahmeh Ahmad ALMomani,1 Haitham Khatatbeh,2 Nada Alqarawi,3 Suliman S Alothaim,4 Amira Mohammed Ali,5 Ibrahim Alasqah3
1Community and Mental Health Nursing Department, Jordan University of Science and Technology Faculty of Nursing, Irbid, 22110, Jordan; 2Clinical Nursing Department, Faculty of Nursing, Yarmouk University, Irbid, 21163, Jordan; 3Department of Community, Psychiatric, and Mental Health Nursing, College of Nursing, Qassim University, Buraydah, 52571, Saudi Arabia; 4Department of Special Education, College of Education, Qassim University, Buraydah, 52571, Saudi Arabia; 5Department of Psychiatric Nursing and Mental Health, Faculty of Nursing, Alexandria University, Smouha, Alexandria, 21527, Egypt
Correspondence: Ibrahim Alasqah, Email [email protected]
Purpose: This study aims to evaluate parental knowledge, acceptability, and involvement in the use of Applied Behavior Analysis (ABA) for the treatment of children with autism spectrum disorder (ASD) in Jordan.
Methods: A descriptive cross-sectional study was conducted with a sample of 157 parents of children with ASD who had been exposed to ABA. Data were collected using self-administered paper-based and online questionnaires, which included demographic characteristics and instruments measuring parental knowledge, involvement, and treatment acceptability.
Results: The majority of participants were mothers (73.5%). A significant proportion of participants’ children exhibited problematic behaviors, with aggression being the most common issue (34.3%). Parental acceptability of ABA was generally high, with 96.4% reporting moderate to high acceptance. The study also found a positive correlation between ABA knowledge, acceptability, and parental involvement in ABA programs.
Conclusion: Enhancing parents’ knowledge of autism and ABA is crucial for effective treatment. To increase parental acceptance and involvement in their child’s ABA, practitioners should implement educational programs that provide parents with a deeper understanding of ABA principles and their practical benefits.
Keywords: applied behavior analysis, autism, child, knowledge, acceptability, involvement
A Letter to the Editor has been published for this article.
Introduction and Background
Autism Spectrum Disorder (ASD) is a group of neurodevelopmental disorders that manifests as constrained, repetitive, and rigid patterns of behavior, interests, or activities that are considered abnormal or excessive for a child’s age and developmental stage.1 In recent years, there has been a dramatic increase in the number of children diagnosed with ASD worldwide.2 According to the WHO, one out of 127 children is affected by ASD.1 The increasing prevalence rates, illness severity,2 and heavy economic burdens3 underscore the need for effective therapeutic options for ASD treatment.4 So there was a need for Evidence-based ASD treatment and a need to be effective and scientifically proven.4 This treatment is based on applied behavior analysis (ABA).5 Involvement, acceptance, and knowledge about ABA treatment are all linked to positive treatment outcomes in ASD.6
Applied behavior analysis (ABA) is a behavior modification intervention based on scientific methods that uses behavioral principles and techniques to identify and modify the environmental factors influencing behaviors.7 The first application of ABA principles with children diagnosed with ASD dates back to the 1960s.8 Since the 1970s, ABA has been consistently used to treat maladaptive behaviors in children with ASD.9 According to Healy and Lydon10 and Viréus-Ortega,8 principles based on ABA treatment should have the following core characteristics:
- First, they should be implemented systematically with an individualized and comprehensive assessment of target skills.
- Second, treatment should be applied as early as the child is diagnosed with ASD, preferably before the age of three.
- Third, treatment should be delivered in a one-to-one ratio of child to therapists. Fourth, treatment should arrange target skills according to a hierarchy of typical development.
- Finally, parents should be involved in ABA-based treatment.
ABA Principles were developed over 60 years ago, based on the early Lovaas model and the subsequent University of California at Los Angeles (UCLA) Young Autism Project. This model established and measured the efficacy of the treatment by empirically testing it.11 The ABA models were comprehensive and intervention-centered.12 Practices, methods, and teaching strategies of ABA aim to reduce problem behaviors and the functional deficits experienced by children with ASD, while also enhancing the development of cognition, language, social skills, and daily living skills.11,13 ABA models are based on behavioral techniques that seek to modify the child’s behavior to the target behavior by manipulating the antecedents and/or consequences of the behavior. Other common techniques include reinforcement, extinction, prompting, video modelling, and the Picture Exchange Communication System (PECS).4
ABA was considered the most effective treatment when administered in an appropriate number of sessions and doses.14,15 Most models are typically implemented for a child with ASD in either the home or school setting for 20 to 40 hours per week over a period ranging from one to four years of the child’s life.11 ABA treatment strategies have shown significant improvement in children with ASD in diverse geographical areas across the globe2, and are socially validated by families who use them at home, with a high level of acceptance and appreciation of the good impact on the entire family.2
Despite the established efficacy and wide availability of information on ABA, significant barriers to involvement persist.4 The use of ABA-based treatment faces many barriers, such as families often lacking access to evidence-based services due to limited knowledge of services, their location, the availability of service providers, and the high cost of treatment.5
Parental involvement in behavioral treatment based on ABA has been identified as a significant predictor of gains in parent knowledge, indicating that such involvement positively affects both conceptual and procedural understanding of the ABA-based intervention.16 In addition, parental knowledge is linked to improvement in skills and performance when parents actively participate in the ABA program.17 Therefore, to enhance the acceptability of ABA services, it is necessary to increase parental knowledge and training.5 Treatment cognitions are also influenced by parental involvement in therapy, particularly the expectation that treatment will be beneficial.18 All parents who reported an improvement in their knowledge of ABA felt confident when caring for a child with ASD and were able to manage the child’s problem behavior and handle day-to-day situations effectively.16 They were satisfied with their involvement in ABA.19 Enhancing parental knowledge of ABA-based programs improved parental involvement, increased treatment acceptability, and strengthened parents’ confidence in caring for their children.
The literature showed that parental knowledge either directly or indirectly improves involvement in ABA-based treatment. These relationships could be visualized using the following conceptual framework (Figure 1). This would help gain an understanding of how these variables might affect each other. All these variables together contribute to enhancing children’s learning, reducing problematic behaviors, and supporting the entire family’s healthy progress. However, there are limited studies assessing these variables that can provide information about Jordanian parents of children with ASD. This may be due to cultural and contextual healthcare delivery in Jordan. Factors such as stigma toward developmental disabilities, the role of the extended family in care decisions, and the newly introduced, less regulated ABA-based treatment in Jordan may affect the parental knowledge, acceptance, and involvement in ABA-based treatment. These variables together made ABA treatment delivery different than models developed in Western culture. Therefore, the findings of this study would shed light on parental knowledge, acceptance, and involvement in ABA-based treatment. This, in turn, would lead to a deeper understanding of the factors that can facilitate the use of ABA-based treatment.
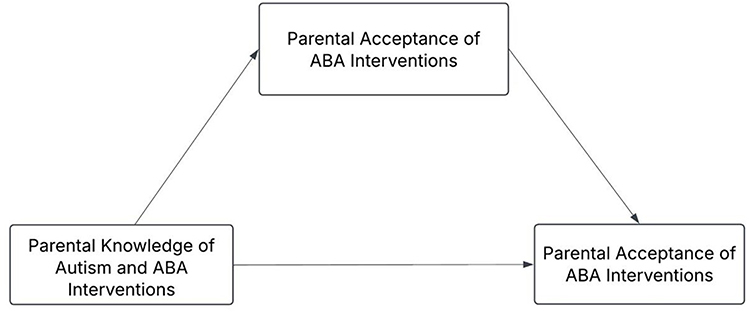 |
Figure 1 An Integrated Conceptual Model of the Relationship between Parental Knowledge, Acceptance, and Involvement in ABA Interventions. |
The purpose of this study is to evaluate parents’ knowledge, acceptability, and involvement in ABA treatment for their autistic children. The specific aims are: (1) to assess differences between participants based on their sociodemographic characteristics; (2) to assess participants’ knowledge, acceptance, and involvement in ABA-based treatment for their children with ASD; and (3) to examine the strength and direction of the relationships between parental knowledge, treatment acceptability, and level of involvement in ABA-based treatment.
Methods
The STROBE guideline for cross-sectional studies was followed in writing this study. A descriptive cross-sectional design was employed. A priori sample size calculation was performed using G*Power 3.1.20 For a biserial point correlation, to detect a moderate effect size (ρ = 0.30) with a two-tailed α of 0.05 and a power of 0.80, a minimum sample of N = 82 was required. A final convenience sample of 157 parents of children with ASD who were exposed to ABA-based treatment in autism-specialized centers in Jordan was used. The authors contacted parents during their visits to the autism centers and checked their eligibility and willingness to participate in the study. Following that, data was collected via self-administered paper-based and online surveys using Google Forms, distributed through the social media platforms of Facebook and WhatsApp. Data collection lasted four months, from the beginning of February 2024 to the end of May 2024. The inclusion criteria include having a child with ASD, receiving treatment from a certified therapist at one of the targeted autism centers, being able to read and write, and the child being more than 18 years old. Parents and caregivers were excluded if their children were diagnosed with another developmental disorder besides ASD, or if the children had been diagnosed with ASD but had not been exposed to ABA. Informed consent was obtained from the participants before data collection. The participants were informed about the purpose of the study, the procedures, and the benefits. The participants were also told that their participation was voluntary, and they could withdraw from the study at any time without any penalty. Anonymity and confidentiality were assured; the data were coded and kept on a password-protected desktop at the principal investigator’s office.
Measures
The standard procedure for translating the study measures from English to Arabic began with two independent, professional faculty members translating the original English items and instructions into Arabic. The translators then met to produce a single consensus Arabic version, resolving any discrepancies in wording or meaning to ensure cultural relevance and clarity for Arabic-speaking parents. A third, independent translator, who was completely blind to the original English version, then performed a back-translation, converting the consensus Arabic version back into English. The research team compared this back-translated English version with the original measures to identify and correct any remaining semantic, idiomatic, or conceptual differences. This iterative process confirmed that the translated Arabic versions maintained the original instruments’ reliability and validity, ensuring that the measured constructs are equivalent across both language versions.
Sociodemographic Questionnaire
This study collected data on participants’ sociodemographic characteristics, including their relationship with the child, parental age, gender, marital status, education level, parents’ occupations, number of children, and whether the child has ASD. In addition, the child’s birth order, presence of problematic behavior, and the type, frequency, and severity of such behavior are considered.
The Treatment Evaluation Inventory-Short Form (TEI-SF)
The Treatment Evaluation Inventory_ Short Form (TEI-SF) was used to assess acceptability. This free tool consists of nine core questions designed to evaluate participants’ acceptance of behavioral treatments. Respondent indicated their answers on a 5-point Likert scale, ranging from “strongly agree”5 to “strongly disagree”,1 with intermediate options (eg, “I believe the treatment will most likely result in permanent improvement”).21–23 Their internal consistency (Cronbach’s α) and construct validity were assessed by comparing the means of different forms and by comparing scores on each short form with full-scale scores. The difference between the two groups was used to determine discriminant validity (estimated effect size 0.7). Scores for all forms showed high internal consistency (Cronbach’s alpha of 0.85) and were highly correlated with total scale scores.24 For the scoring system, the author of the TEI-SF summed the items; Item six is a reversed score. Total scores of TEI–SF are summed, with higher scores indicating greater treatment acceptability.21,22
Parent Involvement Questionnaire
The Parent Involvement Questionnaire was used to assess parental involvement and knowledge. It is divided into five parts, comprising 120 items. In this study, the authors used Part 1 (26 Questions), which is subdivided into four subscales: parent involvement, perception of child progress, belief in intensive behavioral intervention, and Part 5 (22 Questions), which was used to assess parental knowledge about ASD and ABA; the first 2 questions asked parents about their knowledge of ASD and ABA compared to the general population, it was a 5 Likert type scale questions with responses ranging from 1 as low knowledge until 5 for high knowledge. Then the instrument moved to the last 20 items of Yes or No questions. For scoring the knowledge, it was calculated by summing the true items of the ASD knowledge out of 10, and the ABA knowledge out of 10; with 1 for the true choice and 0 for the false choice, and the total score ranged from 0 to 20, with a higher score indicating higher knowledge.
The three domains of the parent involvement subscale are agency involvement, training involvement, and involvement in child programs.25 Agency involvement includes 10 items (Q1-Q10), child program involvement includes 11 items (Q21-Q31), and problem behavior includes 5 items (Q40-Q44). All these items use 5 Likert scale with responses ranging from 1 (lowest) to 5 (highest). For certain questions, there is an additional N/A option for items that do not apply to the child. The score for each subscale is calculated by summing the numerical ratings of the items within that subscale. The internal consistency rating for the parent involvement subscales ranges from 0.72 to 0.95.25 To score the parent involvement tool, sum the scores of each item out of 5 and then calculate the mean.25–27
Data Analysis
The Statistical Package for Social Sciences (SPSS, IBM Corp, Armonk, NY, USA) version 26 for Windows was used to analyze the data. Descriptive statistics were conducted to describe the sample sociodemographic characteristics, as well as knowledge, acceptability, and involvement according to the level of measurement and agreement for describing sample characteristics. To examine differences in knowledge, acceptability, and involvement based on sociodemographic characteristics, the Kruskal–Wallis test was used, as the assumption of homogeneity was violated. To assess the correlation between study variables, the Pearson product-moment correlation coefficient (r) was used. The significance correlation was set at 0.05. Missing values were imputed using variable means (mean imputation) for continuous variables to preserve the complete sample size for analysis. A small percentage of missing data was present in the dataset (< 5% for any variable).
Results
Table 1 presents the sociodemographic distribution of parents. The participating parents were almost exclusively mothers (73.5%) and fathers (25.2%), and the vast majority were currently married (87.5%). Most participants (56.2% of mothers and 43.5% of fathers) held a bachelor’s degree. Regarding employment status, 84.3% of fathers were employed full-time at the time of data collection compared to 32.4% of mothers. Additionally, over 93% of parents did not have another child diagnosed with ASD, and only 36.2% reported that the child diagnosed with ASD was the firstborn. Furthermore, 47.7% of children with ASD exhibited problematic behaviors, with violence being the most frequent behavior (34.3%). It is important to note that some sociodemographic data were missing, and some participants did not complete all survey items; missing items were imputed by means. Of the 275 surveys distributed, 157 were completed by participants. The response rate was 57%.
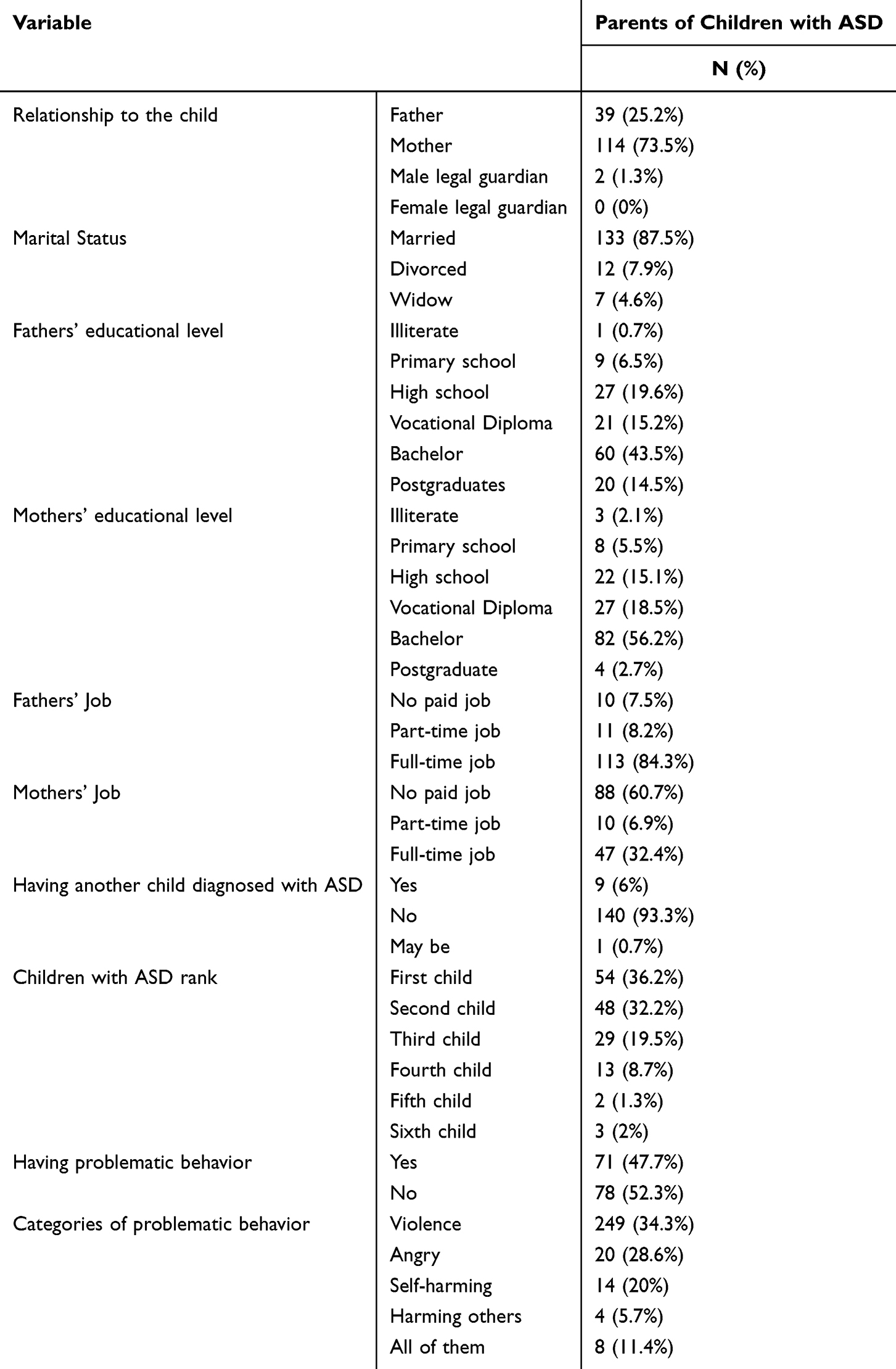 |
Table 1 Description of Sociodemographic Variables for Study Participants |
Table 2 presents the scores of parents of children with ASD across the main study variables. The average age of fathers was 40.5 years (standard deviation [SD] =6.41), while the average age of mothers was 35.1 years (SD =6.55). The average number of children in the household was 3.1 (SD=1.37). The mean acceptability score was 34.00 (SD =4.24), the cut-off for a moderate acceptability score was 27, the median was 34.00, and the lowest response was 11. The highest score was 45 out of 45. Notably, 96.4% of responses were 27 or higher. The mean agency involvement score was 35.21 (SD =6.93). The mean child program involvement score was 56.91 (SD =11.94). The mean ASD knowledge score was 5.20 (SD =4.24), and the average ABA knowledge score was 5.86 (SD =2.48).
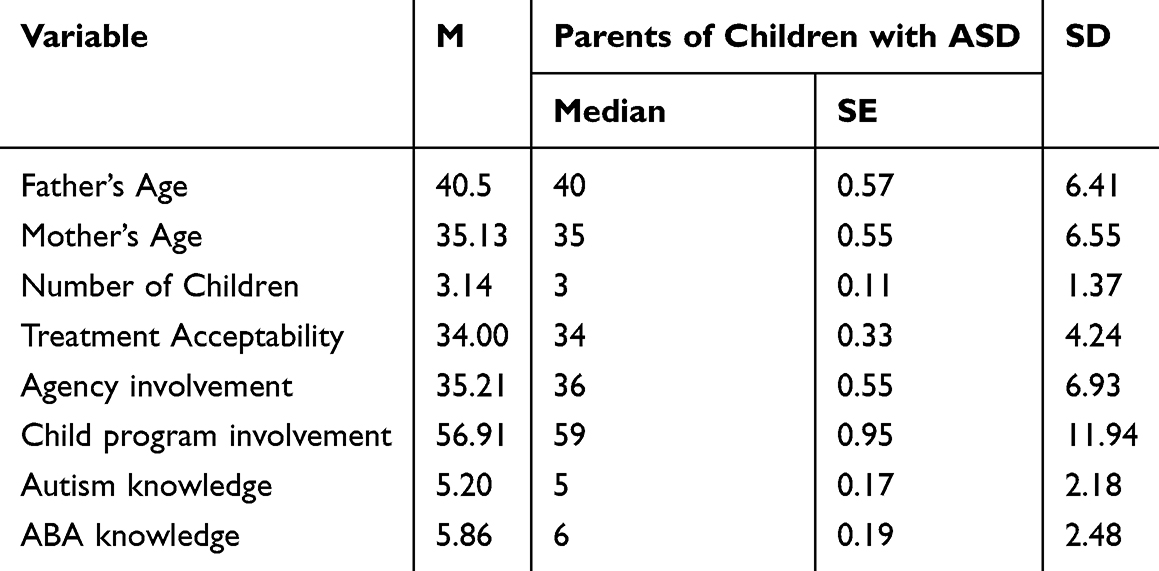 |
Table 2 Descriptive Statistics of Non-Categorical Study Variables |
A Pearson r correlation test was conducted on the non-categorical sociodemographic characteristics of parents of children with ASD (Table 3). No significant correlations were found between the father’s age, mother’s age, number of children in the family, or the rank of the child with ASD and the main study variables. Treatment acceptability showed a significant correlation with agency involvement (r =0.30, p<0.001) and ABA knowledge (r=0.18, p<0.028). No significant correlations were observed between treatment acceptability and child program involvement or autism knowledge. Agency involvement showed significant correlations with treatment acceptability (r=0.30, p<0.001), child program involvement (r=0.48, p<0.001), and ABA knowledge (r=0.31, p<0.001). Child program involvement had significant correlations with agency involvement (r=0.48, p<0.001) and ABA knowledge (r=0.22, p<0.01). Autism knowledge was significantly correlated with ABA knowledge (r=0.49, p<0.001).
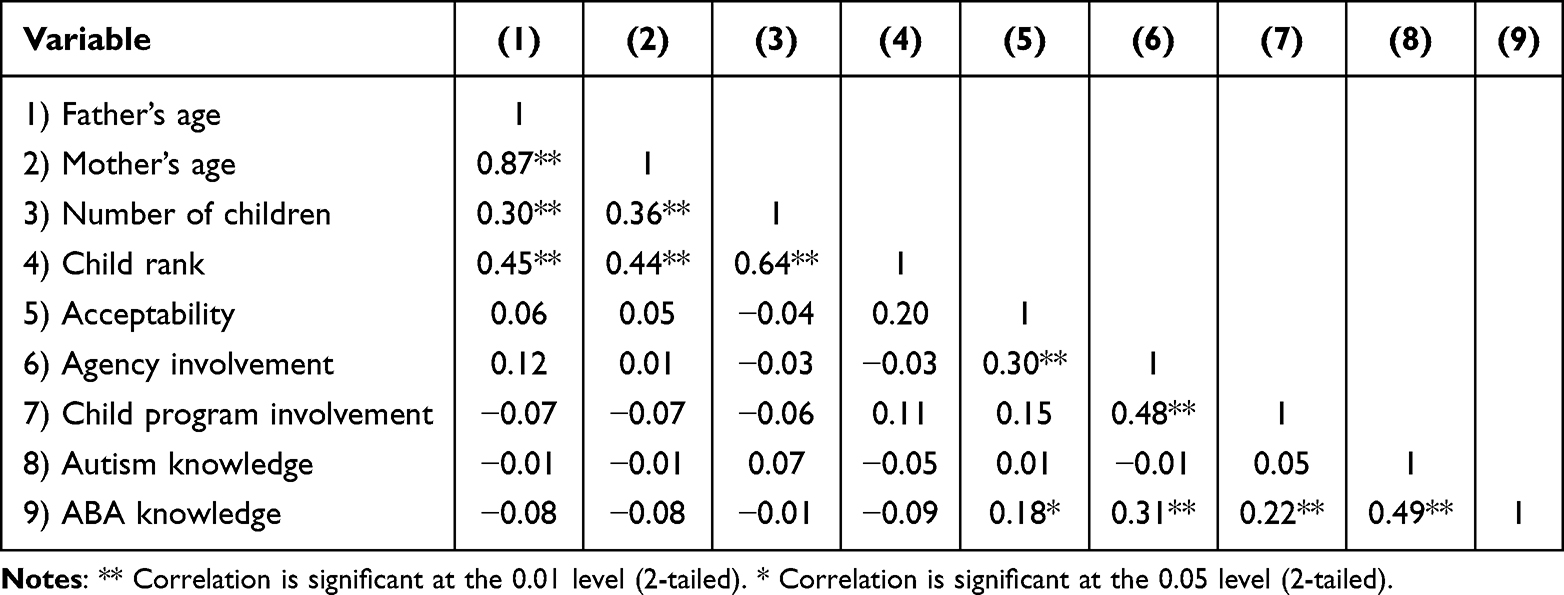 |
Table 3 Correlation Between Study Variables for Parents of Children with ASD |
The normality of the dependent variables (parents’ acceptability, agency involvement, child program involvement, knowledge of autism, and knowledge of ABA) was assessed, with no violations. The distribution of participants across the independent variables (sociodemographic variables) was unequal; thus, the homogeneity assumption was violated. Then, a Kruskal–Wallis test was employed to examine the differences between participants based on their sociodemographic characteristics.
A Kruskal–Wallis test was conducted to examine differences in parental acceptability by the child’s relationship. The results (Table 4) indicated significant differences, H (2, n = 155) = 6.38, p =0.041; the mean ranks were 80.52 for mothers, 74.54 (fathers), and 2.0 for male legal guardians. Post hoc comparisons were performed using Mann–Whitney tests with a Bonferroni-adjusted alpha level of.016 (0.05 ÷ 3). The difference between mothers and male legal guardians was statistically significant (U [N mothers 114, N male legal guardians = 2] = 78.5, z = 2.46, p =0.014). None of the other comparisons were significant after the Bonferroni adjustment (p’s>0.017). No significant differences were found in agency involvement, child program involvement, knowledge of autism, or knowledge of ABA based on the relationship with the child.
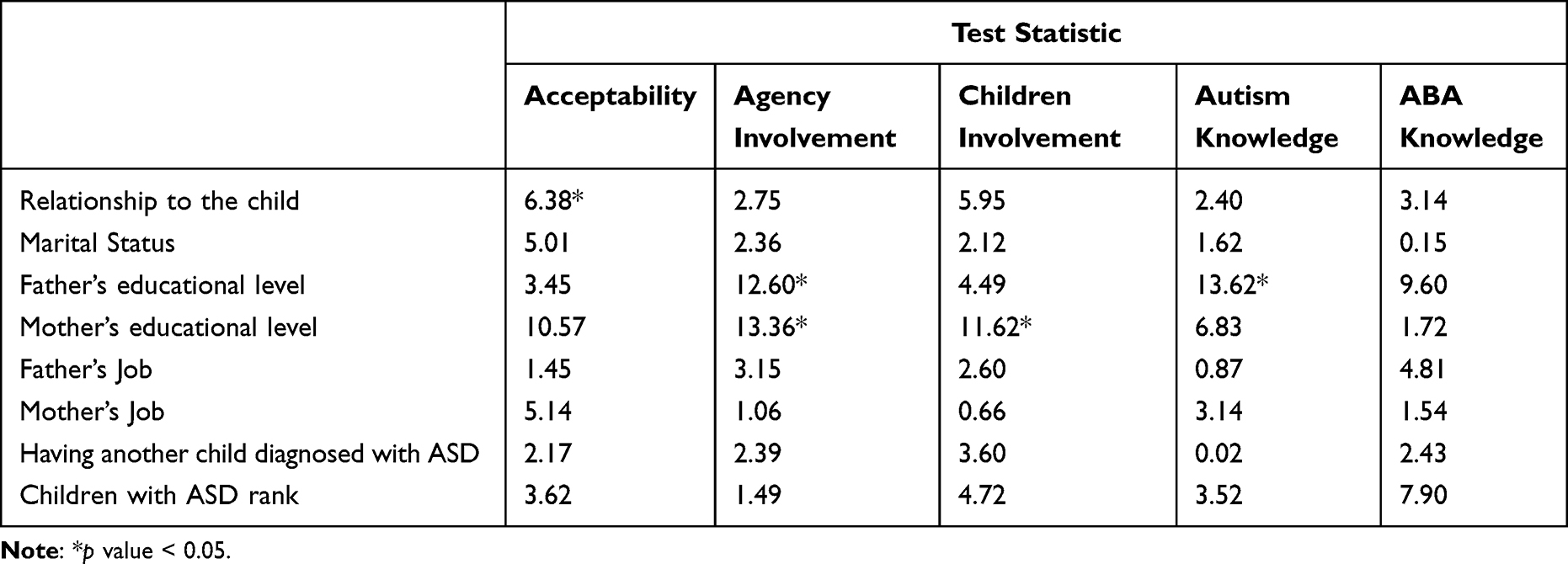 |
Table 4 Comparisons of the Outcome Variables Based on Participants’ Sociodemographic Variables Using Kruskal–Wallis Tests |
Kruskal–Wallis tests were conducted to examine the differences in the dependent variables based on marital status. The results showed no significant differences across these variables. The Kruskal–Wallis tests were significant for involvement H (5, n = 138) = 12.59, p =0.028) across the father’s educational level, with main ranks of 30.50 (illiterate), 43.11 (primary school), 66.70 (high school), 53.26 (vocational diploma), 76.68 (bachelor’s degree), and 82.60 (postgraduate degree). Post hoc comparisons were conducted using Mann–Whitney tests with a Bonferroni-adjusted alpha level of.01 (0.05 ÷ 5). None of the comparisons were significant after the Bonferroni adjustment (p>0.01).
The Kruskal–Wallis test indicated a significant difference in agency involvement across mothers’ educational levels, H (5, n = 146) = 13.36, p =0.020). The mean ranks were 17.33 (illiterate), 62.75 (primary school), 66.20 (high school), 59.80 (vocational diploma), 82.49 (bachelor’s degree), and 85.50 (postgraduate degree). Post hoc comparisons were conducted using Mann–Whitney tests with a Bonferroni-adjusted alpha level of.01 (0.05 ÷ 5). None of the comparisons were significant after the Bonferroni adjustment (p’s>0.01). This suggests an overall association between higher maternal education and greater involvement. However, post-hoc pairwise comparisons did not identify any specific pairwise contrasts between education levels that remained statistically significant. Additionally, significant differences in child program involvement were found across mothers’ educational levels, H (5, n = 146) = 11.62, p =0.040). The mean ranks were 21.50 (illiterate), 65.50 (primary school), 68.82 (high school), 59.96 (vocational diploma), 80.68 (bachelor’s degree), and 98.38 (postgraduate degree). Post hoc comparisons were conducted using Mann–Whitney tests with a Bonferroni-adjusted alpha level of.01 (0.05 ÷ 5). None of the comparisons were significant after the Bonferroni adjustment (p’s>0.01).
Kruskal–Wallis tests revealed no significant differences in the dependent variables based on the father’s occupation, the mother’s occupation, having another child diagnosed with ASD, or the child with ASD rank. An independent t-test was conducted to compare participants’ scores on the dependent variables according to whether a child with ASD exhibited problematic behavior. Parents of children with ASD who displayed problematic behavior had higher mean scores than parents of children with ASD who did not have problematic behavior in acceptability (M with 34.27, M without = 33.86) and agency involvement (M with 36.06, M without = 34.56). In contrast, parents of children with ASD without problematic behavior had higher means in child program involvement (M with 56.21, M without = 57.30), autism knowledge (M with 4.81, M without = 5.74), and ABA knowledge (M with 5.85, M without = 6.03). None of these differences were significant except for the autism knowledge (t (147) = 2.68, p =0.006). In addition, independent t-tests were used to compare participants’ perceptions of their knowledge of autism and ABA based on whether a child with ASD exhibited problematic behavior. No statistical differences were found between the groups.
Discussion
This study is one of the first to identify the relationships between parents’ knowledge, acceptability, and involvement in ABA treatment among Jordanian parents of children with ASD, while also considering sociodemographic characteristics, a scope not previously addressed in Jordan. The study examined whether parents caring for a child with ASD were aware of ASD and ABA, and whether they participated in and accepted the treatment. Additionally, it explored how sociodemographic characteristics can be associated with knowledge, acceptability, and involvement in ABA. The results of the current study showed that knowledge, acceptability, and involvement in ABA treatment were interconnected. This supports the hypothetical relationships among these variables.
Enhanced parental knowledge of autism and ABA is hypothesized to improve their experience in managing these challenges, and may promote positive child behavioral outcomes, and strengthen the relationship between parents and their children with ASD.28 The results of this study indicated a significant correlation between acceptability and ABA knowledge. Training parents and providing them with adequate information and knowledge can help them support their children with ASD and increase their acceptance of ABA treatment. Furthermore, improving parents’ knowledge can enhance their satisfaction and ability to manage their children’s behavior in real-life situations.19,29,30 No significant correlations were found between treatment acceptability and autism knowledge. Parental involvement in ABA treatment can improve their knowledge and teach them how to use and implement ABA strategies. The current findings showed that agency involvement, child program involvement, and autism knowledge had significant correlations with ABA knowledge. These findings are consistent with previous research.31,32
Parental acceptance of ABA-based treatment is associated with high levels of satisfaction, as this treatment helps parents understand their children’s behavior and adjust their parenting approach accordingly.33 In the current study, the majority of the parents reported moderate to high acceptability of ABA treatment. This indicates a high level of acceptance of an ABA-based intervention, which may lead parents to recommend the intervention favorably.19 Moreover, acceptability showed a significant correlation with agency involvement and ABA knowledge. This finding is consistent with a systematic review of nine studies, which reported high levels of satisfaction with ABA-based treatment in most of the reviewed studies.34
Involving a family member in the child’s treatment produced the best outcomes in ABA-based treatment.27 Moreover, such involvement strengthens family relationships by giving parents an effective and manageable role with their children, which renews their enthusiasm and enhances their acceptance of the intervention.35 The findings showed a significant correlation with treatment acceptability, child program involvement, and ABA knowledge. A positive treatment impact was observed over time following the implementation of parent training programs or sessions for families of children with ASD.33,36 Parents become more effectively engaged in play and interaction with their children both at post-treatment and follow-up. In this study, significant correlations between agency involvement and ABA knowledge were found, aligning with prior literature.16,17,31
The results of this study showed that most participants were mothers, indicating that mothers are more frequently involved in the care of children with ASD than fathers. This finding is consistent with a previous study.31 The results showed that mothers demonstrated a higher level of accessibility to ABA treatment than fathers. This indicates that when mothers are the primary caregivers of children with ASD, they are engaged, aware of their children’s needs, and actively involved in monitoring behavioral progression. Moreover, they are more accepting than fathers, which is consistent with a previous study.37
Most fathers held a bachelor’s degree, and most mothers had a bachelor’s degree. A significant difference in agency involvement was found across fathers’ educational level; fathers with postgraduate degrees had higher agency involvement scores than those with bachelor’s degrees. Similarly, a significant difference was observed in agency involvement across mothers’ educational levels; the postgraduate degree mothers have higher agency involvement and child program involvement scores, followed by a bachelor’s degree. This indicates that a higher educational level increases involvement in childcare. The relationship is not driven by large, discrete differences between any two specific education levels. Instead, the pattern may reflect a subtler, gradient-like association where each increment in education corresponds to a small, cumulative increase in involvement.
While overall tests suggested variation by education level, definitive pairwise differences could not be established. The trend, however, aligns with literature suggesting education may facilitate engagement with complex treatment. Parents with higher educational levels show a greater interest in the care of their children with ASD; they were more engaged in behavioral therapy, and they were more likely to be involved in agency and program activities, factors that may affect their children’s developmental outcomes.37,38
Younger mothers have an increased risk of having a child diagnosed with ASD. Research indicates that the risk increases when both parents are older, particularly when there is a relatively large age gap between them.39 The mean age of mothers was 35.1 years, and that of fathers was 40.5 years, which was similar to a previous study.31 In the present study, no significant differences were found between mothers’ and fathers’ ages in ABA knowledge, autism knowledge, acceptability, agency involvement, and child program involvement.
Additionally, the current study found no significant differences between parents with or without another child with ASD in terms of ABA knowledge, autism knowledge, acceptability, agency involvement, and child program involvement. According to Ozonoff et al,40 18.7% of children have a sibling with ASD, an increase from earlier numbers, which ranged between 3% and 10%. The presence of a child diagnosed with ASD increases both physical and emotional demands and alters family norms, including social life, emotional life, and economic status.41
On the other hand, having another child diagnosed with ASD and being aware of ASD, problematic behaviors, and delayed developmental milestones may assist in the detection and diagnosis of siblings with ASD.39 Increased parental attentiveness and familiarity with ASD can lead to earlier screening, which may improve prognosis and reduce negative consequences for the children.
Most Participants reported that their children with ASD exhibited problematic behavior; violence was the most frequent behavior. The findings indicated that acceptability and agency involvement had higher mean scores in treatment for parents of children with ASD who exhibited problematic behavior. This may be due to the effectiveness of ABA treatment and its role in reducing problematic behaviors, making it more acceptable.42 These results are consistent with a previous study.42 In contrast, parents of children with ASD without problematic behavior reported higher means for child program involvement, autism knowledge, and ABA knowledge. This may be attributed to having fewer problematic issues, allowing them to engage more actively in therapeutic involvement.
The intriguing finding that higher acceptability was associated with lower autism knowledge warrants further investigation. It may not reflect a deficient knowledge but rather methodological and parental factors. First, the autism knowledge measure may be biased toward academic knowledge, failing to capture practical, experiential understanding gained by parents. Second, parents of children exhibiting high levels of challenging behaviors may be in a “crisis mode”, wherein immediate behavioral management necessarily takes precedence over broader learning. This finding challenges simple assumptions about the relationship between knowledge and acceptance and suggests that support for families must be tailored to their immediate needs.
The findings of the current study indicated that parents of children with ASD had insufficient knowledge about autism and ABA. The moderate scores suggest that the information gained after diagnosis is often either too technical, poorly delivered, or misaligned with the practical, daily needs of families. When parents are faced with new diagnoses and challenging behaviors, the current methods of psychoeducation are failing to convey essential knowledge effectively. This gap has direct consequences for advocacy, access to services, and informed decision-making. These results highlight the need for better training of professional teams and private care centers on how to provide families with appropriate information and skills to improve parents’ knowledge.
In addition, agency involvement rates were insufficient. Some families did not actively participate in the child’s programs at the centers. In many cases, they simply dropped off their children and returned later, or the private center was responsible for transporting the children. Teaching parents about the effectiveness and importance of aligning their role with programs may improve outcomes for their children. Furthermore, centers should provide their therapists with ongoing training programs to strengthen their skills and ensure high-quality educational and therapeutic services for both children and their families.
The findings of the study were limited by using a convenience sampling procedure, which may affect the generalizability of the results. The use of a convenience sample of parents from ABA-treatment centers is a constraint. It likely captures the most motivated and resourceful subgroup of parents, limiting the generalizability of the very high acceptability rates to the broader population of parents of children with ASD in Jordan (including those who have not accepted or discontinued ABA). This must be thoroughly acknowledged. Although the results were consistent with previous studies regarding the measured variables and their intercorrelations, particular attention should be given to the cultural and social factors unique to the population from which this sample was drawn. The Jordanian parents who participated shared a cultural norm characterized by proximity to extended families, larger social networks, and higher support systems. However, these factors can sometimes contribute to the challenges of raising a child with ASD.
In other words, social support networks may have drawbacks, such as blaming the mother for the child’s diagnosis, stigmatizing the child and family, or the child being bullied by other children within their extended family. Additionally, some parents refused to provide information on certain study variables. In addition, causality cannot be inferred from the results of the current study because the data are cross-sectional. This study was powered to detect main effects in the overall sample but was not specifically powered for subgroup analyses (sociodemographic characteristics). The findings from these subgroup analyses should therefore be interpreted as exploratory and hypothesis-generating, requiring validation in larger sample studies. These issues should be further investigated in future research. Moreover, the response rate was low, which may be due to parental stigma and limited time to complete the survey.
Future research should focus on family income, mothers’ employment status, and the age at which ABA-based treatment is initiated, in relation to parents’ knowledge, acceptability, and involvement in this treatment. Additionally, future studies should investigate the duration and intensity of these treatments, specifically how many hours and for how long parents should be exposed to enhance their knowledge, acceptability, and involvement, as well as to explore correlations with developmental gains in children with ASD. These studies will contribute to improving parents’ knowledge, acceptance, and active involvement.
Conclusions
The literature demonstrates the impact of ABA-based treatment on children with ASD and their families. Enhancing the knowledge of parents and communities about autism and ABA should be a key aim for the government and all community-based centers or agencies. Treatment acceptability in the current study correlated with agency involvement and ABA knowledge. To increase parental acceptance of an intervention, parents should be provided with sufficient information and evidence of its effectiveness. Parental involvement in ABA may enhance outcomes for both children and parents. Finally, we recommend that practitioners use plain-language guides, educators implement structured parent workshops, and policymakers fund accessible psychoeducational programs to enhance parental knowledge and improve the children’s outcomes.
Abbreviations
ABA, Applied Behavior Analysis; ASD, Autism Spectrum Disorder; UCLA, University of California at Los Angeles; PECS, Picture Exchange Communication System; TEI-SF, Treatment Evaluation Inventory_ Short Form; SPSS, Statistical Package for Social Sciences; IRB, Institutional Review Board.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board (IRB) of Jordan University of Science and Technology (Approval No: 754/2023). All methods were performed by relevant guidelines and regulations, including the Declaration of Helsinki and the ethical principles outlined by the journal’s editorial policies.
Acknowledgments
The Researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (APC-QU-2026).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Jordan University of Science and Technology/ Deanship of Research [Research Grant No: 20230754]. The funding does not cover the article processing charge (APC).
Disclosure
The authors declare no conflict of interest.
References
1. WHO. Autism: World Health Organization; 2025 [updated September 17, 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/autism-spectrum-disorders.
2. Makrygianni MK, Gena A, Katoudi S, Galanis P. The effectiveness of applied behavior analytic interventions for children with Autism Spectrum Disorder: a meta-analytic study. Res Autism Spectrum Disord. 2018;51:18–12. doi:10.1016/j.rasd.2018.03.006
3. Qiu S, Lu Y, Li Y, et al. Prevalence of autism spectrum disorder in Asia: a systematic review and meta-analysis. Psychiatry Res. 2020;284:112679. doi:10.1016/j.psychres.2019.112679
4. Gitimoghaddam M, Chichkine N, McArthur L, Sangha SS, Symington V. Applied behavior analysis in children and youth with autism spectrum disorders: a scoping review. Perspect Behav Sci. 2022;45(3):521–557. doi:10.1007/s40614-022-00338-x
5. Antill K. Family-centered applied behavior analysis for children with autism spectrum disorder. Intervention School Clinic. 2020;55(3):185–191. doi:10.1177/1053451219842240
6. Choi KYK, Kovshoff H. Do maternal attributions play a role in the acceptability of behavioural interventions for problem behaviour in children with autism spectrum disorders? Res Autism Spectrum Disord. 2013;7(8):984–996. doi:10.1016/j.rasd.2013.04.010
7. Yu Q, Li E, Li L, Liang W. Efficacy of interventions based on applied behavior analysis for autism spectrum disorder: a meta-analysis. Psychiatry Invest. 2020;17(5):432. doi:10.30773/pi.2019.0229
8. Virués-Ortega J. Applied behavior analytic intervention for autism in early childhood: meta-analysis, meta-regression and dose–response meta-analysis of multiple outcomes. Clinic Psychol Rev. 2010;30(4):387–399. doi:10.1016/j.cpr.2010.01.008
9. Smith T, O ES. Ivar Lovaas: pioneer of applied behavior analysis and intervention for children with autism. J Autism Dev Disorders. 2011;41(3):375–378. doi:10.1007/s10803-010-1162-0
10. Healy O, Lydon S. Early intensive behavioural intervention in autism spectrum disorders. In: Recent Advances in Autism Spectrum Disorders-Volume I. IntechOpen; 2013.
11. Reichow B, Wolery M. Comprehensive synthesis of early intensive behavioral interventions for young children with autism based on the UCLA young autism project model. J Autism Dev Disorders. 2009;39(1):23–41. doi:10.1007/s10803-008-0596-0
12. Eckes T, Buhlmann U, Holling H-D, Möllmann A. Comprehensive ABA-based interventions in the treatment of children with autism spectrum disorder–a meta-analysis. BMC Psychiatry. 2023;23(1):133. doi:10.1186/s12888-022-04412-1
13. Fernandes FDM, Amato C. Análise de Comportamento Aplicada e Distúrbios do Espectro do Autismo: revisão de literatura. CoDAS; 2013: SciELO Brasil.
14. Choi KR, Bhakta B, Knight EA, et al. Patient outcomes after applied behavior analysis for autism Spectrum disorder. J Dev Behav Pediatr. 2022;43(1):9–16. doi:10.1097/DBP.0000000000000995
15. Howard JS, Stanislaw H, Green G, Sparkman CR, Cohen HG. Comparison of behavior analytic and eclectic early interventions for young children with autism after three years. Res Dev Disab. 2014;35(12):3326–3344. doi:10.1016/j.ridd.2014.08.021
16. Ingersoll B, Berger NI. Parent engagement with a telehealth-based parent-mediated intervention program for children with autism spectrum disorders: predictors of program use and parent outcomes. J Med Internet Res. 2015;17(10):e4913.
17. Estes A, Vismara L, Mercado C, et al. The impact of parent-delivered intervention on parents of very young children with autism. J Autism Dev Disorders. 2014;44(2):353–365. doi:10.1007/s10803-013-1874-z
18. Rovane AK, Hock RM, January S-A-A. Adherence to behavioral treatments and parent stress in families of children with ASD. Res Autism Spectrum Disord. 2020;77:101609. doi:10.1016/j.rasd.2020.101609
19. Batton B, Kaplan R, Ellis K, Schmidt C, Nudelman E. Telehealth training in principles of applied behavior analysis for caregivers of young children with autism spectrum disorders during the COVID-19 pandemic. Educ Treatment Children. 2022;45(3):299–303. doi:10.1007/s43494-022-00081-7
20. Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Meth. 2007;39(2):175–191. doi:10.3758/BF03193146
21. Jones GR, George JM. The experience and evolution of trust: implications for cooperation and teamwork. Acad Manage Rev. 1998;23(3):531–546. doi:10.2307/259293
22. Kelley ML, Heffer RW, Gresham FM, Elliott SN. Development of a modified treatment evaluation inventory. J Psychopathol Behav Assess. 1989;11(3):235–247. doi:10.1007/BF00960495
23. Finn CA, Sladeczek IE. Assessing the social validity of behavioral interventions: a review of treatment acceptability measures. School Psychol Quat. 2001;16(2):176. doi:10.1521/scpq.16.2.176.18703
24. Newton J, Sturmey P. Development of a short form of the treatment evaluation inventory for acceptability of psychological interventions. Psychol Rep. 2004;94(2):475–481. doi:10.2466/pr0.94.2.475-481
25. Solish A, Perry A, Minnes P. Participation of children with and without disabilities in social, recreational and leisure activities. J Appl Res Intellect Disabil. 2010;23(3):226–236. doi:10.1111/j.1468-3148.2009.00525.x
26. Solish A, Perry A. Parents’ involvement in their children’s behavioral intervention programs: parent and therapist perspectives. Res Autism Spectrum Disord. 2008;2(4):728–738. doi:10.1016/j.rasd.2008.03.001
27. Solish A, Perry A, Shine R. The Parent Involvement Questionnaire: measuring parents’ involvement in behavioural intervention for their children with an autism spectrum disorder. J Dev Disab. 2015;21(1):34.
28. Ilg J, Jebrane A, Paquet A, et al. Evaluation of a French parent-training program in young children with autism spectrum disorder. Psychologie française. 2018;63(2):181–199. doi:10.1016/j.psfr.2016.12.004
29. Abouzeid N, Rivard M, Mello C, Mestari Z, Boulé M, Guay C. Parent coaching intervention program based on the early start Denver model for children with autism spectrum disorder: feasibility and acceptability study. Res Dev Disab. 2020;105:103747. doi:10.1016/j.ridd.2020.103747
30. Abdelwahab Khedr M, Alqarawi N, Mohammed Hussein R. Uncovering the relationship between bullying, social communication challenges, and the emergence of mental health problems among saudi children with autism spectrum disorder. Children. 2025;12(10):1387. doi:10.3390/children12101387
31. Fisher WW, Luczynski KC, Blowers AP, et al. A randomized clinical trial of a virtual‐training program for teaching applied‐behavior‐analysis skills to parents of children with autism spectrum disorder. J Appl Behav Anal. 2020;53(4):1856–1875. doi:10.1002/jaba.778
32. Steiner AM, Gengoux GW, Klin A, Chawarska K. Pivotal response treatment for infants at-risk for autism spectrum disorders: a pilot study. J Autism Dev Disorders. 2013;43(1):91–102. doi:10.1007/s10803-012-1542-8
33. Green J, Pickles A, Pasco G, et al. Randomised trial of a parent‐mediated intervention for infants at high risk for autism: longitudinal outcomes to age 3 years. J Child Psychol Psychiatry. 2017;58(12):1330–1340. doi:10.1111/jcpp.12728
34. Bradshaw J, Steiner AM, Gengoux G, Koegel LK. Feasibility and effectiveness of very early intervention for infants at-risk for autism spectrum disorder: a systematic review. J Autism Dev Disorders. 2015;45(3):778–794. doi:10.1007/s10803-014-2235-2
35. Jayousi S, Martinelli A, Lucattini P, Mucchi L. ICT framework for supporting applied behavior analysis in the social inclusion of children with neurodevelopmental disorders. Sensors. 2023;23(15):6914. doi:10.3390/s23156914
36. Kasari C, Gulsrud A, Paparella T, Hellemann G, Berry K. Randomized comparative efficacy study of parent-mediated interventions for toddlers with autism. J Consulting Clin Psychol. 2015;83(3):554. doi:10.1037/a0039080
37. Burrell TL, Borrego JJ. Parents’ involvement in ASD treatment: what is their role? Cognit Behav Pract. 2012;19(3):423–432. doi:10.1016/j.cbpra.2011.04.003
38. Eid A, Jobeir A, Alhaqbani O, AlSaud A, Fryling MJ. Assessment of parental acceptability and preference for behavioral interventions for childhood problem behavior in Saudi Arabia. Child Fam Behav Ther. 2019;41(4):237–241. doi:10.1080/07317107.2019.1659548
39. Sandin S, Lichtenstein P, Kuja-Halkola R, Larsson H, Hultman CM, Reichenberg A. The familial risk of autism. JAMA. 2014;311(17):1770–1777. doi:10.1001/jama.2014.4144
40. Ozonoff S, Young GS, Carter A, et al. Recurrence risk for autism spectrum disorders: a baby siblings research consortium study. Pediatrics. 2011;128(3):e488–e95. doi:10.1542/peds.2010-2825
41. MCMd A, Pondé MP. Parenting a child with autism. J Brasileiro Psiquiatria. 2019;68:42–47. doi:10.1590/0047-2085000000223
42. Grindle CF, Kovshoff H, Hastings RP, Remington B. Parents’ experiences of home-based applied behavior analysis programs for young children with autism. J Autism Dev Disorders. 2009;39(1):42–56. doi:10.1007/s10803-008-0597-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Jordanian Population’s Knowledge, Attitudes, and Willingness to Help People with Autism: A Cross-Sectional Study
Abuhamdah SMA, Naser AY, Al Awawdeh S
Journal of Multidisciplinary Healthcare 2023, 16:1203-1213
Published Date: 1 May 2023
Smartphone App-Based Psychoeducation for Caregivers of People with Dementia in Vietnam: A Pilot Randomized Controlled Trial
Nguyen TTT, Vu LDT, Truong KT, Nguyen TC, Thai TT, Schofield P, Nguyen TA, Than THN, Nguyen HT
Clinical Interventions in Aging 2025, 20:1647-1660
Published Date: 20 September 2025