Back to Journals » Journal of Pain Research » Volume 18
Pain Management for Postpartum Pain: A Narrative Review
Authors Zhou L, Li J, Zhou Y, Liang Y, Ma Q, Yang L, Pang Y, Fang Y, Guo Y ![]()
Received 8 July 2025
Accepted for publication 22 October 2025
Published 27 October 2025 Volume 2025:18 Pages 5617—5626
DOI https://doi.org/10.2147/JPR.S552442
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Lianzhen Zhou,1,* Junmin Li,2,* Yali Zhou,2 Yanan Liang,3 Qingling Ma,3 Luyao Yang,3 Yunting Pang,3 Yong Fang,3 Yaqiu Guo3
1Department of Anesthesiology, Jinan Central Hospital, Central Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, People’s Republic of China; 2Department of Obstetrics and Gynecology, Jinan Maternal and Child Health Hospital, Affiliated to Shandong First Medical University, Jinan, People’s Republic of China; 3Department of Anesthesiology, Jinan Maternal and Child Health Hospital, Affiliated to Shandong First Medical University, Jinan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yaqiu Guo; Yong Fang, Department of Anesthesiology, Jinan Maternal and Child Health Hospital, Affiliated to Shandong First Medical University, No. 22029 Jingshi Road, Jinan, 250001, People’s Republic of China, Tel +86-0531-89029588 ; +86-0531-89029532, Email [email protected]; [email protected]
Abstract: Postpartum pain is a complex clinical phenomenon that encompasses multiple types, including uterine contraction pain, perineal pain, breast pain, incisional pain, pelvic pain, low back pain(LBP), and pelvic girdle pain. These conditions can significantly impair maternal recovery and quality of life, thereby exerting adverse effects on maternal and neonatal health outcomes. The underlying mechanisms are diverse, involving tissue injury, inflammatory responses, neural sensitization, myofascial dysfunction, and psychological stress. Given its high prevalence and broad clinical impact, the study and management of postpartum pain hold substantial clinical significance. Although research in this field has increased in recent years, existing studies are largely confined to specific pain types or single intervention modalities, with limited efforts toward a comprehensive integration of the full spectrum of postpartum pain or a systematic analysis of its underlying mechanisms. Therefore, a comprehensive review is warranted to summarize the classifications, pathophysiological mechanisms, and multimodal management strategies of postpartum pain. The objectives of this review are threefold: (1) to systematically categorize different types of postpartum pain and outline their epidemiological characteristics and clinical burden; (2) to summarize the potential etiological factors and pathophysiological mechanisms underlying each pain type; and (3) to evaluate the clinical effectiveness of current multimodal analgesic strategies, with particular attention to the role of non-pharmacological interventions in postpartum pain management. Through this review, we aim to provide clinicians with a structured reference framework, while also identifying priorities for future research, thereby contributing to the development of systematic and individualized management strategies to ultimately improve maternal and neonatal outcomes.
Keywords: postpartum pain, multimodal analgesia, pain assessment tools, perineal pain, pelvic girdle pain, chronic pain
Introduction
Postpartum pain is a multifactorial clinical syndrome resulting from anatomical, physiological, and psychological changes associated with pregnancy and childbirth. It is highly prevalent among postpartum women and can substantially impact early recovery and quality of life. Clinical data suggest that 70%–80% of women experience varying degrees of acute or persistent pain after delivery, manifesting as uterine contraction pain, perineal pain, breast pain, incisional pain, LBP, or pelvic girdle pain.1
Historically, postpartum pain was often considered a physiological inevitability, with empirical opioid administration as the mainstay of treatment. However, as understanding of pain mechanisms and patient experiences has evolved, the limitations of this singular approach have become evident. These include risks of opioid overuse, addiction, respiratory depression, gastrointestinal side effects, and progression to chronic pain. This has driven a shift toward multimodal analgesia strategies, integrating regional nerve blocks, NSAIDs, and non-pharmacological interventions to develop evidence-based, individualized pain management plans.2 Such strategies not only reduce opioid consumption but also lower the incidence of postpartum psychological conditions such as depression and anxiety, ultimately improving maternal and neonatal outcomes.1
Given the heterogeneity and multifactorial nature of postpartum pain mechanisms, its management requires interdisciplinary collaboration and phase-specific interventions. In recent years, multidimensional pain assessment tools—such as the Short-Form Brief Pain Inventory (SF-BPI) and McGill Pain Questionnaire (MPQ)—have been increasingly implemented in clinical settings.1 These tools emphasize that pain is not solely a sensory experience but also encompasses functional, emotional, and social dimensions. Moreover, each type of postpartum pain has distinct pathophysiological underpinnings: uterine contraction pain is linked to oxytocin-mediated myometrial contractions;3 perineal pain often results from tissue trauma and inflammation; incisional pain is associated with local tissue damage and scar adhesions. Chronic pain development frequently involves neural sensitization, mood disturbances, and structural instability, posing significant clinical challenges.
To enhance the scientific and systematic management of postpartum pain, this review synthesizes recent research advances by addressing assessment methods, epidemiological characteristics, pathophysiological mechanisms, and management strategies for various common types of postpartum pain. The aim is to inform clinical practice and support improved postpartum recovery and long-term health outcomes.
Literature Search Strategy
For this review, a comprehensive literature search was conducted in the PubMed and Web of Science database up to June 1, 2025. The following keywords were used: “postpartum pain”, “uterine contraction pain”, “postpartum perineal pain”, “breast pain”, “pelvic pain”, “incisional pain”, “persistent postpartum pain”, “postpartum low-back pain” and “pelvic girdle pain”. After retrieving the relevant studies, a multi-step screening process was employed. Titles and abstracts were initially reviewed to assess relevance, followed by full-text evaluation. Studies that did not specifically address postpartum-related pain were excluded from the final selection.
Assessment of Postpartum Pain
Accurate assessment of postpartum pain is essential for alleviating maternal discomfort and promoting timely recovery.4 The use of validated assessment tools enables clinicians to comprehensively evaluate the location, nature, intensity, duration, and modulating factors of pain, thereby facilitating the development of individualized management strategies.
Clinically, pain assessment methods are broadly categorized into unidimensional and multidimensional tools. Unidimensional tools primarily focus on pain intensity and include the Visual Analog Scale (VAS), Numeric Rating Scale (NRS), Verbal Rating Scale (VRS), and the Faces Pain Scale (FPS).5 These tools are user-friendly and suitable for rapid pain monitoring in routine clinical settings. The characteristics of common unidimensional tools are summarized in Table 1.
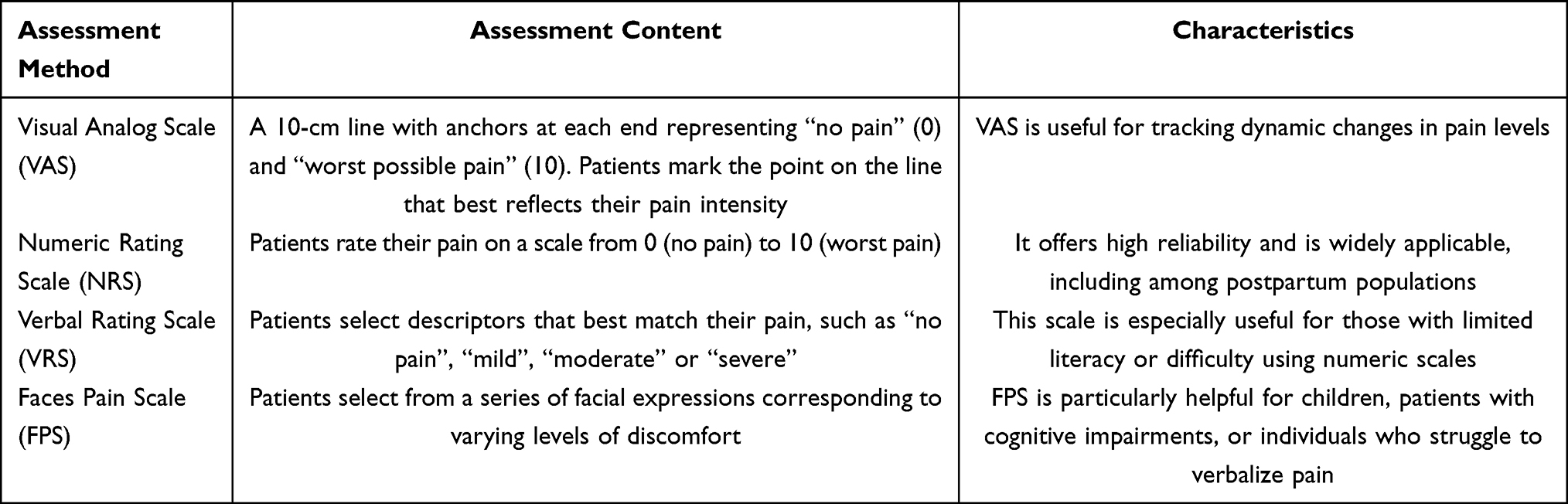 |
Table 1 Common Unidimensional Pain Assessment Methods and Their Characteristics |
In contrast, multidimensional pain assessment tools evaluate not only pain intensity but also its sensory, emotional, and functional impact. Among these, the SF-BPI and the MPQ are widely adopted in postpartum pain research and clinical practice.6,7 The SF-BPI is efficient and available in multiple languages, enabling assessment of pain severity and its effects on daily functioning, emotional well-being, and social interactions.6 The MPQ provides a comprehensive evaluation of the sensory, affective, and cognitive aspects of pain, making it particularly valuable for identifying psychological dimensions of chronic pain.7
Given the complexity of postpartum pain experiences, no single tool is sufficient to capture the full clinical picture. Therefore, integrating multiple assessment methods is key to improving diagnostic accuracy. For example, combining the VRS with the FPS allows for both emotional context and visual representation of pain. Clinicians should select tools based on the patient’s clinical condition, cognitive and linguistic abilities, and the specific goals of assessment. This tailored approach facilitates a deeper understanding of the pain experience and guides the formulation of effective, individualized pain management plans.
Common Types of Postpartum Pain and Their Management
Uterine Contraction Pain
Uterine contraction pain, also known as afterpains, is a common postpartum symptom resulting from rhythmic contractions of the uterine smooth muscle during uterine involution. Typically, the pain arises within 1–2 days post-delivery and lasts approximately 2–3 days.8 A study by Fang et al9 reported that up to 50% of women experience uterine contraction pain within the first 48 hours after vaginal delivery, with those who have a history of dysmenorrhea being more likely to report more severe symptoms. In addition, Holdcroft et al10 found that multiparous women are more likely to experience more intense uterine contraction pain compared to primiparous women.
Several factors influence the severity of uterine contraction pain. Breastfeeding is a major contributor, as infant suckling stimulates endogenous oxytocin release, intensifying uterine contractions and associated pain.11 Similarly, uterotonic agents such as oxytocin and ergot alkaloids—used to prevent postpartum hemorrhage—can exacerbate contraction-induced discomfort.9 Psychological and physiological factors also modulate pain perception; emotional status, previous childbirth experience, and social support all influence how postpartum women experience and report uterine pain.12
Although common, most women perceive uterine contraction pain as tolerable. Studies indicate that nearly 90% of postpartum women do not require targeted treatment, implying that such pain is generally self-limited and does not significantly impede overall recovery.9
Nonetheless, multimodal analgesia is increasingly advocated to manage uterine contraction pain effectively. Epidural analgesia is one of the conventional approaches for postpartum pain management. A study by Mo et al13 demonstrated that programmed intermittent epidural bolus (PIEB) provides superior analgesic efficacy compared to traditional continuous epidural infusion (CEI) following cesarean section, with a lower incidence of motor blockade. In terms of intravenous analgesia, a retrospective study conducted by Zheng et al in 202314 indicated that, compared to the commonly used sufentanil, nalbuphine—acting as a κ-opioid receptor agonist and μ-opioid receptor antagonist—offers more effective relief of uterine contraction pain in multiparous women, while also reducing the incidence of adverse effects such as nausea, pruritus, and urinary retention.
In addition to pharmacological treatments, non-pharmacological interventions have also shown promising potential in alleviating uterine contraction pain. Transcutaneous electrical nerve stimulation (TENS), a non-invasive, low-cost, and easy-to-administer analgesic technique, has been preliminarily applied in clinical practice. A study by de Sousa et al15 demonstrated that high-frequency electrical stimulation applied to the T10–L1 and S2–S4 spinal segments can interfere with the transmission of afferent uterine pain signals, significantly reducing pain scores during breastfeeding in multiparous women. However, a systematic review by Deussen et al published in 20202 emphasized that the mechanisms and clinical efficacy of TENS for managing uterine contraction pain require further validation through high-quality studies.
Perineal Pain
Perineal pain is one of the most frequently reported types of postpartum pain among women who have undergone vaginal delivery. A study by Andrews et al16 reported that approximately 90% of women experience some degree of perineal pain following childbirth, even in the absence of overt perineal lacerations. The incidence increases significantly with episiotomy or spontaneous perineal tears.17,18 Although most cases resolve within two months, about 10% of women report persistent discomfort up to 18 months postpartum.16 In addition, perineal pain is closely associated with sexual dysfunction. The study by Andrews et al16 indicated that approximately 42% of women continued to experience dyspareunia two months postpartum.
The primary mechanism involves trauma to the perineal region during childbirth, including skin, mucosa, and deep muscle tissues (eg, bulbospongiosus, superficial transverse perineal muscles). Tissue injury from compression, tearing, or surgical incision leads to inflammation, edema, and localized nociceptor activation.18
For the management of postpartum perineal pain, multimodal analgesia strategies combining pharmacological and non-pharmacological interventions are commonly employed in clinical practice. Among pharmacological options, NSAIDs, such as ibuprofen and aspirin, alleviate local inflammation and pain by inhibiting prostaglandin synthesis, and are suitable for mild to moderate pain relief.19,20 A systematic review by Abalos et al21 demonstrated that a single dose of paracetamol can effectively relieve perineal pain following vaginal delivery. Regarding local anesthetics, a study by Abu-Zaid et al22 found that ropivacaine offers several advantages over conventional lidocaine, including a longer duration of analgesia and reduced injection discomfort, resulting in significantly higher maternal satisfaction (OR = 7.13, P < 0.001).
As an important adjunct to pharmacological approaches, non-pharmacological therapies have received increasing attention in recent years and have demonstrated promising potential in the management of postpartum perineal pain. A growing body of research suggests that various non-pharmacological interventions can play a beneficial role in alleviating postpartum discomfort.In terms of physical therapies, studies by Kurnaz et al23 and Francisco et al24 confirmed that local application of ice packs is an effective and easy-to-implement method for relieving perineal pain. In addition, a systematic review by Abdelhakim et al25 reported that antenatal perineal massage not only reduces the incidence of perineal tears but also promotes wound healing and alleviates postpartum perineal pain.Traditional Chinese therapies have also shown effectiveness in managing acute postpartum perineal pain. Acupuncture and its related techniques, such as auricular acupressure, have been proven to relieve pain, potentially through activation of the endogenous opioid system. Acupressure, particularly at points such as LV4 (Zhongfeng) and LI4 (Hegu-4), has been shown to significantly reduce pain intensity within 30 to 120 minutes after delivery. This technique offers prolonged analgesic effects, high maternal acceptability, and is considered a safe, economical, and non-invasive intervention.26 Moreover, emerging technologies have been explored in this context. A study by Filippini et al27 found that carbon dioxide (CO2) laser therapy may help reduce postpartum perineal discomfort. However, its clinical efficacy and long-term safety need to be further validated in larger patient populations.
Breast Pain
Postpartum breast pain is a common concern among lactating women and can compromise breastfeeding continuation. A study by Amir et al28 reported that over 70% of first-time mothers experience breast pain. Common etiologies include ductal obstruction, mastitis, breast abscesses, nipple blisters, dermatitis, vasospasm, and milk stasis—with ductal blockage being the most prevalent.29,30
Pathophysiologically, pain is often triggered by retained milk and subsequent inflammation or infection of breast tissue. Predisposing factors include inadequate milk expression, poor latch, sustained breast compression, and hyperlactation. Retained milk creates a favorable environment for microbial growth. A systematic review by Christine et al31 identified Staphylococcus aureus and Candida species as the primary pathogens associated with mastitis. However, a retrospective cohort study by Betts et al30 in 2021 reported that many patients did not experience sustained relief following antifungal treatment. Based on these findings, the evidence supporting Candida infection as a cause of breastfeeding-related breast pain remains insufficient. The study recommends that clinical evaluations should not rely on presumptive diagnoses based solely on suspected Candida involvement.
Management of postpartum breast pain should be based on the specific etiology. In cases of ductal obstruction, warm compresses, gentle massage, and milk expression (manual or through breastfeeding) are effective.32 For infectious mastitis, mild cases can be managed conservatively, while moderate-to-severe cases may require antibiotics (cephalosporins). Breast abscesses often necessitate ultrasound-guided aspiration or surgical drainage. For nipple-related conditions, such as blisters or fissures, proper hygiene, drying, and application of breast milk can prevent secondary infection. Fluconazole may be considered when fungal infection is confirmed by culture or clinical evidence.33
In addition, several non-pharmacological therapies have been preliminarily applied and validated in the clinical management of breast pain, offering more treatment options—particularly for patients who are unable or unwilling to use medications. A study by Çağan et al34 demonstrated that the Oketani breast massage technique can effectively relieve breast engorgement. Han et al32 found that auricular acupressure significantly increased the pressure pain threshold in specific regions of the breast, suggesting its potential effectiveness in alleviating breast tenderness. Although these interventions have shown promising initial results, their efficacy and underlying mechanisms require further confirmation through high-quality studies.
Pelvic Pain
A study by Åhlund et al35 reported that approximately 10% of women experience pelvic pain, including perineal pain, within the first year postpartum. The incidence is notably higher among those with anal sphincter injuries or severe perineal lacerations. The underlying mechanisms are multifactorial, often involving pelvic floor trauma, inflammation, and myofascial dysfunction. Vaginal delivery may result in perineal tears, sphincter damage, and pelvic support structure laxity, leading to localized pain.36 Repetitive muscle strain and persistent inflammation may cause peripheral nerve sensitization, making even minor stimuli painful. Neuroinflammation further amplifies nociceptor excitability and disrupts neurotransmitter function, contributing to typical myofascial pelvic pain characterized by hyperalgesic trigger points in pelvic floor muscles.37 Chronic pelvic pain is frequently associated with genitourinary dysfunction, including urinary incontinence and bowel irregularities, which compound physical and psychological burden.
Physical therapy is an important component of postpartum pelvic pain management and includes interventions such as pelvic floor muscle training and radiofrequency therapy. A systematic review by Woodley et al38 demonstrated that pelvic floor muscle training can effectively prevent urinary incontinence and improve pelvic floor muscle strength. In addition, a study by Li et al37 found that radiofrequency therapy may alleviate myofascial pelvic pain by delivering thermal energy to enhance local blood circulation and reduce muscle tension.
Notably, an interview study by Buurman et al39 revealed that many women have limited awareness and inadequate preparation for postpartum pelvic pain. Therefore, greater emphasis should be placed on health education by obstetricians and midwives, particularly regarding pelvic floor dysfunction prevention and management, to help mitigate long-term impacts on women’s quality of life.
Incisional Pain After Cesarean Section
Incisional pain following cesarean delivery is common and may affect maternal mobility, infant bonding, and breastfeeding.13 Its etiology is complex, involving surgical trauma, inflammatory responses, and scar tissue formation.40 Mechanical injury to abdominal and uterine tissues activates local inflammation and cytokine release (IL-6, TNF-α), which sensitize peripheral nerves.41 Edema and scar adhesion can further activate nociceptors or compress nerves, leading to persistent or referred pain.42 Postoperative scar tissue formation may also lead to nerve compression, which may lead to intractable incisional pain or referred pain.43
The management of incisional pain following cesarean section primarily relies on multimodal analgesia strategies. Among these, neuraxial analgesia—such as epidural or intrathecal administration of morphine—remains one of the most effective approaches. However, it may be associated with adverse effects including pruritus, nausea, vomiting, and respiratory depression.13 In recent years, regional nerve block techniques have gained attention as effective alternatives. Qin et al41 demonstrated that approaches such as the transversus abdominis plane (TAP) block and the erector spinae plane (ESP) block provide satisfactory postoperative analgesia and significantly reduce opioid requirements. Local anesthetic techniques have also emerged as promising adjuncts. For instance, lidocaine patches and intraoperative fascial infiltration of bupivacaine combined with epinephrine have been explored. A study by de Queiroz et al44 found that 5% lidocaine patches effectively reduced pain scores within the first 36 hours postoperatively, although they did not significantly impact opioid consumption, recovery quality, or adverse event rates. A study by Garmi et al45 demonstrated that intraoperative wound infiltration with bupivacaine combined with epinephrine significantly reduced incisional pain following cesarean section and decreased the need for rescue opioid analgesics postpartum. No intervention-related adverse effects were observed, indicating favorable safety and analgesic efficacy. This technique may serve as an effective strategy for postoperative pain management after cesarean delivery.
In addition, scar adhesion and the choice of skin closure technique after cesarean section are also important factors influencing incisional pain.A study by Li et al40 demonstrated that autologous fat grafting not only improves the appearance and texture of scar adhesions but also helps alleviate pain associated with scar tissue to some extent. Nitsche et al42 found that the use of absorbable subcutaneous staples can reduce the need for postoperative analgesics and thereby support enhanced recovery after surgery. For specific populations, Ibrahim et al43 reported that in obese women, continuous subcutaneous suturing may lower the risk of incisional infection compared to interrupted skin sutures, although it may be associated with increased short-term pain.
Persistent Postpartum Pain (PPP)
PPP is a chronic pain condition that affects maternal health, mental well-being, and family functioning.46 A study by Valinger et al47 reported that 4% to 31% of women continue to experience varying degrees of chronic pain after childbirth, with some cases persisting for several years or even more than a decade. Common manifestations include pelvic girdle pain, LBP, and persistent incisional pain.48
The mechanisms of PPP involve inflammatory pathways, joint instability, and abnormal neural modulation. A study by Yurashevich et al49 found that levels of the proinflammatory cytokine interleukin-1β (IL-1β) in the cerebrospinal fluid were significantly elevated in patients with persistent pain following cesarean section, suggesting that neuroinflammation may play a key role in the development of chronic pain. Structural instability—such as lax ligaments or sacroiliac joint dysfunction—also contributes to chronic pelvic and lumbar pain.50
Several risk factors for PPP have been identified. A study by Eisenach et al51 indicated that the intensity of acute pain within the first 36 hours after delivery is a strong predictor of PPP, even more influential than the mode of delivery (vaginal or cesarean). Psychological stressors such as postpartum depression and anxiety further increase risk, with emotional distress shown to exacerbate PPP.46
Current treatment includes NSAIDs, opioids, and in select cases, surgical interventions. According to a report by Capobianco et al,50 minimally invasive sacroiliac joint fusion can effectively relieve pain symptoms in patients with severe sacroiliac joint dysfunction. In addition, a study by Stuge et al52 demonstrated that targeted muscle stabilization training shows beneficial effects in improving pain intensity, functional status, and quality of life.
Postpartum Low Back Pain
LBP is frequently reported by postpartum women, with prevalence estimates ranging from 15% to 70%. While some recover shortly after delivery, 5%–40% experience persistent symptoms for more than six months.53–55
The causes of postpartum LBP are multifactorial and include musculoskeletal, hormonal, and structural changes.During pregnancy, hormonal shifts and abdominal expansion lead to stretching and weakening of the abdominal fascia, linea alba, and rectus abdominis, impairing trunk stability and increasing mechanical load on the lumbar spine. A study by Chen et al56 demonstrated that reduced rectus abdominis thickness is significantly associated with an increased risk of postpartum low back pain. Furthermore, according to A. Abde et al,57 machine learning analyses revealed a strong correlation between postpartum low back pain and abnormal trunk movement patterns, particularly limitations in flexion, extension, and lateral bending functions. Pregnancy- and lactation-associated osteoporosis, though rare, is a notable risk for vertebral compression fractures and persistent LBP. Postpartum women with low bone mineral density should receive calcium and vitamin D supplementation and engage in weight-bearing exercises to reduce fracture risk.58,59
The management of postpartum low back pain commonly relies on a multimodal approach, incorporating exercise rehabilitation, physical therapy, and pharmacological interventions. Among these, a study by Saleem et al60 demonstrated that core muscle training—particularly targeting the rectus abdominis—can significantly enhance lumbar stability and reduce pain scores. Additionally, orthopedic manual therapy has shown promising results in alleviating postpartum low back pain, as reported by Schwerla et al,61 although further studies with extended follow-up periods are needed to confirm its long-term efficacy. Traditional therapies are also increasingly utilized in this context. For instance, a study by Akbarzadeh et al54 found that dry cupping therapy applied to the BL23 (Shenshu) acupoint can effectively relieve symptoms, suggesting its potential role as a complementary treatment in postpartum low back pain management. Advanced imaging techniques such as high-frequency ultrasound and shear wave elastography are now used to assess rectus abdominis function and build predictive models for LBP risk.56,57
Pelvic Girdle Pain (PPGP)
Postpartum pelvic girdle pain (PPGP) is a prevalent musculoskeletal disorder during and after pregnancy, often progressing to chronic pain if left unmanaged. Prevalence varies due to inconsistent diagnostic criteria. A study by Vermani et al62 reported that approximately 45% of pregnant women experience pelvic girdle pain during pregnancy, with the majority recovering spontaneously within three months postpartum. Notably, approximately 19% of women still experience PPGP 12 years after delivery.63
The pathophysiology remains unclear but is thought to involve mechanical strain and hormonal effects, particularly elevated relaxin levels, which increase ligament laxity and pelvic joint mobility.62 This instability is considered a major contributor to pain.62,64
Risk factors include a history of LBP, BMI >25, antepartum PPGP, depression, heavy labor, and the need for mobility aids during pregnancy.65–67
In terms of management, PPGP is typically addressed through multimodal interventions, primarily involving non-pharmacological therapies such as physical therapy and exercise training. A study by Gutke et al68 provided strong evidence supporting the beneficial effects of acupuncture and pelvic support belts in the treatment of PPGP. Furthermore, a systematic review by Franke et al69 demonstrated that osteopathic manipulative treatment (OMT) significantly improves pain levels and functional status in women with PPGP. In addition, research by Vleeming et al70 concluded that the current body of scientific evidence is sufficient to recommend appropriate exercise during pregnancy to alleviate or prevent the onset and progression of PPGP.
Discussion
This review provides a comprehensive summary of the epidemiological characteristics, underlying mechanisms, clinical types, and management strategies of persistent postpartum pain. Current evidence indicates that postpartum pain is not merely a short-term complication of childbirth but may progress to chronic or persistent pain, exerting long-lasting effects on women’s quality of life and psychological well-being. However, despite the increasing number of studies in recent years, both the clinical recognition and intervention rates remain relatively low.
At the mechanistic level, multiple factors—including local tissue injury, neural sensitization, hormonal fluctuations, psychosocial influences, and chronic inflammatory responses—are believed to interact and contribute to the onset and persistence of postpartum pain. This complexity highlights the need for future studies to integrate basic and clinical research data and further elucidate the interplay among these mechanisms.
In terms of management, pharmacological therapy remains the cornerstone. Acetaminophen and NSAIDs are widely recommended as first-line options due to their safety and efficacy, while opioids are reserved for short-term use in moderate-to-severe pain to minimize risks of dependence and adverse effects. Regional nerve blocks and epidural analgesia are also widely employed in cesarean delivery and labor analgesia, providing effective acute pain control and reducing systemic medication use. At the same time, non-pharmacological interventions have gained increasing attention as important adjuncts. Physical therapies—such as thermotherapy, cryotherapy, electrical stimulation, ultrasound, and pelvic floor muscle training—help relieve inflammation and muscle tension while promoting tissue repair and functional recovery. Rehabilitation approaches, including progressive exercise and postural correction, support improvement in muscle dysfunction and enhance physical stability. Psychosocial support, including cognitive-behavioral therapy, postpartum education, and family involvement, has also been shown to reduce pain perception and mitigate the risk of chronicity.
Growing evidence suggests that combining pharmacological and non-pharmacological interventions represents a leading approach for individualized pain relief and functional recovery. For instance, routine use of NSAIDs supplemented with early pelvic floor rehabilitation or physical therapy can shorten the duration of pain and improve maternal quality of life. Nevertheless, most existing studies are limited by small sample sizes, short follow-up periods, and the lack of standardized outcome measures, which restrict the generalizability and validation of long-term efficacy. Therefore, future research should prioritize large-scale, multicenter randomized controlled trials to verify the effectiveness and safety of non-pharmacological therapies and combined pharmacological–non-pharmacological approaches. Additionally, efforts should focus on identifying optimal drug dosages, refining regional anesthesia techniques, and optimizing rehabilitation modalities, thereby advancing the development of systematic and precise multimodal management strategies.
Conclusion
Postpartum pain is highly prevalent, diverse in presentation, and exerts a broad impact on women’s health. It manifests not only as acute pain, such as incisional or perineal pain, but also as chronic or persistent pain, imposing a sustained burden on maternal physical and mental well-being and overall quality of life. Epidemiological data reveal substantial variation in the incidence of different pain types, yet the overall burden remains considerable. Although recent advances have been made in assessment tools, mechanistic studies, and therapeutic approaches, multimodal management strategies that combine pharmacological and non-pharmacological interventions have only gradually become a clinical trend. Current practice continues to face major challenges, including a lack of standardized diagnostic criteria, insufficient identification of risk factors, and limited implementation of individualized interventions. Future research priorities should include: (1) establishing standardized, multidimensional systems for pain assessment and classification; (2) further elucidating the pathophysiological mechanisms underlying different types of postpartum pain; and (3) developing evidence-based, comprehensive management pathways with optimized integration of pharmacological and non-pharmacological approaches. Collectively, these efforts may enable earlier identification and more precise interventions for postpartum pain, ultimately improving maternal and neonatal outcomes.
Funding
This research was supported by Jinan Science And Technology Bureau (202328019).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Horvath B, Kloesel B, Cross SN. Persistent postpartum pain - a somatic and psychologic perfect storm. J Pain Res. 2024;17:35–44. doi:10.2147/JPR.S439463
2. Deussen AR, Ashwood P, Martis R, Stewart F, Grzeskowiak LE. Relief of pain due to uterine cramping/involution after birth. Cochrane Database Syst Rev. 2020;10(10):CD004908. doi:10.1002/14651858.CD004908.pub3
3. Uvnäs-Moberg K, Ekström-Bergström A, Berg M, et al. Maternal plasma levels of oxytocin during physiological childbirth - a systematic review with implications for uterine contractions and central actions of oxytocin. BMC Pregnancy Childbirth. 2019;19(1):285. doi:10.1186/s12884-019-2365-9
4. Sultan P, Jensen SE, Taylor J, et al. Proposed domains for assessing postpartum recovery: a concept elicitation study. BJOG. 2022;129:1.
5. Fahey JO. Best practices in management of postpartum pain. J Perinat Neonatal Nurs. 2017;31:126–136. doi:10.1097/JPN.0000000000000241
6. Sultan P, Ando K, Sultan E, et al. A systematic review of patient-reported outcome measures to assess postpartum pain using consensus based standards for the selection of health measurement instruments (cosmin) guidelines. Br J Anaesth. 2021;127(2):264–274. doi:10.1016/j.bja.2021.03.035
7. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: visual analog scale for pain (VAS Pain), numeric rating scale for pain (NRS Pain), mcgill pain questionnaire (MPQ), short-form mcgill pain questionnaire (SF-MPQ), chronic pain grade scale (CPGS), short form-36 bodily pain scale (SF-36 BPS), and measure of intermittent and constant osteoarthritis pain (ICOAP). Arthritis Care Res. 2011;63(11):S240–S252.
8. Zhao X, Liu B, Zhang Q, Wang H, Tian Y, Wang F. Moxibustion for uterine contraction pain: a protocol for systematic review and meta-analysis. Medicine. 2022;101(48):e32195. doi:10.1097/MD.0000000000032195
9. Fang X, Huan Y, Tao Y, et al. Incidence, severity, and determinants of uterine contraction pain after vaginal delivery: a prospective observational study. Int J Obstet Anesth. 2021;46:102961. doi:10.1016/j.ijoa.2021.102961
10. Holdcroft A, Snidvongs S, Cason A, Doré CJ, Berkley KJ. Pain and uterine contractions during breast feeding in the immediate post-partum period increase with parity. Pain. 2003;104(3):589–596. doi:10.1016/S0304-3959(03)00116-7
11. Wen L, Hilton G, Carvalho B. The impact of breastfeeding on postpartum pain after vaginal and cesarean delivery. J Clin Anesth. 2015;27(1):33–38. doi:10.1016/j.jclinane.2014.06.010
12. Eshkevari L, Trout KK, Damore J. Management of postpartum pain. J Midwifery Women’s Health. 2013;58(6):622–631. doi:10.1111/jmwh.12129
13. Mo X, Zhao T, Chen J, et al. Programmed intermittent epidural bolus in comparison with continuous epidural infusion for uterine contraction pain relief after cesarean section: a randomized, double-blind clinical trial. Drug Des Devel Ther. 2022;16:999–1009. doi:10.2147/DDDT.S350418
14. Zheng K, Chen B, Sun J. Nalbuphine may be superior to sufentanil in relieving postcesarean uterine contraction pain in multiparas: a retrospective cohort study. Drug Des Devel Ther. 2023;17:1405–1415. doi:10.2147/DDDT.S394664
15. de Sousa L, Gomes-Sponholz FA, Nakano AMS. Transcutaneous electrical nerve stimulation for the relief of post-partum uterine contraction pain during breast-feeding: a randomized clinical trial. J Obstetr Gynaecol Res. 2014;40(5):1317–1323. doi:10.1111/jog.12345
16. Andrews V, Thakar R, Sultan AH, Jones PW. Evaluation of postpartum perineal pain and dyspareunia--a prospective study. Eur J Obstet Gynecol Reprod Biol. 2008;137(2):152–156. doi:10.1016/j.ejogrb.2007.06.005
17. Bretelle F, Fabre C, Golka M, et al. Capacitive-resistive radiofrequency therapy to treat postpartum perineal pain: a randomized study. PLoS One. 2020;15(4):e0231869. doi:10.1371/journal.pone.0231869
18. Manresa M, Pereda A, Goberna-Tricas J, Webb SS, Terre-Rull C, Bataller E. Postpartum perineal pain and dyspareunia related to each superficial perineal muscle injury: a cohort study. Int Urogynecol J. 2020;31(11):2367–2375. doi:10.1007/s00192-020-04317-1
19. Shepherd E, Grivell RM. Aspirin (single dose) for perineal pain in the early postpartum period. Cochrane Database Syst Rev. 2020;7(7):CD012129. doi:10.1002/14651858.CD012129.pub3
20. Wuytack F, Smith V, Cleary BJ. Oral non-steroidal anti-inflammatory drugs (single dose) for perineal pain in the early postpartum period. Cochrane Database Syst Rev. 2021;1(1):CD011352. doi:10.1002/14651858.CD011352.pub3
21. Abalos E, Sguassero Y, Gyte GM. Paracetamol/Acetaminophen (single administration) for perineal pain in the early postpartum period. Cochrane Database Syst Rev. 2021;1(1):CD008407. doi:10.1002/14651858.CD008407.pub3
22. Abu-Zaid A, Alomar O, Abuzaid M, et al. Ropivacaine versus lidocaine infiltration for postpartum perineal pain: a systematic review and meta-analysis. J Gynecol Obstetr Human Reproduct. 2021;50(8):102074. doi:10.1016/j.jogoh.2021.102074
23. Kurnaz D, Fışkın SG, Demirgöz Bal M. The effect of postpartum interventions on healing and pain in women with perineal trauma: a systematic review and meta-analysis. Int J Nurs Stud. 2025;162:104976. doi:10.1016/j.ijnurstu.2024.104976
24. Francisco AA, De Oliveira SMJV, Steen M, Nobre MRC, De Souza EV. Ice pack induced perineal analgesia after spontaneous vaginal birth: randomized controlled trial. Women Birth. 2018;31(5):e334–e340. doi:10.1016/j.wombi.2017.12.011
25. Abdelhakim AM, Eldesouky E, Elmagd IA, et al. Antenatal perineal massage benefits in reducing perineal trauma and postpartum morbidities: a systematic review and meta-analysis of randomized controlled trials. Int Urogynecol J. 2020;31(9):1735–1745. doi:10.1007/s00192-020-04302-8
26. Şolt Kirca A, Kanza Gul D. The effect of acupressure applied to points lv4 and li4 on perceived acute postpartum perineal pain after vaginal birth with episiotomy: a randomized controlled study. Arch Gynecol Obstetrics. 2020;301(2):473–481. doi:10.1007/s00404-020-05439-z
27. Filippini M, Farinelli M, Lopez S, Ettore C, Gulino FA, Capriglione S. Postpartum perineal pain: may the vaginal treatment with CO2 laser play a key-role in this challenging issue? J Maternal-Fetal Neonatal Med. 2021;34(8):1190–1197. doi:10.1080/14767058.2019.1628208
28. Amir LH, Baeza C, Charlamb JR, Jones W. Identifying the cause of breast and nipple pain during lactation. BMJ. 2021;374:n1628. doi:10.1136/bmj.n1628
29. Leung SS. Breast pain in lactating mothers. Hong Kong Med J. 2016;22(4):341–346. doi:10.12809/hkmj154762
30. Betts RC, Johnson HM, Eglash A, Mitchell KB. It’s not yeast: retrospective cohort study of lactating women with persistent nipple and breast pain. Breastfeeding Med. 2021;16(4):318–324. doi:10.1089/bfm.2020.0160
31. Betzold CM. Results of microbial testing exploring the etiology of deep breast pain during lactation: a systematic review and meta-analysis of nonrandomized trials. J Midwifery Women’s Health. 2012;57(4):353–364. doi:10.1111/j.1542-2011.2011.00136.x
32. Han S, Kim B, Park H. Auricular acupressure on breast pain among breastfeeding mothers receiving gentle hand techniques: a randomized, single-blind, sham-controlled trial. J Hum Lact. 2024;40(2):248–258. doi:10.1177/08903344241228545
33. Amir LH, Donath SM, Garland SM, et al. Does Candida and/or Staphylococcus play a role in nipple and breast pain in lactation? A cohort study in Melbourne, Australia. BMJ open. 2013;3(3):e002351. doi:10.1136/bmjopen-2012-002351
34. Çağan ES, Taşkın R, Solmaz E, Balcı R, Eminov E. The effect of oketani massage on breastfeeding success and breast engorgement in mothers delivering by cesarean section: randomized controlled study. Afr J Reprod Health. 2025;29(3):85–93. doi:10.29063/ajrh2025/v29i3.11
35. Åhlund S, Rådestad I, Zwedberg S, Lindgren H. Perineal pain the first year after childbirth and uptake of post-partum check-up- a Swedish cohort study. Midwifery. 2019;78:85–90. doi:10.1016/j.midw.2019.08.004
36. Huber M, Larsson C, Lehmann J-P, Strigård K, Lindam A, Tunón K. Sonographic postpartum anal sphincter defects and the association with pelvic floor pain and dyspareunia. Acta Obstet Gynecol Scand. 2023;102(10):1290–1297. doi:10.1111/aogs.14606
37. Ma Y, Zhang X, Wu G, Wu L, Ma Y, Zhang X. Evaluating the effectiveness of radiofrequency therapy and manual pelvic fascial release in treating myofascial pelvic pain. Int Urogynecol J. 2024;35(6):1219–1225. doi:10.1007/s00192-024-05763-x
38. Woodley SJ, Lawrenson P, Boyle R, et al. Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst Rev. 2020;5(5):CD007471. doi:10.1002/14651858.CD007471.pub4
39. Buurman MBR, Lagro-Janssen ALM. Women’s perception of postpartum pelvic floor dysfunction and their help-seeking behaviour: a qualitative interview study. Scand J Caring Sci. 2013;27(2):406–413. doi:10.1111/j.1471-6712.2012.01044.x
40. Li S-H, Wu Y-D, Wu -Y-Y, et al. Autologous fat transplantation for the treatment of abdominal wall scar adhesions after cesarean section. J Plast Surg Hand Surg. 2021;55(4):210–215. doi:10.1080/2000656X.2020.1856675
41. Qin Y, Yang Y, Qin S, Xiong Z. Regional nerve block in postoperative analgesia after cesarean section: a narrative review. Medicine. 2024;103(52):e41159. doi:10.1097/MD.0000000000041159
42. Nitsche J, Howell C, Howell T. Skin closure with subcuticular absorbable staples after cesarean section is associated with decreased analgesic use. Arch Gynecol Obstetrics. 2012;285(4):979–983. doi:10.1007/s00404-011-2121-5
43. Ibrahim MI, Moustafa GF, Al-Hamid ASA, Hussein MR. Superficial incisional surgical site infection rate after cesarean section in obese women: a randomized controlled trial of subcuticular versus interrupted skin suturing. Arch Gynecol Obstetrics. 2014;289(5):981–986. doi:10.1007/s00404-013-3098-z
44. de Queiroz VKP, da Nóbrega Marinho AM, de Barros GAM. Analgesic effects of a 5% lidocaine patch after cesarean section: a randomized placebo-controlled double-blind clinical trial. J Clin Anesthesia. 2021;73:110328. doi:10.1016/j.jclinane.2021.110328
45. Garmi G, Parasol M, Zafran N, Rudin M, Romano S, Salim R. Efficacy of single wound infiltration with bupivacaine and Adrenaline during cesarean delivery for reduction of postoperative pain: a randomized clinical trial. JAMA Netw Open. 2022;5(11):e2242203. doi:10.1001/jamanetworkopen.2022.42203
46. Bjelland Engdahl BEK, Stuge B, Eberhard-Gran M, Eberhard‐Gran M. The effect of emotional distress on persistent pelvic girdle pain after delivery: a longitudinal population study. BJOG. 2013;120(1):32–40. doi:10.1111/1471-0528.12029
47. Valinger Aggeryd K, Bergström C, Mogren I, Persson M. A limited life - a mixed methods study on living with persistent pregnancy-related lumbopelvic pain more than 12 years postpartum in Sweden. Disability Rehabil. 2022;44(13):3062–3070. doi:10.1080/09638288.2020.1852447
48. Sjödahl J, Gutke A, Öberg B. Predictors for long-term disability in women with persistent postpartum pelvic girdle pain. Eur Spine J. 2013;22(7):1665–1673. doi:10.1007/s00586-013-2716-6
49. Yurashevich M, Cooter WM, Sims SC, et al. Inflammatory changes in the plasma and cerebrospinal fluid of patients with persistent pain and postpartum depression after elective cesarean delivery: an exploratory prospective cohort study. Canad J Anaesthes J Canad D’anesthesie. 2023;70(12):1917–1927. doi:10.1007/s12630-023-02603-2
50. Capobianco R, Cher D. Safety and effectiveness of minimally invasive sacroiliac joint fusion in women with persistent post-partum posterior pelvic girdle pain: 12-month outcomes from a prospective, multi-center trial. SpringerPlus. 2015;4(1):570. doi:10.1186/s40064-015-1359-y
51. Eisenach JC, Pan PH, Smiley R, Lavand’homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94. doi:10.1016/j.pain.2008.07.011
52. Stuge B, Laerum E, Kirkesola G, Vøllestad N. The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: a randomized controlled trial. Spine. 2004;29(4):351–359. doi:10.1097/01.BRS.0000090827.16926.1D
53. Mogren IM. Does caesarean section negatively influence the post-partum prognosis of low back pain and pelvic pain during pregnancy? Eur Spine J. 2007;16(1):115–121. doi:10.1007/s00586-006-0098-8
54. Akbarzadeh M, Ghaemmaghami M, Yazdanpanahi Z, Zare N, Azizi A, Mohagheghzadeh A. The effect dry cupping therapy at acupoint bl23 on the intensity of postpartum low back pain in primiparous women based on two types of questionnaires, 2012; a randomized clinical trial. Int J Community Based Nurs Midwifery. 2014;2(2):112–120.
55. Tavares P, Barrett J, Hogg-Johnson S, et al. Prevalence of low back pain, pelvic girdle pain, and combination pain in a postpartum Ontario population. JOGC. 2020;42:473–480.
56. Chen H, Lin Y, Cai Y, Liao J. Evaluation of rectus abdominis muscle using high-frequency ultrasound and shear wave elastography to construct a risk prediction model for postpartum low back pain. Acad Radiol. 2025;32(2):899–906. doi:10.1016/j.acra.2024.10.041
57. Abdel Hady A, Abd El-Hafeez D. Utilizing machine learning to analyze trunk movement patterns in women with postpartum low back pain. Sci Rep. 2024;14(1):18726. doi:10.1038/s41598-024-68798-6
58. Karadeli E, Uslu N. Postpartum sacral fracture presenting as lumbar pain. J Women’s Health. 2009;18(5):663–665. doi:10.1089/jwh.2008.1189
59. Terzi R, Terzi H, Özer T, Kale A. A rare cause of postpartum low back pain: pregnancy- and lactation-associated osteoporosis. Biomed Res Int. 2014;2014:287832. doi:10.1155/2014/287832
60. Saleem Z, Khan AA, Farooqui SI, Yasmeen R, Rizvi J. Effect of exercise on inter-recti distance and associated low back pain among post-partum females: a randomized controlled trial. J Family Reprod Health. 2021;15(3):202–209. doi:10.18502/jfrh.v15i3.7139
61. Schwerla F, Rother K, Rother D, Ruetz M, Resch K-L. Osteopathic manipulative therapy in women with postpartum low back pain and disability: a pragmatic randomized controlled trial. J Am Osteopathic Assoc. 2015;115(7):416–425. doi:10.7556/jaoa.2015.087
62. Vermani E, Mittal R, Weeks A. Pelvic girdle pain and low back pain in pregnancy: a review. Pain Practice. 2010;10(1):60–71. doi:10.1111/j.1533-2500.2009.00327.x
63. Bergström C, Persson M, Nergård K-A, Mogren I. Prevalence and predictors of persistent pelvic girdle pain 12 years postpartum. BMC Musculoskelet Disord. 2017;18(1):399. doi:10.1186/s12891-017-1760-5
64. Casagrande D, Gugala Z, Clark SM, Lindsey RW. Low back pain and pelvic girdle pain in pregnancy. J Am Acad Orthop Surg. 2015;23(9):539–549. doi:10.5435/JAAOS-D-14-00248
65. Wiezer M, Hage-Fransen MAH, Otto A, et al. Risk factors for pelvic girdle pain postpartum and pregnancy related low back pain postpartum; a systematic review and meta-analysis. Musculoskelet Sci Pract. 2020;48:102154. doi:10.1016/j.msksp.2020.102154
66. Aldabe D, Ribeiro DC, Milosavljevic S, Dawn Bussey M. Pregnancy-related pelvic girdle pain and its relationship with relaxin levels during pregnancy: a systematic review. Eur Spine J. 2012;21(9):1769–1776. doi:10.1007/s00586-012-2162-x
67. Burani E, Marruganti S, Giglioni G, Bonetti F, Ceron D, Cozzi Lepri A. Predictive factors for pregnancy-related persistent pelvic girdle pain (PPGP): a systematic review. Medicina. 2023;60:59. doi:10.3390/medicina60010059
68. Gutke A, Betten C, Degerskär K, Pousette S, Olsén MF. Treatments for pregnancy-related lumbopelvic pain: a systematic review of physiotherapy modalities. Acta Obstet Gynecol Scand. 2015;94(11):1156–1167. doi:10.1111/aogs.12681
69. Franke H, Franke J-D, Belz S, Fryer G. Osteopathic manipulative treatment for low back and pelvic girdle pain during and after pregnancy: a systematic review and meta-analysis. J Bodyw Mov Ther. 2017;21:752–762. doi:10.1016/j.jbmt.2017.05.014
70. Vleeming A, Albert HB, Ostgaard HC, Sturesson B, Stuge B. European guidelines for the diagnosis and treatment of pelvic girdle pain. Eur Spine J. 2008;17(6):794–819. doi:10.1007/s00586-008-0602-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Balanced Opioid-Free Anesthesia on Chronic Postsurgical Pain After Video-Assisted Thoracoscopic Surgery: A Randomized Controlled Trial Protocol
Huo WW, Qian J, Zhao HX, Dou W, Chen SM, Ji FH, Peng K
Journal of Pain Research 2025, 18:2459-2466
Published Date: 15 May 2025