Back to Journals » International Journal of General Medicine » Volume 14
Paradoxical Association Between Intradialytic Blood Pressure Change and Long-Term Mortality with Different Levels of Interdialytic Weight Gain
Authors Yu J, Chen X, Li Y, Wang Y, Liu Z, Shen B, Teng J, Zou J, Ding X
Received 21 October 2020
Accepted for publication 30 December 2020
Published 19 January 2021 Volume 2021:14 Pages 211—220
DOI https://doi.org/10.2147/IJGM.S288038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Jinbo Yu,1– 3 Xiaohong Chen,1– 3 Yang Li,1– 3 Yaqiong Wang,1– 3 Zhonghua Liu,1– 3 Bo Shen,1– 3 Jie Teng,1– 3 Jianzhou Zou,1– 3 Xiaoqiang Ding1– 3
1Division of Nephrology, Zhongshan Hospital, Shanghai Medical College, Fudan University, Shanghai, People’s Republic of China; 2Shanghai Institute of Kidney Disease and Dialysis, Shanghai, People’s Republic of China; 3Shanghai Key Laboratory of Kidney and Blood Purification, Shanghai, People’s Republic of China
Correspondence: Xiaoqiang Ding
Division of Nephrology, Zhongshan Hospital, Shanghai Medical College, Fudan University, Shanghai 200032, People’s Republic of China
Tel +86-2164041990
Email [email protected]
Background: A greater interdialytic weight gain (IDWG) implies a greater ultrafiltration rate, which might lead to hemodynamic instability and intradialytic blood pressure (BP) change in hemodialysis patients. However, current studies have not explicated the impact of IDWG on the association between intradialytic BP changes and prognosis, especially in patients without cardiac dysfunction and diabetes. In this study, we aimed to explore the relationship between absolute intradialytic BP changes and mortality with different IDWG levels.
Methods: A total of 204 hemodialysis patients (without cardiac dysfunction and diabetes) were included in this prospective observation study, with a mean follow-up of 55.32± 20.99 months. Initially, we collected IDWG, IDWG% (percentages according to dry weight), and pre-/post-BPs of 36 consecutive dialysis sessions during three months enrollment. And the average value of them was defined as baseline value. Patients were divided into 3 cohorts according to IDWG% tertiles (< 3.3%, 3.3%– 4.6%, ≥ 4.6%). Comparisons between different tertiles were analyzed.
Results: Compared to the low IDWG% group (tertile 1, T1), patients of high IDWG% group (tertile 3, T3) were younger, had higher ultrafiltration rate, less residual kidney function, lower BMI and dry weight, longer dialysis vintage and higher N terminal pro B type natriuretic peptide levels (P< 0.05). Correlations were found between IDWG% and intradialytic BP changes. Kaplan–Meier analysis and multivariate Cox regression model adjusted for demographic data, dialysis information and predialysis BPs indicated that greater absolute intradialytic BP changes were associated with worse prognosis in T1 group (P< 0.05). While in T3 group, less absolute intradialytic BP changes were associated with higher mortality (P< 0.05).
Conclusion: There is a paradoxical association between absolute intradialytic BP changes and long-term mortality with different IDWG levels. Both BP stability and volume balance are crucial to patients’ prognosis.
Keywords: all-cause mortality, hemodialysis, interdialytic weight gain, intradialytic blood pressure
Introduction
Intradialytic blood pressure (BP) changes over time, related to blood volume changes during hemodialysis (HD). In general, the patient’s BP is highest before dialysis. During dialysis, the blood volume decreases gradually with ultrafiltration, and the BP drops gently. After dialysis, blood volume increases with the retention of water and sodium, and the BP rises successively, until the next dialysis treatment session. Recent studies have shown that intradialytic BP variation could be a prognostic factor. Considerable BP variability was associated with all-cause and cardiovascular mortality.1 A U-shaped association between SBP changes and mortality was found in the previous study.2 So not only BP variability but also BP changes might have prognostic effects on mortality. Interdialytic weight gain (IDWG), corresponding to ultrafiltration losses during dialysis, is mostly influenced by oral fluid intake minus residual urine output (when present) and insensible fluid losses. Several studies have found associations between great IDWG and adverse outcome.3–5 A greater IDWG implies a greater ultrafiltration rate, which might lead to hemodynamic instability and intradialytic BP change.
However, current studies have not explicated the impact of IDWG on the association between intradialytic BP changes and prognosis, especially in patients without cardiac dysfunction and diabetes. Thus, we conducted this study to test the predictive effects of absolute intradialytic BP changes on long-term mortality with diverse IDWG% levels in patients without cardiac dysfunction and diabetes mellitus.
Methods
Patients and Study Design
We prospectively studied the outcome of patients, who started HD before Jan 2013 in the blood purification center, Zhongshan Hospital, Fudan University, Shanghai, China. Inclusion criteria were patients older than 18 and chronic HD for at least three months, undergoing HD three times a week, in a stable condition without cardiac dysfunction and diabetic mellitus. They were followed until Dec 31, 2019. Patients were initially evaluated during three months, determining the IDWG and pre-/post-dialysis BP as an average of the 36 consecutive HD sessions given during that period. IDWG is expressed as the difference between the predialysis weight and the weight at the end of the previous dialysis session, and IDWG% is obtained using the percentage relationship between the average IDWG and the patient’s dry weight. Percentage of IDWG = ([current predialysis weight (kg) – previous postdialysis weight (kg)/target dry weight (kg)]) * 100.6 Dry weight was targeted every month by clinical performance (eg, edema) and serum N terminal pro B type natriuretic peptide (NT-proBNP). Patients were divided according to the tertile levels of IDWG%, which was <3.3% (T1), 3.3%–4.6% (T2), and ≥4.6% (T3) (Figure 1). The study was approved by our institutional clinical research ethics review board (Ethics Committee of Zhongshan Hospital, Fudan University) and was conducted according to the Declaration of Helsinki principles. Each participant signed an informed consent form before entering the study. The primary endpoint was all-cause mortality.
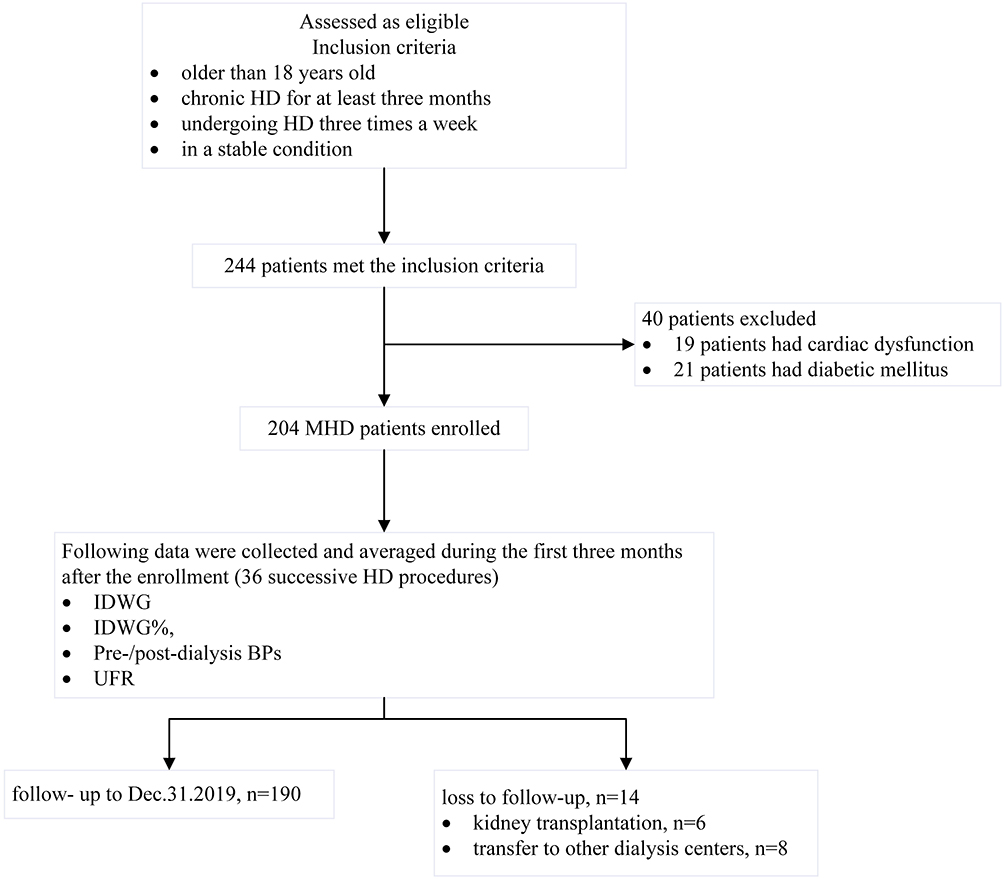 |
Figure 1 Flowchart of the study. |
BP Measurements
Patients received HD three times per week. BP was measured before HD (predialysis) in a sitting position and after HD with the patient in a supine position (post-dialysis) (BP measured just before a detachment of dialysis circuit from the patient).7 Patients had their BP measured per the standard protocol using an automated stand-alone device or one integrated into the HD machine with an appropriately sized pressure cuff around the non-access upper arm positioned at heart level. Well-trained nurses took all the BPs.
During dialysis, BP change was determined by finding the absolute value of post-dialysis BP minus predialysis BP. Mean arterial pressure (MAP) was calculated as MAP = [systolic blood pressure (SBP) + (2 × diastolic blood pressure (DBP))]/3. Pulse pressure (PP) was calculated as PP= SBP ˗ DBP. Intradialytic BP change (ΔBP) was estimated by averaging BP changes of 36 consecutive hemodialysis in the 3-month run-in period.
Patients were divided according to levels of absolute intradialytic BP changes: SBP change >20mmHg and ≤20mmHg, DBP change >10mmHg and ≤10mmHg, MAP change >15mmHg and ≤15mmHg, PP change >10mmHg and ≤10mmHg.2
Date Collection
Patient characteristics (demographics, comorbidity, biochemistry, and medications) were extracted from patient charts by their treating physician at the beginning of the run-in phase and the end of the study.
Biochemical Measurements
Blood sampling was performed during a midweek non-dialysis day. Serum albumin, pre-albumin, hemoglobin, and creatinine were measured using standard methods in the routine clinical laboratory.
Echocardiography
Transthoracic echocardiographic examinations were conducted using a Philips echocardiographic machine (Philips IE33, Eindhoven, the Netherlands) with a 3.5-MHz multiphase array probe by a single experienced cardiologist during a midweek non-dialysis day, within 2 hours after blood sampling, both at the entry and the endpoint of the study. Measurements of the left ventricular internal dimension, interventricular septal thickness, and posterior wall thickness were made at end-diastole according to the recommendations of the Penn Convention. Left ventricular mass was calculated with the Devereux formula. The left ventricular mass index (LVMI) was obtained by dividing left ventricular mass by height in meters rose to the power of 2.7. The left ventricular ejection fraction (EF) was determined by two-dimensional echocardiography.
Statistical Analysis
Continuous variables were expressed as mean ± Standard Deviation or median (interquartile range), while categorical variables were appropriately presented as numbers and percentages. To compare groups of normal variables, we used One-Way ANOVA, whereas for skewed and categorical variables Mann–Whitney U and chi-square test were performed, respectively. Pearson correlation coefficient was calculated to study the relationship between IDWG% and intradialytic BP changes. Survival was calculated with the Kaplan–Meier method and the comparison between groups with the Log rank test. Multivariate cox regression analysis, adjusted for age, gender, BMI, residual kidney function, dialysis vintage and predialysis BPs, was used to test the association between intradialytic BP changes and mortality in different IDWG% groups. Two-sided P < 0.05 was considered significant. All analyses were performed using SPSS version 24 (SPSS Inc., Chicago, IL, USA).
Results
Patient Characteristics and 5-Year Mortality
A total of 204 patients were recruited with a mean follow-up of 55.32±22.99 months. Fourteen (6.9%) were censored during the 6-year observation period because of kidney transplantation (n=6) and transfer to other hemodialysis centers (n=8). During the follow-up, 61 (32.1%) patients died with a mortality rate of 6.4 per 100-person year, including 22 fatal cardiovascular events, 18 cerebrovascular events, 8 deaths attributed to severe infection, 8 to sudden death, and 5 to cancer. The mortality rates for IDWG% tertiles showed no significant difference, which was 36.5% in T1, 30.2% in T2 and 29.7% in T3.
Table 1 summarizes the baseline characteristics of the study cohort. Compared to the low IDWG% group, patients of the high IDWG% group were younger, had higher ultrafiltration rate, less residual kidney function, lower BMI and dry weight, longer dialysis vintage and higher NT-proBNP levels (P<0.05).
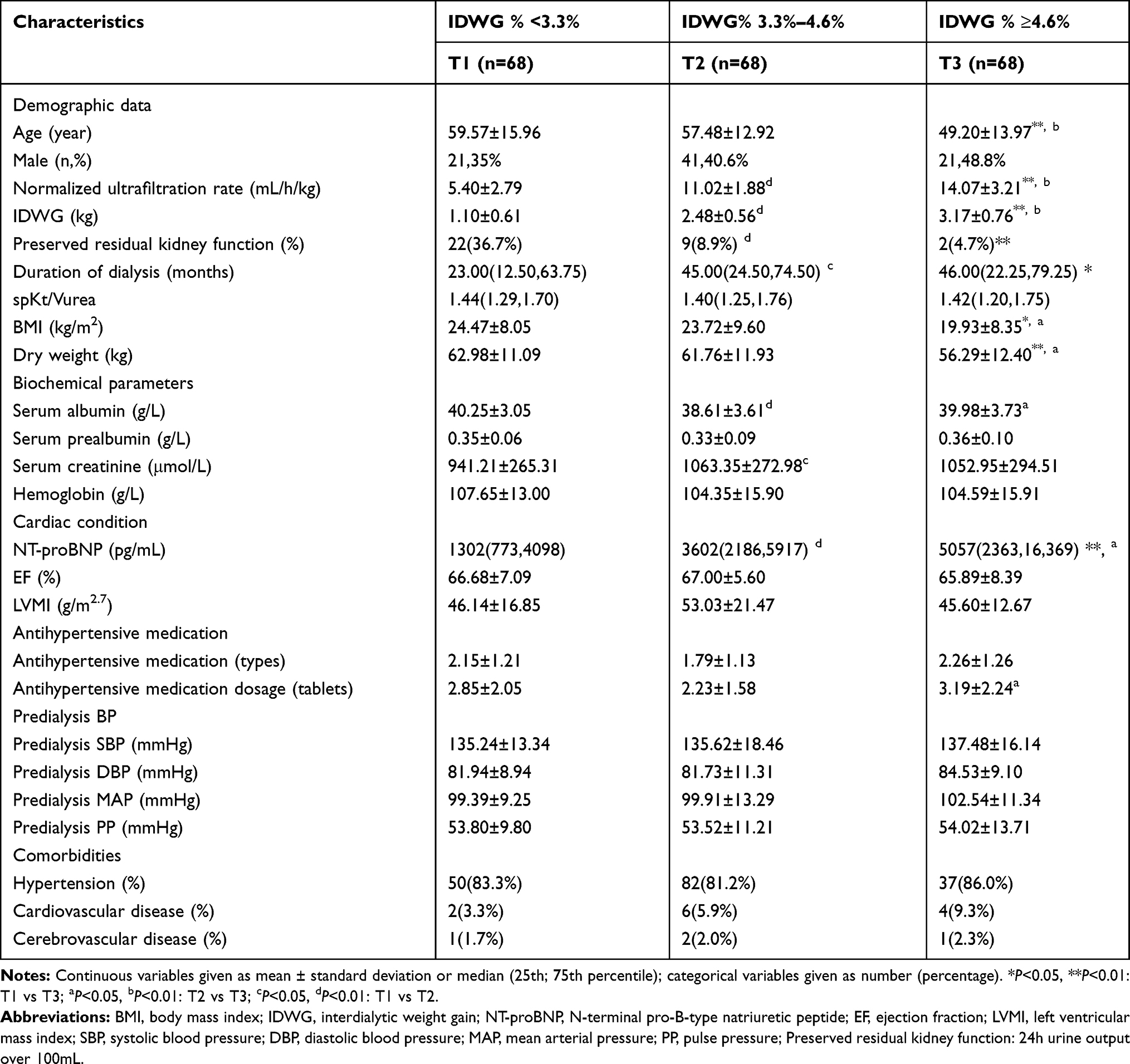 |
Table 1 Demographic, Clinical and Biochemical Data of the Patients |
Relationship Between IDWG% and Intradialytic BP Changes
Predialysis BPs, including SBP, DBP, MAP, PP, showed no significant difference among IDWG% tertiles in our study (Table 1). Instead, significant associations were found between IDWG% and intradialytic SBP changes (r=0.229, P=0.001), DBP changes (r=0.192, P=0.008), MAP changes (r=0.222, P=0.002) and PP changes (r=0.190, P=0.009) (Figure 2).
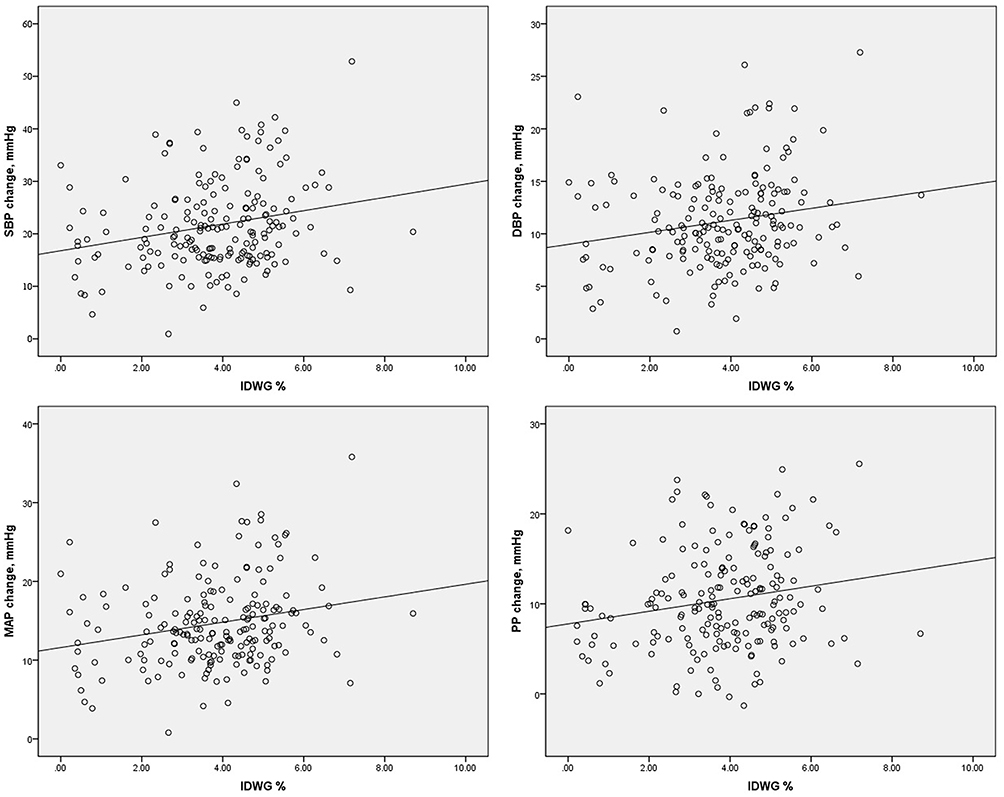 |
Figure 2 Association |
Prognostic Effects of Intradialytic BP Changes with Different IDWG% Groups
We tested the predictive effects of intradialytic BP changes on long-term mortality in different IDWG% tertiles. Kaplan–Meier analysis indicated that intradialytic SBP changes >20mmHg, DBP changes >10mmHg, MAP changes >15mmHg, PP changes >10mmHg were associated with worse prognosis (P=0.042, 0.033, 0.010, 0.013, respectively) in T1 group, while in T3 group, Kaplan–Meier analysis indicated that intradialytic SBP changes >20mmHg, DBP changes >10mmHg, MAP changes >15mmHg, PP changes >10mmHg were associated with better prognosis (P=0.021, 0.012, 0.010, 0.034, respectively). In T2 group, only PP changes >10mmHg was associated with worse prognosis (P=0.035) (Figure 3A–C).
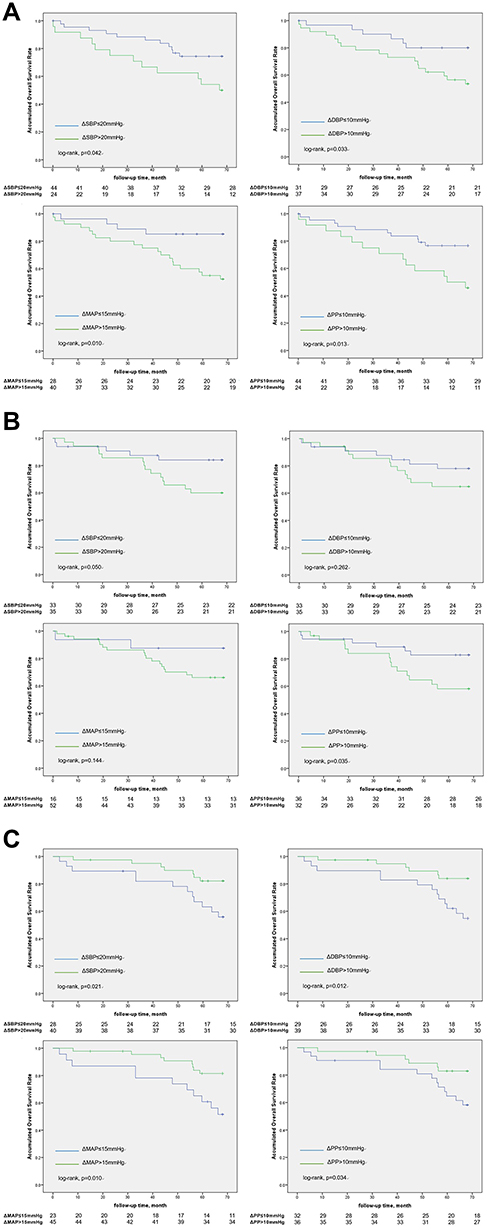 |
Figure 3 (A) Accumulative overall survival rate of different intradialytic blood pressure change in low IDWG% group. (B) Accumulative overall survival rate of different intradialytic blood pressure change in median IDWG% group. (C) Accumulative overall survival rate of different intradialytic blood pressure change in high IDWG% group. |
As the effects of intradialytic BP changes on survival might be affected by predialysis BPs, we constructed multivariate Cox regression models, including predialysis BPs (SBP, DBP, MAP, PP), age, gender, BMI, residual kidney function and dialysis vintage in different IDWG% groups. In T1 group, we found that the multivariate Cox regression model indicated that the adjusted hazard ratio for death was 2.80, 3.00, 3.09, 3.53, as intradialytic SBP changes over 20mmHg, DBP changes over 10mmHg, MAP changes over 15mmHg, PP changes over 10mmHg (P<0.05). While in T3 group, the adjusted hazard ratio for death was 0.25, 0.21, 0.25, 0.25 as intradialytic SBP changes over 20mmHg, DBP changes over 10mmHg, MAP changes over 15mmHg, PP changes over 10mmHg, after adjusting for covariates (P<0.05). No significant prognostic effects were found in intradialytic BP changes on survival in T2 group (Table 2).
 |
Table 2 Cox Regression Analysis of Intradialytic Blood Pressure Changes on Mortality of Different IDWG% Tertiles |
Discussion
Our prospective cohort study with a follow-up period of six years revealed a paradoxical association between intradialytic BP changes and long-term mortality with different levels of IDWG in patients without cardiac dysfunction and diabetes. For low IDWG% patients, greater intradialytic BP changes were associated with worse prognosis, while for high IDWG% patients, less intradialytic BP changes can predict poor outcome.
Predialysis volume overload is the sum of IDWG and residual post-dialysis volume overload. It results mostly from failure to achieve an adequate volume status at the end of the dialysis session.8 In that context, we consider IDWG might reflect predialysis volume overload to some extent. Several studies have found that IDWG was associated with better nutritional status,6,9,10 suggesting a role of greater appetite and higher food and fluid intake. Increasing percentage of IDWG is associated with increases in predialysis BP and BP changes with hemodialysis.6,11 In another study, increased IDWG during the long interdialytic period was associated with minor effects on BP control, as reflected in predialysis BP measurements.12 In our study, we found that predialysis BPs had no significant difference among groups of different IDWG% levels. However, we observed direct associations between IDWG% and intradialytic BP changes. As dialysis treatment time is essentially fixed for most patients, greater IDWG implies a greater fluid removal rate during dialysis (ie, ultrafiltration), which is associated with hemodynamic instability, causing intradialytic BP changes.13,14 This correlation might reflect several compensatory mechanisms that occur in response to fluid accumulation in dialysis patients, including predominant extravascular volume expansion, vaso-relaxation due to suppression of the renin-angiotensin system and neuro-humoral responses, the long-term effect of volume expansion in cardiac function, and the mere presence of diastolic dysfunction.15–17
Great IDWG was associated with increased adverse outcomes and mortality in some observational studies.3–5,18,19 However, there was no significant difference in the mortality of the three IDWG groups in our study. This might be partly due to the small sample size and the definition of the IDWG% group, which was according to IDWG% tertiles. In our study, the high IDWG% group was defined as IDWG % ≥4.6%. In related studies, only the extremes of IDWG (>4.8% of body weight, >5.7% of body weight, and ≥4.0 kg, respectively) were associated with adverse outcomes, and the mortality risk was also relatively small.3–5 Furthermore, results on the association between IDWG and mortality were not adjusted for ultrafiltration rates. As higher ultrafiltration rates have been shown to be associated with a higher mortality risk,20 IDWG might have been associated even less strongly with mortality risk if adjustments for ultrafiltration rates had been performed.
The relationship between BP and prognosis has been controversial. Recent studies have found that great BP change was an independent risk factor for hospitalization, all-cause mortality, and cardiovascular mortality in HD patients.1,2,21–23 The relationship between BP and outcomes is confounded by such factors as day-to-day variations in fluid intake (reflected by IDWG) that are associated with nutritional status and subsequent clinical outcomes.6,10 To explore the relationships between intradialytic BP changes and long-term mortality with different IDWG levels, we divided patients into three groups according to IDWG% tertile levels. For low IDWG% patients, more considerable intradialytic BP changes were associated with worse prognosis, while for high IDWG% patients, less intradialytic BP changes can predict poor outcome.
Great BP changes in the low IDWG% group may reflect a sort of vascular instability due to fluid gain. A person who is not gaining much fluid but whose BP is labile demonstrates a labile or unstable BP compensatory mechanism; this predicts the adverse outcome. Patients with high IDWG% levels had a higher ultrafiltration rate, less residual kidney function and higher NT-proBNP levels in our study. The higher IDWG% calls for a greater ultrafiltration rate and leads to greater intradialytic BP changes subsequently. For those patients, less ultrafiltration led to less BP changes and long-term insufficient ultrafiltration might stand for an unthorough of volume depletion, leading to recessive volume excess. Moreover, IDWG has been regarded as related to non-adherence, and adherence to fluid restriction is necessary to reduce IDWG.3,24 Those patients might not reach their actual “dry weight” after each dialysis session and their predialysis BPs might be higher than the actual state. Thus, less intradialytic BP changes were associated with poor prognosis. On the other hand, patients of high IDWG% were younger than the other two groups, and they might have better compensatory function towards volume fluctuation during dialysis. Suggesting, for the high predialysis volume status patients, whose compensatory ability is tolerable to the great volume fluctuation, patients’ traits are crucial to intradialytic BP regulation. A recent meta-analysis of peridialysis BP levels and risk of all-cause mortality suggested the interpretation of the peridialysis BP mortality associations should be based on the features of the dialysis population.25
Zhang26 suggested that the same predialysis SBP can be associated with either increased or decreased mortality, depending on the direction and degree of peridialytic SBP change. The study revealed that in the presence of lower predialysis SBP, a peridialytic SBP rise is beneficial, while a further peridialytic SBP decline is unfavorable. They found the presence of a predialysis SBP of 130mmHg, and a peridialytic SBP decrease of <30mmHg was not associated with increased mortality, whereas a peridialytic SBP increase was associated with better outcomes. On the other hand, when the predialysis SBP was 110mmHg, a further peridialytic SBP decrease was associated with increased mortality, whereas a peridialytic SBP increase was associated with better outcomes. Thus, the predictive effects of intradialytic BP changes on mortality might be influenced by predialysis BP. We constructed a multivariate Cox model, including predialysis BPs. After adjusting for demographic data, dialysis information and predialysis BPs, a similar paradoxical association still exists in our study.
We hypothesize that the patients with cardiac dysfunction and diabetes mellitus were excluded in our study might be part of the explanation of the results, so our targeted patients might have better BP regulation ability towards intradialytic volume depletion. Our results cannot be interpreted as unlimited great intradialytic BP changes would do good for patients’ outcome. Due to the study sample size, we could not conclude a safe range for intradialytic BP changes. The possibility that BP’s effect on prognosis may have resulted from unrecognized associations between BP and essential covariates. So further research is needed to understand the underlying mechanism.
In this study, we assess the relationship between intradialytic BP changes and mortality with various predialysis volume status in patients without cardiac dysfunction and diabetic mellitus. We testified positive relationships between IDWG% and intradialytic BP changes. Furthermore, we revealed a paradoxical association between intradialytic BP change and long-term mortality with different IDWG levels.
However, our study has several limitations. First was the small sample size. We only tested the degree of intradialytic BP change, not the direction. Second, the study patients were free of cardiac dysfunction and diabetes, so further research might target whether our study’s results could be testified in hemodialysis patients with various comorbidities. Third, we did not evaluate the effect of different vascular accesses on patients’ hemodynamic stability. Last, we did not use objective methods (eg, bio-impedance) to evaluate fluid status, which is more objective and accurate to evaluate volume status.
Conclusion
There is a paradoxical association between intradialytic BP change and long-term mortality with different IDWG levels in patients without cardiac dysfunction and diabetic mellitus. For low IDWG% patients, more considerable intradialytic BP changes were associated with worse prognosis, while for high IDWG% patients, less intradialytic BP changes can predict poor outcome. We should avoid over ultrafiltration for those with low IDWG% and prevent great intradialytic BP changes. In contrast, for those with high IDWG%, apart from patients’ education of controlling IDWG, we should evaluate volume status more frequently, set ultrafiltration rate properly in consideration of cardiac function and other compensatory mechanisms, as well as focus more on intradialytic BP changes to make patients reach “actual” dry weight. So individualized treatments, including both fluid management and BP management, should be taken to achieve hemodynamic stability for patients’ outcomes.
Acknowledgments
The National Natural Science Foundation of China (Grant No.81903969), the Youth Foundation of Zhongshan Hospital (Grant No.2019ZSQN22), Shanghai “science and technology innovation plan” technical standard project (No. 19DZ2205600), Shanghai Municipal Hospital Frontier Technology Project supported by Shanghai ShenKang Hospital Development Center (No. SHDC12018127).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Flythe JE, Inrig JK, Shafi T, et al. Association of intradialytic blood pressure variability with increased all-cause and cardiovascular mortality in patients treated with long-term hemodialysis. Am J Kidney Dis. 2013;61(6):966–974. doi:10.1053/j.ajkd.2012.12.023
2. Chou JA, Elani S, Nguyen DV, et al. Intradialytic hypotension, blood pressure changes and mortality risk in incident hemodialysis patients. Nephrol Dial Transplant. 2018;33:149–159. doi:10.1093/ndt/gfx037
3. Rajiv S, Bragg-Gresham Jennifer L, Rayner HC, et al. Nonadherence in hemodialysis: associations with mortality, hospitalization, and practice patterns in the DOPPS. Kidney Int. 2003;64:254–262. doi:10.1046/j.1523-1755.2003.00064.x
4. Foley RN, Herzog CA, Collins AJ, et al. Blood pressure and long-term mortality in United States hemodialysis patients: USRDS Waves 3 and 4 Study. Kidney Int. 2002;62:1784–1790. doi:10.1046/j.1523-1755.2002.00636.x
5. Kalantar-Zadeh K, Regidor DL, Kovesdy CP, et al. Fluid retention is associated with cardiovascular mortality in patients undergoing long-term hemodialysis. Circulation. 2009;119:671–679. doi:10.1161/CIRCULATIONAHA.108.807362
6. López-Gómez Juan M, Maite V, Rosa J, et al. Interdialytic weight gain as a marker of blood pressure, nutrition, and survival in hemodialysis patients. Kidney Int Supp. 2005;93:S63–68. doi:10.1111/j.1523-1755.2005.09314.x
7. K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis. 2005;45:S1–153.
8. Manfred H, Angelo K, Marlies A, et al. Significance of interdialytic weight gain versus chronic volume overload: consensus opinion. Am J Nephrol. 2013;38:78–90. doi:10.1159/000353104
9. Testa A, Plou A. Clinical determinants of interdialytic weight gain. J Ren Nutr. 2001;11:155–160. doi:10.1053/jren.2001.24362
10. Sezer S, Ozdemir FN, Arat Z, Perim O, Turan M, Haberal M. The association of interdialytic weight gain with nutritional parameters and mortality risk in hemodialysis patients. Ren Fail. 2002;24:37–48. doi:10.1081/JDI-120002659
11. Inrig JK, Patel UD, Gillespie BS, et al. Relationship between interdialytic weight gain and blood pressure among prevalent hemodialysis patients. Am J Kidney Dis. 2007;50:
12. Shantier M, Martin WP, Singh R, et al. Increased weight gain during the long interdialytic period is associated with minor effects on blood pressure control in clinically stable in-centre haemodialysis patients. Nephron. 2019;141(2):87–97. doi:10.1159/000494221
13. Ezio M, Paola G, Roberto Z, et al. Association between high ultrafiltration rates and mortality in uraemic patients on regular haemodialysis. A 5-year prospective observational multicentre study. Nephrol Dial Transplant. 2007;22:3547–3552. doi:10.1093/ndt/gfm466
14. Stefánsson BV, Brunelli SM, Claudia C, et al. Intradialytic hypotension and risk of cardiovascular disease. Clin J Am Soc Nephrol. 2014;9:2124–2132. doi:10.2215/CJN.02680314
15. Stewart GA, Mark PB, Johnston N, et al. Determinants of hypertension and left ventricular function in end stage renal failure: a pilot study using cardiovascular magnetic resonance imaging. Clin Physiol Funct Imaging. 2004;24:387–393. doi:10.1111/j.1475-097X.2004.00583.x
16. Doulton TW, MacGregor GA. Blood pressure in haemodialysis patients: the importance of the relationship between the renin-angiotensin-aldosterone system, salt intake and extracellular volume. J Renin Angiotensin Aldosterone Syst. 2004;5:14–22. doi:10.3317/jraas.2004.001
17. Graziani G, Finazzi S, Mangiarotti R, et al. Different cardiovascular responses to hemodialysis-induced fluid depletion and blood pressure compliance. J Nephrol. 2010;23:55–61.
18. Flythe JE, Curhan GC, Brunelli SM. Disentangling the ultrafiltration rate-mortality association: the respective roles of session length and weight gain. Clin J Am Soc Nephrol. 2013;8:1151–1161. doi:10.2215/CJN.09460912
19. Wong MM, McCullough KP, Bieber BA, et al. Interdialytic weight gain: trends, predictors, and associated outcomes in the international dialysis outcomes and practice patterns study (DOPPS). Am J Kidney Dis. 2017;69:367–379. doi:10.1053/j.ajkd.2016.08.030
20. Flythe JE, Kimmel SE, Brunelli SM. Rapid fluid removal during dialysis is associated with cardiovascular morbidity and mortality. Kidney Int. 2011;79:250–257. doi:10.1038/ki.2010.383
21. Park J, Rhee CM, Sim JJ, et al. A comparative effectiveness research study of the change in blood pressure during hemodialysis treatment and survival. Kidney Int. 2013;84(4):795–802. doi:10.1038/ki.2013.237
22. Lu J, Zhu M, Liu S, et al. The relationship between survival rate and intradialytic blood pressure changes in maintenance hemodialysis patients. Ren Fail. 2017;39(1):417–422. doi:10.1080/0886022X.2017.1305407
23. Stidley CA, Hunt WC, Tentori F, et al. Changing relationship of blood pressure with mortality over time among hemodialysis patients. J Am Soc Nephrol. 2006;17(2):513–520. doi:10.1681/ASN.2004110921
24. Casey J, Johnson V, McClelland P. The relationship between interdialytic weight gain and patient compliance. A single centred cohort study (n=21). EDTNA ERCA J. 2001;27:187–189. doi:10.1111/j.1755-6686.2001.tb00175.x
25. Han YC, Tu Y, Zhou LT, et al. Peridialysis BP levels and risk of all-cause mortality: a dose-response meta-analysis. J Hum Hypertens. 2019;33(1):41–49. doi:10.1038/s41371-018-0103-9
26. Zhang H, Preciado P, Wang Y, et al. Association of all-cause mortality with predialysis systolic blood pressure and its peridialytic change in chronic hemodialysis patients. Nephrol, Dialysis, Transpl. 2020;35. doi:10.1093/ndt/gfaa139.SO059
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.