Back to Journals » Drug, Healthcare and Patient Safety » Volume 18
Paracetamol Overdose in Somali Children Under Five: An Emerging Public Health Concern
Authors Hassan WM ![]()
Received 11 March 2026
Accepted for publication 12 May 2026
Published 16 May 2026 Volume 2026:18 607702
DOI https://doi.org/10.2147/DHPS.S607702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemalkumar B Mehta
Widad Mohamed Hassan
Department of Internal Medicine, Dr Sumait Hospital, SIMAD University, Mogadishu, Somalia
Correspondence: Widad Mohamed Hassan, Email [email protected]
Abstract: Paracetamol (acetaminophen) is widely used for pain and fever management in children under five; however, accidental overdose is an increasing public health concern in low-resource settings such as Somalia. This narrative review highlights key risk factors, clinical consequences, and prevention strategies relevant to the Somali context based on published literature. Misconceptions about dosing, reliance on age rather than weight, and unrestricted access contribute to inappropriate administration and increased risk of hepatotoxicity and acute liver failure. While metabolic pathways in young children differ from adults, increased vulnerability in this setting is more strongly associated with malnutrition, dosing errors, and delayed access to healthcare. Toxicity results from accumulation of N-acetyl-p-benzoquinone imine (NAPQI), leading to oxidative stress and liver injury. Early treatment with N-acetylcysteine (NAC) is essential, yet delayed presentation and limited availability of antidotes in Somalia worsen outcomes. There is currently limited published data on the incidence of paracetamol overdose and NAC availability in Somalia. Strengthening caregiver education, pharmacy-based counseling, access to essential antidotes, and national poison surveillance systems is critical to reducing preventable pediatric liver injury in Somalia.
Keywords: paracetamol, pediatric overdose, hepatotoxicity, Somalia, public health, N-acetylcysteine
Introduction
Paracetamol (acetaminophen) is among the most commonly used medications to treat pain and fever in young children,1,2 its effectiveness, safety, and over-the-counter availability have made it a first-line treatment for pediatric febrile illnesses globally. However, despite its widespread use, children under five are particularly vulnerable to accidental overdose, which can result in hepatotoxicity and, in severe cases, acute liver failure.1,3
Globally, paracetamol overdose is one of the leading causes of drug-induced liver injury in children, highlighting the need for careful dosing and early recognition of toxicity.3,4
Recent reports continue to highlight the ongoing clinical burden of accidental paracetamol overdose in children, including medication-related dosing errors in healthcare settings.5
Although Somalia-specific epidemiological data are limited, medication poisoning and paracetamol overdose are increasingly recognized as important causes of pediatric toxicity in low-resource settings and across sub-Saharan Africa.
In low-resource settings like Somalia, unrestricted access to paracetamol, limited caregiver knowledge regarding weight-based dosing, and socioeconomic constraints contribute to a higher risk of pediatric overdose.2,5 Caregivers may administer paracetamol at shorter-than-recommended intervals or unintentionally use multiple formulations containing paracetamol, increasing the risk of toxicity.4,5
Commentary Methods Approach
This manuscript is a narrative review. Relevant literature was identified through searches of PubMed and Google Scholar using keywords including “paracetamol overdose,” “acetaminophen toxicity,” “pediatric poisoning,” and “low-resource settings.” Articles were selected based on relevance to pediatric populations and applicability to resource-limited contexts, including Somalia. Additional references were identified from cited literature.
Paracetamol Use and Self-Medication in Somali Children
Paracetamol is widely administered at home for fever, colds, and pain in children under five.5 Caregivers often lack awareness of safe dosing intervals and may give the drug multiple times within a short period, at inappropriate or overly frequent dosing intervals, under the misconception that frequent administration accelerates recovery.2,4,5 Miscalculation of doses based on age rather than weight, use of multiple formulations, and overlapping administration of combination products further increase the risk of overdose.5,6 In addition, the absence of standardized pediatric labeling and insufficient pharmacy counseling exacerbate the problem, leaving caregivers without clear guidance on safe administration.6,7 This combination of factors contributes to repeated exposure to hepatotoxic doses in vulnerable children.
Pharmacology and Clinical Consequences
Paracetamol is metabolized primarily in the liver through glucuronidation and sulfation pathways. A small proportion is converted to the highly reactive metabolite N-acetyl-p-benzoquinone imine (NAPQI), which is detoxified by glutathione under normal circumstances.2,3 In cases of overdose, these detoxification pathways become overwhelmed, leading to the accumulation of NAPQI, oxidative stress, hepatocellular injury, and potentially fulminant hepatic failure.2,3,8
Although paracetamol metabolism differs between young children and adults, increased vulnerability in this setting is more strongly associated with malnutrition, dosing errors, and delayed access to healthcare rather than intrinsic immaturity of liver enzymes alone.5,7 Early administration of N-acetylcysteine (NAC) is critical to prevent progression to liver failure; however, delayed healthcare presentation, which is common among children in Somalia because of geographical barriers, delayed healthcare access, and transportation challenges, and reliance on traditional remedies, significantly increases the risk of severe outcomes.4,7,8
Recent pediatric emergency department studies continue to demonstrate that paracetamol overdose remains a significant cause of poisoning-related hospital presentations in children.9
Clinical Algorithm for Suspected Paracetamol Overdose in Children
- Suspected or Confirmed Ingestion
- → Obtain history of ingestion (dose, timing, formulation)
- Assess Time Since Ingestion
- → Determine whether timing is known or unknown
- At ≥4 Hours Post-Ingestion
- → Measure serum paracetamol concentration (if available)
- Risk Assessment
- → Plot level on the Rumack–Matthew nomogram (if available)
- Treatment Decision
- If above treatment line, unknown timing, or high-risk ingestion:
- Initiate N-acetylcysteine (NAC) immediately
- Monitoring
- Assess liver function tests (ALT, AST, INR)
- Monitor clinical status
- Ongoing Management
- Complete full NAC protocol according to hospital guidelines
- Refer severe cases to higher-level care if necessary
Recommended weight-based dosing guidelines for paracetamol in children are presented in (Table 1).
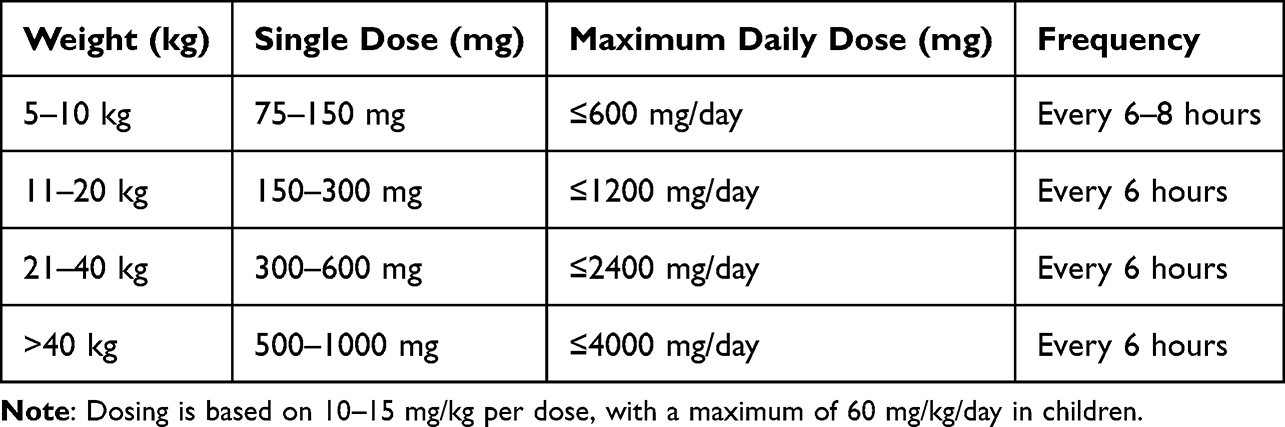 |
Table 1 Recommended Paracetamol Dosing in Children (Weight-Based) |
Health System Challenges in Somalia
The management of pediatric drug poisoning in Somalia faces substantial healthcare system limitations. There is currently no national poison control center or dedicated pediatric toxicology infrastructure, limiting early recognition, reporting, and coordinated management of paracetamol toxicity.4,8 In addition, systematic national surveillance data on pediatric drug poisoning remain unavailable, making it difficult to estimate the true burden of disease and develop targeted prevention strategies.10
Access to essential antidotes such as N-acetyl cysteine (NAC) is inconsistent, particularly in rural and resource-limited areas.4,10 Healthcare access may also be delayed by geographical barriers, transportation difficulties, financial constraints, and reliance on traditional remedies before hospital presentation.5,7
Pharmacy regulation and caregiver counseling practices are inconsistent, and many caregivers may not receive clear instructions regarding appropriate pediatric dosing intervals or weight-based dosing.6,7 Limited public awareness and the absence of standardized pediatric dosing tools further increase the risk of unintentional overdose.5,6
These gaps highlight the urgent need for improved public education, strengthened pharmacy oversight, better access to essential antidotes, and the development of national poison surveillance systems in Somalia.
The key risk factors and corresponding preventive strategies relevant to the Somali context are summarized in (Table 2).
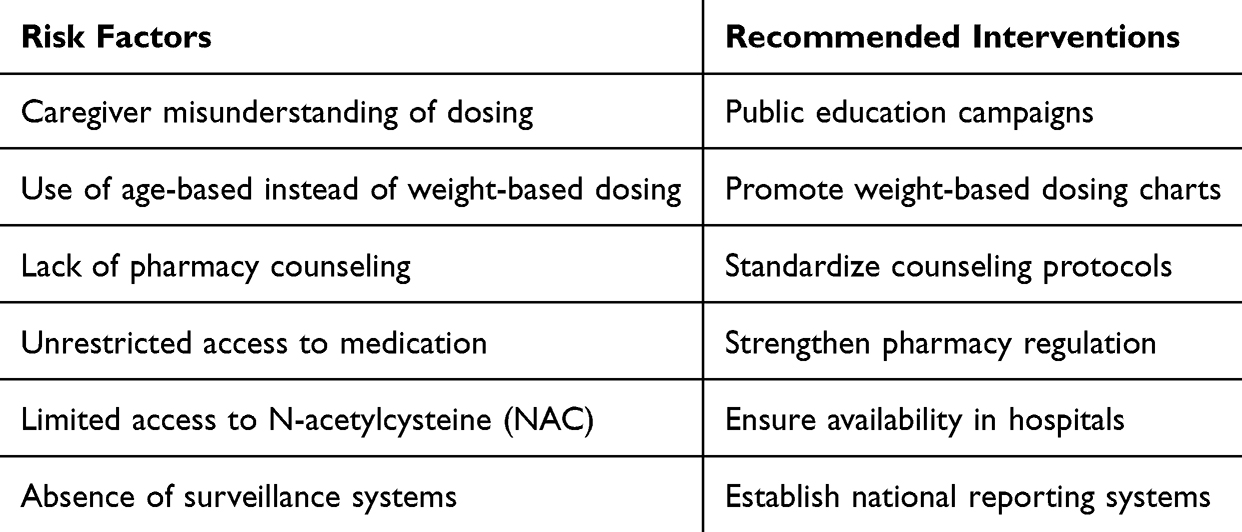 |
Table 2 Risk Factors and Recommended Interventions for Pediatric Paracetamol Overdose in Somalia |
Opportunities for Prevention and Policy Action
Effective strategies to reduce paracetamol-related harm in children under five require interventions at multiple levels. First, caregiver education is critical, including public campaigns on safe pediatric dosing, correct measurement of syrup, and recognition of overdose signs.5,10 Second, pharmacy oversight should be strengthened through standardized labeling, enforcement of counseling protocols, and regulation of over-the-counter pediatric paracetamol sales.5,6
Third, clinical preparedness can be improved by ensuring the availability of NAC, providing weight-based dosing charts, and establishing pediatric poison management protocols in hospitals.4 Recent international epidemiological studies have shown that pediatric paracetamol overdose remains an important public health concern in both high- and low-resource healthcare settings.11 Finally, systematic data collection through surveillance of pediatric drug toxicity is necessary to inform evidence-based policy and preventive measures.12
Coordinated action across these domains can reduce preventable liver injury and associated morbidity and mortality in Somali children.
Limitations
This commentary has several limitations. First, published Somalia-specific epidemiological data on pediatric paracetamol overdose remain extremely limited, restricting accurate estimation of disease burden and clinical outcomes. Second, as a narrative review, this manuscript does not present original clinical or population-based data. Third, some of the evidence discussed was derived from studies conducted in other low-resource and international settings, which may not fully reflect the healthcare context in Somalia. Nevertheless, the available literature highlights important gaps in caregiver awareness, poison surveillance, and pediatric toxicology infrastructure that warrant further research and public health attention in Somalia.
Conclusion
Paracetamol remains an essential medication for managing fever and pain in children; however, in Somalia, its misuse among children under five represents a growing public health concern. Addressing this issue requires prioritizing practical and scalable interventions, particularly strengthening caregiver education and pharmacy-based counseling on safe dosing practices. Improving access to essential treatments such as N-acetylcysteine and establishing basic surveillance systems are also critical steps. Targeted, context-specific strategies are urgently needed to reduce preventable liver injury and improve child health outcomes in Somalia.
Acknowledgments
We are pleased to declare that this research was generously funded by SIMAD University. The author would like to express sincere gratitude for encouragement and support for the Center of Research and Development, SIMAD University.
Disclosure
The author declares no conflicts of interest in this work.
References
1. Graham GG, Scott KF. Mechanism of action of paracetamol. Am J Ther. 2005;12(1):46–4. doi:10.1097/00045391-200501000-00008
2. Prescott LF. Paracetamol: past, present, and future. Am J Ther. 2000;7(2):143–147. doi:10.1097/00045391-200007020-00008
3. Larson AM, Polson J, Fontana RJ, et al. Acetaminophen-induced acute liver failure: results of a United States multicenter study. Hepatology. 2005;42(6):1364–1372. doi:10.1002/hep.20948
4. Rumack BH. Acetaminophen hepatotoxicity: the first 35 years. J Toxicol Clin Toxicol. 2004;42(1):3–20. doi:10.1081/clt-120028749
5. Rumack BH. Management of Acetaminophen overdose: 2018 update. Toxicol Rev. 2018;37(1):1–12. doi:10.1007/s40264-018-0642-4
6. Whitcomb DC, Block GD. Clinical pharmacology of Acetaminophen. Gastroenterology. 1994;106(4):1017–1036. doi:10.1016/0016-5085(94)90728-5
7. Ostapowicz G, Fontana RJ, Schiødt FV, et al. Results of a prospective multicenter study of acute liver failure. Hepatology. 2002;35(5):1189–1200. doi:10.1053/jhep.2002.33162
8. Graham GG, Scott KF. Pharmacokinetics and safety of paracetamol in children. Paediatr Drugs. 2005;7(4):225–233. doi:10.2165/00148581-200507040-00002
9. Prescott LF. Paracetamol and the liver. Paediatr Drugs. 2000;2(2):91–98. doi:10.2165/00128072-200002020-00002
10. Ozcan AS, Ozturk B, Akkaya B, et al. Evaluation of paracetamol overdoses in the pediatric emergency department. Turk Arch Pediatr. 2025;60(6):670–675.
11. Tse Y. Accidental intravenous paracetamol overdoses in children. Arch Dis Child. 2024;109:526–527. doi:10.1136/archdischild-2023-326123
12. Kempf ON, Helt TW, Johansen KB, et al. Paracetamol overdose in Danish children and adolescents during COVID-19 restrictions. Dan Med J. 2024;71(5):A08230494.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diphtheria Outbreak in Somalia: An Alarming Public Health Crisis, Challenges, and Solutions
Siad AS, Yusuf AM, Warsame MO, Nor MA, Abshir SN, Mohammed AI
Infection and Drug Resistance 2026, 19:563822
Published Date: 12 February 2026