Back to Journals » Journal of Pain Research » Volume 18
Pain Relief During Cystoscopic Ureteral Stent Extraction by Transcutaneous Electrical Acupoint Stimulation: A Double-Blinded, Randomized, Controlled Trial
Authors Chen Q, Lian H, Wang J, Chen L, Shi R, Qian M ![]()
Received 22 September 2025
Accepted for publication 20 December 2025
Published 30 December 2025 Volume 2025:18 Pages 7261—7273
DOI https://doi.org/10.2147/JPR.S569374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rushna Ali
Qiaoling Chen,1,* Huidan Lian,2,* Junlu Wang,2,* Lili Chen,3 Ruolin Shi,4 Meizi Qian2
1Operating Room, Pingyang Hospital Affiliated to Wenzhou Medical University, Pingyang County, Wenzhou, Zhejiang, 325400, People’s Republic of China; 2Department of Anesthesia, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China; 3Department of Nursing, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China; 4Operating Room, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruolin Shi, Operating Room, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China, Email [email protected] Meizi Qian, Department of Anesthesia, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China, Email [email protected]
Background: Acupuncture has pain-relief effects, but no data are available on transcutaneous electrical acupoint stimulation (TEAS) for pain relief during transurethral removal of ureteral stents. This study aimed to evaluate the efficacy of TEAS in reducing pain during cystoscopic ureteral stent extraction.
Methods: This prospective, double-blinded, randomized controlled trial enrolled 122 patients scheduled for cystoscopic ureteral stent removal between June 2023 and March 2024. Participants were randomized into three groups: TEAS at Hegu (LI4) and Neiguan (PC6) (Group A, n=37), TEAS at Sanyinjiao (SP6) and Zusanli (ST36) (Group B, n=38), and sham TEAS (Group C, n=47). TEAS or sham TEAS were administered 30 minutes before the procedure. The primary endpoint was pain measured by visual analog scale (VAS) at stent removal (T2). Secondary endpoints included VAS at cystoscope insertion (T1) and 10 minutes post-procedure (T3), along with hemodynamic parameters.
Results: Baseline characteristics were comparable (p > 0.05). Both TEAS groups showed significantly lower VAS scores during stent removal (T2: median 0.00 [IQR: 0.00– 2.50] for Group A and median 0.00 [IQR0.00– 2.50] for group B vs 0.00 [IQR: 2.00– 5.00] for Group C; p = 0.027) and at 10 minutes post-procedure (T3: median 0.00 [IQR: 0.00– 0.00] for Group A and median 0.00 [IQR0.00– 1.00] for group B vs 0.00 [IQR: 0.00– 2.00] for Group C; p = 0.012). Repeated measures ANOVA with gender and age group as covariates revealed a significant Time × Gender interaction (F = 7.044, p = 0.006), indicating different temporal patterns of pain reduction between males and females. However, no significant interaction was found involving the Age Group factor or the three-way interaction with the treatment groups. No significant hemodynamic differences were observed. One patient in Group C withdrew due to severe pain.
Conclusion: TEAS effectively reduces procedural and post-procedural pain during cystoscopic ureteral stent extraction without affecting hemodynamic stability. Notably, the analgesic effect of TEAS demonstrated gender-specific temporal patterns (Time × Gender interaction, p = 0.006), being more pronounced in female patients, while remaining consistently effective across all age groups. These findings support TEAS as a valuable non-pharmacological analgesic adjunct in outpatient urological procedures, though further multicenter and heterogeneous population studies are warranted to validate its generalizability.
Keywords: transcutaneous electrical acupoint stimulation, TEAS, cystoscopic ureteral stent extraction, randomized controlled trial, pain management
Introduction
In urological practice, ureteral stents are inserted to maintain ureteral luminal patency, to protect ureteral anastomosis or graft, and to repair minor ureteric injuries.1 Cystoscopic ureteral stent removal is commonly conducted as a day-case procedure in an outpatient surgical unit with local analgesics (2% lidocaine gel, 5mL) administered as a urethral meatal block.2 While efficient, this approach is associated with significant pain and anxiety for many patients, reported prevalence of pain is remarkably high, with one systematic review indicating it occurs in up to 32% of patients3 and other studies noting that over 50% may report moderate-to-severe pain,4 thereby highlighting the need for adjunctive non-pharmacological analgesic methods.5
Acupuncture, a treatment dating back at least 2500 years in China, has been reported useful in perioperative anesthesia and postoperative analgesia.6,7 Transcutaneous electrical acupoint stimulation (TEAS) enhances reproducibility and eliminates invasiveness compared to manual needling, while alleviating preoperative anxiety and postoperative pain.8,9
Although evidence for TEAS specifically in ureteral stent extraction is scarce, its efficacy has been demonstrated in other urological and surgical settings, showing reductions in intra-operative analgesic consumption and postoperative pain.10,11 The acupoints Hegu (LI4), Neiguan (PC6), Sanyinjiao (SP6), and Zusanli (ST36) were selected based on Traditional Chinese Medicine principles for pain relief and viscera regulation,12 and their combination at 2/100 Hz is supported by neurophysiological research for activating both central opioid and non-opioid pathways to produce broad-spectrum analgesia.13,14 Thus, we hypothesized that TEAS at LI4 combined with PC6, SP6 combined ST3 could alleviate pain during cystoscopic ureteral stent removal, providing a non-invasive analgesic alternative.
Materials and Methods
Trial Design and Patients
Our clinical trial was approved by the Institutional Review Board of the First Affiliated Hospital of Wenzhou Medical University (IRB00001052-13,003)(2022)-No.(199–01), which conforms to the provisions of the Declaration of Helsinki (as revised in Tokyo 2004). Written informed consent was obtained from all subjects. The trial was registered prior to patient enrollment at the Chinese Clinical Trial Registry (ChiCTR2300072451).
This was a prospective, single-center, double-blinded, randomized controlled clinical trial conducted in ethnic Chinese who undergoing Cystoscopic ureteral stent removal at The First Affiliated Hospital of Wenzhou Medical University. The study was completed between June 2023 to March 2024. Information regarding the study was provided to all patients. Due to the need for stimulation adjustment and visible muscle responses, the acupuncturists were not blinded, which is a common limitation in TEAS trials.
Inclusion criteria include the following:
- Aged 18–80 years;
- American Society of Anesthesiologists (ASA) classification levels I–III;
- Those undergoing cystoscopic ureteral stent removal and participate in the study voluntarily and signing informed consent.
Exclusion criteria include the following:15
- Local skin infection at the acupoints above;
- Upper limb or lower limb nerve damage;
- Participating in other clinical studies within the past 4 weeks;
- Inability to understand the visual analog scale (VAS) score;
- Application to a pacemaker, any device to assist the heart or lungs, Holter monitoring, or any implanted device sensitive to microwaves;
- Gravida, puerperant and patients with positive urine pregnancy tests;
- Combined with preoperative pain, using central analgesic drugs, addicted to or dependent on opioids;
- Considered not suitable for this study.
Figure 1 shows the trial flow chart for the patient screening, treatment allocation, intervention, outcomes assessment and data analysis.
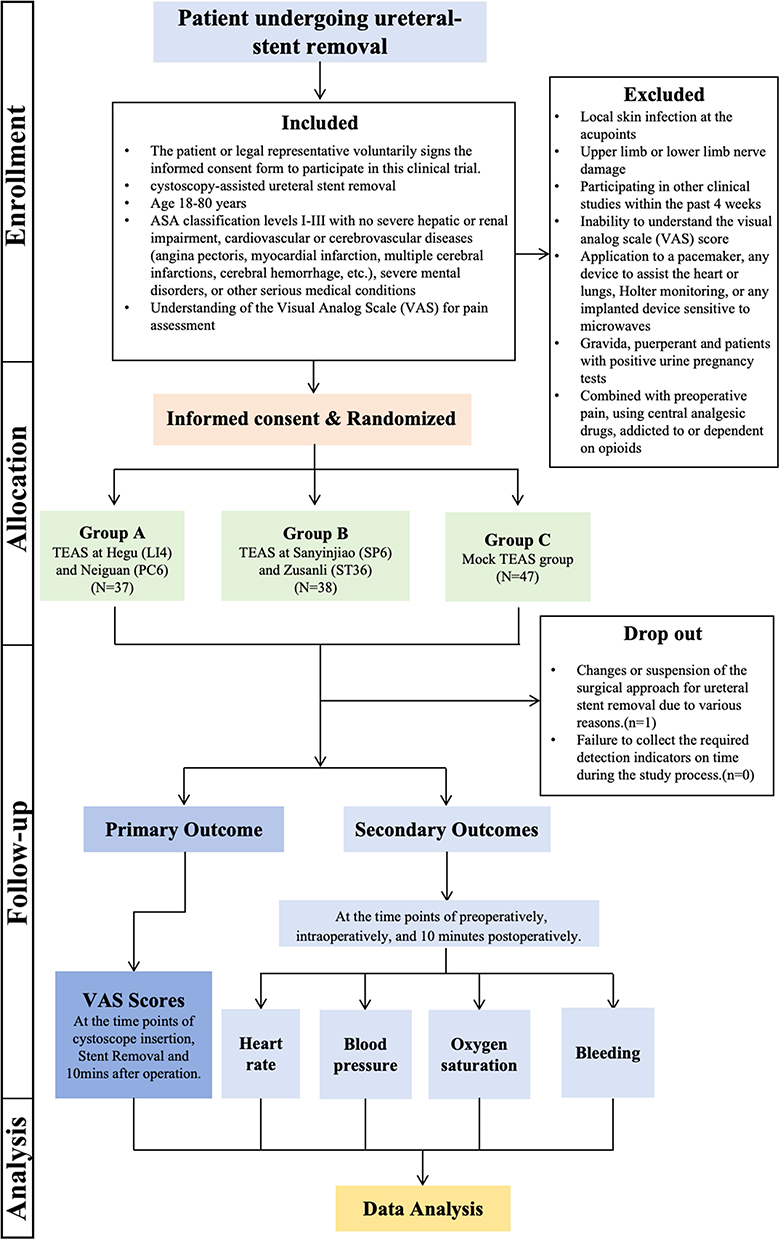 |
Figure 1 Flowchart of the trial This diagram illustrates the enrollment, allocation, intervention, and analysis process of the study. Patients scheduled for cystoscopic ureteral stent removal were assessed for eligibility. Those who met inclusion criteria were randomized into three groups: Group A (TEAS at LI4 and PC6), Group B (TEAS at SP6 and ST36), and Group C (sham TEAS). One patient in Group C was excluded due to intolerable pain requiring general anesthesia. Primary and secondary outcomes were assessed as scheduled. |
Randomized and Mask
Participants were randomly assigned (in a 1:1:1 ratio) into three groups to receive either TEAS on Hegu (LI4) and Neiguan (PC6) acupoints (Group A), TEAS on Sanyinjiao (SP6) and Zusanli (ST36) acupoints (Group B) or sham TEAS (Group C), with the help of a computer-generated table of random numbers by an independent statistician. The independent statistician created identical sealed envelopes before surgery containing three different groups. The acupuncturist opened the envelope and performed TEAS. Patients undergoing Cystoscopic ureteral stent removal and the physician who evaluated the levels of pain and recorded hemodynamic values were blinded to grouping. The evaluation was performed by one physician who received unified training. Due to the need for real-time adjustment of stimulation intensity and the visible muscle responses in active TEAS groups, the acupuncturists could not be blinded. However, the patients undergoing the procedure and the physician who evaluated all outcomes were fully blinded to the group assignments.
Cystoscopic Ureteral Stent Removal
Cystoscopic ureteral stent removal was performed under local anesthesia (2% lidocaine gel, 5mL) with the patient in the lithotomy position. A rigid cystoscope was introduced into the bladder, and the distal end of the stent was identified and grasped using forceps. The stent was gently withdrawn under direct visualization, and the bladder and ureteral orifices were re-examined to ensure complete removal. The procedure was completed without complications, and the patient was discharged home on the same day after meeting standard postoperative criteria.
Intervention
According to the theory of traditional Chinese medicine,12 acupoints Hegu (LI4) and Neiguan (PC6), Sanyinjiao (SP6) and Zusanli (ST36) were selected as the potential analgesic acupoints. For subjects allocated to the TEAS treatment group, TEAS (HANS-200A; Nanjing Jisheng Medical Technology Company, Nanjing, China) was administered 30 min before Cystoscopic ureteral stent removal procedure.
LI4 (Hegu at the dorsum of both hands between the thumb and index figure), PC6 (Neiguan at the palmar side of the forearm, 2 cun above the rasceta, between the palmaris longus tendon palmar tendon and the flexor carpi radialis muscle tendon), SP6 (Sanyinjiao at the tibial aspect of the leg, posterior to the medial border of the tibia, 3 cun superior to the prominence of the medial malleolus), ST36 (Zusanli at the lateral side of the lower leg, on the line of Dubi and Jiexi, 3 cun below Dubi and one finger width lateral to the anterior border of the tibia),15,16 received self-adhesive cutaneous electrode pads of 4×4 cm (Shown in Figure 2). The “cun” in traditional Chinese medicine generally refers to “the same body size”. The distance between the radial ends of the first and second transverse patterns of the patient’s middle finger is “1 inch”. Four fingers, excluding the thumb, are placed side by side and generally refer to “3 cun”. The TEAS was administered using a HANS-200A device at a dense-disperse frequency of 2/100 Hz, alternating every 3 seconds, with a symmetric biphasic waveform. TEAS was applied bilaterally. The stimulation intensity was individually titrated to a strong but comfortable level, defined as the maximum tolerance threshold for each patient, which typically elicited visible muscle twitching without causing pain. The current was initiated at 0 mA and gradually increased in 1–2 mA increments until the target sensation was achieved. The mean stimulation intensity administered across the active TEAS groups was 12.6 ± 2.4 mA (range: 8–18 mA). The average duration of a typical operation was approximately 5 min.
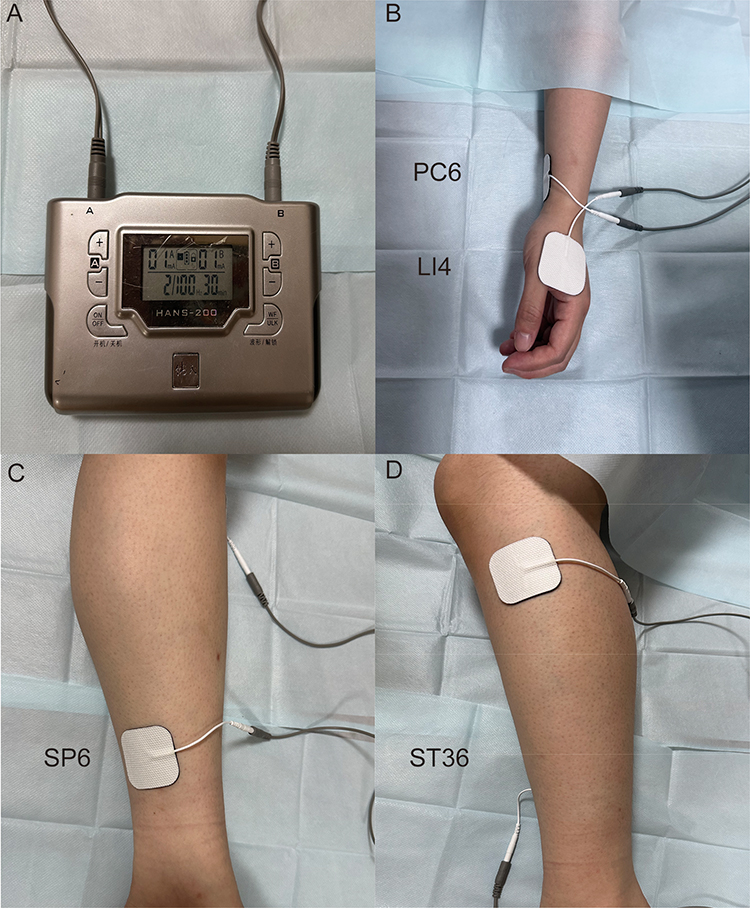 |
Figure 2 Acupoints selected in this trial (A) Transcutaneous acupoint electrical stimulation instrument (HANS200A) (B) Hegu (LI4) and Neiguan (PC6); (C) Sanyinjiao (SP6); (D) Zusanli (ST36). |
For patients in the sham TEAS group, electrodes were attached to the same acupoints (LI4, PC6, SP6, ST36). The electrodes were connected to the HANS-200A device, which was turned on to display active output settings; however, the device was internally modified to deliver no electrical current, ensuring patients received no active stimulation while experiencing the same visual and auditory cues as the active groups.
Heart rate, mean arterial pressure and peripheral oxygen saturation were measured at the timepoints on the cystoscopic insertion, the removal of the stent and the 10 mins within the end of the procedure, respectively. One patient, which was not included in the final statistical population, was unable to tolerate the procedure due to severe pain, then the procedure was rescheduled and successfully completed in the main operating room under general anesthesia.
Endpoints
The primary endpoint was the visual analog scale (VAS) for pain at the timepoint of stent removal. The secondary endpoints were the VAS for pain at the timepoint of the Cystoscope Insertion and the VAS within 10min after procedure finished. The heart rate, blood pressure and peripheral oxygen saturation were also recorded.
Adverse Events
Adverse events (AEs) were followed by the investigators until 1 hour later after the procedure. Any adverse events, such as skin irritation, dizziness, or discomfort at the stimulation site, were to be immediately recorded and managed. The stimulation would be adjusted or terminated if any intolerable side effect occurred. Throughout the study period, patients were closely monitored for such events during the 30-minute TEAS session and for one-hour post-procedure. We report that no such TEAS-related adverse events were observed in our cohort, underscoring the safety of the intervention in this setting.
Sample Size
The sample size was calculated a priori using G*Power software (version 3.1.9.7). The calculation was based on the primary outcome of pain incidence during cystoscopic ureteral stent extraction. A previous systematic review reported a pain prevalence of 31% during this procedure.17 We hypothesized that TEAS could achieve a clinically significant reduction, corresponding to an absolute risk reduction of 20% (ie, reducing the pain incidence from 31% to 11% in the active groups). This translates to an effect size (Cohen’s w) of approximately 0.26. For a Chi-square test (aiming to detect this difference among three groups), with an α error of 0.05 and a desired power (1-β) of 80%, a total sample size of 93 (31 per group) was required. Anticipating a potential dropout rate of 20%, we aimed to enroll a total of 111 patients. Ultimately, 122 patients were recruited, which exceeds the minimum required sample size and further strengthens the study’s power.
Statistical Analysis
Data were analyzed using SPSS 19.0 (IBM, Armonk, NY, USA). Continuous data were tested for normal distribution using the Shapiro–Wilk test. Normally distributed continuous variables are presented as means ± standard deviation and were analyzed using the one way-ANOVA. Continuous data with a skewed distribution were presented as medians (range) and were analyzed using the Kruskal–Wallis one way ANOVA or Mann–Whitney U-test, and the Bonferroni correction was used to adjust the p value for multiple comparisons. Categorical data were presented as frequencies and were analyzed using the Chi-square test. The p values <0.05 were considered statistically significant. To investigate the potential influence of gender and age on the primary pain outcome, a repeated-measures analysis of variance (ANOVA) was performed with VAS scores across time points (T1, T2, T3) as the within-subjects factor, and Group (A, B, C), Gender, and Age Group (young: ≤45 years; middle: 45–65 years; old: ≥65 years) as between-subjects factors. Mauchly’s test was used to assess sphericity, and the Greenhouse-Geisser correction was applied when the assumption was violated. The primary interactions of interest were Time × Gender and Time × Age Group. Partial eta squared (η2) was reported as the measure of effect size for significant effects.
Results
Patients
A total of 122 subjects were recruited between June 2023 to March 2024. Subjects were randomized, and 122 subjects were analyzed, including Group A (TEAS on LI4 and PC6, n=37), Group B (TEAS on SP6 and ST36, n=38), and Group C (sham TEAS, n=47). All patients were followed up 1 hour after procedure. As shown in Table 1, there were no significant intergroup differences in age, gender, body mass index (BMI), blood pressure, heart rate, peripheral oxygen saturation, duration of procedure, duration of ureteral placement or number of stents 30 mins before the procedure (T0) (Table 1).
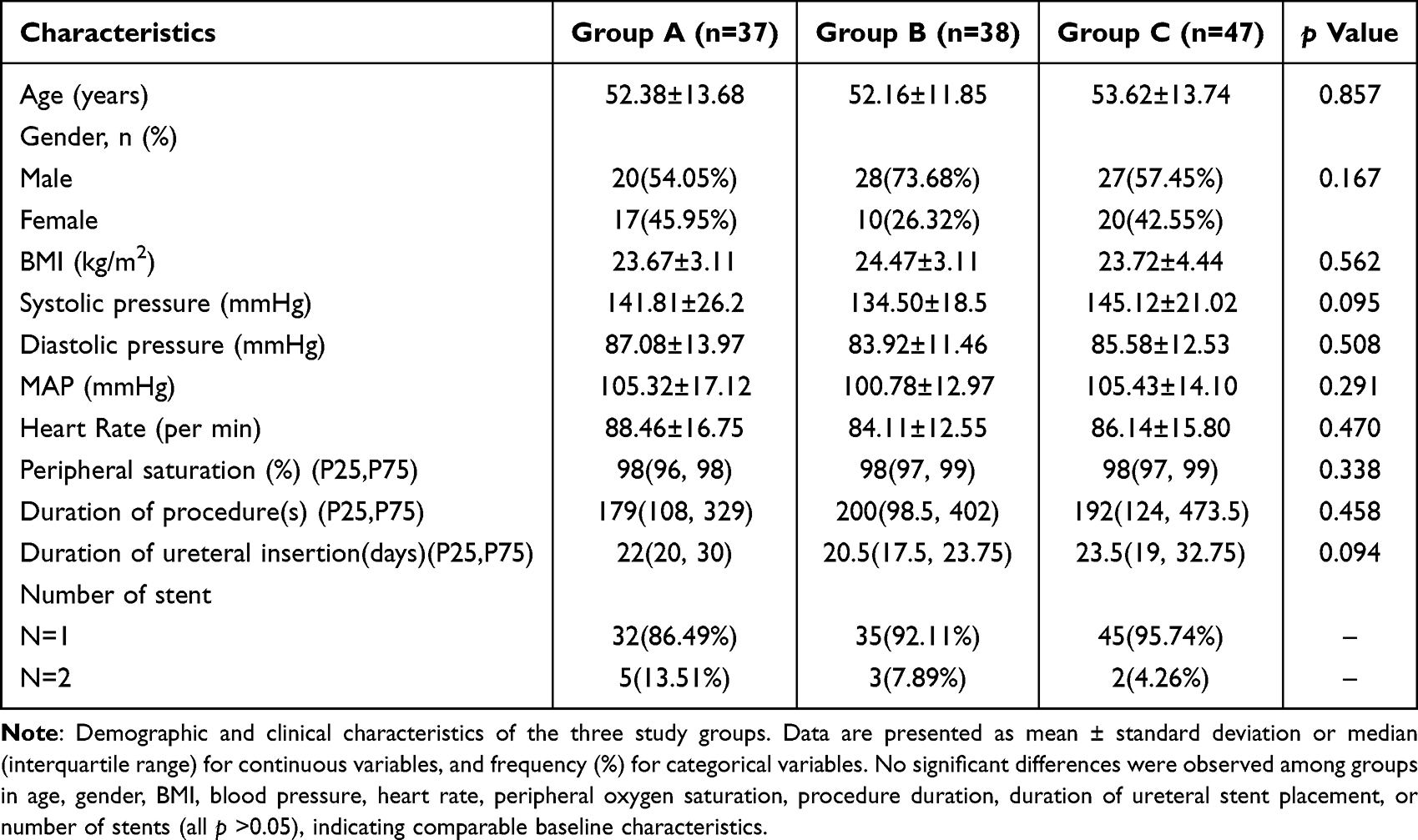 |
Table 1 Baseline Characteristics of the Patients |
Primary Endpoint: Pain Assessment (VAS Scores)
VAS at Cystoscope Insertion (T1): The median VAS scores were 1.00 (IQR: 0.00–3.00) for Group A, 1.00 (IQR: 0.00–3.00) for Group B, and 2.00 (IQR: 1.00–5.25) for Group C. Although Group C exhibited higher pain scores, the Kruskal–Wallis test showed no statistically significant difference among the groups (H =5.542, p =0.063).
VAS at Stent Removal (T2): The median VAS scores were 0.00 (IQR: 0.00–2.50) for Group A, 0.00 (IQR: 0.00–2.50) for Group B, and 0.00 (IQR: 2.00–5.00) for Group C. A significant difference was observed among the groups (H =7.222, p =0.027). Post hoc analysis revealed that Group C had significantly higher pain scores compared to Group A (p =0.014) and Group B (p=0.047).
VAS 10 Minutes Post-Procedure (T3):
The median VAS scores were 0.00 (IQR: 0.00–0.00) for Group A, 0.00 (IQR: 0.00–1.00) for Group B, and 0.00 (IQR: 0.00–2.00) for Group C. The Kruskal–Wallis test indicated a significant difference (H =8.860, p =0.012). Post hoc analysis showed that Group C had significantly higher pain scores compared to Group A (p =0.011) and Group B (p =0.020) (Table 2).
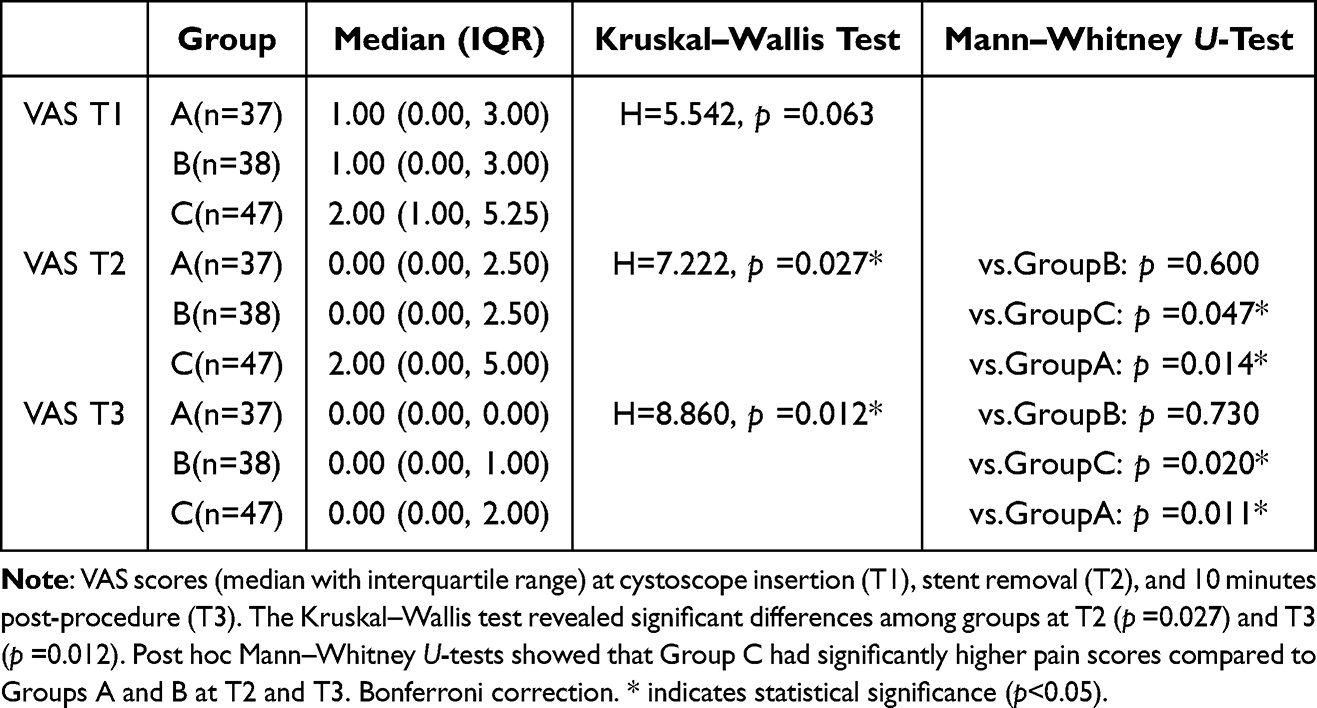 |
Table 2 Visual Analog Scale (VAS) Pain Scores at Different Time Points |
Influence of Gender and Age on Pain Scores
A repeated-measures ANOVA was conducted to examine the effects of gender and age group on the trajectory of pain scores. The analysis revealed a statistically significant Time × Gender interaction (F =7.044, p =0.006, partial η2 =0.068), indicating that the pattern of pain reduction over the procedure differed between male and female patients. In contrast, the Time × Age Group interaction was not significant (F =0.061, p =0.964, partial η2 =0.001), suggesting that the temporal pattern of pain was consistent across different age strata. Furthermore, no significant three-way interactions (Time × Group × Gender or Time × Group × Age Group) were observed (all p > 0.05), indicating that the analgesic effect of TEAS relative to sham did not differentially vary by gender or age. The between-subjects analysis confirmed a significant main effect of Gender (F =7.506, p=0.007, partial η2 =0.065), with females experienced overall lower pain levels throughout the study period. (Figure 3), while the main effect of Age Group was not significant (p =0.148). Detailed results are presented in Table 3.
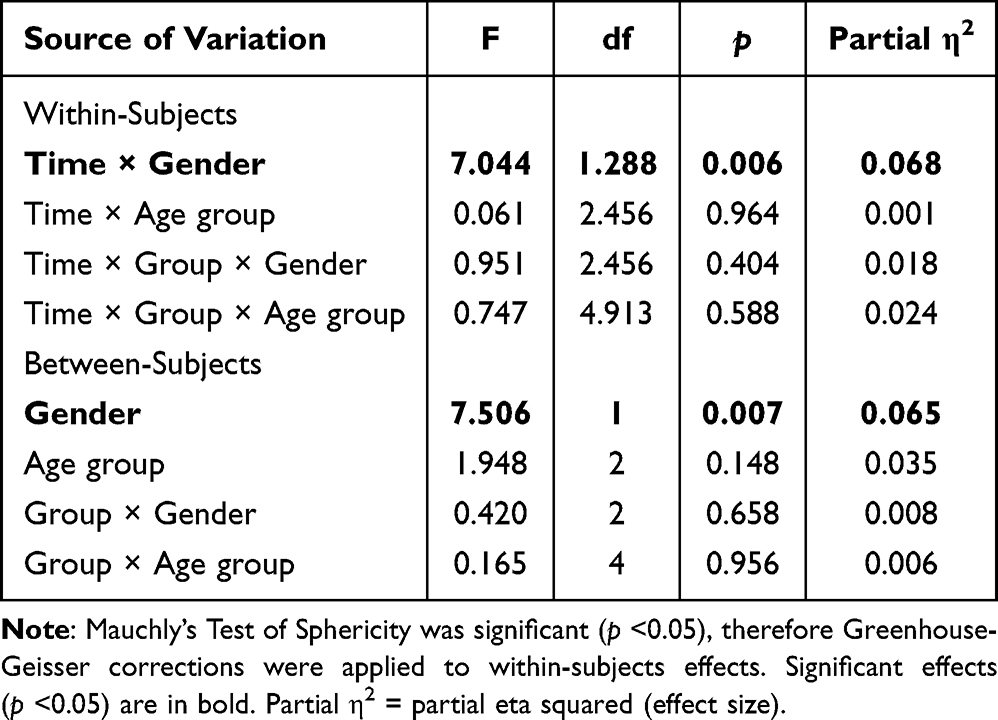 |
Table 3 Repeated Measures ANOVA of VAS Pain Scores with Gender and Age Group as Covariates |
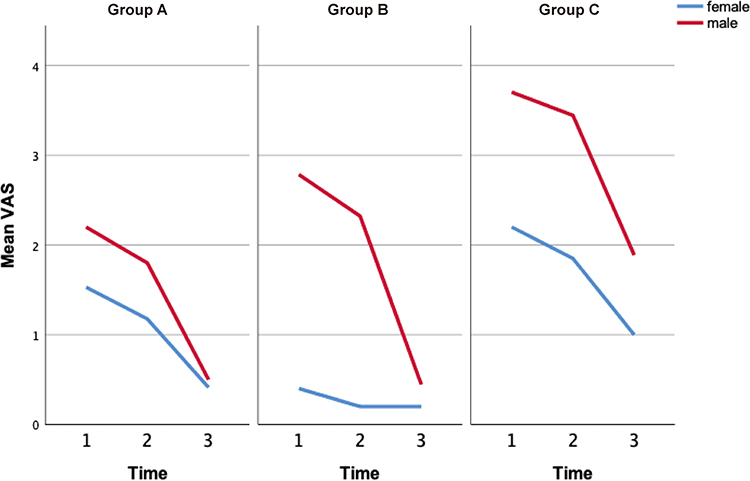 |
Figure 3 Mean VAS Pain Scores by Gender Across Time Points in Three Treatment Groups Visual Analog Scale (VAS) pain scores are presented as means across three timepoint assessments. Panels show results for (Group (A) Treatment Group A, (Group (B) Treatment Group B, and (Group (C) Control Group. Within each panel, scores are shown for male (red line) and female (blue line) participants. The time × gender interaction was statistically significant (F= 7.044, p =0.006). |
Secondary Endpoints
Hemodynamic Parameters: No significant differences were observed in systolic blood pressure (SBP), diastolic blood pressure (DBP), or mean arterial pressure (MAP) among the groups at any timepoint (all p > 0.05). However, post hoc analysis revealed a significant difference in SBP at T2 between Group B and Group C (p < 0.05). Heart Rate (HR): Heart rates were comparable across all groups at T0, T1, T2, and T3 (all p > 0.05). Peripheral Oxygen Saturation (SpO2): SpO2 levels were similar among the groups at all timepoints (all p > 0.05) (Table 4).
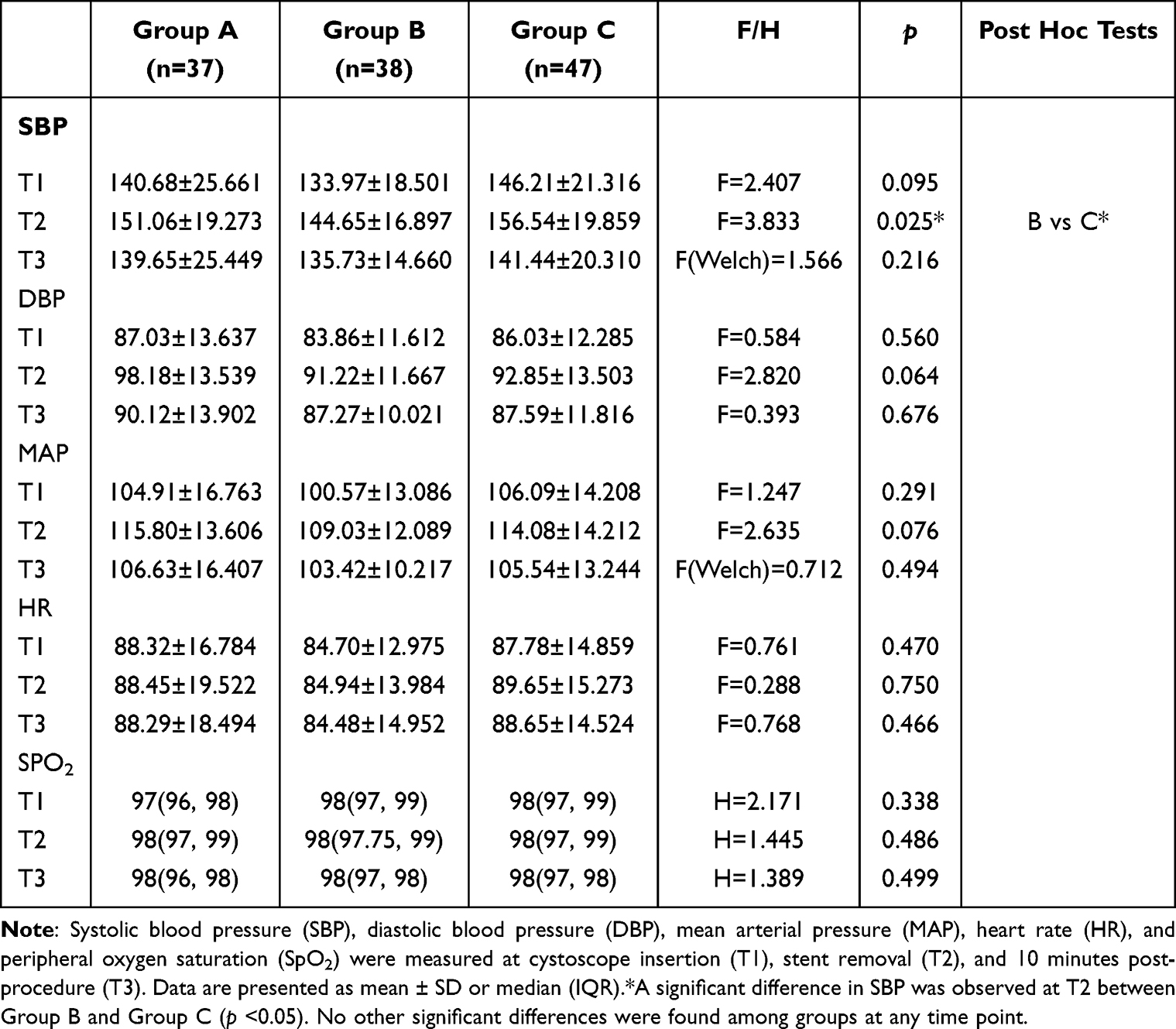 |
Table 4 Hemodynamic Parameters at Different Time Points |
Adverse Events
No severe adverse events were reported during the study. One patient in Group C experienced intolerable pain, requiring rescheduling of the procedure under general anesthesia. This patient was excluded from the final analysis.
Discussion
The findings of this randomized controlled trial demonstrate that transcutaneous electrical acupoint stimulation (TEAS) significantly reduces pain during cystoscopic ureteral stent extraction compared to sham TEAS. This study provides robust evidence supporting the clinical utility of TEAS as a non-invasive, adjunctive analgesic method for this common urological procedure. The results align with previous research highlighting the analgesic effects of acupuncture and related techniques in perioperative settings,18,19 while also addressing a gap in the literature regarding TEAS-specific applications for ureteral stent removal.
The primary endpoint analysis revealed that both TEAS groups (LI4/PC6 and SP6/ST36) exhibited significantly lower pain scores during stent removal (T2) and at 10 minutes post-procedure (T3) compared to the sham group. This suggests that TEAS not only mitigates procedural pain but also contributes to post-procedural comfort. The lack of significant differences in pain scores at cystoscope insertion (T1) may be attributed to the localized nature of TEAS effects, which are more pronounced during the mechanical stimulation of stent removal.15,20 The selection of acupoints—LI4 and PC6 (upper limb) and SP6 and ST36 (lower limb)—was based on traditional Chinese medicine principles, which associate these points with pain modulation and visceral function regulation.14 The comparable efficacy between the two TEAS groups implies that both acupoint combinations are viable for pain management in this context, offering flexibility in clinical practice.
The secondary endpoints, including hemodynamic parameters (blood pressure, heart rate, and SpO2), showed no significant differences among the groups, reinforcing the safety profile of TEAS. The absence of hemodynamic perturbations is particularly noteworthy, as it suggests that TEAS does not impose additional physiological stress on patients undergoing stent removal.21 This stability is critical for outpatient procedures, where rapid recovery and discharge are prioritized. The lone exception—a transient difference in systolic blood pressure at T2 between Group B and the sham group—may reflect a minor autonomic response to TEAS but lacks clinical significance given the overall stability.22 The sample size, though adequate for detecting pain score differences, may have been underpowered to identify rare adverse events or subtle hemodynamic changes.
Our secondary analysis incorporating gender and age as covariates yielded insightful findings. The significant Time × Gender interaction, coupled with the main effect of gender, indicate that female patients experienced a distinct pain trajectory compared to their male counterparts, with significantly more favorable postoperative pain recovery. This aligns with well-established literature on gender differences in pain perception, often attributed to a complex interplay of hormonal, psychological, and sociocultural factors.23 The absence of a significant Time × Age Group interaction implies that the physiological process of acute procedural pain and its modulation by TEAS were consistent across the adult age spectrum included in our study.
This study has several limitations that should be considered when interpreting the results. First, as a single-center trial conducted in an ethnically homogeneous Chinese population, the generalizability of our findings to other healthcare settings and diverse demographic groups may be limited. Future multicenter studies involving heterogeneous populations are warranted to validate and extend our conclusions. Crucially, the lack of significant three-way interactions (Time × Group × Gender/Age) demonstrates that the superior analgesic efficacy of TEAS over sham stimulation was maintained irrespective of the patient’s gender or age. This reinforces the robustness and general applicability of TEAS within the diverse demographic typically undergoing this urological procedure. Second, the study’s methodology adhered to rigorous standards, including randomization, blinding, and predefined outcome measures, which enhance the validity of the findings. The use of a sham TEAS group controlled for placebo effects, and the double-blinding of patients and assessors minimized bias.24 Regarding blinding, while the patients and the outcome assessors (physicians evaluating pain and recording hemodynamic parameters) were successfully blinded to the group assignments, the acupuncturists administering the TEAS could not be blinded. This was inherent to the intervention, as the adjustment of stimulation intensity to the patient’s tolerance threshold and the observation of muscle twitching in the active groups made it impossible to conceal the treatment allocation from the operator. This is a common methodological challenge in trials involving physical stimulation techniques.25 Although every effort was made to standardize the interaction between the acupuncturist and the patient, the potential for performance bias cannot be entirely ruled out. Future studies could explore alternative sham techniques to improve blinding fidelity. Third, and importantly, our study was not designed or powered to directly compare the effectiveness between the two active acupoint combinations (LI4/PC6 vs SP6/ST36). While both were superior to sham TEAS, the absence of a statistically significant difference between them should not be interpreted as evidence of equivalence. Future studies with a head-to-head comparative design and a non-inferiority or superiority framework are required to determine if one combination is clinically superior to the other for this specific procedure. Additionally, the short follow-up period (1 hour post-procedure) precludes assessment of longer-term effects, such as delayed pain or urinary symptoms.
The observed pain reduction in TEAS groups aligns with mechanistic studies suggesting that acupuncture and TEAS modulate pain through endogenous opioid release, gate control mechanisms, and autonomic nervous system regulation.26 The dense-disperse frequency (2/100 Hz) used in this study is known to activate both opioid and non-opioid pathways, providing broad-spectrum analgesia.14 This may explain why TEAS was effective without the need for additional pharmacological interventions, such as opioids, which carry risks of side effects and dependency.27
One patient in the sham group withdrew due to intolerable pain, underscoring the clinical relevance of TEAS in improving procedural tolerance. While this event did not significantly impact the overall results, it highlights the potential of TEAS to reduce the need for rescue analgesia or procedural rescheduling under general anesthesia,28,29 thereby optimizing resource utilization in outpatient settings.
Several other important aspects merit consideration. First, while a formal cost-effectiveness analysis was not within the scope of this study, the TEAS intervention is inherently low-cost, non-pharmacological, and can be administered by trained nursing staff, which suggests its potential for reducing healthcare expenditures associated with procedural analgesia and managing drug-related side effects.30,31 Second, although patient satisfaction was not a predefined quantitative endpoint in our trial, the significant reduction in procedural pain (VAS scores) and the fact that no patient in the TEAS groups requested rescue analgesia or withdrew due to pain indirectly reflect an improved patient experience and tolerance. Future studies should incorporate validated satisfaction questionnaires to quantitatively assess this important outcome. Finally, as noted earlier, the generalizability of our findings to non-Chinese populations may be limited by the ethnic and cultural homogeneity of our cohort. The efficacy of TEAS is likely influenced by genetic backgrounds, cultural beliefs regarding acupuncture, and pain coping mechanisms, which vary across different ethnic groups.32 Therefore, our promising results warrant further validation through international, multi-center, randomized controlled trials in diverse demographic and healthcare settings.
Conclusion
In conclusion, this trial provides compelling evidence that TEAS is an effective and safe adjunct for pain relief during cystoscopic ureteral stent extraction. Its non-invasive nature, absence of hemodynamic effects, and compatibility with outpatient protocols make it a promising option for enhancing patient comfort. These findings advocate for the integration of TEAS into routine clinical practice, particularly in settings where minimizing pharmacological analgesia is desirable. Further research should explore optimal stimulation parameters, cost-effectiveness, and patient satisfaction to solidify TEAS’s role in urological pain management.
Data Sharing Statement
The datasets generated and analyzed during the current study are included in this published article. Due to the constraints of the ethical approval and the informed consent agreements with the participants, additional individual de-identified participant data will not be shared. Further raw data that support the findings of this study will be made available by the corresponding author, Meizi Qian, upon reasonable request, starting from the date of publication and for a period of six months thereafter. Requests for data access can be directed to [email protected].
Institutional Review Board Statement
Our clinical trial was approved by the Institutional Review Board of the First Affiliated Hospital of Wenzhou Medical University (IRB00001052-13003)(2022)-No.(199-01), which conforms to the provisions of the Declaration of Helsinki (as revised in Tokyo 2004). This study was registered at the Chinese Clinical Trials Registry (ChiCTR), Protocol ID Number ChiCTR2300072451.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was supported by the Natural Science Foundation of Zhejiang Province (LQ21H150007), The Medical and Health Research Project of Zhejiang Province (2025KY990) and Wenzhou Science and Technology Bureau, Zhejiang Province, China (Y2023062).
Disclosure
Jisheng Han is the inventor of the TEAS stimulator. The remaining authors declare that they have no conflicts of interest for this work.
References
1. Chathuranga A, Sagara Ruwan Kumara AMG, Sandamalee K, et al. Cystoscopic extraction of an inadvertently placed ureteral stent in inferior vena cava. Asian J Urol. 2020;7(4):373–375. doi:10.1016/j.ajur.2019.09.001
2. Juliebø-jones P, Pietropaolo A, Haugland JN, et al. Current status of ureteric stents on extraction strings and other non-cystoscopic removal methods in the paediatric setting: a systematic review on behalf of the European Association of Urology (EAU) Young Academic Urology (YAU) Urolithiasis Group. Urology. 2022;160:10–16. doi:10.1016/j.urology.2021.11.022
3. Loh-Doyle JC, Low RK, Monga M, et al. Patient experiences and preferences with ureteral stent removal. J Endourol. 2015;29(1):35–40. doi:10.1089/end.2014.0402
4. Joshi HB, Stainthorpe A, Macdonagh RP, et al. Indwelling ureteral stents: evaluation of symptoms, quality of life and utility. J Urol. 2003;169(3):1065–1069. doi:10.1097/01.ju.0000048980.33855.90
5. Taylor L, Cho A, Smeulders N. Seamless post-operative removal of JJ stents in the paediatric population: securing the JJ stent to the tip of the urethral balloon catheter avoids a further operation. J Pediatr Urol. 2020;16(4):500–501. doi:10.1016/j.jpurol.2020.06.028
6. Wetzel B, Pavlovic D, Kuse R, et al. The effect of auricular acupuncture on fentanyl requirement during Hip arthroplasty: a randomized controlled trial. Clin J Pain. 2011;27(3):262–267. doi:10.1097/AJP.0b013e3181fd516c
7. Zhou J, Chi H, Cheng TO, et al. Acupuncture anesthesia for open heart surgery in contemporary China. Int J Cardiol. 2011;150(1):12–16. doi:10.1016/j.ijcard.2011.04.002
8. Wang H, Xie Y, Zhang Q, et al. Transcutaneous electric acupoint stimulation reduces intra-operative remifentanil consumption and alleviates postoperative side-effects in patients undergoing sinusotomy: a prospective, randomized, placebo-controlled trial. Br J Anaesth. 2014;112(6):1075–1082. doi:10.1093/bja/aeu001
9. Huang S, Peng W, Tian X, et al. Effects of transcutaneous electrical acupoint stimulation at different frequencies on perioperative anesthetic dosage, recovery, complications, and prognosis in video-assisted thoracic surgical lobectomy: a randomized, double-blinded, placebo-controlled trial. J Anesth. 2017;31(1):58–65. doi:10.1007/s00540-015-2057-1
10. Tan SY, Jiang H, Ma Q, et al. Effects of transcutaneous electrical acupoint stimulation on early postoperative pain and recovery: a comprehensive systematic review and meta-analysis of randomized controlled trials. Front Med. 2024;11:1302057. doi:10.3389/fmed.2024.1302057
11. Szmit M, Krajewski R, Rudnicki J, et al. Application and efficacy of transcutaneous electrical acupoint stimulation (TEAS) in clinical practice: a systematic review. Adv Clin Exp Med. 2023;32(9):1063–1074. doi:10.17219/acem/159703
12. Choi SH, Chang IM. A Milestone in Codifying the Wisdom of Traditional Oriental Medicine: TCM, Kampo, TKM, TVM-WHO international standard terminologies on traditional medicine in the western pacific region. Evid Based Complement Alternat Med. 2010;7(3):303–305. doi:10.1093/ecam/nen083
13. Tian L, Feng X, Zhang R, et al. Pain relief during oocyte retrieval by transcutaneous electrical acupoint stimulation: a single-blinded, randomized, controlled multicenter trial. Evid Based Complement Alternat Med. 2020;2020:3285648. doi:10.1155/2020/3285648
14. Han JS. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci. 2003;26(1):17–22. doi:10.1016/S0166-2236(02)00006-1
15. Chang XL, Liu XM, An LX, et al. Effects of transcutaneous electrical acupoint stimulation (TEAS) on postoperative pain in patients undergoing gastric and esophageal ESD surgery: a study protocol for a prospective randomized controlled trial. BMC Complement Med Ther. 2023;23(1):253. doi:10.1186/s12906-023-04075-9
16. Liu W, Ding Y, Xie H, et al. Efficacy and safety of transcutaneous electrical acupoint stimulation for the management of primary dysmenorrhoea: protocol for a randomised controlled trial in China. BMJ Open. 2024;14(6):e078895. doi:10.1136/bmjopen-2023-078895
17. Gauba A, Ramachandra MN, Saraogi M, et al. Music reduces patient-reported pain and anxiety and should be routinely offered during flexible cystoscopy: outcomes of a systematic review. Arab J Urol. 2021;19(4):480–487. doi:10.1080/2090598X.2021.1894814
18. Acar HV. Acupuncture and related techniques during perioperative period: a literature review. Complement Ther Med. 2016;29:48–55. doi:10.1016/j.ctim.2016.09.013
19. Lee A, Fan LT. Stimulation of the wrist acupuncture point P6 for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2009(2):Cd003281.
20. Wu Y, Zhou J, Zhu F, et al. The effects of pain relief on proprioception and muscle strength for tibial plateau fractures: a randomized controlled trial. Musculoskelet Sci Pract. 2022;62:102658. doi:10.1016/j.msksp.2022.102658
21. Park J, Sohn Y, White AR, et al. The safety of acupuncture during pregnancy: a systematic review. Acupunct Med. 2014;32(3):257–266. doi:10.1136/acupmed-2013-010480
22. Zhang R, Lao L, Ren K, et al. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
23. Fillingim RB, King CD, Ribeiro-Dasilva MC, et al. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009;10(5):447–485. doi:10.1016/j.jpain.2008.12.001
24. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172(19):1444–1453. doi:10.1001/archinternmed.2012.3654
25. Wang XC, Liu XY, Shi KL, et al. Blinding assessment in clinical trials of traditional Chinese medicine: exploratory principles and protocol. J Integr Med. 2023;21(6):528–536. doi:10.1016/j.joim.2023.10.003
26. Han JS. Acupuncture and endorphins. Neurosci Lett. 2004;361(1–3):258–261. doi:10.1016/j.neulet.2003.12.019
27. Meissner K, Fässler M, Rücker G, et al. Differential effectiveness of placebo treatments: a systematic review of migraine prophylaxis. JAMA Intern Med. 2013;173(21):1941–1951. doi:10.1001/jamainternmed.2013.10391
28. Liu J, Zhang K, Zhang Y, et al. Perioperative transcutaneous electrical acupoint stimulation reduces postoperative pain in patients undergoing thoracoscopic surgery: a randomized controlled trial. Pain Res Manag. 2024;2024:5365456. doi:10.1155/2024/5365456
29. Ao L, Shi J, Bai Y, et al. Effects of transcutaneous electrical acupoint stimulation on perioperative immune function and postoperative analgesia in patients undergoing radical mastectomy: a randomized controlled trial. Exp Ther Med. 2021;21(3):184. doi:10.3892/etm.2021.9615
30. Wang D, Shi H, Yang Z, et al. Efficacy and safety of transcutaneous electrical acupoint stimulation for postoperative pain: a meta-analysis of randomized controlled trials. Pain Res Manag. 2022;2022:7570533. doi:10.1155/2022/7570533
31. Yu M, Qian H, Gan M. Comparison of different interventions for the reduction of labor pain: a systematic review and network meta-analysis. Medicine. 2024;103(10):e37047. doi:10.1097/MD.0000000000037047
32. Dusek JA, Kallenberg GA, Storrow AB, et al. Acupuncture in the emergency department (ACUITY): results from a BraveNet multi-center feasibility randomized controlled trial. Integr Med Res. 2024;13(4):101095. doi:10.1016/j.imr.2024.101095
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.