Back to Journals » Journal of Pain Research » Volume 13
Pain Diagnosis, Pain Coping, and Function in Individuals with Chronic Musculoskeletal Pain
Authors Ferreira-Valente A ![]() , Queiroz-Garcia I
, Queiroz-Garcia I ![]() , Pais-Ribeiro J
, Pais-Ribeiro J ![]() , Jensen MP
, Jensen MP ![]()
Received 26 October 2019
Accepted for publication 7 March 2020
Published 22 April 2020 Volume 2020:13 Pages 783—794
DOI https://doi.org/10.2147/JPR.S236157
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Alexandra Ferreira-Valente,1,2 Inês Queiroz-Garcia,1 José Pais-Ribeiro,1 Mark P Jensen2
1William James Center for Research, ISPA – Instituto Universitário, Lisbon, Portugal; 2Department of Rehabilitation Medicine, University of Washington, Seattle, WA, USA
Correspondence: Alexandra Ferreira-Valente
William James Center for Research, ISPA - Instituto Universitário, Rua Jardim do Tabaco, no 34, Lisbon 1149-041, Portugal
Tel +351 969082988
Fax +351 218860954
Email [email protected]
Purpose: Research supports a role for coping responses in adjustment to chronic pain. However, it is likely that some coping responses play a larger role in adjustment to pain for some individuals than others. The identification of the factors that moderate the association between coping responses and pain-related outcomes has important clinical implications. This study sought to determine if musculoskeletal pain diagnosis moderates the associations between eight pain-coping responses and both pain and function.
Patients and Methods: A non-probabilistic sample of 323 persons with different chronic musculoskeletal pain conditions completed measures of pain intensity, physical function, psychological function, and pain-coping responses.
Results: With only one exception, the frequency of use of pain-coping responses was not associated with pain diagnosis. Statistically significant moderation effects of pain diagnosis on the association between coping and pain outcomes were found for two coping responses: 1) support seeking when predicting pain intensity, and 2) resting when predicting both physical and psychological function.
Conclusion: The findings indicate that coping responses tend to play a similar role in patients’ pain and function across different musculoskeletal pain conditions, with some important exceptions. If the findings are found to replicate in other samples, they would have important implications for determining when psychosocial pain treatments might (and when they might not) need to be adapted for specific diagnostic groups.
Keywords: pain etiology, moderation effect, coping responses, pain, physical function, psychological function
Introduction
Chronic pain is a significant health problem estimated to affect about 20% to 30% of the world population.1,2 It is associated with significant costs to society, to individuals with chronic pain, and their families, often interfering significantly with many aspects of the person with chronic pain’s life.1,3-7
Chronic pain is a multidimensional subjective experience influenced by biological, psychological, and social factors.8–15 Pain-coping responses are among the psychological factors that have been shown to play an important role in adjustment to chronic pain.6,8,9,16,17 Coping can be defined as the thoughts and behaviors a person has and engages in to manage pain and its impact. Coping has been shown to be associated with measures of physical and psychological function, and treatment-related changes in coping responses have been shown to be associated with treatment outcomes in individuals with chronic pain.9,11,16–20
Those coping responses most strongly and consistently associated with function include responses that tend to be associated with worse function (eg, guarding, resting, praying/hoping and asking for assistance) and those that tend to be associated with better function (eg, task persistence).9,16,21-23 Recent research suggests that pain severity, its impact on function, and response to multidisciplinary pain treatment vary to some extent as a function of the etiology of the pain.3,14,24,25 Moreover, limited research suggests that pain diagnosis may moderate the association between psychosocial factors and physical and psychological function.26,27
These findings support the possibility that the role that a coping response plays in an individual’s adjustment to chronic pain may be influenced by a variety of factors, including pain diagnosis. For example, the use of relaxation may play an important role in preventing or reducing the impact of headache,28 while relaxation may play only a minor role in preventing or reducing the impact of low back pain.29
Research regarding the moderating impact of pain diagnosis on the associations between coping and pain-related outcomes would have important research and clinical implications. If a moderation effect of pain diagnosis on the effects of coping is found, this knowledge could inform decisions regarding the coping responses that should be encouraged or taught, or discouraged, in different diagnostic groups. On the other hand, if it turns out that pain diagnosis is found to have little or no moderation effects on the association between coping and pain-related outcomes, we could be confident that psychosocial intervention programs that teach and encourage coping responses thought to be adaptive and that discourage coping responses thought to be maladaptive would have similar beneficial effects for individuals with chronic pain, regardless of pain diagnosis. However, research examining the moderating role of pain diagnosis on the associations between psychological factors (eg, pain-coping responses, catastrophizing, solicitous response from significant others) and measures of adjustment to chronic pain is still in its infancy.27
This study sought to address this knowledge gap. Specifically, this study aims to [1] compare pain diagnosis groups with respect to the frequency of use of different pain-coping responses and [2] evaluate the moderating effects of pain diagnosis on the associations between coping and pain and function in a sample of individuals with a variety of chronic musculoskeletal pain diagnoses (ie, Osteoarthrosis, Rheumatoid Arthritis, Ankylosing Spondylitis, Disc Hernia, and “other” musculoskeletal conditions). To address this question, we used data from an earlier study that examined the direct associations between pain-coping responses and three pain-related outcomes (ie, pain intensity, physical function and psychological function) in a sample of patients of chronic musculoskeletal pain.9 We hypothesized that pain diagnosis would moderate the association between some pain-coping responses and pain-related outcomes (ie, pain intensity, physical function and psychological function; see Figure 1). However, we did not have any a priori hypotheses regarding which diagnostic groups would demonstrate stronger versus weaker associations between specific coping responses and the criterion variables, given the lack of previous research in this area.
 |
Figure 1 Hypothesized moderation models. |
Material and Methods
This is an observational correlational study using a cross-sectional design.
Participants
Minimum sample size required to perform the moderation analysis factor analysis using structural using ordinary least squares (OLS) multiple linear regression-based trajectory analyses was determined using an a priori power calculation, as described below. This calculation indicated that 89 participants would be needed to be able to detect significant effects. Participants were 323 adults with chronic musculoskeletal pain who were outpatients of one of seven Portuguese health institutions (namely, Hospital de Ovar – Dr. Francisco Zagalo, Centro de Medicina de Reabilitação do Alcoitão, Hospital S. João de Deus, Hospital da Prelada, Hospital Infante D. Pedro, Centro de Reabilitação de São Jorge, and Serviço de Medicina Física e Reabilitação da Associação Nacional de Espondilite Anquilosante). Study inclusion criteria were: [1] being at least 18 years old; [2] experiencing pain for at least 3 months due to a musculoskeletal condition; [3] absence of a physical disability that would prevent study participation; and [4] absence of dementia and cognitive impairment, or of a significant psychopathology. Patients with a diagnosis of fibromyalgia were also excluded from the study, as recommended by the healthcare providers involved in the identification of prospective participants, due to both the uncertainty of fibromyalgia’s etiology as well as the need to avoid confounding effects that might arise from the high comorbidity of this condition with depression and other psychopathologies.30,31
The majority of the participants were women (n = 213, 66%). Mean age was 61.02 years (SD = 15.23, range = 18 to 90 years). Education level was low, with the plurality of the participants having attended only primary education (n = 149, 46%); 2% (n = 5) reported that they had never been to school. The majority of the participants were married or living with a significant other (n = 200, 62%), 16% were widowed (n = 52), 14% were single (n = 45), and 8% were divorced or separated (n = 26). Thirty-one percent of the participants had osteoarthrosis (n = 99), 18% had ankylosing spondylitis (n = 57), 10% had a disc hernia (n = 33), 9% had rheumatoid arthritis (n = 31), and 32% had some other musculoskeletal condition (such as osteoporosis or scoliosis; n=103). The majority of the participants had chronic pain for at least 2 years (n = 223, 69%), with 38% (n = 123) reporting to have pain for more than 10 years.
Measures
Participants were asked to complete a sociodemographic and clinical history questionnaire (sex, age, marital status, education level, pain duration), as well as measures of pain intensity, physical function, psychological function and pain-coping responses.
Pain Intensity
Average pain intensity in the previous 24 h was assessed using a 0–10 Numerical Rating Scale (NRS), where 0 indicated “No pain” and 10 indicated “Worst imaginable pain.” Previous research supports the validity and responsivity of the NRS as a measure of pain intensity.32,33 Previous research also supports the test–retest reliability [intraclass correlation coefficient (95% CI) of 0.95 (0.93–0.96)] of the 0–10 NRS.34
Physical and Psychological Function
Physical and psychological function was assessed with the Portuguese Medical Outcomes Study 12-item Short Form Health Survey (SF-12).35–37 The SF-12 provides a Physical Component Summary (PCS) score and a Mental Component Summary (MCS) score ranging from 0 to 100, with higher scores indicating better physical and psychological function, respectively. Previous research supports the validity and reliability of the Portuguese SF-1235–37 and establishes the norms for the healthy general population. The median values for the Portuguese healthy adult population, according to Pais-Ribeiro, are 76 for the PCS and 71.42 for the MCS.38
Pain Coping Responses
The frequency of use of a number of commonly used pain-coping responses was assessed with the Portuguese version of the brief (16 item, 2 items per scale) version of the Chronic Pain Coping Inventory (CPCI-16).16,39 The CPCI-16 items assess eight pain coping domains: Guarding (ie, limiting or restricting the movement of body parts), Resting (ie, engaging in pain-contingent resting activities, such as lying or sitting down), Asking for Assistance (ie, asking for help with an activity, such as a household chore), Relaxation (ie, using a relaxation strategy, such as listening to music), Task Persistence (ie, continuing with activities despite pain), Exercise/Stretch (ie, engaging in muscle stretching/strengthening activities), Support Seeking (ie, talking or get-together with someone), Coping Self-statements (ie, thinking positive thoughts on purpose about a certain problem and one’s ability to cope with it). Respondents are asked to indicate the number of days (in the past seven) that they used (at least once) each strategy to cope with pain. Responses to the two items for each scale are averaged into a single score representing the coping domain assessed by those items; scores can range from 0 to 7, with higher scores indicating a more frequent use of the coping response. Previous research supports the validity and reliability of the subscales of the original version of the CPCI (0.71 < α <0.91; test–retest reliability of 0.60 to 0.83 for a 4-week interval), both for the English and Portuguese versions of the CPCI.40–46 The validity of the subscales of the CPCI-16 has been supported by: [1] their strong correlations (r ≥ 0.70) with the corresponding subscales of the original version of the CPCI; [2] the patterns of associations with pain, disability and depression; and [3] the ability to detect statistically significant differences as a result of a psychosocial intervention when compared to pre-treatment scores.21 Previous research has also supported the concurrent validity of the Portuguese versions of the CPCI-16.16,39
Procedures
A non-probabilistic sample of Portuguese adults experiencing pain for at least 3 months due to a musculoskeletal condition was recruited among the outpatients of the above-mentioned health institutions. A healthcare provider from each of the above-mentioned health institutions identified prospective participants meeting the inclusion criteria and confirmed their pain-related diagnosis prior to invitation to participate. Prospective participants were invited to participate while waiting for the physical therapy session to start. All prospective participants were informed of the study aims and procedures, were given the opportunity to ask any questions they had about the study, and were assured anonymity and confidentiality. Those potential participants who expressed a willingness to participate were asked to provide written informed consent and then complete the study measures. The study procedures were reviewed and approved by the Ethics review boards of seven healthcare institutions in Portugal. The study was conducted in accordance with the Declaration of Helsinki.
Data Analysis
The minimum sample size recommended to detect a significant effect in moderation analysis using ordinary least squares (OLS) multiple linear regression-based trajectory analyses was determined using an a priori power calculation using an online calculator, assuming a medium effect size of 0.15 (Cohen’s f2; based on previous research showing moderating effects of demographic variables in the association between measures of coping and function in other samples of individuals with chronic pain), an alpha level of 0.05, and power of 0.8.47–49 We first computed frequencies and percentages (categorical variables) and means and standard deviations (continuous variables) of the study measures, both for the entire sample and by diagnostic group for descriptive purposes. Differences between the diagnostic groups in coping responses and the study criterion variables (ie, pain intensity, physical function, and psychological function) were tested using a one-way ANOVAs, with the coping and study criterion variables as the dependent variables, and diagnosis group as the independent variable. Prior to these analyses, we evaluated test assumptions (normality and homogeneity of variances), with Levene’s test and by computing skewness (Sk) and kurtosis (Ku), with values of Sk and Ku lower than 3 and 10, respectively, indicating an absence of severe deviance from the normal distribution.50,51 If a significant diagnosis group effect was found, we planned to perform between-diagnosis comparisons using post hoc Bonferroni difference tests. Effect sizes were estimated using η2p.52 Finally, to test the hypothesized moderation effect of pain diagnosis on the associations between the measure of pain coping and the criterion measures, were performed moderation analysis using OLS multiple linear regression-based trajectory analyses. Moderation effects were estimated and probed using PROCESS macro for SPSS (v. 3.2, freely available at http://www.afhayes.com), as described by Hayes53 and Hayes and Matthes,54 using 5000 bootstrap samples with a 95% confidence interval, and HC3 Davidson-MacKinnon estimator as the heteroscedasticity-consistent standard error and covariance matrix estimator.55,56 The multicategorical moderator (ie, five pain diagnoses) was indicator-coded into five levels, using the group of participants with other musculoskeletal conditions as the indicator. Sex and age were included as covariates.53,57 Because each coping domain is computed as an average of only two items, missing data from any of the coping scales resulted in that scale score being excluded from the analyses. Seven participants did not provide information about their age. Missing values relative to participants’ age were replaced with the series mean.58 All statistical analyses were performed using IBM SPSS Statistics (v. 25, SPSS Inc., Chicago, IL). Alpha was set at 0.05 for all analyses.
Results
Description of the Study Participants and Study Variables
Tables 1 and 2 present descriptive information for the study measures for the total sample and for each diagnostic group. As can be seen, the sample was characterized by moderate levels of pain and significant physical and psychological dysfunction in comparison with the Portuguese healthy adult population [PCS: t(312) = 29.15; p < 0.001; d = 1.65; MCS: t(312) = 13.09; p < 0.001; d = 0.74]. CPCI Coping Self-Statements (M = 4.35, SD = 2.05), CPCI Exercise/Stretch (M = 3.92, SD = 2.18) and CPCI Task Persistence (M = 3.90, SD = 2.29) were the most frequently used coping responses, while the least frequently used coping responses were CPCI Seeking Support (M = 2.63, SD = 2.45) and CPCI Asking for Assistance (M = 2.69, SD = 2.39).
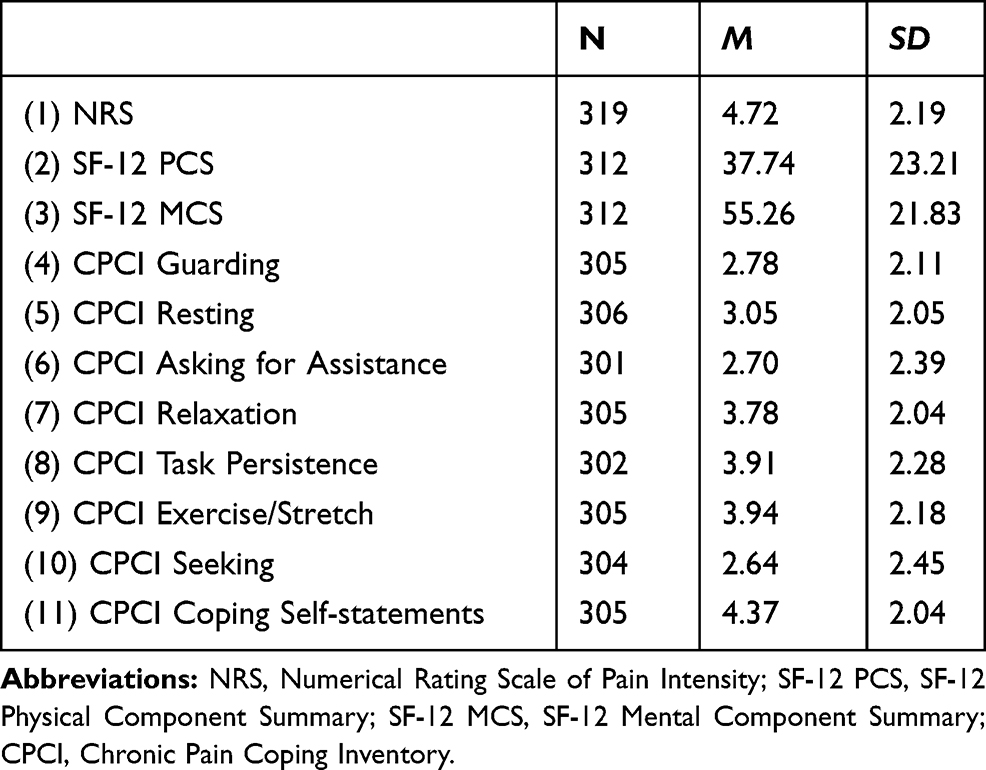 |
Table 1 Descriptive Statistics for the Study Variables, for the Total Sample |
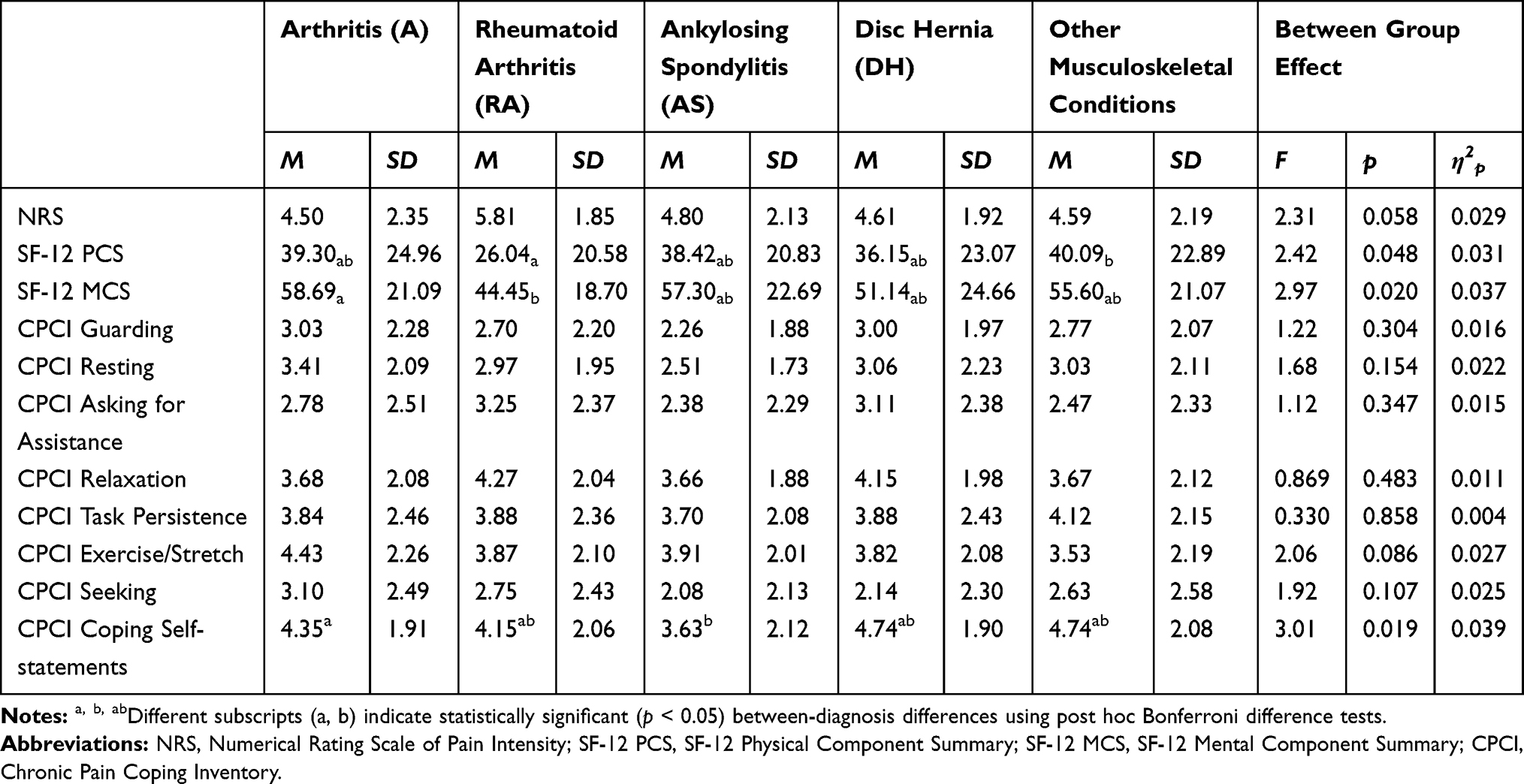 |
Table 2 Descriptive Statistics of the Study Variables by Pain Diagnosis |
Pain intensity and the frequency of use of all but one pain-coping response were not significantly different between the pain diagnosis categories. There were statistically significant differences, albeit with small effect sizes, with respect to physical function [F(4, 307) = 2.42; p = 0.048; ηp2 = 0.031; π = 0.693], psychological function [F(4, 307) = 2.97; p = 0.020; ηp2 = 0.037; π = 0.793], and the frequency of use of coping self-statements as a pain-coping response [F(4, 300) = 3.01; p = 0.019; ηp2 = 0.039; π = 0.797]. Participants with rheumatoid arthritis (SF-12 PCS: M = 26.04, SD = 20.58; SF-12 MCS: M = 44.45, SD = 18.70) reported worse physical function than those with other musculoskeletal conditions (SF-12 PCS: M = 40.09, SD = 22.89), and worse psychological function than participants with osteoarthrosis (SF-12 MCS: M = 58.69, SD = 21.09). Finally, participants with osteoarthrosis reported greater frequency of use of coping self-statements (CPCI Coping Self-statements: M = 4.35, SD = 1.91) than participants with ankylosing spondylitis (CPCI Coping Self-statements: M = 3.63, SD = 2.12).
Pain Diagnosis Moderation Effects
The results of the OLS multiple linear regression analyses are summarized in Table 3. As can be seen, variables entered in Step 1 accounted for from 12% (for CPCI Task Persistence subscale) to 15% (for CPCI Asking for Assistance subscale) of the variance of pain intensity, from 15% (for CPCI Task Persistence subscale) to 37% (for CPCI Asking for Assistance subscale) of the variance of physical function, and from 13% (for CPCI Task Persistence subscale) to 22% (for CPCI Resting subscale) of the variance of psychological function. A statistically significant moderation effect of pain diagnosis was found in only for three [13%] out of 24 OLS regression analyses. Interaction effects were found for CPCI Seeking subscale when predicting pain intensity (ΔR2 = 0.024, p = 0.039), and for CPCI Resting subscale when predicting both physical (ΔR2 = 0.027, p = 0.017) and psychological function (ΔR2 = 0.03, p = 0.018). Conditional effects of significant interaction effects are depicted in Figure 2.
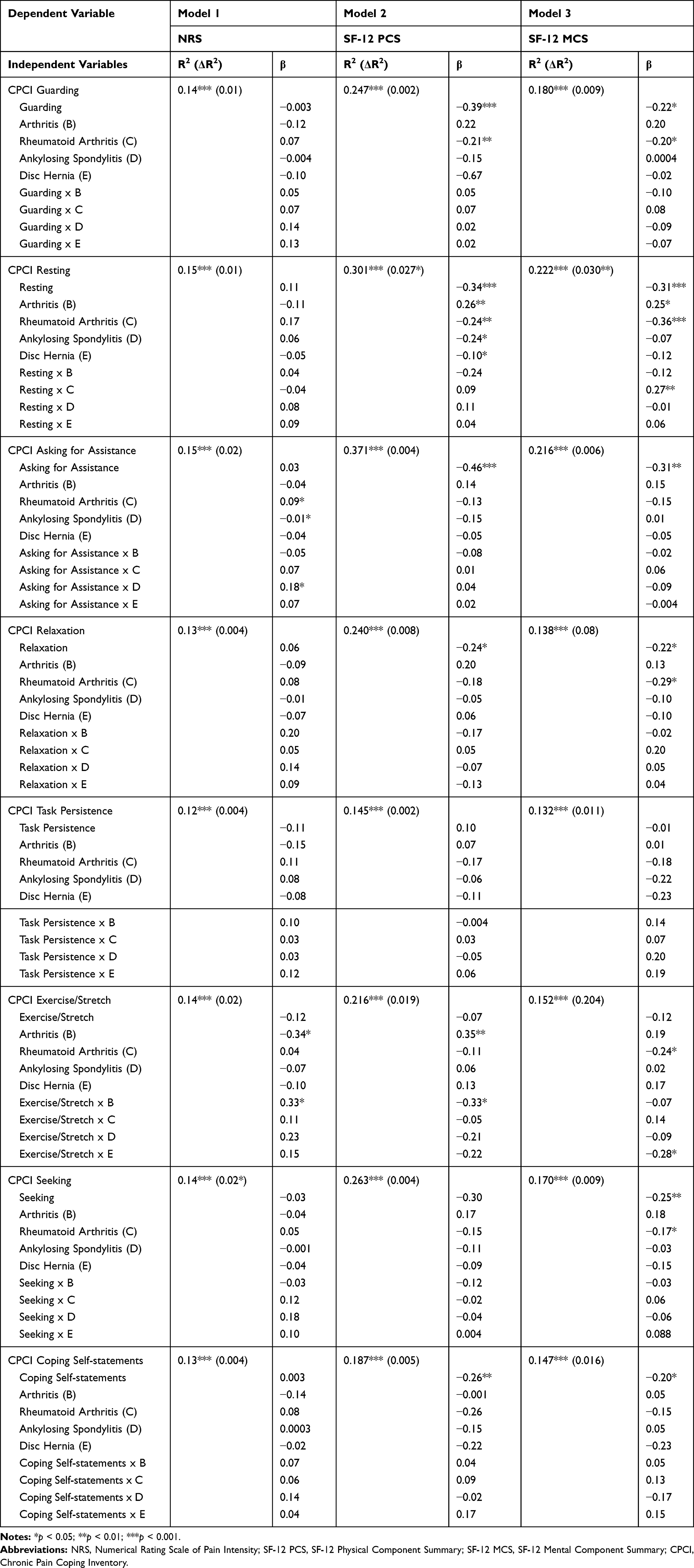 |
Table 3 Ordinary Least Squares Regression Models Coefficients |
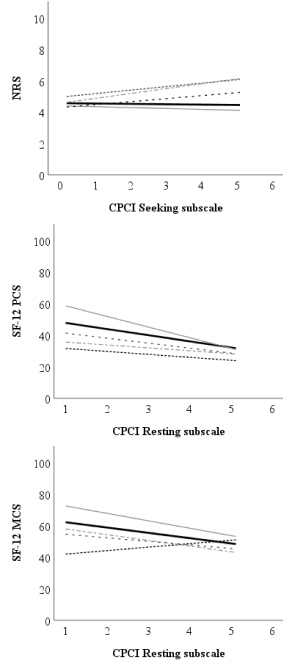





The probe of the statistically significant interaction effects revealed that CPCI Seeking subscale predicted increases in pain intensity for participants with rheumatoid arthritis [b = 0.023, t(291) = 2.06, p = 0.041], and ankylosing spondylitis [b = 0.311, t(291) = 2.87, p = 0.004], but not for participants with osteoarthrosis [b = −0.058, t(291) = 0.60, p = 0.552], disc hernia [b = 0.191, t(291) = 1.19, p = 0.237], and other musculoskeletal conditions [b = −0.023, t(291) = 0.28, p = 0.782]. On the other hand, CPCI Resting subscale predicted decreases in physical function among individuals with osteoarthrosis [b = −6.76, t(290) = 6.82, p < 0.001] and of other musculoskeletal conditions [b = −3.91, t(290) = 4.18, p < 0.001], but not at pain diagnosis of rheumatoid arthritis [b = −1.89, t(290) = 1.27, p = 0.204], ankylosing spondylitis [b = −1.84, t(290) = 1.30, p = 0.196] and disc hernia [b = −3.17, t(290) = 1.67, p = 0.097]. Finally, simple slope analysis revealed that CPCI Resting subscale predicted decreases in psychological function for participants with osteoarthrosis [b = −4.72, t(290) = −5.08, p < 0.001], ankylosing spondylitis [b = −3.63, t(290) = 2.18, p = 0.030] and with other musculoskeletal conditions [b = −3.38, t(290) = 3.77, p < 0.001], but not for participants with rheumatoid arthritis [b = 2.19, t(290) = 1.62, p = 0.178] and disc hernia [b = −2.26, t(290) = 0.943, p = 0.347].
Discussion
This study sought to determine if patients with chronic musculoskeletal pain reported differences in the use of different pain coping responses as a function of diagnosis, and if diagnosis moderated the associations between pain-coping responses and measures of pain and function. We anticipated that pain diagnosis would moderate the association between some pain-coping response and pain-related outcomes. Findings showed that, with only one exception, pain-coping responses are independent of pain etiology. The findings also provided limited support to the hypothesized moderation effect of pain diagnosis on the association between coping responses and some pain-related outcomes.
The results indicated that the way people with chronic pain cope with their pain is mostly independent of pain diagnosis. In fact, for all but one pain coping responses (CPCI Coping Self-Statements), pain diagnosis groups showed a similar frequency of use of coping responses. These findings are consistent with previous research comparing individuals with chronic pain due to different rheumatic illnesses, for which an effect of pain diagnosis was found for only coping responses of ignoring pain sensations and distancing from pain.31 While previous research focusing the predictors of coping responses suggest that stressor-related characteristics (eg, level of perceived stress associated with the stressor or cluster of stressors) may be associated with the coping responses employed to cope with the stressor, it is possible that other pain-related characteristics and/or domains – but not the etiology of pain – influence pain-coping responses. These include variables such as culture, context, gender, age, personality, and appraisals, all of which have been shown in previous studies to be associated with the way one copes with a given stressor.16,59–63
It is also possible that one pain characteristic or domain not assessed in this study – the recurrence or persistency of pain – may influence how an individual copes with chronic pain. Although all of the participants in this study had pain for at least 3 months, temporal patterns of pain intensity could potentially have varied from one participant to another. It is possible, for example, that individuals with long-lasting stable pain experience different levels of perceived stress than individuals with intermittent pain.59 Relatedly, it is possible that individuals with long-lasting stable pain may cope with pain differently than individuals whose pain is of shorter duration.59,64 Future research is needed to evaluate the role of the temporal aspects of pain on coping.
Our findings provide limited support for the hypothesis that pain diagnosis moderates the association between some pain-coping response and pain-related outcomes. However, we found that more often than not, the effects of pain-coping responses on pain and function do not vary as a function of pain diagnosis. This finding is consistent with Leventhal’s Self-regulation Model of Health and Illness.65 As a result, pain treatments that target these coping responses for change, for example, treatments that encourage the use of task persistence as a strategy to deal with pain and that discourage the practice of strategies thought to be maladaptive (eg, guarding, asking for assistance) in response to pain are likely to have similar benefits to individuals with musculoskeletal chronic pain, regardless of pain type or etiology.
However, three moderation effects did emerge. These findings are consistent with the possibility that the positive and negative effects of some psychosocial factors – such as coping responses – on physical and psychological function may vary as a function of pain etiology.27 Consequently, if the findings from the current study replicate, the findings would also suggest that there may be certain pain conditions where some coping responses play a larger role than others. For example, in treatment programs provided for patients with rheumatoid arthritis or ankylosing spondylitis, relative to other patients with other pain conditions, it may be particularly important to discourage social support seeking. Similarly, it may also be more important to discourage resting in patients with osteoarthrosis and ankylosing spondylitis than in patients with disc hernia and rheumatoid arthritis.
This study has a number of limitations that need to be taken into consideration when interpreting the results. First, the use of a cross-sectional design does not allow us to draw causal conclusions regarding the associations among the variables studied. Second, the use of a convenience sample raises the possibility that the sample may not have been representative of the population of patients with chronic musculoskeletal pain in Portugal. Future research is needed to establish the generalizability of the findings, and draw potentially existing causal pathways between the variables. Third, we limited the sample to only individuals with chronic musculoskeletal pain. Individuals with other pain conditions, such as fibromyalgia, headache or neuropathic pain, were not included. It is possible that a greater number of moderation effects might have emerged, had we included participants with these other chronic pain conditions, including fibromyalgia. Future research is needed to evaluate this possibility. Forth, while the inclusion of participants of different age ranges (from 18 to 90 years old) increases the generalizability of the study findings across different age groups, the sample’s mean age was high (over 60 years old). Despite the fact that all moderation analysis controlled for the possible effects of sex and age as covariates, it is possible that the results – especially for the two most frequently used coping responses – might have been different in a younger sample. Future research is needed to assess the moderation effects of pain etiology on the association between coping responses and measures of function in samples of young and middle-aged individuals with chronic pain. Fifth, as noted by Ferreira-Valente et al.9,16 and Sharma et al,66 patients’ cultural background and socioeconomic may not only influence pain-coping responses employed by patients, but also moderate the association between pain-coping responses and pain outcomes. Thus, findings from the present study, with a sample of Portuguese patients with chronic musculoskeletal pain, may not generalize across countries and cultures. Future research is needed to establish the generalizability of these findings to other countries and cultures. Finally, the sample sizes of different pain diagnosis groups were uneven, and two of such groups had a small sample size (33 and 31), compromising the power available to test for moderating effects. It is possible that more moderation effects would have emerged had we had a larger sample size within each chronic pain condition group. Future research should seek to replicate the findings from this study using larger sample sizes, if possible.
Conclusion
Despite the study’s limitations, the findings provide important new evidence regarding the associations between coping, pain, and function in individuals with chronic musculoskeletal pain. Specifically, they indicate that there tends to be more similarities than differences in the role of pain-coping responses across different musculoskeletal conditions. At the same time, some few differences may exist, and these are important to consider in pain treatment. For example, the findings suggest that patients with osteoarthritis or ankylosing spondylitis should be encouraged not to engage in rest as a way of coping with pain. Further studies replicating and extending these findings would be useful to determine the reliability of the findings. Future research should also examine the moderating effects of pain diagnosis on the association between pain-coping responses and measures of pain and function in representative samples of individuals with chronic musculoskeletal pain, including individuals with fibromyalgia. This research should also be extended to individuals with a greater variety of chronic pain conditions beyond only musculoskeletal pain, and evaluate the possible effects of pain duration and the intermittency versus stability of pain on pain-coping strategies.
Acknowledgments
The authors gratefully acknowledge the Portuguese Foundation for Science and Technology for AFV’s FCT post-doctoral grant (SFRH/BPD/121452/2016), as well as the William James Center for Research (UID/PSI/04810/2019).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287. doi:10.1016/j.ejpain.2005.06.009
2. Kroska EB. A meta-analysis of fear-avoidance and pain intensity: the paradox of chronic pain. Scand J Pain. 2016;13:43–58. doi:10.1016/j.sjpain.2016.06.011
3. Adams L, Turk D. Psychosocial factors and central sensitivity syndromes. Curr Rheumatol Rev. 2015;11(2):96–108. doi:10.2174/1573397111666150619095330
4. Azevedo LF, Costa-Pereira A, Mendonça L, Dias CC, Castro-Lopes JM. Epidemiology of chronic pain: a population-based nationwide study on its prevalence, characteristics and associated disability in Portugal. J Pain. 2012;13(8):773–783. doi:10.1016/j.jpain.2012.05.012
5. Gouveia M, Augusto M. Custos indirectos da dor crónica em Portugal [Indirect costs of chronic pain in Portugal]. Rev Port Saúde Pública. 2011;29(2):100–107. Portuguese. doi:10.1016/S0870-9025(11)70013-X
6. Jensen MP, Turk DC. Contributions of psychology to the understanding and treatment of people with chronic pain: why it matters to ALL psychologists. Am Psychol. 2014;69(2):105–118. doi:10.1037/a0035641
7. Morlion B, Walch H, Yihune G, et al. The pain associates’ international network initiative: a novel practical approach to the challenge of chronic pain management in Europe. Pain Pract. 2008;8(6):473–480. doi:10.1111/j.1533-2500.2008.00236.x
8. Costa LDCM, Maher CG, McAuley JH, Hancock MJ, Smeets RJEM. Self-efficacy is more important than fear of movement in mediating the relationship between pain and disability in chronic low back pain. Eur J Pain. 2011;15(2):213–219. doi:10.1016/j.ejpain.2010.06.014
9. Ferreira-Valente A, Pais-Ribeiro J, Jensen MP. Association between psychosocial factors and pain intensity, physical functioning, and psychological functioning in patients with chronic pain: a cross-cultural comparison. Clin J Pain. 2014;30(8):713–723. doi:10.1097/AJP.0000000000000027
10. Miró J, Huguet A, Jensen MP. Pain beliefs predict pain intensity and pain status in children: usefulness of the pediatric version of the survey of pain attitudes. Pain Med. 2014;15(6):887–897. doi:10.1111/pme.12316
11. Osborne TL, Jensen MP, Ehde DM, Hanley MA, Kraft G. Psychosocial factors associated with pain intensity, pain-related interference, and psychological functioning in persons with multiple sclerosis and pain. Pain. 2007;127(1):52–62. doi:10.1016/j.pain.2006.07.017
12. Rippentrop EA. A review of the role of religion and spirituality in chronic pain populations. Rehabil Psychol. 2005;50(3):278–284. doi:10.1037/0090-5550.50.3.278
13. Rippentrop EA, Altmaier EM, Chen JJ, Found EM, Keffala VJ. The relationship between religion/spirituality and physical health, mental health, and pain in a chronic pain population. Pain. 2005;116(3):311–321. doi:10.1016/j.pain.2005.05.008
14. Edwards RR, Dworkin RH, Sullivan MD, Turk DC, Wasan AD. The role of psychosocial processes in the development and maintenance of chronic pain. J Pain. 2016;17(9):T70–T92. doi:10.1016/j.jpain.2016.01.001
15. Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87:168–182. doi:10.1016/j.pnpbp.2018.01.017
16. Ferreira-Valente A, Pais-Ribeiro J, Jensen MP, Almeida R. Coping with chronic musculoskeletal pain in Portugal and in the United States: a cross-cultural study. Pain Med. 2011;12(10):1470–1480. doi:10.1111/j.1526-4637.2011.01208.x
17. Thong ISK, Tan G, Lee TYC, Jensen MP. A comparison of pain beliefs and coping strategies and their association with chronic pain adjustment between Singapore and United States. Pain Med. 2017;18(9):1668–1678. doi:10.1093/pm/pnw237
18. Esteve R, Ramírez-Maestre C, López-Martínez AE. Adjustment to chronic pain: the role of pain acceptance, coping strategies, and pain-related cognitions. Ann Behav Med. 2007;33(2):179–188. doi:10.1007/BF02879899
19. López-Martínez AE, Esteve-Zarazaga R, Ramírez-Maestre C. Perceived social support and coping responses are independent variables explaining pain adjustment among chronic pain patients. J Pain. 2008;9(4):373–379. doi:10.1016/j.jpain.2007.12.002
20. Alschuler KN, Otis JD. Coping strategies and beliefs about pain in veterans with comorbid chronic pain and significant levels of posttraumatic stress disorder symptoms: coping strategies and beliefs about pain in veterans. Eur J Pain. 2012;16(2):312–319. doi:10.1016/j.ejpain.2011.06.010
21. Jensen MP, Keefe FJ, Lefebvre JC, Romano JM, Turner JA. One- and two-item measures of pain beliefs and coping strategies. Pain. 2003;104(3):453–469. doi:10.1016/S0304-3959(03)00076-9
22. Tan G, Nguyen Q, Cardin SA, Jensen MP. Validating the use of two-item measures of pain beliefs and coping strategies for a Veteran population. J Pain. 2006;7(4):252–260. doi:10.1016/j.jpain.2005.11.007
23. Woby SR, Roach NK, Urmston M, Watson PJ. Psychometric properties of the TSK-11: a shortened version of the tampa scale for kinesiophobia. Pain. 2005;117(1):137–144. doi:10.1016/j.pain.2005.05.029
24. Morasco BJ, Greaves DW, Lovejoy TI, Turk DC, Dobscha SK, Hauser P. Development and preliminary evaluation of an integrated cognitive-behavior treatment for chronic pain and substance use disorder in patients with the hepatitis C virus. Pain Med. 2016;17(12):2280–2290. doi:10.1093/pm/pnw076
25. Turk DC, Adams LM. Using a biopsychosocial perspective in the treatment of fibromyalgia patients. Pain Manag. 2016;6(4):357–369. doi:10.2217/pmt-2016-0003
26. Bernardes SF, Forgeron P, Fournier K, Reszel J. Beyond solicitousness: a comprehensive review on informal pain-related social support. Pain. 2017;158(11):2066–2076. doi:10.1097/j.pain.0000000000001033
27. Glette M, Landmark T, Jensen MP, et al. Catastrophizing, solicitous responses from significant others, and function in individuals with neuropathic pain, osteoarthritis, or spinal pain in the general population. J Pain. 2018;19(9):983–995. doi:10.1016/j.jpain.2018.03.010
28. Rosen NL. Psychological issues in the evaluation and treatment of tension-type headache. Curr Pain Headache Rep. 2012;16(6):545–553. doi:10.1007/s11916-012-0301-z
29. Wellington J. Noninvasive and alternative management of chronic low back pain (efficacy and outcomes): nonmedical management of chronic low back pain. Neuromodulation Technol Neural Interface. 2014;17:24–30. doi:10.1111/ner.12078
30. Jahan F, Nanji K, Qidwai W, Qasim R. Fibromyalgia syndrome: an overview of pathophysiology, diagnosis and management. Oman Med J. 2012;27(3):192–195. doi:10.5001/omj.2012.44
31. Bucourt E, Martaillé V, Goupille P, et al. A comparative study of fibromyalgia, rheumatoid arthritis, spondyloarthritis, and Sjögren’s syndrome; Impact of the disease on quality of life, psychological adjustment, and use of coping strategies. Pain Med. 2019:pnz255. doi:10.1093/pm/pnz255
32. Ferreira-Valente A, Pais-Ribeiro J, Jensen MP. Validity of four pain intensity rating scales. Pain. 2011;152(10):2399–2404. doi:10.1016/j.pain.2011.07.005
33. Jensen M. Measurement of pain. In: Fishman S, Ballantyne J, Rathmell J, editors. Bonica’s Management of Pain. Media, PA: Williams & Wilkins; 2010:251–270.
34. Alghadir A, Anwer S, Iqbal A, Iqbal Z. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J Pain Res. 2018;11:851–856. doi:10.2147/JPR.S158847
35. Ferreira PL. Development of the Portuguese version of MOS SF-36 Part II: validation tests. Acta Médica Port. 2000;13:119–127.
36. Ferreira PL. Development of the Portuguese version of MOS SF-36 Part I: cultural and linguistic adaptation. Acta Médica Port. 2000;13:55–66.
37. Ferreira PL, Santana P. Percepção de estado de saúde e de qualidade de vida da população activa: contributo para a definição de normas portuguesas [Perception of health status and quality of life of the active population: contribution to the definition of Portuguese standards]. Rev Port Saúde Pública. 2003;21:15–30. Portuguese.
38. Pais-Ribeiro J. O Importante é a Saúde: Estudo de Adaptação de Uma Técnica de Avaliação Do Estado de Saúde - SF-36 [Health is Important: Study on the Adaptation of a Health Status Assessment Technique - SF-36]. Lisboa: Fundação Merck Sharp & Dohme; 2005. Portuguese.
39. Ferreira-Valente A, Pais-Ribeiro J, Jensen MP. Additional contribution for the study of the Portuguese version of two brief pain coping questionnaires. In: Actas do VIII Congresso Iberoamericano de Avaliação/Evaluación Psicológica. XV Conferência Internacional Avaliação Psicológica: Formas e Contextos [Proceeding of the 8th Iberoamerican Congress of Psychologycal Assessment. 15th International Conference of Psychological Assessment: Ways and Contexts]. Lisboa: Sociedade Portuguesa de Psicologia; 2011:784–792. Portuguese.
40. Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment. Pain. 1983;17(1):33–44. doi:10.1016/0304-3959(83)90125-2
41. Jensen IB, Linton SJ. Coping strategies questionnaire (CSQ): reliability of the swedish version of the CSQ. Scand J Behav Ther. 1993;22(3–4):139–145. doi:10.1080/16506079309455940
42. Portnoi AG. Dor, Stress e Coping: Grupos Operativos em Doentes com Síndrome de Fibromialgia [Pain, Stress and Coping: Operating Groups in Patients with Fibromyalgia Syndrome]. São Paulo: Instituto de Psicologia da Universidade de São Paulo; 1999. Portuguese.
43. Wilkie D, Keefe F. Coping strategies of patients with lung cancer-related pain. Clin J Pain. 1991;7(4):292–299. doi:10.1097/00002508-199112000-00007
44. Jensen MP, Turner JA, Romano JM, Strom SE. The chronic pain coping inventory: development and preliminary validation. Pain. 1995;60(2):203–216. doi:10.1016/0304-3959(94)00118-X
45. Romano JM, Jensen MP, Turner JA. The chronic pain coping inventory-42: reliability and validity. Pain. 2003;104(1):65–73. doi:10.1016/S0304-3959(02)00466-9
46. Costa J, Pinto-Gouveia J. Avaliação da dor: utilização do questionário de auto-resposta the Survey of Pain Attitudes (SOPA) e Chronic Pain Coping Inventory (CPCI-42) na população portuguesa [Pain assessment: use of the Survey of Pain Attitudes (SOPA) and Chronic Pain Coping Inventory (CPCI-42) self-answer questionnaire in the Portuguese population]. Psychologica. 2008;49:168–207. Portuguese.
47. Soper D. A-priori sample size calculator for structural equation models. 2018. Available from: www.danielsoper.com/statcalc.
48. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
49. Molton I, Jensen MP, Ehde DM, Carter GT, Kraft G, Cardenas DD. Coping with chronic pain among younger, middle-aged, and older adults living with neurological injury and disease. J Aging Health. 2008;20(8):972–996. doi:10.1177/0898264308324680
50. Kline P. The Handbook of Psychological Testing.
51. Kline R. Principles and Practice of Structural Equation Modeling.
52. Cohen J. Eta-squared and partial eta-squared in fixed factor ANOVA designs. Educ Psychol Meas. 1973;33(1):107–112. doi:10.1177/001316447303300111
53. Hayes AF. Introduction to Mediation, Moderation and Conditional Process Analysis.
54. Hayes AF, Matthes J. Computational procedures for probing interactions in OLS and logistic regression: SPSS and SAS implementations. Behav Res Methods. 2009;41(3):924–936. doi:10.3758/BRM.41.3.924
55. Hayes AF, Cai L. Using heteroskedasticity-consistent standard error estimators in OLS regression: an introduction and software implementation. Behav Res Methods. 2007;39(4):709–722. doi:10.3758/BF03192961
56. Long JS, Ervin LH. Using heteroscedasticity consistent standard errors in the linear regression model. Am Stat. 2000;54(3):217. doi:10.2307/2685594
57. Bauer DJ, Curran PJ. Probing interactions in fixed and multilevel regression: inferential and graphical techniques. Multivar Behav Res. 2005;40(3):373–400. doi:10.1207/s15327906mbr4003_5
58. Tabachnick B, Fidell L. Using Multivariate Statistic.
59. Chan M Individual and stressor-related predictors of coping response among vietnamese American and European American adolescents. 2016. Available from: https://escholarship.org/uc/item/6rc3n6rq.
60. Lazarus R, Folkman S. Stress, Appraisal, and Coping. New York, NY: Springer Publishing Company; 1984.
61. Ferreira-Valente A, Pais-Ribeiro J, Jensen MP. Coping, depression, anxiety, self-efficacy and social support: impact on adjustment to chronic pain. Escr Psicol. 2009;2(3).
62. Vlaeyen JWS, Crombez G, Linton SJ. The fear-avoidance model of pain. Pain. 2016;157(8):1588–1589. doi:10.1097/j.pain.0000000000000574
63. Van Damme S, Crombez G, Eccleston C. Coping with pain: a motivational perspective. Pain. 2008;139(1):1–4. doi:10.1016/j.pain.2008.07.022
64. Holmes JA, Stevenson CAZ. Differential effects of avoidant and attentional coping strategies on adaptation to chronic and recent-onset pain. Health Psychol. 1990;9(5):577–584. doi:10.1037/0278-6133.9.5.577
65. Leventhal H, Brissette I, Leventhal E. The common-sense model of self-regulation of health and illness. In: Cameron L, Leventhal H, editors. The Self-Regulation of Health and Illness Behaviour. London: Routledge; 2003:42–65.
66. Sharma S, Abbott JH, Jensen MP. Why clinicians should consider the role of culture in chronic pain. Braz J Phys Ther. 2018;22(5):345–346. doi:10.1016/j.bjpt.2018.07.002
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.