Back to Journals » Patient Preference and Adherence » Volume 17
Parental Hesitancy on COVID-19 Vaccination for Children Under Five Years in Thailand: Role of Attitudes and Vaccine Literacy
Authors Maneesriwongul W ![]() , Butsing N, Deesamer S
, Butsing N, Deesamer S
Received 21 December 2022
Accepted for publication 9 February 2023
Published 10 March 2023 Volume 2023:17 Pages 615—628
DOI https://doi.org/10.2147/PPA.S399414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Wantana Maneesriwongul, Nipaporn Butsing, Suhong Deesamer
Ramathibodi School of Nursing, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Nipaporn Butsing, Ramathibodi School of Nursing, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Thung Phaya Thai, Ratchathewi, Bangkok, 10400, Thailand, Email [email protected]
Introduction: Global vaccination efforts to control the COVID-19 pandemic may be impeded by vaccine hesitancy. Attitudes and vaccine literacy are important factors that reduce vaccine hesitancy. The role of attitudes and vaccine literacy of parents on COVID-19 vaccine intention for their children under five years was unknown.
Objective: This study aimed to assess parents’ characteristics, vaccine literacy, attitudes toward the COVID-19 vaccine, and vaccine intention/hesitancy and to determine factors influencing parents’ vaccine intention for their children under five years of age.
Methods: A cross-sectional study was conducted using an online self-administered questionnaire before the authorization of the COVID-19 vaccine for very young children in Thailand. The sample consisted of 455 parents with children under five years old. The online questionnaire included parents’ sociodemographic data, vaccine literacy, attitudes toward COVID-19 vaccine, and vaccine intention to get their children vaccinated.
Results: About 98% of the parents received their COVID-19 vaccination, whereas only 45.1% reported they would have their children under five years old get vaccinated. About 54.9% were either not sure or refused their child’s COVID-19 vaccination. A multiple logistic regression model identified factors that increased the odds of parents’ vaccine intention: parents aged > 35 years, attitudes on safety and efficacy of COVID-19 vaccine for children, advice about the COVID-19 vaccines from healthcare personnel, and the belief that COVID-19 vaccine is helpful for their children. Attitudes that COVID-19 vaccination in children could be fatal decreased parents’ vaccine intention. Need for more information about the COVID-19 vaccine for children and concern about the vaccine’s side effects were the most frequent reasons for vaccine hesitancy and refusal.
Conclusion: Parents should be provided with accurate information from healthcare personnel and media sources about the safety and effectiveness of the COVID-19 vaccine for young children under five years of age to overcome their hesitancy.
Keywords: COVID-19, vaccine hesitancy, children, parents, attitudes, vaccine literacy
Introduction
The COVID-19 pandemic continues to pose severe constraints on healthcare systems and socioeconomic development worldwide.1,2 Global vaccination is recognized as a key strategy to mitigate the effects of the pandemic. Several COVID-19 vaccines have been rapidly developed3,4 and have been shown to reduce severe illness, hospitalization, and mortality rates.5 Priority for receiving the vaccine has been frontline healthcare workers and high-risk older adults, followed by all adults, adolescents, and children 5–11 years old.2 However, younger children under five years had formerly been omitted until late June 2022, when Pfizer-BioNTech and Moderna COVID-19 vaccines were authorized for children between six months and five years of age.6
Children are generally less likely than adults to be symptomatic from COVID-19 and less likely to develop a severe disease that requires hospitalization.7 However, a high risk of severe COVID-19 has been reported among infants and children under five years of age.8 During the Omicron-predominant period, the cumulative hospitalization rate among unvaccinated children was more than twice as high as among vaccinated children (19.1 vs 9.2 per 100,000 population).9 Children living with an underlying disease are also more likely to need hospital admission due to COVID-19 than those who are healthy.10
In Thailand, the proportion of children infected with COVID-19 from April to November 2021 was approximately 20% of all COVID-19 cases.11 Amid the fifth wave of Omicron in early 2022, the infection rate in Thailand increased among children 0–9 years old and 10–19 years old. During the first nine months of 2022, the infection rate and death rate of COVID-19 among unvaccinated children under five years old were 1.5 times and 3 times higher, respectively, than older children who were vaccinated. During the same time period, there were 69 deaths and 443 intubated cases among children under 5 years in Thailand.12
The multi-generational high-density family living in Thailand increases the susceptibility of older adults and other vulnerable family members to getting COVID-19. The age groups and proportions of child infection from exposure to COVID-19 from family/household members were recently reported to be the following: 0–4 years (37.16%), 5–9 years (30.18%), 10–14 years (20.01%), and 15–19 years (12.99%), indicating that more than one-third of the household exposures in Thailand were in the youngest age group.13 In addition to household exposures, clusters of COVID-19 cases in Thailand have also been reported in preschools and childcare facilities.14 This is significant because approximately 800,000 children between 3 and 5 years of age attend public-funded childcare facilities in Thailand.15 Thus, young children are at risk of acquiring COVID-19 from others and a risk to others.
Although vaccines may reduce the risk of death and severity from COVID-19 infection, the newly developed COVID-19 vaccines for very young children have raised questions about vaccine safety and long-term health effects. The concern has led to uncertainty among parents about whether they should accept the COVID-19 vaccine for their children. Vaccine hesitancy has been reported as a significant factor in lower vaccination rates and a substantial barrier to accomplishing the target population’s coverage.5 Vaccine hesitancy remains a major public health challenge in controlling the COVID-19 pandemic.16
Vaccine literacy and positive attitudes are important factors that affect vaccination intention and reduce vaccine hesitancy.17,18 Negative attitudes about vaccines have been significantly linked to vaccine hesitancy.17,19,20 Inadequate vaccine literacy is significantly associated not only with personal attitudes toward COVID-19 vaccination18,21 but also with COVID-19 vaccine intention/hesitancy.17,22
Therefore, this study aimed to assess parents’ background characteristics, vaccine literacy, attitude towards the COVID-19 vaccine, and vaccine intention/hesitancy and to determine factors influencing parents’ vaccine intention for their children under five years of age.
Materials and Methods
Study Design
This study is part of a larger project titled, “Trends analysis of child COVID-19 vaccination, parents’ COVID-19 vaccine literacy, attitudes toward COVID-19 vaccine, and intention to vaccinate their children against COVID-19 and factors predicting intention to vaccinate their children against COVID-19”. The data were collected online using a cross-sectional study design from January 13 to May 25, 2022, before the CDC’s recommendation in June 2022 of the COVID-19 vaccine for children between six months and five years of age. The aims were to assess parents’ intention to have their children under five years of age vaccinated against COVID-19 and examine its influencing factors.
Study Sample
A sample of 455 parents in Thailand was recruited online. The inclusion criteria were 1) having one or more children under five years of age, 2) being able to read and understand Thai, and 3) agreeing to participate in the study. Using a 30% response probability based on a previous study to calculate a sample size,23 a significance level of 0.05, and statistical power of 0.80, the minimum sample size required for this study was 425. Participants were voluntarily recruited using convenience sampling.
Instruments
The online survey form collected participants’ sociodemographic characteristics, COVID-19 vaccination status, COVID-19 vaccine literacy, attitudes toward COVID-19 vaccination, and parental vaccination intention for their child(ren). The sociodemographic characteristics were the participants’ age, sex, education, region of residence, income sufficiency, occupation, the child’s age, and the presence of an underlying disease. To measure the participants’ vaccination status, they were asked about their own COVID-19 vaccinations, “Have you already received the COVID-19 vaccination?” (1 = Yes, 0 = No).
To measure COVID-19 vaccine literacy (VL), the participants responded to the Thai COVID-19 VL scale,24 which was translated from the original scale.22 It is composed of two subscales: functional VL (4 items) and interactive/critical VL (8 items). The functional VL subscale measures literacy skills about language capabilities, such as “When reading or listening to information about COVID-19 vaccines, did you find the texts were difficult to understand?” The interactive/critical VL subscale assesses communication, problem-solving, and decision-making skills, such as “When looking for information about COVID-19 vaccines, have you considered the credibility of the sources?” The item response options are 1 = Never, 2= Rarely, 3 = Sometimes, and 4 = Often. A higher average score in each subscale means a higher vaccine literacy. Each subscale had an adequate Cronbach’s alpha of 0.899 and 0.921, respectively, for internal consistency.
The participants’ attitudes toward the COVID-19 vaccine were measured by a 10-item scale developed by the research team with five positive and five negative items. Content validity was assessed by a pediatrician and two nurse educators in infectious disease and pediatric nursing. Examples of positive questions are “I think the COVID-19 vaccine is helpful for children”, “COVID-19 vaccine is safe and effective for children”, and “Advice about the COVID-19 vaccines for children from medical personnel is reliable.” Examples of negative questions are “COVID-19 vaccination can cause adverse effects in children”, “COVID-19 vaccination in children can be fatal”, and “There are other ways to prevent children from COVID-19 better than vaccination”. The Cronbach’s alphas for the positive and negative subscales and overall alpha were 0.91, 0.75, and 0.81, respectively. The Likert responses are on a rating scale ranging from 1 to 7. Items were recoded into two categories: Disagree (scores ≤ 4) and Agree (scores 5 to 7).
To measure the participants’ intention for their children to get vaccinated, participants were asked, “Will you have your children get vaccinated against COVID-19?” The three response options were 0 = Definitely not, 1 = Maybe/not sure, and 2 = Definitely yes.
Ethical Consideration
Ethical approval to conduct the study was obtained from the Committee on Human Rights Related to Research Involving Human Subjects, Faculty of Medicine Ramathibodi Hospital, Mahidol University (COA.MURA2021/1005) and (COA.MURA2022/614) and conducted in accordance with the guidelines of the Declaration of Helsinki.
Data Collection
Data were collected using an online questionnaire. Recruiting messages containing a URL link and a quick response code were openly circulated via social media platforms (LINE application and Facebook) of individuals’ contact network, community/social groups of coworkers, health workers, village health volunteers, teachers, child caregivers, and parents to reach out to parents in all regions of Thailand. Participation in this study was voluntary and anonymous. There was no monetary incentive for participating. Potential participants provided online consent by clicking “accept” on the online consent form before responding to the questionnaire. Based on the response data, the calculated acceptance rate was 91.2%.
Data Analysis
Frequencies, percentages, means, and standard deviations were used to analyze the characteristics of the participants. The R statistical software (version 3.6.3) was used to analyze data.25 Univariate and multiple logistic regression models were performed to identify the factors associated with parents’ intention to have their children vaccinated against COVID-19.26 Variables having a univariate test with p <0.25 were selected as candidate variables for the regression model.26 Backward multiple logistic regression was used to fit the model. The alpha level was set at 0.05 for statistical significance.
Results
Sociodemographic Characteristics, Attitudes, and Vaccine Literacy of the Participants
A total of 455 parents with children younger than five years of age completed the online survey (Table 1). The participants were from all geographical areas of Thailand, although over half came from the Central and Southern regions. The median age was somewhat higher than the mean age. Most of the participants were < 35 years, were female, had an adequate income, and had earned a bachelor’s degree or higher. About one-third of them were healthcare personnel. Almost all the participants had received the COVID-19 vaccination. The median age of the children was slightly lower than the mean age. A few of the children had an underlying disease, such as asthma, allergy, or G6PD deficiency. Although most of the participants reported they had been vaccinated against COVID-19, less than half responded that they definitely would have their children get vaccinated against COVID-19. The majority were either not sure or refused to consider vaccination for their children.
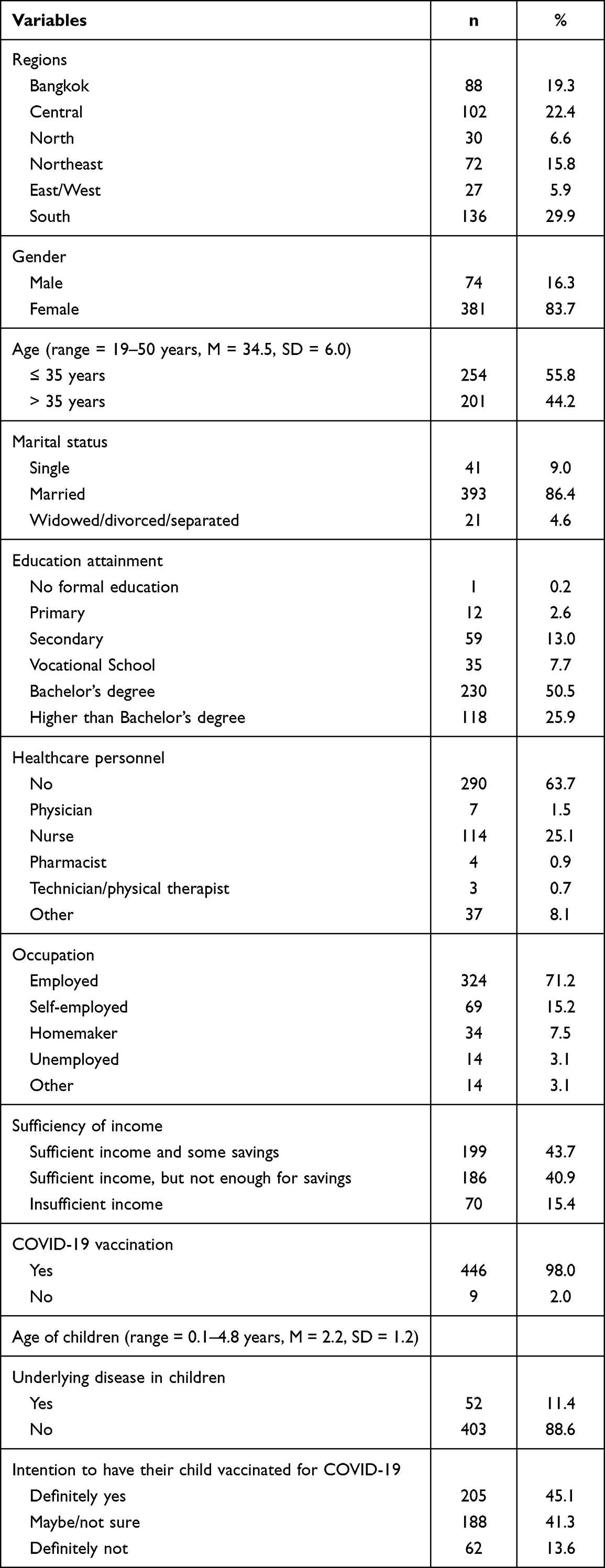 |
Table 1 Sociodemographic Characteristics and Vaccine Responses of the Participants (n = 455) |
Overall, most participants held positive attitudes about the COVID-19 vaccines because the vaccines could reduce the severity of COVID-19 in children (Table 2). More than three-fourths thought that advice about the COVID-19 vaccines for children from medical personnel was reliable, and that the COVID-19 vaccine would be helpful for children. The one negative attitude that most participants held was the belief that children could produce a natural immunity against COVID-19 without receiving the vaccine. Some uncertainty existed among the participants in that more than 40% thought there were better ways to prevent children from COVID-19 than getting vaccinated or believed that the COVID-19 vaccine could cause adverse effects in children, possibly even fatality.
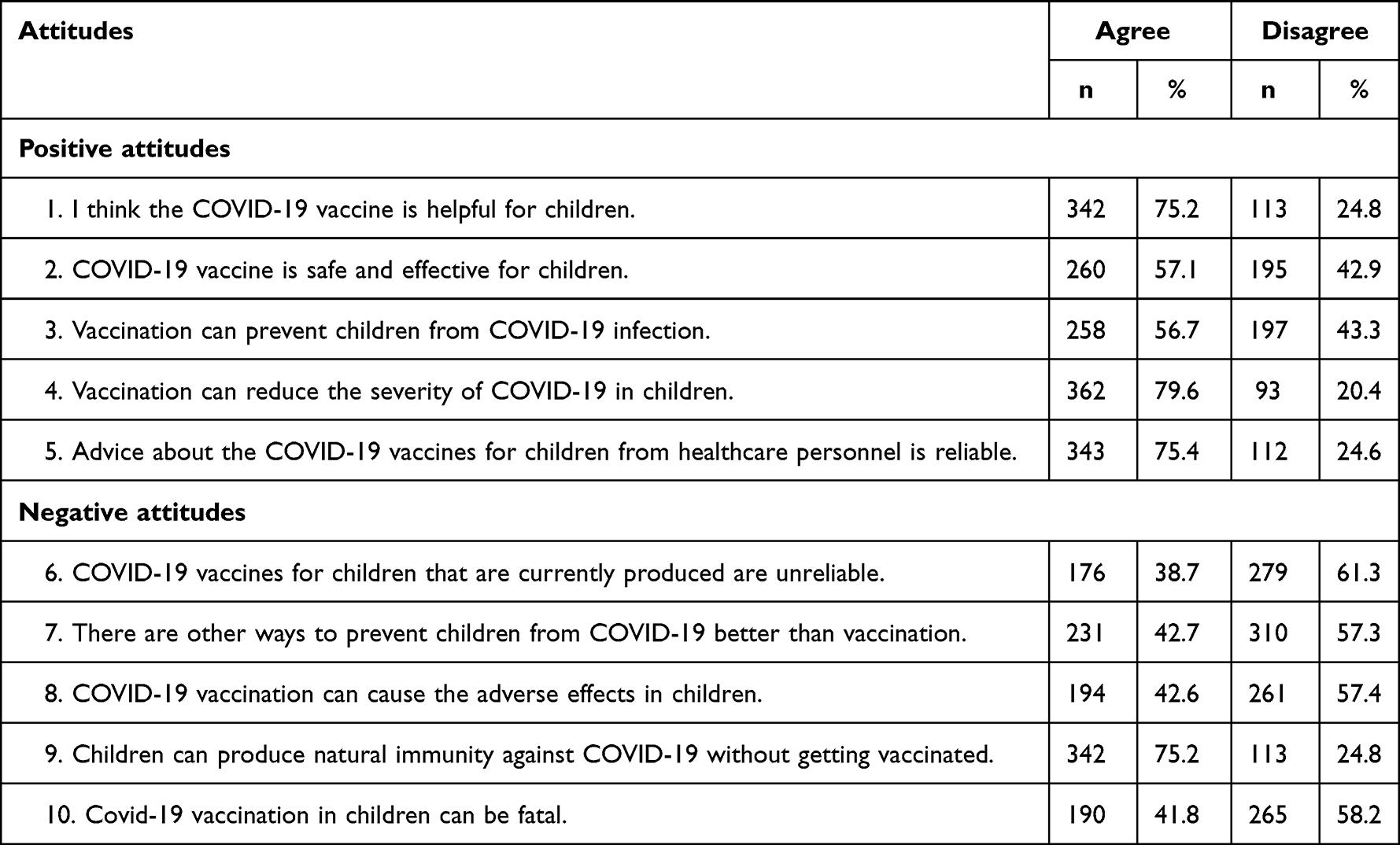 |
Table 2 Participants’ Positive and Negative Attitudes Toward the COVID-19 Vaccine (n = 455) |
The majority of participants’ informative literacy skills about COVID-19 vaccines had scores midrange in that they “rarely” or “sometimes” had problems in reading and understanding information about the COVID-19 vaccine (Table 3). Scores for their interactive/critical literacy skills were somewhat higher in that approximately 80% reported “sometimes” and “often” on items about checking whether the information was correct, consulting more than one source of information, and considering the credibility of the sources. The overall mean score for interactive/critical literacy skills was higher than the mean for information literacy skills.
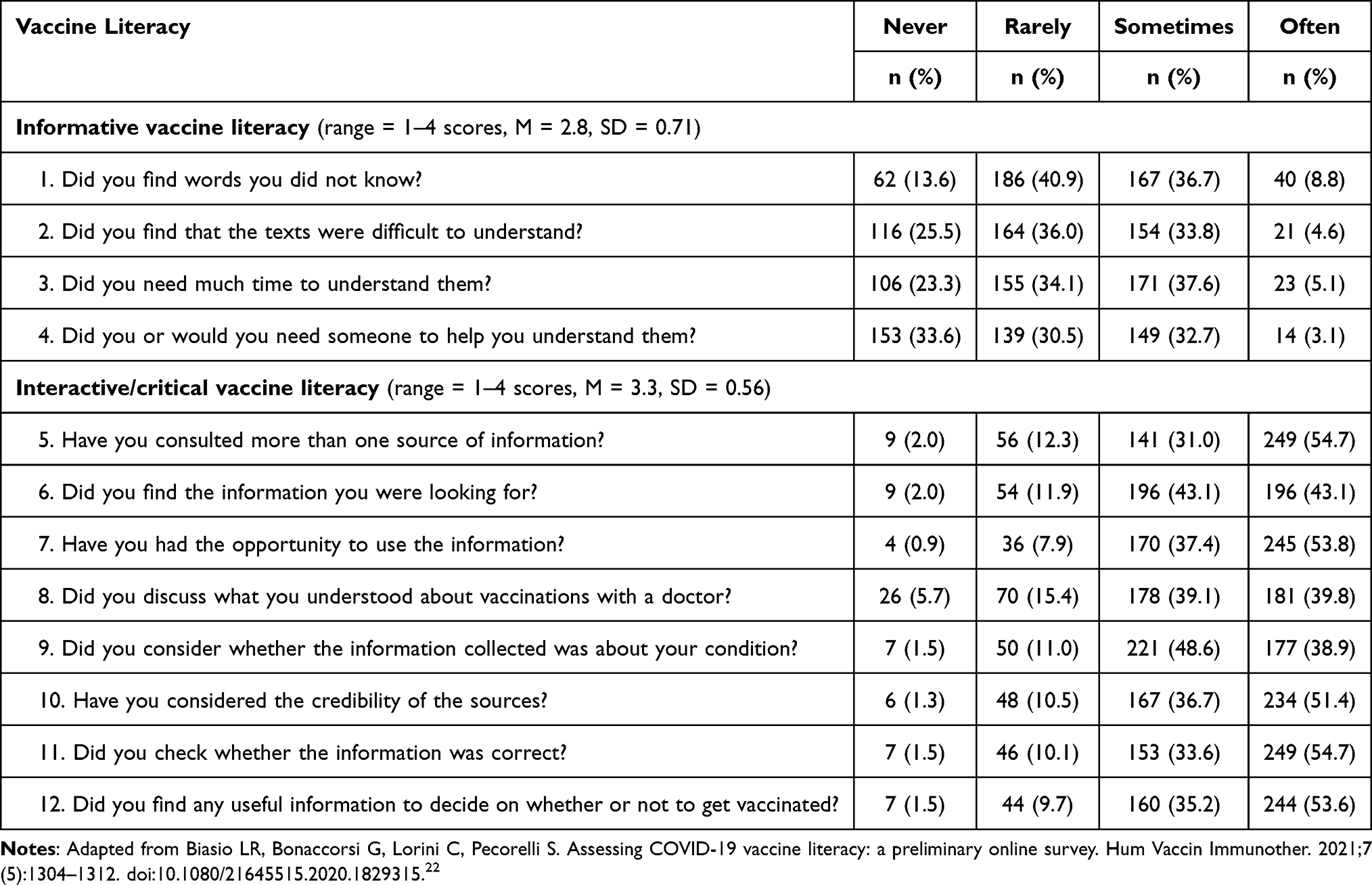 |
Table 3 Participants’ Informative and Interactive/Critical Skills About the COVID-19 Vaccine (n = 455) |
Factors Predicting Participants’ Intention to Vaccinate Their Children Against COVID-19
The univariate logistic regression analyses showed that participants over the age of 35 were more likely to intend to vaccinate their children against COVID-19 compared to those who were younger (Table 4). The odds of intention increased for each year of the child’s age. Unemployed participants and those who reported an insufficient income were less likely to intend to vaccinate their children against COVID-19 compared to those who were employed or who reported a sufficient income. No other sociodemographic characteristics were significantly associated with the participants’ intention to vaccinate their children against COVID-19.
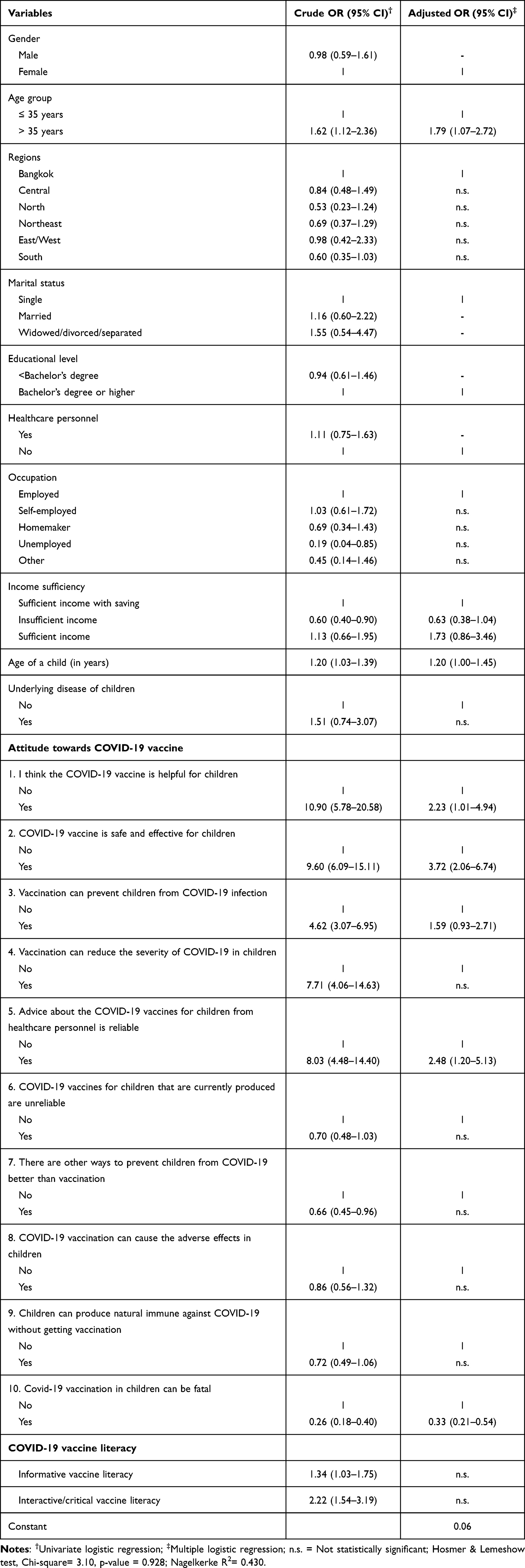 |
Table 4 Factors Associated with Parents’ Intention to Allow Their Children to Receive the COVID-19 Vaccine (n = 455) |
The scores from both the informative literacy skills and the interactive/critical literacy skills were significantly associated with higher odds of participants’ intention to vaccinate their child against COVID-19. All positive attitude items were significantly associated with higher odds of participants’ intention to vaccinate their child against COVID-19. Two negative attitudes were significantly associated with lower odds of participants’ intention to vaccinate their child: those who believed that there are other ways to prevent children from COVID-19 and those who believed that COVID-19 vaccination in children can be fatal.
Similar to univariate logistic regression results, the multiple logistic regression model indicated that participants over 35 years of age significantly predicted their intention to vaccinate their children against COVID-19. Moreover, the positive attitudes of a belief that the COVID-19 vaccine is safe and effective for children, the belief that advice about the COVID-19 vaccines from medical personnel is reliable, and the belief that the COVID-19 vaccine is helpful for children significantly predicted participants’ intention to vaccinate their children. The negative attitude that believing the COVID-19 vaccination in children can be fatal was also a significant predictor in the model.
Participants gave reasons for considering why their children would receive the COVID-19 vaccine (Figure 1). The top three reasons were that 1) “COVID-19 vaccination will reduce the severity of symptoms if infected with COVID-19”, 2) “COVID-19 vaccination will prevent COVID-19 infection, although it is not 100% effective”, and 3) “to protect my children from contracting COVID-19 when they go to school” (Figure 1).
 |
Figure 1 Reasons for participants’ allowing children to receive the COVID-19 vaccine (n = 205). |
The participants reported their hesitancy to vaccinate their children (Figure 2). The top three reasons that were barriers for children receiving the vaccine were 1) I would like to know more information about COVID-19 vaccine for children, 2) I want my children to get a well-tested COVID-19 vaccine, and 3) COVID-19 vaccine may have serious/unsafe side effects to my children.
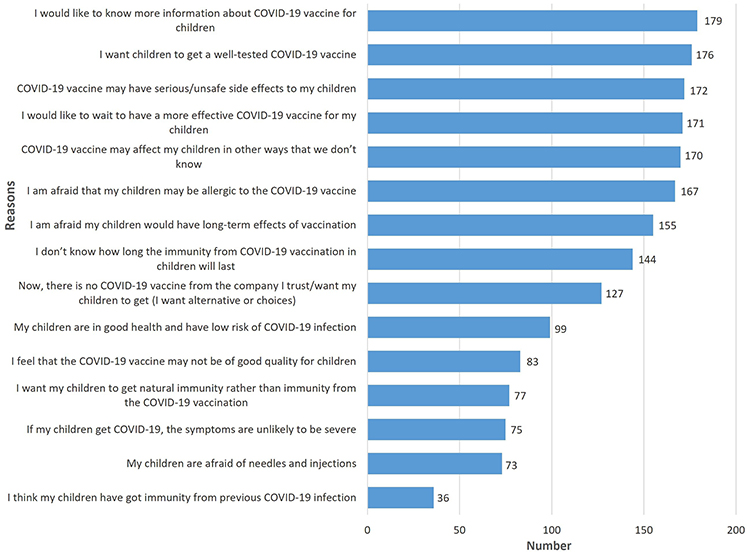 |
Figure 2 Reasons for hesitancy in allowing children to be vaccinated against COVID-19 (n = 188). |
The participants who did not intend to have their children get vaccinated reported concerns related to vaccine efficacy and adverse effects (Figure 3). The top three concerns were 1) the COVID-19 vaccine may have serious side effects in children, 2) I feel that the period of development and testing the COVID-19 vaccines for children is too short, and 3) I am afraid that my child will be allergic to the COVID-19 vaccine.
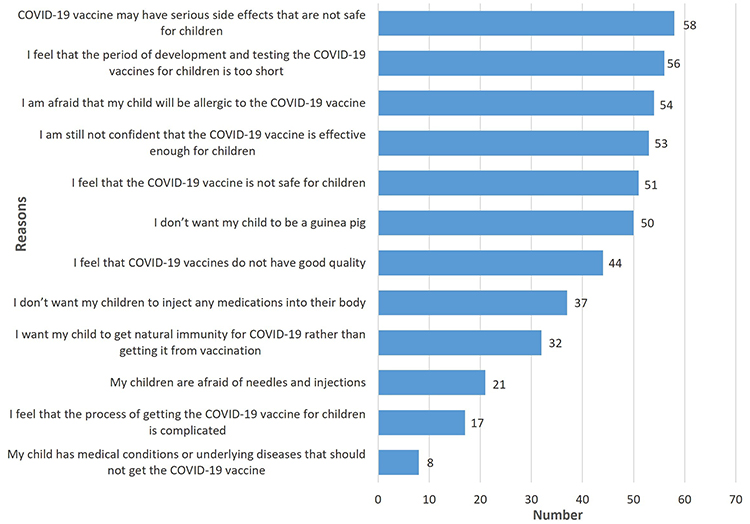 |
Figure 3 Reasons for participants’ refusing their children to receive the COVID-19 vaccine (n = 62). |
Discussion
We sought to determine factors that influenced Thai parents’ vaccine intention for their children under five years of age. Most studies in other countries that have focused on parents’ vaccine intention in this age group were conducted in early 2022 before the midyear authorization of Pfizer-BioNTech and Moderna vaccines for children between six months and five years of age. We found that less than half of Thai parents intended to have their very young children get vaccinated. This is similar to one survey conducted in the US during the first half of 2022 (45.6%),27 but is a higher rate than three other US surveys conducted between April and May 2022: 18%,28 31.3%,23 and 39.7%.29
A scoping review of studies between 2020 and 2021 revealed that the rate of vaccination acceptance for children or adolescents varied widely from 4.9% to 91% and the median acceptance rate was 53.70%.20 They reported that the median acceptance rate after the adolescent vaccine approval (64.2%) was higher than the rate before approval (49.4%).20 None of the studies included in this review, however, focused specifically on parents’ vaccine intention for young children aged under five years of age. Not until early 2022 were most studies conducted of parents’ vaccine intention in that age group.
Vaccine intention rates of COVID-19 for children can differ by the child’s age.23,28 The rate for children under five years old in our study was lower than what has been reported in older children 5–11 years old in Germany (51%),30 Saudi Arabia (61.9%),31 and Canada (63.1%).32 The reported rates of COVID-19 vaccine intention for children has varied across nations due to different time periods of data collection, the COVID-19 situation in the countries, and the period of national vaccine rollout.33–35
One study reported that the most influencing factor on vaccine acceptance for children was the parents’ own willingness to get vaccinated against COVID-19.20 While this association was significant in previous studies,23,36,37 our findings showed that there was a large difference between parents’ intention rate to have their children vaccinated and their own vaccination rate (45.1% versus 98.0%). Thus, we did not test the association between parents’ intention to vaccinate themselves and their intention to vaccinate their children.
We found that parents who were older than 35 years were more likely to have a vaccine intention for their children, whereas unemployed parents or those with insufficient income were less likely to do so. These findings are congruent with previous research.23,37,38 Although we did not find that other sociodemographic characteristics were significant factors, other studies have shown that parents with a bachelor’s degree or higher23,38–40 and healthcare personnel41,42 were more likely to have the intention to vaccinate their children between 5 and 11 years of age.
In the univariate logistic regression, we found that as the very young child got older, the parents’ intention to vaccinate them increased, a similar result reported by Willis et al.43 However, the child’s age was not a significant predictor of parents’ intention in the multiple logistic regression model. In studies of older children, parents were more likely to have the vaccine intention for children 5–11 years old44,45 and those ≥12 years old.40,46 However, a scoping review reported that parents had a lower rate of vaccine intention/acceptance for younger children.20
Like previous studies in children 5–11 years old,40,47,48 we found that having an underlying health condition was not a significant factor associated with parents’ vaccine intention. However, others have reported a relationship between the two factors,49,50 including a finding that younger children with COVID-19 infection and an underlying condition(s) had 19 times higher odds of severe hospitalization.51
Studies have shown that parents with a higher vaccine literacy are more likely to have their children vaccinated against COVID-1952 and an increase in vaccine intention/acceptance in children53 and adults.22,54,55 Because VL enhances a person’s understanding, it involves the decision-making process about vaccination.22,55 We did find a significant association between informative and interactive/critical VL and the parents’ vaccine intention for their children under five years of age in univariate analysis, but neither was a significant factor in the multivariate model. This may be due to parents’ lack of knowledge about the development of a COVID-19 vaccine for the age group. This would make the parents’ judgment about the risks and benefits of the vaccine for their very young children more difficult. Therefore, parents’ vaccine intention for children less than five years old was strongly influenced by parents’ attitudes but not VL.
It has been reported in various studies that parents’ positive attitudes about COVID-19 vaccination are a significant factor in vaccine intention for children.52,56 Forming the basis for parental attitudes that influence vaccine intention are their beliefs that the COVID-19 vaccine is helpful,36 safe and effective,23,36,50,52,57,58 can prevent children from COVID-19 infection,23,59,60 and reduce the severity of COVID-19 in children.59 In addition, we found that parents’ belief in the reliability of medical personnel’s advice/information was associated with higher odds of vaccine intention against COVID-19. This has also been supported by previous studies.23,36,37,58,61
Our results that parents’ negative attitudes are a barrier to vaccine intention are congruent with other studies such as the belief that “there are other ways to prevent children from COVID-19 better than vaccination”32,61,62 and “COVID-19 vaccination in children can be fatal”.23,32 These parental concerns about the vaccine’s side effects can lead to low confidence in their use and have been reported to be the most common barrier to getting vaccinated against COVID-19 in children.57
Websites and social media platforms can provide trustworthy information about COVID-19 and COVID-19 vaccines, but many may be sources of disinformation and fake news.35 Parents with low VL who consume inaccurate information may develop negative attitudes and have low vaccine confidence.20,63 Unfortunately, many parents trust unreliable social media sources which result in increased vaccine hesitancy.20,37
Inadequate VL has been associated not only with personal attitudes toward COVID-19 vaccination but also with COVID-19 vaccine hesitancy.17 Reducing vaccine hesitancy could be achieved by decreasing negative attitudes.19 An important strategy to increase vaccination intention/acceptance would be to enhance positive attitudes about vaccines.17,18,23 Understanding factors influencing parents’ vaccine intention and hesitancy and recognizing the key roles of attitudes and VL and how they interact, could be beneficial for health professionals to tailor specific interventions for parents of children under five years old in order to promote COVID-19 vaccine uptake.
Enhancing positive attitudes about vaccines could be an important strategy to increase vaccine intention and acceptance.17,18,23 Targeted public health campaigns on social media platforms with accurate information about the health benefits and usefulness of COVID-19 vaccines would play a significant role in decreasing negative attitudes and dispelling vaccine hesitancy.19
Strengths and Limitations
We report the first study in Thailand to investigate parents’ vaccine literacy, attitudes toward COVID-19 vaccine, and vaccine intention for children less than five years of age. It was conducted prior to the authorization of Pfizer-BioNTech and Moderna vaccines for children in this age group. The convenience sample of parents underrepresented males, those with low socioeconomic status who did not have internet access, and those who may not have been competent in using digital devices. Although the online survey reached parents with diverse background characteristics from every region in Thailand, the use of a convenience sample decreases the generalizability of the results.
Implications for Practice and Research
Because there is evidence linking negative attitudes with low confidence in vaccines and vaccine hesitancy, effective communication strategies are needed by healthcare personnel about the COVID-19 vaccine and vaccination of young children. Consistent communication with accurate information about research and development of the vaccines by health authorities and health institutions is crucial to identifying and dispelling fake news and disinformation so that public confidence in the COVID-19 vaccine programs will be enhanced. Policymakers need to consider the essential role of vaccine literacy and the key role of healthcare professionals when developing campaigns to target vulnerable groups of parents who have lower socioeconomic status and low vaccine literacy to dispel negative attitudes and reinforce vaccine uptake in children under five years of age. Monitoring child vaccinations, parents’ vaccine literacy, attitudes, and hesitancy is needed as the COVID-19 pandemic has been fluctuating. Interventions promoting vaccine literacy are needed to overcome parents’ vaccine hesitancy by motivating them and enhancing their confidence in the vaccines.
Conclusions
Less than half of Thai parents had vaccine intention to get their children under five years of age vaccinated against COVID-19. The factors of parents’ vaccine intention were parents >35 years old, the belief that the COVID-19 vaccine is safe and effective for children, advice about the COVID-19 vaccines from healthcare personnel is reliable and helpful for children, and that COVID-19 vaccination in children can be fatal. Parents’ belief that the “COVID-19 vaccine is safe and effective for children” was the strongest influencing factor, whereas the strongest barrier to vaccine intention was their belief that “COVID-19 vaccination in children can be fatal.” Targeting parents with lower vaccine literacy, negative attitudes, and low vaccine confidence is a crucial health prevention measure for very young children.
Data Sharing Statement
Data supporting this study are available from the corresponding author.
Acknowledgments
The researchers would like to thank the parents who participated in this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kaye AD, Okeagu CN, Pham AD, et al. Economic impact of COVID-19 pandemic on healthcare facilities and systems: international perspectives. Best Pract Res Clin Anaesthesiol. 2021;35(3):293–306. doi:10.1016/j.bpa.2020.11.009
2. World Health Organization. Strategy to achieve global Covid-19 vaccination by mid-2022; 2021. Available from: https://cdn.who.int/media/docs/default-source/immunization/covid-19/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022.pdf.
3. Kaur SP, Gupta V. COVID-19 vaccine: a comprehensive status report. Virus Res. 2020;288:198114. doi:10.1016/j.virusres.2020.198114
4. World Health Organization. Vaccine efficacy, effectiveness and protection; 2021. Available from: https://www.who.int/news-room/feature-stories/detail/vaccine-efficacy-effectiveness-and-protection.
5. Mohammed I, Nauman A, Paul P, et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: a systematic review. Hum Vaccin Immunother. 2022;18(1):2027160. doi:10.1080/21645515.2022.2027160
6. Centers for Disease Control and Prevention. CDC recommends COVID-19 vaccines for young children; 2022. Available from: https://www.cdc.gov/media/releases/2022/s0618-children-vaccine.html#print.
7. Irfan O, Muttalib F, Tang K, Jiang L, Lassi ZS, Bhutta Z. Clinical characteristics, treatment and outcomes of paediatric COVID-19: a systematic review and meta-analysis. Arch Dis Child. 2021;106(5):440–448. doi:10.1136/archdischild-2020-321385
8. World Health Organization. Interim statement on COVID-19 vaccination for children and adolescents; 2021. Available from: https://www.who.int/news/item/11-08-2022-interim-statement-on-covid-19-vaccination-for-children.
9. Shi DS, Whitaker M, Marks KJ, et al. Hospitalizations of children aged 5–11 years with laboratory-confirmed COVID-19 – COVID-NET, 14 states, March 2020–February 2022. MMWR Morb Mortal Wkly Rep. 2022;71(16):574–581. doi:10.15585/mmwr.mm7116e1
10. Harwood R, Yan H, Talawila Da Camara N, et al. Which children and young people are at higher risk of severe disease and death after hospitalisation with SARS-CoV-2 infection in children and young people: a systematic review and individual patient meta-analysis. EClinicalMedicine. 2022;44:101287. doi:10.1016/j.eclinm.2022.101287
11. Department of Disease Control. Situation of COVID-19 in children (ages 0–18 years) in Thailand from 1 April – 24 November 2021: Report number 8. 2021. Thai.
12. Center of COVID-19 Information. The Government Public Relations Department (Thailand); 2022. Available from: https://th-th.facebook.com/informationcovid19.
13. ThaiPost. Found children aged 10–14 years infected with COVID up to 20.22 percent. Most come family members. Encourage more children to be vaccinated; 2022. Thai. Available from: https://www.thaipost.net/covid-19-news/83164.
14. Thai PBS. Prevalence of COVID-19 among Thai children was 31,811 cases in 4 months; 2021. Thai. Available from: https://www.thaipbs.or.th/news/content/307445.
15. Ministry of Education. Statistical report in Thailand; 2018. Available from: http://social.nesdc.go.th/SocialStat/StatReport_Final.aspx?reportid=3536&template=2R2C&yeartype=M&subcatid=20.
16. Hou Z, Tong Y, Du F, et al. Assessing COVID-19 vaccine hesitancy, confidence, and public engagement: a global social listening study. J Med Internet Res. 2021;23(6):e27632. doi:10.2196/27632
17. Fisher KA, Bloomstone SJ, Walder J, Crawford S, Fouayzi H, Mazor KM. Attitudes toward a potential SARS-CoV-2 vaccine: a survey of U.S. adults. Ann Intern Med. 2020;173(12):964–973. doi:10.7326/m20-3569
18. Kadoya Y, Watanapongvanich S, Yuktadatta P, et al. Willing or hesitant? A socioeconomic study on the potential acceptance of COVID-19 vaccine in Japan. Int J Environ Res Public Health. 2021;18(9):4864. doi:10.3390/ijerph18094864
19. Dodd RH, Cvejic E, Bonner C, Pickles K, McCaffery KJ. Willingness to vaccinate against COVID-19 in Australia. Lancet Infect Dis. 2021;21(3):318–319. doi:10.1016/s1473-3099(20)30559-4
20. Liu Y, Ma Q, Liu H, Guo Z. Public attitudes and influencing factors toward COVID-19 vaccination for adolescents/children: a scoping review. Public Health. 2022;205:169–181. doi:10.1016/j.puhe.2022.02.002
21. Motoki K, Saito T, Takano Y. Scientific literacy linked to attitudes toward COVID-19 vaccinations: a pre-registered study. Front Commun. 2021;6. doi:10.3389/fcomm.2021.707391
22. Biasio LR, Bonaccorsi G, Lorini C, Pecorelli S. Assessing COVID-19 vaccine literacy: a preliminary online survey. Hum Vaccin Immunother. 2021;7(5):1304–1312. doi:10.1080/21645515.2020.1829315
23. Fisher CB, Bragard E, Jaber R, Gray A. COVID-19 vaccine hesitancy among parents of children under five years in the United States. Vaccines. 2022;10(8):1313. doi:10.3390/vaccines10081313
24. Maneesriwongul W, Butsing N, Visudtibhan PJ, Leelacharas S, Kittipimpanon K. Translation and psychometric testing of the Thai COVID-19 vaccine literacy scale. Pacific Rim Int J Nurs Res. 2021;26(1):175–186.
25. R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2018. Available from: http://www.R-project.org/.
26. Hosmer DW, Lemeshow S. Applied Logistic Regression.
27. Scherer AM, Gidengil CA, Gedlinske AM, et al. COVID-19 vaccination intentions, concerns, and facilitators among US parents of children ages 6 months through 4 years. JAMA Netw Open. 2922;5(8):e2227437. doi:10.1001/jamanetworkopen.2022.27437
28. Sparks G, Lopes L, Montero A, et al. KFF COVID-19 vaccine monitor. Kaiser Family Foundation. Available from: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-april-2022/.
29. Mangat C, Rich J, Sanghavi D, et al. Parents’ perspective on COVID-19 vaccine in children 6 months through 4 years: a cross-sectional study from Northwest Wisconsin. BMJ Open. 2022;12(9):e065453. doi:10.1136/bmjopen-2022-065453
30. Brandstetter S, Böhmer MM, Pawellek M, et al. Parents’ intention to get vaccinated and to have their child vaccinated against COVID-19: cross-sectional analyses using data from the KUNO-kids health study. Eur J Pediatr. 2021;180(11):3405–3410. doi:10.1007/s00431-021-04094-z
31. Almalki OS, Alfayez OM, Al Yami MS, Asiri YA, Almohammed OA. Parents’ hesitancy to vaccinate their 5–11-year-old children against COVID-19 in Saudi Arabia: predictors from the Health Belief Model. Front Public Health. 2022;10:842862. doi:10.3389/fpubh.2022.842862
32. Humble RM, Sell H, Dubé E, et al. Canadian parents’ perceptions of COVID-19 vaccination and intention to vaccinate their children: results from a cross-sectional national survey. Vaccine. 2021;39(52):7669–7676. doi:10.1016/j.vaccine.2021.10.002
33. de Figueiredo A, Larson HJ. Exploratory study of the global intent to accept COVID-19 vaccinations. Commun Med. 2021;1:30. doi:10.1038/s43856-021-00027-x
34. Sallam M, Al-Sanafi M, Sallam M. A global map of COVID-19 vaccine acceptance rates per country: an updated concise narrative review. J Multidiscip Healthc. 2022;15:21–45. doi:10.2147/jmdh.S347669
35. Shakeel CS, Mujeeb AA, Mirza MS, Chaudhry B, Khan SJ. Global COVID-19 vaccine acceptance: a systematic review of associated social and behavioral factors. Vaccines. 2022;10(1). doi:10.3390/vaccines10010110
36. Choi SH, Jo YH, Jo KJ, Park SE. Pediatric and parents’ attitudes towards COVID-19 vaccines and intention to vaccinate for children. J Korean Med Sci. 2021;36(31):e227–e227. doi:10.3346/jkms.2021.36.e227
37. Horiuchi S, Sakamoto H, Abe SK, et al. Factors of parental COVID-19 vaccine hesitancy: a cross sectional study in Japan. PLoS One. 2021;16(12):e0261121. doi:10.1371/journal.pone.0261121
38. Bagateli LE, Saeki EY, Fadda M, Agostoni C, Marchisio P, Milani GP. COVID-19 vaccine hesitancy among parents of children and adolescents living in Brazil. Vaccines. 2021;9(10):1115. doi:10.3390/vaccines9101115
39. McElfish PA, Willis DE, Shah SK, et al. Parents’ and guardians’ intentions to vaccinate children against COVID-19. Vaccines. 2022;10(3):361. doi:10.3390/vaccines10030361
40. Zychlinsky Scharff A, Paulsen M, Schaefer P, et al. Students’ age and parental level of education influence COVID-19 vaccination hesitancy. Eur J Pediatr. 2022;181(4):1757–1762. doi:10.1007/s00431-021-04343-1
41. Babicki M, Pokorna-Kałwak D, Doniec Z, Mastalerz-Migas A. Attitudes of parents with regard to vaccination of children against COVID-19 in Poland. A nationwide online survey. Vaccines. 2021;9(10):1192. doi:10.3390/vaccines9101192
42. Temsah MH, Alhuzaimi AN, Aljamaan F, et al. Parental attitudes and hesitancy about COVID-19 vs. routine childhood vaccinations: a national survey. Front Public Health. 2021;9:752323. doi:10.3389/fpubh.2021.752323
43. Willis DE, Schootman M, Shah SK, et al. Parent/guardian intentions to vaccinate children against COVID-19 in the United States. Hum Vaccin Immunother. 2022;18(5):2071078. doi:10.1080/21645515.2022.2071078
44. Ellithorpe ME, Aladé F, Adams RB, Nowak GJ. Looking ahead: caregivers’ COVID-19 vaccination intention for children 5 years old and younger using the health belief model. Vaccine. 2022;40(10):1404–1412. doi:10.1016/j.vaccine.2022.01.052
45. Goldman RD, Yan TD, Seiler M, et al. Caregiver willingness to vaccinate their children against COVID-19: cross sectional survey. Vaccine. 2020;38(48):7668–7673. doi:10.1016/j.vaccine.2020.09.084
46. Gewirtz-Meydan A, Mitchell K, Shlomo Y, Heller O, Grinstein-Weiss M. COVID-19 among youth in Israel: correlates of decisions to vaccinate and reasons for refusal. J Adolesc Health. 2022;70(3):396–402. doi:10.1016/j.jadohealth.2021.11.016
47. Ali M, Proma TS, Tasnim Z, et al. Parental COVID-19 vaccine hesitancy for children with neurodevelopmental disorders: a cross-sectional survey. Trop Med Health. 2022;50(1):24. doi:10.1186/s41182-022-00415-6
48. Miraglia Del Giudice G, Napoli A, Corea F, Folcarelli L, Angelillo IF. Evaluating COVID-19 vaccine willingness and hesitancy among parents of children aged 5–11 years with chronic conditions in Italy. Vaccines. 2022;10(3):396. doi:10.3390/vaccines10030396
49. Di Giuseppe G, Pelullo CP, Lanzano R, Napolitano F, Pavia M. Knowledge, attitudes, and behavior of incarcerated people regarding COVID-19 and related vaccination: a survey in Italy. Sci Rep. 2022;12(1):960. doi:10.1038/s41598-022-04919-3
50. Russo L, Croci I, Campagna I, et al. Intention of parents to immunize children against SARS-CoV-2 in Italy. Vaccines. 2021;9(12):1469. doi:10.3390/vaccines9121469
51. European Centre for Disease Prevention and Control. Interim public health considerations for COVID-19 vaccination of children aged 5–11 years; 2021. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/TGU-20211119-1925_final-for-publication.pdf.
52. Gendler Y, Ofri L. Investigating the influence of vaccine literacy, vaccine perception and vaccine hesitancy on Israeli parents’ acceptance of the COVID-19 vaccine for their children: a cross-sectional study. Vaccines. 2021;9(12):1391. doi:10.3390/vaccines9121391
53. Wang X, Zhou X, Leesa L, Mantwill S. The effect of vaccine literacy on parental trust and intention to vaccinate after a major vaccine scandal. J Health Commun. 2018;23(5):413–421. doi:10.1080/10810730.2018.1455771
54. Kittipimpanon K, Maneesriwongul W, Butsing N, Janepanish Visudtibhan P, Leelacharas S. COVID-19 vaccine literacy, attitudes, and vaccination intention against COVID-19 among Thai older adults. Patient Prefer Adherence. 2022;16:2365–2374. doi:10.2147/PPA.S376311
55. Ratzan S, Parker RM. Vaccine literacy—helping everyone decide to accept vaccination. J Health Commun. 2020;25(10):750–752. doi:10.1080/10810730.2021.1875083
56. Yılmaz M, Sahin MK. Parents’ willingness and attitudes concerning the COVID-19 vaccine: a cross-sectional study. Int J Clin Pract. 2021;75(9):e14364. doi:10.1111/ijcp.14364
57. Lin Y, Hu Z, Zhao Q, Alias H, Danaee M, Wong LP. Chinese parents’ intentions to vaccinate their children against SARS-CoV-2 infection and vaccine preferences. Hum Vaccin Immunother. 2021;17(12):4806–4815. doi:10.1080/21645515.2021.1999143
58. Szilagyi PG, Shah MD, Delgado JR, et al. Parents’ intentions and perceptions about COVID-19 vaccination for their children: results from a national survey. Pediatrics. 2021;148(4). doi:10.1542/peds.2021-052335
59. Alobaidi S. Predictors of intent to receive the COVID-19 vaccination among the population in the Kingdom of Saudi Arabia: a survey study. J Multidiscip Healthc. 2021;14:1119–1128. doi:10.2147/JMDH.S306654
60. Chen H, Li X, Gao J, et al. Health Belief Model perspective on the control of COVID-19 vaccine hesitancy and the promotion of vaccination in China: web-based cross-sectional study. J Med Internet Res. 2021;23(9):e29329. doi:10.2196/29329
61. Ebrahimi OV, Johnson MS, Eblin S. Risk, trust, and flawed assumptions: vaccine hesitancy during the COVID-19 pandemic. Front Public Health. 2021;9:Article700213. doi:10.3389/fpubh.2021.700213
62. Paul E, Steptoe A, Fancourt D. Attitudes towards vaccines and intention to vaccinate against COVID-19: implications for public health communications. Lancet Reg Health Eur. 2021;1:100012. doi:10.1016/j.lanepe.2020.100012
63. Pan F, Zhao H, Nicholas S, Maitland E, Liu R, Hou Q. Parents’ decisions to vaccinate children against COVID-19: a scoping review. Vaccines. 2021;9(12):1476. doi:10.3390/vaccines9121476
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Parental Attitudes Towards Vaccination Against COVID-19 in China During Pandemic
Lu L, Gu W, Xie H, Wang X, Cao L, Shan M, Wu P, Tian Y, Zhou K
Infection and Drug Resistance 2022, 15:4541-4546
Published Date: 15 August 2022
COVID-19 Vaccine Literacy, Attitudes, and Vaccination Intention Against COVID-19 Among Thai Older Adults
Kittipimpanon K, Maneesriwongul W, Butsing N, Janepanish Visudtibhan P, Leelacharas S
Patient Preference and Adherence 2022, 16:2365-2374
Published Date: 30 August 2022
Acceptance and Hesitancy Toward the Covid-19 Vaccine Among Medical Students in Kabul, Afghanistan
Azimi M, Yadgari MY, Atiq MA
Infection and Drug Resistance 2023, 16:457-461
Published Date: 25 January 2023
Assessment of Parental Knowledge, Awareness, and Perception About Autism Spectrum Disorders in Aseer Region, Southwestern Saudi Arabia
AlAlmaei Asiri WM, Shati AA, Al-Qahtani SM, Al-Qahtani YA, Aldarami MS, Alamri FD, Alshahrani HS, Esam Mahmood S
International Journal of General Medicine 2023, 16:557-564
Published Date: 16 February 2023
Treatment Adherence and Related Factors Among Children with Attention-Deficit/Hyperactivity Disorder in Saudi Arabia
Alsubaie MA, Alshehri ZY, Alawadh IA, Abulreesh RY, Altaweel HM, Alateeq DA
Patient Preference and Adherence 2024, 18:337-348
Published Date: 3 February 2024