Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Paramedic Ability in Interpreting Electrocardiogram with ST-segment Elevation Myocardial Infarction (STEMI) in Saudi Arabia
Authors Alrumayh AA ![]() , Mubarak AM
, Mubarak AM ![]() , Almazrua AA, Alharthi MZ, Alatef DF, Albacker TB, Samarkandy FM, Alsofayan YM
, Almazrua AA, Alharthi MZ, Alatef DF, Albacker TB, Samarkandy FM, Alsofayan YM ![]() , Alobaida M
, Alobaida M ![]()
Received 22 April 2022
Accepted for publication 20 July 2022
Published 4 August 2022 Volume 2022:15 Pages 1657—1665
DOI https://doi.org/10.2147/JMDH.S371877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdullah A Alrumayh,1 Abdullah M Mubarak,1 Abdulkarim A Almazrua,2 Musab Z Alharthi,3 Deem F Alatef,4 Turki B Albacker,5 Fahad M Samarkandy,6 Yousef M Alsofayan,7 Muath Alobaida1
1Department of Basic Sciences, Prince Sultan Bin Abdulaziz College for Emergency Medical Services, King Saud University, Riyadh, Saudi Arabia; 2Department of Aviation and Marine, Prince Sultan Bin Abdulaziz College for Emergency Medical Services, King Saud University, Riyadh, Saudi Arabia; 3Department of Accident and Trauma, Prince Sultan Bin AbdulazizCollege for Emergency Medical Services, King Saud University, Riyadh, Saudi Arabia; 4Department of Emergency Medical Services and Disaster Management, King Saud Medical City, Riyadh, Saudi Arabia; 5Department of Cardiac Sciences, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 6Department of Operational Affairs, Saudi Red Crescent Authority, Riyadh, Saudi Arabia; 7Executive Directorate of Medical Affairs, Saudi Red Crescent Authority, Riyadh, Saudi Arabia
Correspondence: Muath Alobaida, Department of Basic Sciences, Prince Sultan Bin Abdulaziz College for Emergency Medical Services, King Saud University, Riyadh, Saudi Arabia, Email [email protected]
Objective: To evaluate paramedic ability in recognizing 12-lead Electrocardiogram (ECG) with ST-segment Elevation myocardial infarction (STEMI) in Saudi Arabia.
Methods: This is a quantitative exploratory cross-sectional study using an electronic survey of paramedics was conducted between June and September 2021. The survey included demographics, educational and clinical experiences, and multiple 12-lead ECG strip questions to assess participants’ ability to recognize STEMI. We reported the overall sensitivity, specificity, and correct proportions with 95% Confidence Intervals (CI).
Results: Eighty-four paramedics completed the survey, and 65% of them were between 24 and 29 years old, with a median, of three years of field experience. Overall sensitivity and specificity were 58.39% (95% CI, 50.4% to 66.1%) and 29.01% (95% CI, 25.15% to 33.1%), respectively. In total, 67.1% correctly identified inferior STEMI, whereas only 50% correctly identified lateral STEMI. Both STEMIs were correctly identified by 41%, and the majority misinterpreted STEMI mimics (ECG rhythms with similar ECG morphology to STEMI). The proportion who correctly recognized left bundle branch block was 14.8%, pericarditis was 10.9%, and ventricular pacing was 1.4%. However, almost third of participants correctly identified right bundle branch block (32.9%) and left ventricle hypertrophy (30.7%). Overall, there was no correlation between the correct ECG interpretation of STEMIs and educational and clinical experiences.
Conclusion: Paramedics were able to identify STEMI events in prehospital settings with moderate sensitivity and low specificity with limited ability to differentiate between STEMI and STEMI mimics. Therefore, additional training in ECG interpretation could improve their clinical decision-making, and to ensure that proper care and treatment is provided. Further research on a large, representative sample of paramedics across the country could provide more definitive evidence to establish a greater degree of accuracy in detecting STEMI in prehospital settings.
Keywords: paramedic, electrocardiogram, ST segment elevation myocardial infarction, emergency medical services, myocardial infarction
Key Messages
- Paramedics in Saudi Arabia are more likely to identify the presence of STEMI patterns than the type of STEMI.
- The overall accuracy of ECG interpretation by paramedics is proportionally lower than in other countries, and further training is warranted.
- The results suggested no plausible evidence that education levels and years of experience were potential predictors of successful interpretation of 12-lead ECG.
Introduction
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality worldwide.1,2 Diagnosing and treating acute coronary occlusion involves early and rapid interpretation of a 12-lead Electrocardiogram (ECG), which helps reduce the chances of mortality and improves timely reperfusion.3 Moreover, the shorter the door-to-balloon time, the higher the likelihood of reperfusion following percutaneous coronary intervention.3 Studies on patient with Acute Myocardial Infarction (AMI) have shown the benefits of early fibrinolytic therapies.4 Delays in treatment initiation may result in complete myocardial injury, which, over time, leads to irreversible damage.5,6 American Heart Association and American College of Cardiology guidelines recommend obtaining and monitoring 12-lead ECGs within ten minutes of any suspected AMI. Pre-arrival activation of cardiac catheterization laboratory may be performed based on prehospital ECG interpretation in patients with suspected STEMI.7,8 Various studies have been conducted to evaluate the accuracy of paramedics, cardiologists, health-care residents, and emergency physicians in diagnosing STEMI.9,10 It has been reported that cardiologists were more precise in detecting STEMIs than paramedics and were less influenced by confounding factors in the presenting ECGs.9 Another study has reported that paramedic diagnoses of STEMI were correct in about 80% of the cases.10 In contrast, another study stated that skilled paramedics could precisely recognize STEMIs on the ECG with a sensitivity of 70% and a specificity of 90%.11
A scenario-based study performed on paramedics at Yale University School of Medicine revealed that for STEMI diagnosis, paramedics’ sensitivity was 92.6%, and their specificity was 85.4%.11 Similarly, a study in Canada found that paramedics had a sensitivity rate of 95% and a specificity of 96%.12 The existing literature reveals some degree of heterogeneity due to varying levels of training, experience, and exposure to cardiovascular emergencies among Emergency Medical Services (EMS) personnel.
Nevertheless, studies that evaluate paramedics’ accuracy in 12-lead ECG interpretation are still lacking. Therefore, this study aims to evaluate Saudi paramedics’ ability to interpret various STEMIs in 12-lead ECGs in a primary EMS service in Saudi Arabia.
Method
Study Design and Setting
This is a quantitative exploratory cross-sectional study that was conducted on paramedic providers, using an electronic assessment survey measuring the accuracy in interpreting ECGs with STEMI. We distributed the survey to all paramedics employed by the Saudi Red Crescent Authority (SRCA) in Riyadh, Saudi Arabia. The study took place between June 1, and September 1, 2021 when we visited multiple SRCA ambulance sites to ask on-duty paramedics to fill out e-assessment surveys. Participants were asked to complete an anonymous computer-based survey after obtaining their consent to take part in our study. The first section of the survey included participants’ demographics, field experience, levels of ECG training and practice, qualifications, confidence in their ability to interpret STEMI, and weekly exposure to field ECG interpretation.
The second section of the survey asked the paramedics to read and answer from multiple strips of 12-lead ECGs that corresponded to the study’s ECG criteria, which were adopted and modified from a previous study.13 The criteria for selecting the 12-lead ECG strips were as follows: (1) Each 12-lead ECG strip had to be recorded in prehospital or hospital settings, with a wave morphology of STEMI, STEMI mimic, or Normal Sinus Rhythm (NSR); (2) Each ECG strip had to be reviewed, diagnosed interpreted by two blinded cardiologists independently. Disagreements on diagnosis could be resolved by a third independent cardiologist as an option but were not required. Moreover, although all ECGs were retrieved from online sources,13–21 these ECGs were validated per the study criteria.
Initially, the participants were asked whether the ECG strip represented a pattern of STEMI. The selected ECGs included two NSRs; two random types of STEMIs; and five potential STEMI mimics (Left ventricular Hypertrophy [LVH], Ventricular Pacing (VP), pericarditis, and Left and Right Bundle Branch Blocks [LBBB, RBBB]). The survey displayed each ECG question in random order for 60 seconds. Once the participant had provided a response, or 60 seconds had elapsed, the ECG was automatically removed from view, and the participant was moved to the next ECG strip. This time-limit function used in the study is particularly useful in studying the accuracy of interpreting 12-lead ECGs with STEMI, as it creates digitally simulating experience to mimic real STEMI calls seen in uncontrolled, prehospital settings.
Participants and Sample Size
The study sample included all paramedics included in the SRCA administrative database of registered and employed in SRCA stations in Riyadh. In total, there were 106 Advanced Life Support (ALS) paramedics in Riyadh (Department of Operational Affairs, Saudi Red Crescent Authority, personal communication, May 01, 2021), out of whom we recruited 84 participants from 32 different stations. The remaining 22 were either on extended vacation or were could not be reached, with no rejections occurring during recruitment. The study team members provided the survey to the paramedics, with an average completion time of 16 minutes. Since the introductory statement was provided in each survey, the study team members were not allowed to offer any explanations or clarifications to participants in order to avoid explanatory bias.
Key Outcome Measures
The primary outcomes were the sensitivity and specificity of the paramedic in recognizing 12-lead ECGs with STEMI. The secondary outcome was a determination of the effect of exposure on their sensitivity and specificity in recognizing STEMI. These exposures were recent ECG training (over the past two years), time of last ECG course (in months), the average duration of the ECG course (in days), number of ECGs interpreted per week (rhythm per week), valid advanced cardiovascular life support license, level of confidence (3-point Likert scale), the effect of computerized ECG interpretation (3-point Likert scale), years of experience as an ALS paramedic, and level of educational qualification.22 Further, confidence and weekly ECG exposure were predictive measure for higher accuracy, as described.23
Statistical Analysis
The collected data were analyzed using Stata (version 15.1; Stata Corp., College Station, TX). Descriptive statistics were performed to describe the variables of interest, where categorical variables were presented as count and percentage, while continuous variables were presented as mean ± SD or median with interquartile range (IQR), given its normality. Data normality was evaluated using the Shapiro–Wilk normality test.24 We calculated the sensitivity and specificity, as previously described.23 Additionally, we studied the correlation of the correct identification of ECG interpretation using polychoric correlation for Likert scale variables. Spearman correlation was used as well to determine correlations between the correct interpretation of STEMI ECGs and variables of interest. Results yielding a p-value of less than 0.05 were considered statistically significant.
Ethical Considerations
The data were kept confidential and securely stored separately, with no personally identifiable information of participants. No individual identities were used in any reports or publications resulting from the study. Only some of the researchers had access to these files for the sake of data analysis. Ethical approval was obtained for this study from the institutional Review Board (IRB)/ethical research committee at King Saud University Hospital (research project number 21/0432/IRB/06/05/2021) and the SRCA research committee.
Results
The baseline characteristics of the participants are shown in Table 1. Eighty-four surveys were collected from SRCA participants under the direction and supervision of the research team members. Sixty-five percent (55/84) of the respondents were aged between 24 and 29 years old, with a median IQR of three years of EMS experience. Those who received course training on ECGs within the preceding two years were 59% (50/84), and 48% (24/50) within the last 7–12 months. Over half (27/50) of the respondents took a two-day ECG course. Two-thirds (56/84) of the paramedics stated that they received or interpreted one or two ECG per week in the field. Also, 57% (48/84) stated that they were confident in identifying The STEMIs on a prehospital ECG. 69% (58/84) felt that they were comfortable with the impact of a computer-generated rhythm diagnosis on their ECG interpretation decision.
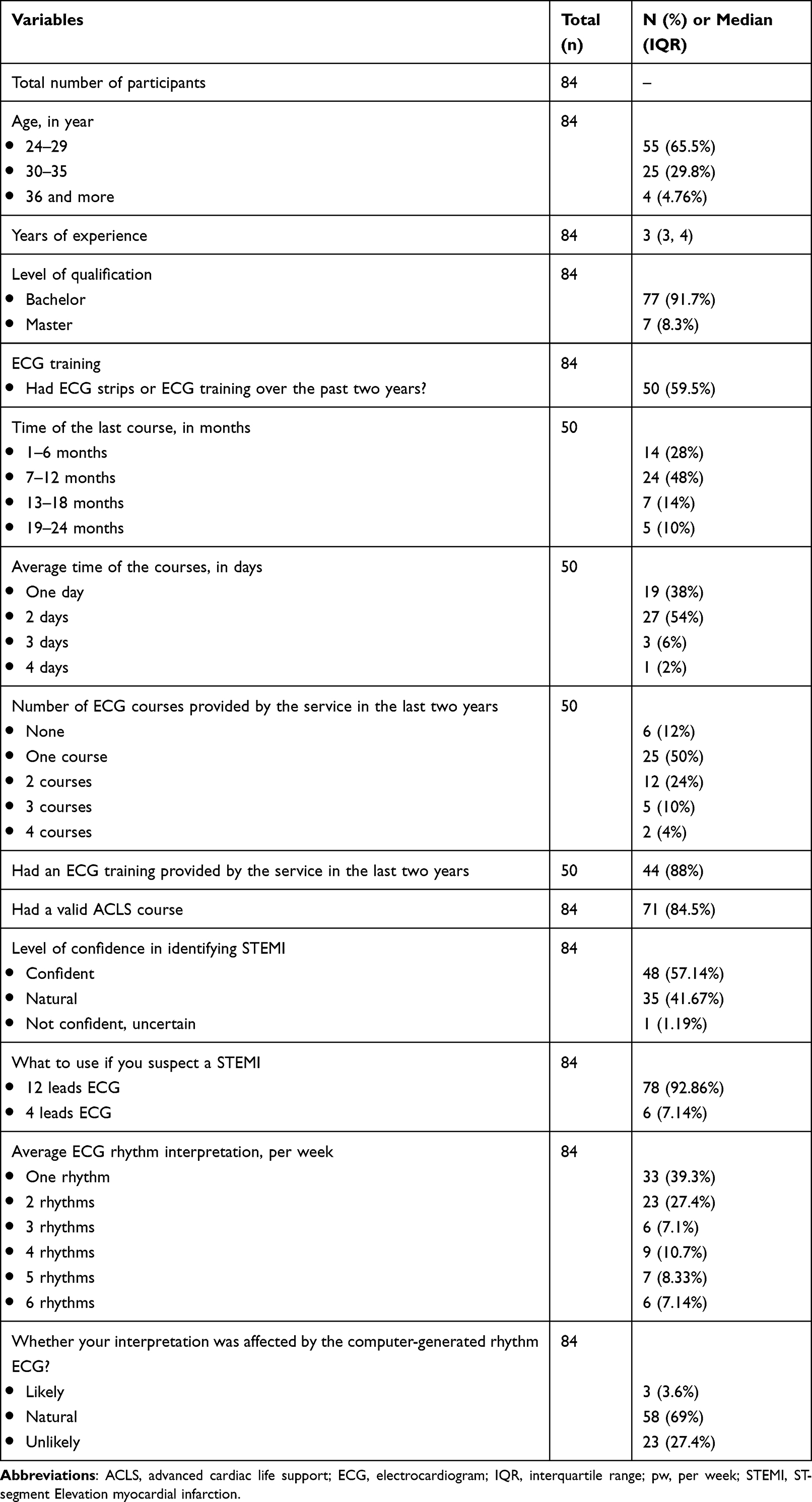 |
Table 1 Baseline Characteristics of Advance Life Support Paramedic, in Riyadh, Saudi Arabia |
Overall, there were nine ECGs in the survey; two were NSRs as non-STEMI ECGs, which paramedics had accurately identified 72.3% (47/65) and 47.9% (34/71) of the time, respectively. STEMI and STEMI mimics are presented in Table 2. Two ECGs represented inferior and lateral STEMI, where over two-thirds of paramedics 67.1% (53/79) correctly identified the inferior STEMI; however, 50% (41/82) failed to recognize the lateral STEMI and 20% misinterpreted lateral as inferior STEMI. Paramedics who were confident in their ECG skills interpreted lateral STEMI 66% (27/41) of the time, compared to paramedics who were neutral and had 34% (14/41) accuracy (p = 0.1). However, there is little plausible evidence of correlation between the paramedics who were confident and correctly identified inferior STEMI 67% (35/53) as compared to the paramedics who were neutral in 12-lead interpretation and had correctly identified inferior STEMI 34% (18/53) (p = 0.02). Overall sensitivity and specificity were 58.39% (94/161, 95%, CI, 50.36% to 66.09%) and 29.01% (152/524, 95% CI, 25.15% to 33.10%), respectively. Also, the stratified proportions of paramedics who recognized STEMI mimics as STEMI only (false positive) are presented in Table 2.
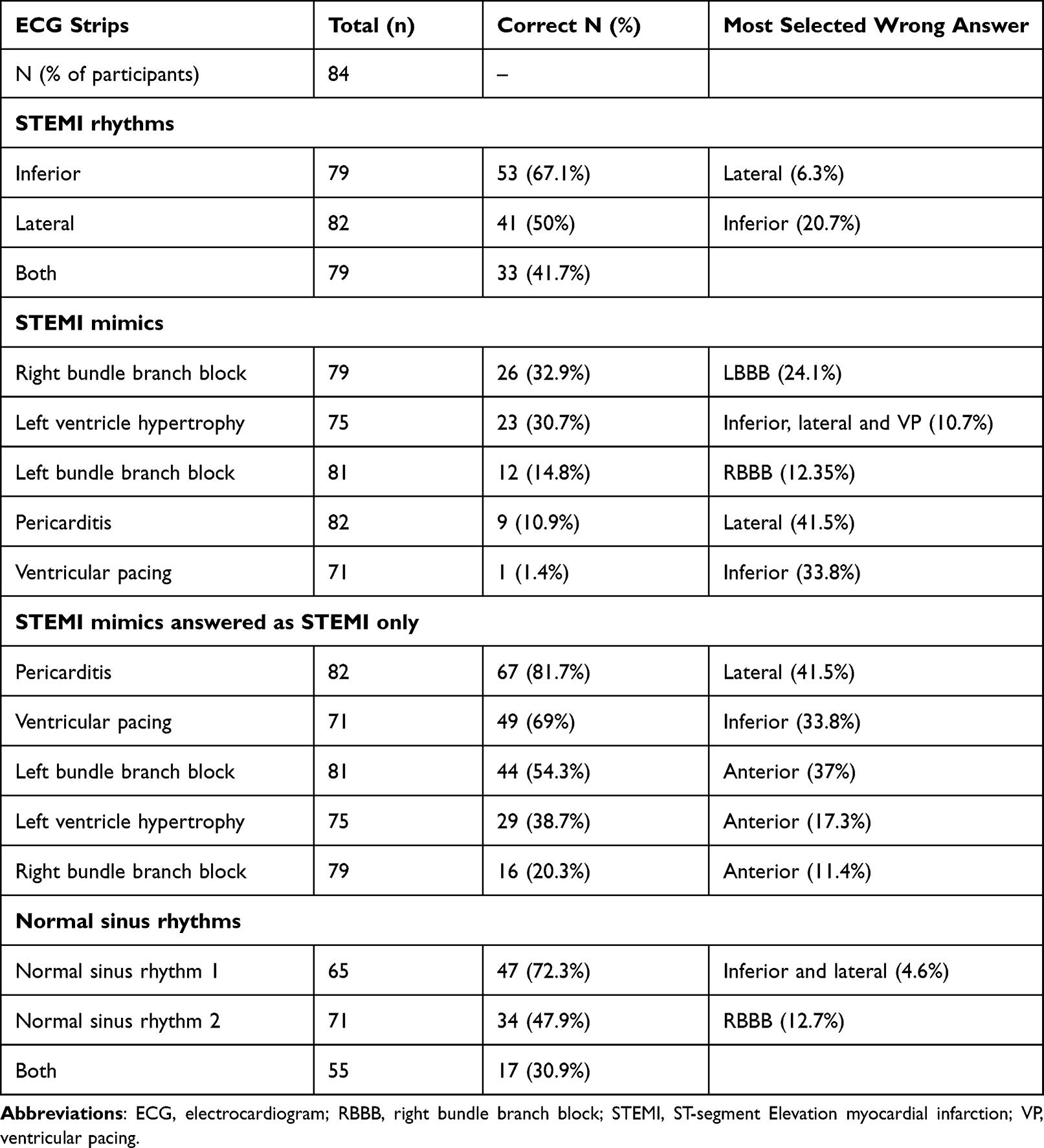 |
Table 2 Accurate Identification of STEMI and STEMI Mimics by Paramedics |
Moreover, most paramedics misinterpreted the remaining five ECGs with STEMI mimics. For example, participants accurately interpreted LBBB only 14.8% (12/81) of the time, pericarditis 10.9% (9/82), and VP 1.4% (1/71). However, almost one-third of the paramedics correctly identified RBBB and LVH at 32.9% (26/79) and 30.7% (23/75), respectively. Both STEMIs (inferior and lateral) were correctly identified by 41% (33/79). However, none of the paramedics could correctly recognize all the STEMI mimics as not STEMI.
Overall, there was no correlation between the correct ECG interpretation of STEMI and years of experience, level of qualification, the average number of ECG interpretations per week, and level of comfort or confidence.
Discussion
This study measured the ability of paramedics to correctly interpret ECGs with STEMI in prehospital settings in the city of Riyadh, Saudi Arabia. This study is the first nationwide article to examine ALS paramedics’ accuracy levels in interpreting ECGs in Saudi. Paramedics must have a high level of accuracy in differentiating between normal ECGs and STEMIs, as this will enhance the early recognition of suspected AMI and, ultimately, improve patient survival. It is also crucially important for paramedics to be able to identify different types of STEMI as this might have an impact following different treatment strategies (such as administration of nitroglycerine with caution in a known right-side infarction or avoid inappropriate STEMI activation for STEMI mimics).
Former studies have examined paramedics’ ability to interpret a 12-lead ECG with STEMI.10,12,13,25–28 These studies showed that paramedics could safely and effectively identify a STEMI in a 12-lead ECG with sensitivity ranging from 75% to 99% and specificity ranging from 53% to 96%. However, most of these studies followed a different method to generate their outcomes (they did not use a survey tool). Furthermore, some of these studies provided pre- and post-training, unlike our study, to paramedics before examining them.12,25
A large previous study following the same method used in this study was conducted on paramedics to measure the diagnostic accuracy for identifying STEMIs. They reported that almost 97% of the participants were able to recognize NSRs. Also, nearly 96% of the participants identified the inferior STEMI correctly. In comparison, 22% and 50% failed to interpret the anterior and lateral STEMIs, respectively.13 In contrast, our study showed that almost one-third of paramedics could successfully recognize NSRs, and 67.1% and 50% could identify inferior and lateral MI, respectively. It is interesting to observe similar findings of lateral MI between these studies.13 However, both STEMIs (inferior and lateral) were successfully identified by only 41% of the participants in our study. Also, our participants’ overall sensitivity and specificity decreased significantly, compared to other studies, to 75% and 53%, respectively, when STEMI mimics and other abnormal ECGs were included.13 In contrast with the results of this study, our overall sensitivity and specificity rates were 58.4% and 29%, respectively. It is plausible that there was a greater experience, larger sample size, and higher exposure to ECGs in the study conducted by Mencl et al,13 which resulted in higher diagnostic accuracy of the paramedics compared to our study.
Moreover, a possible explanation for the low sensitivity in identifying STEMIs might be partially related to the level of experience among paramedics who completed the survey. However, there was no correlation between the years of experience and the correct interpretation of ECGs with STEMI. Despite the low number of interpreted ECGs in our study, compared to previous studies,11,13 paramedics working for SRCA are newly qualified, which might be a result of reform efforts by the Ministry of Health and local health authorities, bringing fresh recruits to the primary prehospital arm in the country and better developing the prehospital arena in Saudi Arabia.29 This might explain the lower levels of experience among paramedics in the city of Riyadh, and perhaps the low level of diagnostic accuracy.
There was no correlation between confidence level in identifying ECGs with STEMIs and correct identification of lateral STEMI (p = 0.1). However, there is little plausible evidence of correlation between paramedics who were confident and the number of correctly identified inferior STEMI (p = 0.02).
Moreover, a previous study noted that there is no correlation or association between the level of participants’ confidence and higher accuracy in interpreting ECGs.11,30 Nevertheless, this is consistent with our findings, which reveal no correlation between the level of confidence and the increased diagnostic accuracy of paramedics in interpreting ECGs.
Furthermore, there was no correlation between the average number of ECGs interpreted per week and the number of correctly interpreted ECGs with STEMI (p = 0.43). However, previous studies have shown that a higher average of ECGs interpreted per week leads to a better accuracy rate. For instance, a study among health-care professionals at the London Health Sciences Centre reported a positive correlation between the increased number of ECG interpretations by health-care providers per week and the accuracy of STEMI diagnosis.31 They defined the threshold of interpreting ECGs per week, which was 20 ECGs, as being linked to enhanced accuracy in interpreting ECGs with STEMI. However, two-third of our participants stated that, on average, they interpreted only one or two ECG cases per week. Consequently, lower exposure to ECGs and fewer years of experience may affect the accuracy rates in interpreting ECGs. Also, a systematic review on the effectiveness of paramedics in interpreting ECGs to recognize STEMI showed that the more opportunities for training and practice a paramedic received, the greater their ability was to accurately identify ECGs with STEMI accurately.32 This emphasizes the importance of training and prior experience interpreting ECGs with STEMI to enhance the accuracy and confidence of paramedics.30 Finally, given the low number of interpreting EGCs for many ALS paramedics, we suggest that they may not rely solely on their ECG interpretation to activate the cardiac catheterization laboratory. Also, the presented results may justify and support the current ACS care pathway in prehospital settings in SRCA, where paramedics and a medical director (an experienced emergency physician) exchange the 12-lead ECG using a secure, two-way online communication method to confirm the presence of STEMI. This online communication method also facilitates pre-arrival notification of the receiving hospital that allow early activation of AMI pathway and early treatment interventions; subsequently leads to favorable patient outcomes. Further research is recommended assess training needs in the context of ECG, a larger sample size on a national scale, and different methodologies to assess the gap of knowledge of paramedics in interpreting a 12-lead ECGs.
Limitations
The diagnostic dilemma lies that misinterpreting ECG with STEMI-mimics will lead to inappropriate catheterization laboratory activation and overburdening the receiving hospital, while misinterpreting ECG with STEMI may impact patient care and increase mortality. Thus, in light of the results, the potential benefit of identifying the presence of STEMI outweigh the risk of misinterpreting the location of infarction or STEMI mimics. This result is clinically significant where early 12-lead ECG interpretation by paramedics is crucial for diagnosis and initiating early activation of the catheterization laboratory.
This study has some limitations, as it is a cross-sectional study that can only suggest association rather than causation. The study, however, is still valuable and can provide the basis for future work. The authors tried to avoid significant limitations found in the literature regarding the number and type of ECGs used to detect the accuracy of paramedics in interpreting STEMIs in 12-lead ECGs. Previous studies assessing the ability of ECG interpretations with STEMI included NSRs and STEMI ECGs without STEMI mimics, which might be easy to identify since there are no STEMI mimics to differentiate and accurately assess paramedics’ diagnostic ability.
While these STEMI mimics are not routinely seen as emergency cases and are treated less often by paramedics (for example, pericarditis, VP, LVH), including them would enhance the ability of paramedics to accurately interpret ECGs.11,30 Therefore, this issue was overcome by adding STEMI mimics, such as LBBB, pericarditis, VP, and LVH, to ensure the best patient outcomes and make the scenarios closer to real-life situations.
Although the sample size in this study is relatively small, the paramedic profession is a growing specialty in Saudi Arabia, with 106 paramedic specialists in Riyadh employed in SRCA. Of those, we had a response rate of 79.2% in our study, with zero rejection, assuming a representative sample of our paramedic group. Therefore, given the small sample size, we are unable to detect any significant correlations. Furthermore, this study was carried out in the only governmental and primary institution that provides prehospital services in Saudi Arabia.
Another limitation is that the type of ECG provided in the survey was limited to one lateral and one inferior STEMI, which might create an incomplete assessment. Other ECGs might have been easier or harder for paramedics to interpret. Subsequently, it might be unrealistic to assume that paramedics are not able to accurately interpret STEMI ECGs solely based on missing two ECGs. Moreover, there is a risk that we may be biased in choosing ECG strips that are hard to interpret. However, we attempted to minimize this limitation by choosing ECG strips from real patients, ones that we reviewed and validated with two external consultant cardiologists who were not part of the study. To overcome the challenges associated with technical issues and time-constrained surveys, we provided illustrative figures as instructions within the survey. Furthermore, the survey should take 16 minutes on average if participants spend the whole 60 seconds on each ECG question; however, based on our pilot study (n = 10 external paramedics), participants took less than 60 seconds to finish each ECG question. This made time fatigue less likely to occur and unburdened the overall time survey.
Conclusion
Paramedics were able to identify STEMI events in prehospital settings with moderate sensitivity and low specificity with limited ability to differentiate between STEMI and STEMI mimics. Therefore, additional training in ECG interpretation could improve their clinical decision-making, and to ensure that proper care and treatment is provided. Further research on a large, representative sample of paramedics across the country could provide more definitive evidence to establish a greater degree of accuracy in detecting STEMI in prehospital settings.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author [MA], upon reasonable request.
Acknowledgments
The authors wish to recognize the efforts of (i) all the paramedics who provide care for the citizens of Riyadh whose interest and enthusiasm made this project possible; (ii) Mr Abdulrahman Bahmaid and Mr Ahmed Aljuraywi, for their help during the study.
Disclosure
All authors have no conflicts of interest to disclose.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
2. World Health Organization. Cardiovascular diseases (cvds) [Online]; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
3. Moscarella E, Brugaletta S, Sabate M. Latest STEMI treatment: a focus on current and upcoming devices. Expert Rev Med Devices. 2018;15(11):807–817. doi:10.1080/17434440.2018.1538778
4. Goodman SG, Menon V, Cannon CP, Steg G, Ohman EM, Harrington RA. Acute ST-segment elevation myocardial infarction: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest. 2008;133(6Suppl):708S–75S. doi:10.1378/chest.08-0665
5. Cannon CP, Sayah AJ, Walls RM. ER TIMI-19: testing the reality of prehospital thrombolysis. J Emerg Med. 2000;19(3Suppl):21S–25S. doi:10.1016/S0736-4679(00)00251-1
6. Bassand J-P, Hamm CW, Ardissino D, et al. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: the task force for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes of the European Society of Cardiology. Eur Heart J. 2007;28(13):1598–1660. doi:10.1093/eurheartj/ehm161
7. Cannon C, Brindis R, Chaitman B, et al.; American College of Cardiology Foundation. American heart association task force on clinical data standards. Circulation. 2013;127(9):1052–1089. doi:10.1161/CIR.0b013e3182831a11
8. Ting HH, Krumholz HM, Bradley EH; Ting HH, Krumholz HM, Bradley EH, Cone DC, Curtis JP, Drew BJ, et al. Implementation and integration of prehospital ECGs into systems of care for acute coronary syndrome: a scientific statement from the American Heart Association Interdisciplinary Council on Quality of Care and Outcomes Research, Emergency Cardiovascular Care Committee, Council on Cardiovascular Nursing, and Council on Clinical Cardiology. Circulation. 2008;118(10):1066–1079. doi:10.1161/CIRCULATIONAHA.108.190402
9. Sejersten M, Young D, Clemmensen P, et al. Comparison of the ability of paramedics with that of cardiologists in diagnosing ST-segment elevation acute myocardial infarction in patients with acute chest pain. Am J Cardiol. 2002;90(9):995–998. doi:10.1016/S0002-9149(02)02685-1
10. Cantor WJ, Hoogeveen P, Robert A, et al. Prehospital diagnosis and triage of ST-elevation myocardial infarction by paramedics without advanced care training. Am Heart J. 2012;164(2):201–206. doi:10.1016/j.ahj.2012.05.009
11. Trivedi K, Schuur JD, Cone DC. Can paramedics read ST-segment elevation myocardial infarction on prehospital 12-lead electrocardiograms? Prehosp Emerg Care. 2009;13(2):207–214. doi:10.1080/10903120802706153
12. Le May MR, Davies RF, Dionne R, et al. Comparison of early mortality of paramedic-diagnosed ST-segment elevation myocardial infarction with immediate transport to a designated primary percutaneous coronary intervention center to that of similar patients transported to the nearest hospital. Am J Cardiol. 2006;98(10):1329–1333. doi:10.1016/j.amjcard.2006.06.019
13. Mencl F, Wilber S, Frey J, Zalewski J, Maiers JF, Bhalla MC. Paramedic ability to recognize ST-segment elevation myocardial infarction on prehospital electrocardiograms. Prehosp Emerg Care. 2013;17(2):203–210. doi:10.3109/10903127.2012.755585
14. Jenkins D, Gerred SJ. ECGs by Example E-Book. Elsevier Health Sciences; 2011.
15. Buttner R, Burns E. Inferior STEMI [Online]; 2021. Available from: https://litfl.com/inferior-stemi-ecg-library.
16. Buttner R, Burns E. Lateral STEMI [Online]; 2021. Available from: https://litfl.com/lateral-stemi-ecg-library/.
17. B26. Left Bundle Branch Block (LBBB) [Online]; 2020. Available from: https://www.stemlynsblog.org/b26-left-bundle-branch-block-lbbb/.
18. ecgmadesimple. ECG 478 [Online]; 2008. Available from: http://www.ecgmadesimple.com/index.php?option=com_content&view=article&id=478&Itemid=416.
19. Gul EE, Boles U, Ali FS, Abdollah H. Loss of atrial pacing in a patient with a dual-chamber permanent pacemaker: what is the mechanism? J Arrhythmia. 2017;33(2):159. doi:10.1016/j.joa.2016.08.002
20. de Bliek EC. ST elevation: differential diagnosis and caveats. A comprehensive review to help distinguish ST elevation myocardial infarction from nonischemic etiologies of ST elevation. Turk J Emerg Med. 2018;18(1):1–10. doi:10.1016/j.tjem.2018.01.008
21. Smith SW. Is this a simple right bundle branch block? [Online]. 2012. Available from: http://hqmeded-ecg.blogspot.com/2012/04/is-this-simple-right-bundle-branch.html.
22. Huitema AA, Alemayehu M, Steiner OL, Bagur R, Lavi S. Improving electrocardiography diagnostic accuracy in emergency medical services personnel. CJC Open. 2019;1(1):28–34. doi:10.1016/j.cjco.2018.11.006
23. MedCalc Software Ltd. Diagnostic test evaluation calculator. Available from: https://www.medcalc.org/calc/diagnostic_test.php.
24. Shapiro SS, Wilk MB. An analysis of variance test for normality (complete samples). Biometrika. 1965;52(3/4):591–611. doi:10.1093/biomet/52.3-4.591
25. Ducas RA, Wassef AW, Jassal DS, et al. To transmit or not to transmit: how good are emergency medical personnel in detecting STEMI in patients with chest pain? CanJ Cardiol. 2012;28(4):432–437. doi:10.1016/j.cjca.2012.04.008
26. Feldman JA, Brinsfield K, Bernard S, White D, Maciejko T. Real-time paramedic compared with blinded physician identification of ST-segment elevation myocardial infarction: results of an observational study. Am J Emerg Med. 2005;23(4):443–448. doi:10.1016/j.ajem.2004.10.011
27. Le May MR, Dionne R, Maloney J, et al. Diagnostic performance and potential clinical impact of advanced care paramedic interpretation of ST-segment elevation myocardial infarction in the field. CJEM. 2006;8(6):401–407. doi:10.1017/S1481803500014196
28. Lee CH, Van Gelder CM, Cone DC. Early cardiac catheterization laboratory activation by paramedics for patients with ST-segment elevation myocardial infarction on prehospital 12-lead electrocardiograms. Prehosp Emerg Care. 2010;14(2):153–158. doi:10.3109/10903120903537213
29. Khattab E, Sabbagh A, Aljerian N, et al. Emergency medicine in Saudi Arabia: a century of progress and a bright vision for the future. Int J Emerg Med. 2019;12(1):16. doi:10.1186/s12245-019-0232-0
30. O’Donnell D, Mancera M, Savory E, Christopher S, Schaffer J, Roumpf S. The availability of prior ECGs improves paramedic accuracy in recognizing ST-segment elevation myocardial infarction. J Electrocardiol. 2015;48(1):93–98. doi:10.1016/j.jelectrocard.2014.09.003
31. Huitema AA, Zhu T, Alemayehu M, Lavi S. Diagnostic accuracy of ST-segment elevation myocardial infarction by various healthcare providers. Int J Cardiol. 2014;177(3):825–829. doi:10.1016/j.ijcard.2014.11.032
32. Funder JL, Ross L, Ryan S. How effective are paramedics at Interpreting ECGs in order to recognize STEMI? A systematic review. Australas J Paramed. 2020;17. doi:10.33151/ajp.17.772
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Integrative Systematic Review of Promoting Patient Safety Within Prehospital Emergency Medical Services by Paramedics: A Role Theory Perspective
Strandås M, Vizcaya-Moreno MF, Ingstad K, Sepp J, Linnik L, Vaismoradi M
Journal of Multidisciplinary Healthcare 2024, 17:1385-1400
Published Date: 26 March 2024