Back to Journals » Journal of Pain Research » Volume 15
Pain Assessment in Chinese Parkinson’s Disease Patients Using King’s Parkinson’s Disease Pain Scale
Authors Gao L, Huang W, Cai L, Peng Y
Received 10 December 2021
Accepted for publication 26 February 2022
Published 10 March 2022 Volume 2022:15 Pages 715—722
DOI https://doi.org/10.2147/JPR.S353249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Liang Gao, Weiling Huang, Laisheng Cai, Yufen Peng
Department of Neurology, The First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
Correspondence: Yufen Peng; Liang Gao, Tel +86 791-88692511, Email [email protected]; [email protected]
Purpose: To assess Parkinson’s disease (PD)-related pain using the Chinese translation of King’s Parkinson’s disease Pain Scale (KPPS).
Patients and Methods: A cohort of 200 patients with primary PD was recruited for this study. Their demographic and clinical features, including age, disease duration, levodopa equivalent daily dose (LEDD), and scores on the Unified Parkinson’s Disease Rating Scale-III (UPDRS III), Hoehn-Yahr Scale (H&Y), Mini-Mental State Examination (MMSE), Activities of Daily Living Scale (ADL), Hamilton Depression Rating Scale (HAMD), Hamilton Anxiety Rating Scale (HAMA), Pittsburgh Sleep Quality Index (PSQI), Visual Analogue Scale (VAS) and KPPS, were recorded.
Results: The prevalence of PD-related pain was 44.5%. Among the patients with PD-related pain, the average KPPS score was 41.2 ± 26.8. Pain was most commonly located in the lower limbs (60.7%), upper limbs (22.5%) and waist (21.3%). The most common pain type was musculoskeletal pain (68.5%). Compared with the PD group without pain, the PD group with pain had a longer disease duration (p = 0.022), higher LEDD (p = 0.008), higher UPDRSIII score (p = 0.018), higher H&Y stage (p = 0.003), higher HAMD score (p < 0.001), higher HAMA score (p < 0.001), lower ADL score (p = 0.046) and higher PSQI score (p < 0.001). PD-related pain was correlated with the H&Y stage and the PSQI score (p < 0.05). Cut-off points of 0, 34, and 70 were obtained to discriminate pain severity levels between no pain, mild, moderate, and severe pain, respectively.
Conclusion: Chinese version of KPPS is not only an easy tool for characterization and scoring of pain in PD patients but also has the ability to distinguish between different levels of pain severity.
Keywords: Parkinson’s disease, pain, clinical characteristics, King’s Parkinson’s disease Pain Scale
Introduction
Parkinson’s disease (PD) is a chronic and progressive neurodegenerative disorder characterized by motor symptoms of resting tremor, rigidity, bradykinesia, and postural instability. In recent years pain is increasingly recognized as a prevalent and troublesome non-motor symptom that negatively affects the quality of life in individuals with PD.1,2 PD-related pain is classified into five categories with different pathophysiologies including musculoskeletal, neuropathic radicular, dystonia-related, akathitic discomfort, and primary central parkinsonian pain, which can coexist in the same individual.3–5 In addition, there are studies classified PD-related pain using an anatomy-based classification or a syndrome-based classification recently.6,7
About 40–85% of the patients with PD suffer from various types of pain,6,8,9 however, most of them do not receive appropriate and regular analgesic treatment because it is poorly understood and the amount of pain is not accurately measured.10,11 Before the King’s Parkinson’s disease Pain Scale (KPPS) was published as the first disease-specific scale to assess pain in PD, most of the descriptive data on pain in PD was obtained using non-disease-specific assessment tools.12
KPPS has already been used as a reliable tool available in English language to assess various types of PD-related pain.9 However, based on the suggestion of KPPS developers, more studies are needed in other languages to better generalize the results and make more use of this scale. Recently, a validated version in German, French, Spanish, Turkish, Hindi, Persian, and Bulgarian were published.11,13–16 Questionnaires or studies on the reliability and validity of KPPS assessing PD-related pain in Chinese language do not exist. In present study we aimed to estimate the occurrence of pain in PD patients using KPPS in Chinese language and to validate it.
Materials and Methods
Participants
Our cross-sectional and observational study included 200 PD patients who attended the Department of Neurology at the First Affiliated Hospital of Nanchang University between March 2018 and March 2021. All subjects from both the outpatient department and the ward were examined by experienced neurologists and met the Movement Disorder Society (MDS) Clinical Diagnostic Criteria for Parkinson’s disease (MDS-PD Criteria).17 Individuals with atypical or secondary parkinsonism, pain with known causes, on analgesic therapeutics due to other diseases or a history of neurosurgery were excluded. Moreover, those with parkinsonian syndromes, including progressive supranuclear palsy, multiple system atrophy and corticobasal degeneration, as well as those with serious medical diseases and psychological illness, were also excluded. Written informed consent was obtained from all subjects before participation in the study. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University.
Clinical Assessment Protocol
The demographic features and clinical data, including age, sex, disease duration and use of anti-Parkinson medication, were collected by movement disorder specialists using a standard questionnaire during face-to-face interviews. The Unified Parkinson’s Disease Rating Scale (UPDRS) part III was used to assess motor disability, and the Hoehn-Yahr (H&Y) scale was used to establish disease severity. The KPPS and Visual Analogue Scale (VAS) were used to assess pain symptoms. The Mini-Mental State Examination (MMSE) was used to evaluate global cognitive function. In addition, affective disorders were assessed with the Hamilton Depression Rating Scale (HAMD) and the Hamilton Anxiety Rating Scale (HAMA). The Pittsburgh Sleep Quality Index (PSQI) was used to assess the sleep quality of the patient, and the quality of the activities of daily life scale (ADL) was used to assess the ability to perform daily activities.
Statistical Analysis
Statistical analysis was performed with the Statistical Package for the Social Sciences version 23.0 (SPSS, Chicago, IL, USA). Measurement data are presented as the mean ± standard deviation. The homogeneity of variance of the variables was assessed by Levene’s test. Differences in demographic and clinical characteristics between groups were analysed using independent two tailed t-tests. The enumeration data were expressed as the rate (%), and the chi-squared test was used for comparisons between groups. KPPS score was correlated with demographic factors and other scores, and correlation coefficient was calculated. Multiple logistic regression analysis was used to assess the risk factors. Receiver operating characteristic (ROC) curve analysis was applied to determine the optimal cut-off points of the total score of KPPS for different pain severity levels and p values of <0.05 were considered statistically significant.
Results
Characteristics of the Sample
A total of 200 patients were recruited for this study. Of these patients, 108 (54%) patients were male, and 92 (46%) were female. Table 1 shows the demographic data and baseline clinical characteristics of the whole cohort. There were 89 (44.5%) patients with pain and 111 (55.5%) patients without pain, so the prevalence of pain in PD was 44.5%.
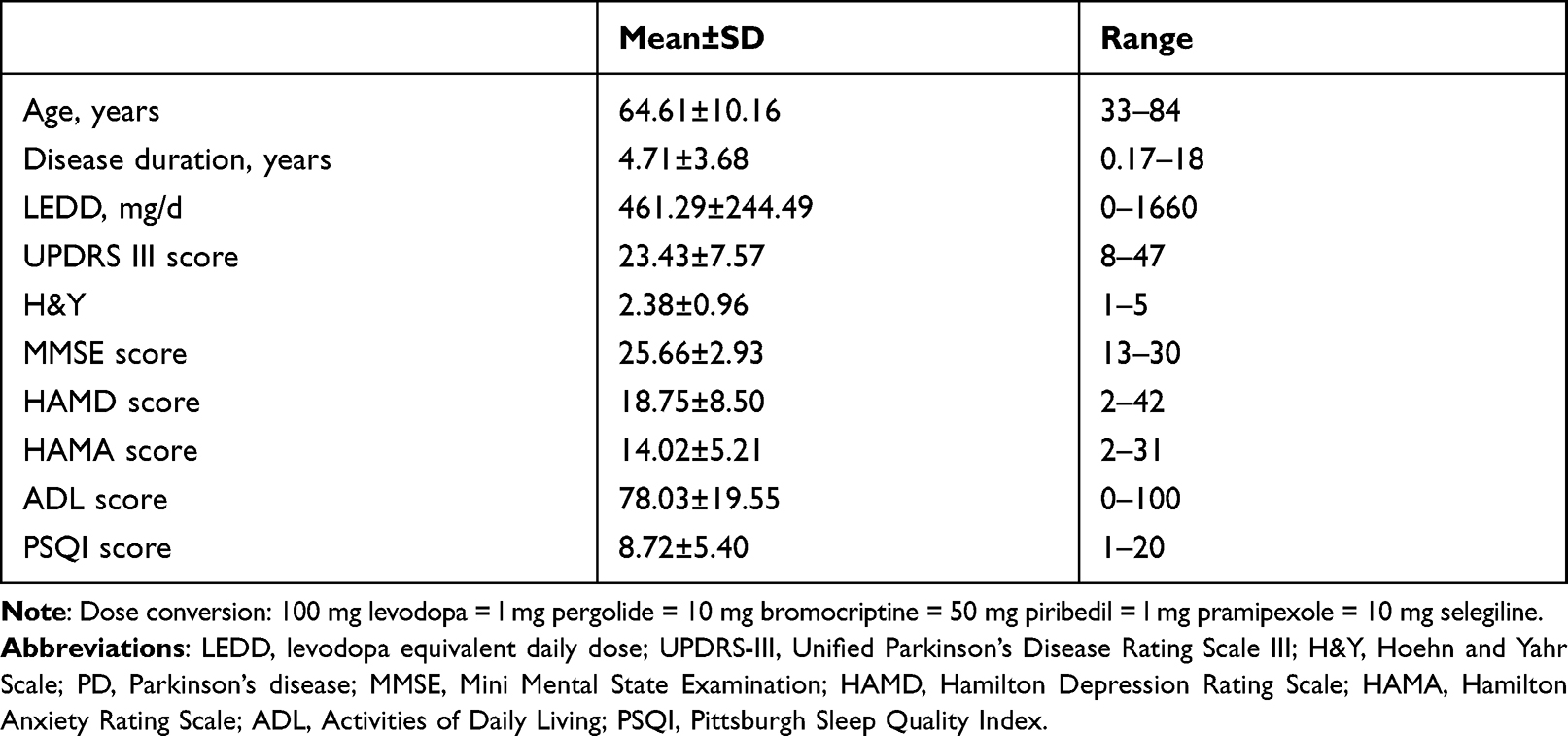 |
Table 1 Baseline Clinical Characteristics of All Study Participants (n=200) |
Pain Types
Among the 89 patients of PD with pain, 54 (60.7%) reported pain located in the lower limbs, 20 (22.5%) reported pain located in the upper limbs, 19 (21.3%) reported pain located in the waist, 9 (10.1%) reported pain located in the joints, 8 (9%) reported pain located in the back, 6 (6.7%) reported pain located in the shoulder and neck, and 2 (2.2%) reported pain located in the head. Twenty-four patients (27%) reported pain in two or more locations.
The range of the total KPPS score was 5–134 points, with an average of 41.2±26.8 points. The specific findings are shown in Table 2. According to the Ford classification, 55 (61.8%) patients had musculoskeletal pain, 24 (27%) patients had dystonia-related pain, 13 (14.6%) patients had neuropathic radicular pain, 9 (10.1%) patients had central pain, 5 (5.6%) patients had akathitic discomfort, and 17 (19.1%) patients had two types of pain. Twenty-four (27%) patients with PD-related pain were treated with analgesics.
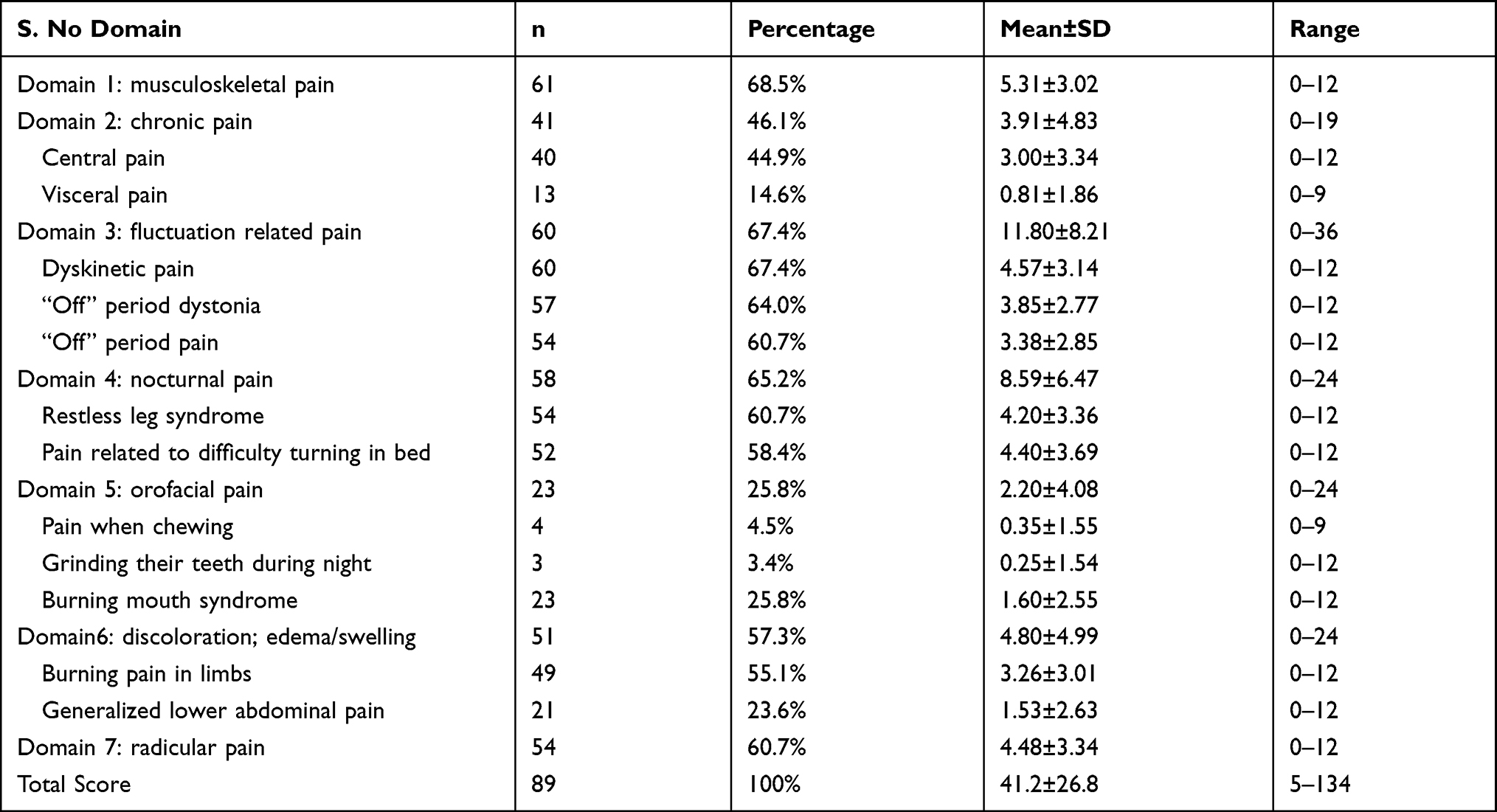 |
Table 2 Types of Pain in PD Patients as Measured by KPPS |
Effects of Pain on Motor and Non-Motor Symptom
Between-group comparisons of gender, age, course of disease, equivalent daily dose of levodopa, motor symptoms and non-motor symptoms are shown in Table 3. There were no significant differences regarding gender and age between the groups; however, PD patients with pain had longer disease duration (p=0.022) and a higher levodopa equivalent daily dose (p=0.008) than patients without pain.
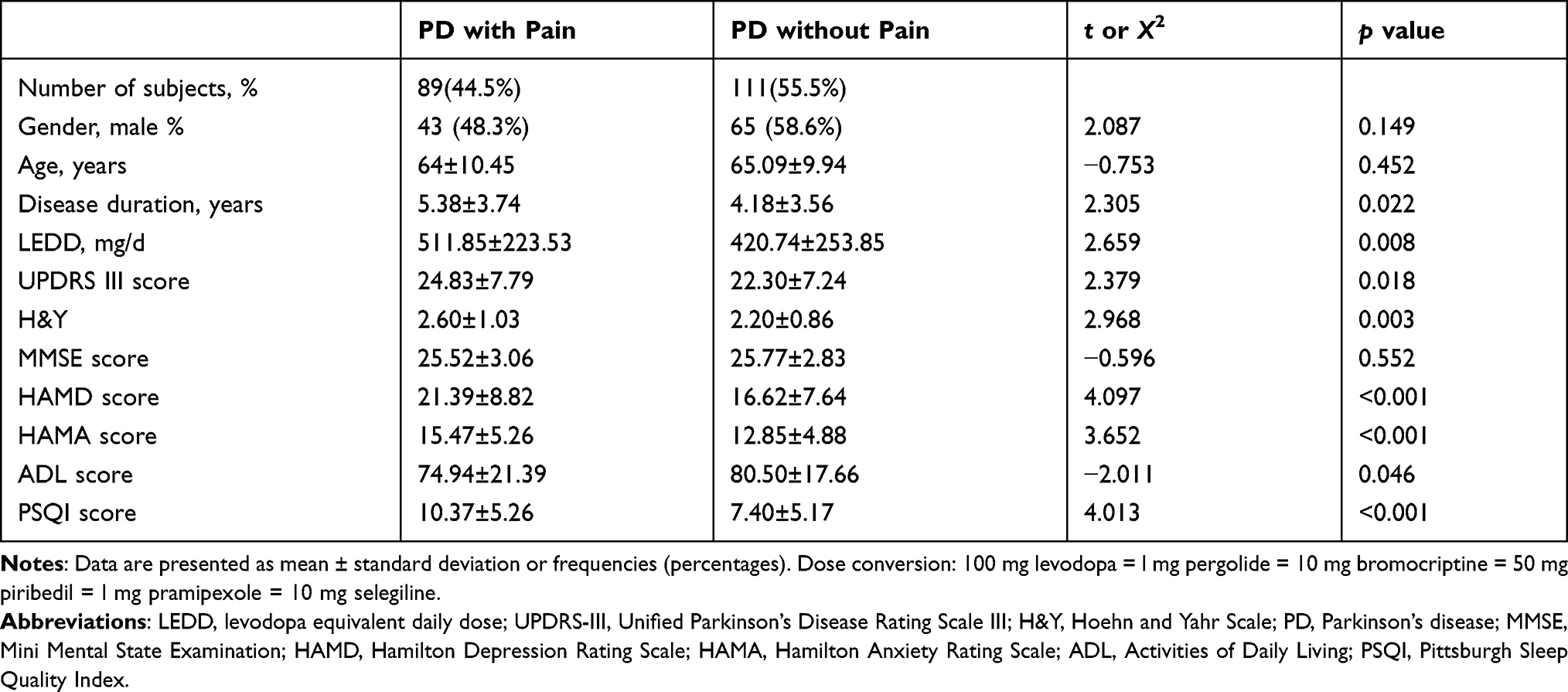 |
Table 3 Demographic and Clinical Characteristics of Parkinson’s Disease (PD) Patients with Pain and PD Patients without Pain |
The PD with pain group had a higher UPDRSIII score (p=0.018) and higher H&Y stage (p=0.003), suggesting that patients with PD-related pain had more severe motor disorders and conditions. HAMD and HAMA scores were higher in the PD with pain group (p<0.001), suggesting that these patients were more prone to mood disorders such as anxiety and depression. In addition, PSQI scores were higher (p<0.001) and ADL scores were lower (p<0.046) in the PD with pain group, suggesting that these patients had worse sleep quality and lower daily living ability. However, there was no significant difference in MMSE scores between the two groups (p>0.05).
Risk Factors for Pain
The mean KPPS scores had a weak correlation with LEED (r = 0.212). KPPS scores correlated positively with UPDRS III score (r = 0.521), H&Y (r = 0.644), MMSE score (r = −0.425), HAMD score (r = 0.467), HAMA score (r = 0.485), ADL score (r = −0.611) and PSQI score (r = 0.533) (Table 4).
 |
Table 4 Correlation of KPPS Scores with Various Factors (n=89) |
Multiple logistic regression analysis showed that PD-related pain was associated with H&Y stage [mild (OR=1.000), moderate (OR=2.394, 95% CI: 1.281–4.473, p=0.006), severe (OR=3.184, 95% CI: 1.128–8.986, p=0.029) and PSQI scores (OR=2.068, 95% CI: 1.129–3.786, p=0.019)]. After adjusting for confounding factors, H&Y stage and PSQI were shown to be risk factors for PD-related pain (Table 5).
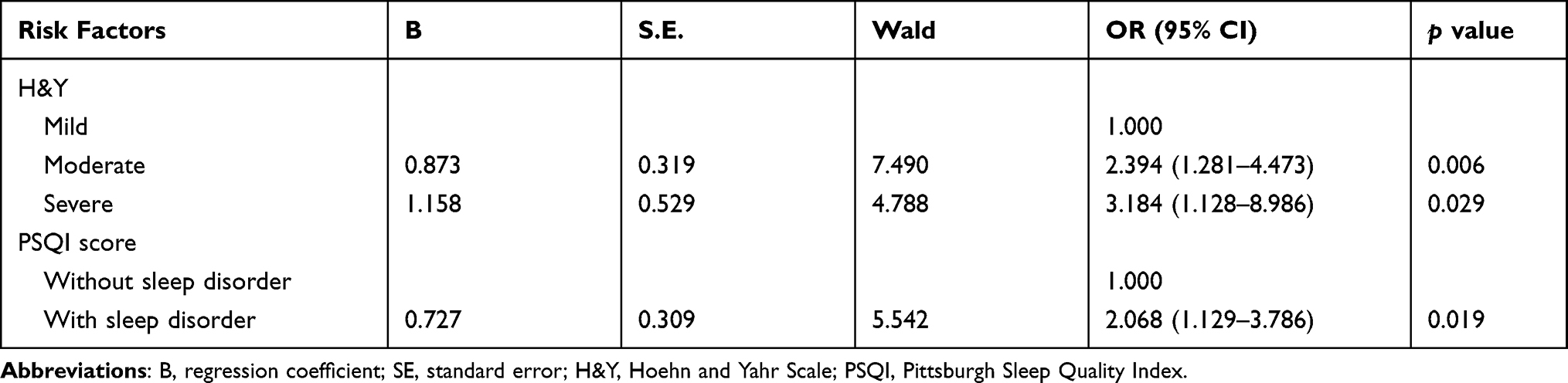 |
Table 5 Logistic Regression Analysis of Risk Factors of Parkinson’s Disease Related Pain |
KPPS Cut-Off Points
Table 6 shows the validity parameters acquired from ROC analysis for the total score of KPPS in separate pain severity levels. The cut-off point to discriminate no pain from mild pain was more than 0 (sensitivity = 100% and specificity = 100%). A cut-off point greater than 34 (sensitivity = 92.30% and specificity = 92.32%) and greater than 70 (sensitivity = 100% and specificity = 76.93%) was obtained to distinguish mild pain from moderate pain, and moderate pain from severe pain, respectively.
 |
Table 6 Validity Values of the King’s Parkinson’s Disease Scale for Discriminating Pain Level in People with Parkinson’s Disease (n=200) |
Discussion
The aim of the present study was to assess types and frequency of PD-related pain using Chinese translation of KPPS and to validate the Chinese version in Chinese PD patients. We also compared the clinical characteristics between PD patients with pain and those without pain, identified the risk factors for PD-related pain and examined the KPPS cut-off points for pain severity levels.
In the present study, the prevalence of PD-related pain was 44.5%, which was lower than the average reported in the literature. The prevalence of PD-related pain in the current literature is approximately 60% on average and varies from 40% to 85%;8,9,18 this wide range is related to a lack of objective methods for pain measurement, different patient groups, and the methods of data collection. In addition, the diagnosis and treatment of PD related pain is complex in case of prevalent comorbidities. To date, pain in PD patients has not been properly acknowledged or treated, and many patients do not receive any medication or physical therapy for pain.19 In our cohort, only 27% of patients with PD-related pain received treatment. Therefore, clinicians should pay attention to the evaluation and treatment of PD-related pain to improve the quality of life of patients.
Over-all the most common locations of pain in our PD patients were lower limb (60.7%), upper limb (22.5%) and waist (21.3%), which is consistent with the results of some previous studies.18,20 However, Kubo and Camacho-Conde et al found that the lower back region was the most common location of pain.6,21
We assess types and frequency of PD-related pain using Chinese translation of KPPS, and found that the most common types of pain were musculoskeletal pain (68.5%), fluctuation-related pain (67.4%) and nocturnal pain (65.2%). A similar pattern is reported by other authors as well.4,8,9,22–25 The mean total KPPS score in our study was 41.2±26.8, which was higher than the results of some previous studies.14,15,22 According to the Ford classification, the most common types of PD-related pain are musculoskeletal pain and dystonia-related pain, followed by neuropathic radicular pain and central pain, which is consistent with the results of a previous study.26
Our study found that patients in the PD with pain group had a longer disease duration and higher levodopa equivalent daily dose than patients without PD-related pain. However, many studies found that PD-related pain was not associated with the course of disease.9,19 Most studies have suggested that PD-related pain is not associated with gender and age,21 while some studies found that female PD patients and early-onset PD patients were more likely to have pain compared with the general population and late-onset PD patients.9,27 In our study, there was no gender or age difference between the two groups.
The presence of pain was related to more severe motor symptoms, as measured by the H&Y scale and the UPDRS III, and this finding was consistent with previous reports.27–29 Vila-Cha et al also found that pain was related to more severe motor symptoms and comorbidities.28 In addition, among patients with pain, those with the central parkinsonian subtype had lower levodopa responsiveness for non-axial motor symptoms and greater pain-related responsiveness to antiparkinsonian treatment. However, other series have failed to find significant associations between pain and more severe motor symptoms in patients with PD.9,19,21
PD-related pain may negatively impact patients both psychologically and emotionally, leading to depression, anxiety and sleep deprivation and affecting daily routines.2,29–32 Fu et al found that patients with PD-related pain had disrupted sleep continuity, altered sleep architecture, depressed mood, and compromised activities of daily living.33 Our study also found that patients with PD-related pain were more likely to have mood disorders such as anxiety and depression, have a lower ability of daily living, and have poorer sleep quality. In addition, our study did not find significant differences in cognitive function between patients with and without pain, which was consistent with another study.34
KPPS cut-off points could help researchers and clinicians to design personalized treatment plans for each of the individuals, by identifying the characteristics such as the severity level of the pain. Taghizadeh et al found that the KPPS cut-off points of 0, 17, and 68 could discriminate pain severity levels between no pain, mild, moderate, and severe pain, respectively.11 In this study, we also found that discriminative validity of the total KPPS score was adequate to allow classification of different levels of pain intensity. According to the results, the cut-off point 0 differentiates no pain from mild pain, 34 differentiates mild from moderate pain, and 70, moderate from severe pain.
When interpreting these data, several limitations should be acknowledged. First, it is possible that our results are caused in part by the type of patients enrolled in our study and by the limitations of our methodology. Second, this study did not include a control group, which would be important for distinguishing PD-related pain from pain in healthy subjects. Third, a larger sample size of PD patients would increase the power of detecting statistically significant results. Future large-scale multicenter case-control studies should be conducted to determine the clinimetric properties of the Chinese version of KPPS.
Conclusion
Pain is a common and disabling non-motor symptom in patients with PD. PD-related pain has a substantial impact on the motor and non-motor aspects of patients. KPPS is not only an easy tool for characterization, scoring, and follow-up of pain in PD patients but also has the ability to distinguish between different levels of pain severity. Chinese version of KPPS has a very good agreement with other languages version. In the future, this scale may be used widely to measure pain in Chinese patient with PD.
Acknowledgments
The authors thank the patients and their families for their participation in the study. This study was supported by the key research and development plan of science and technology department of Jiangxi Province (NO.20202BBGL73104), science and technology project of Jiangxi provincial health commission (NO.202110017), and science and technology project of Jiangxi administration of traditional Chinese medicine (NO.2020A0310). The authors also thank Dr. Jieqing Yu for her help in the revision process.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Langston JW. The Parkinson’s complex: Parkinsonism is just the tip of the iceberg. Ann Neurol. 2006;59:591–596. doi:10.1002/ana.20834
2. Nguy V, Barry BK, Moloney N, et al. The associations between physical activity, sleep, and mood with pain in people with Parkinson’s disease: an observational cross-sectional study. J Parkinsons Dis. 2020;10:1161–1170. doi:10.3233/JPD-201938
3. Ford B. Pain in Parkinson’s disease. Mov Disord. 2010;25(Suppl 1):S98–103. doi:10.1002/mds.22716
4. Coimbra MR, Almeida-Leite CM, de Faria-fortini I, Christo PP, Scalzo PL. King’s Parkinson’s Disease Pain Scale (KPPS): cross-cultural adaptation to Brazilian Portuguese and content validity. Clin Neurol Neurosurg. 2021;208:106815. doi:10.1016/j.clineuro.2021.106815
5. Chaudhuri KR, Schapira AH. Non-motor symptoms of Parkinson’s disease: dopaminergic pathophysiology and treatment. Lancet Neurol. 2009;8:464–474. doi:10.1016/S1474-4422(09)70068-7
6. Camacho-Conde JA, Campos-Arillo VM. The phenomenology of pain in Parkinson’s disease. Korean J Pain. 2020;33:90–96. doi:10.3344/kjp.2020.33.1.90
7. Valkovic P, Minar M, Singliarova H, et al. Pain in Parkinson’s disease: a cross-sectional study of its prevalence, types, and relationship to depression and quality of life. PLoS One. 2015;10:e0136541. doi:10.1371/journal.pone.0136541
8. Hirsi JO, Yifru YM, Metaferia GZ, Bower JH. Prevalence of pain in patients with Parkinson’s disease in Addis Ababa, Ethiopia. Parkinsonism Relat Disord. 2019;61:214–218. doi:10.1016/j.parkreldis.2018.09.030
9. Silverdale MA, Kobylecki C, Kass-Iliyya L, et al. A detailed clinical study of pain in 1957 participants with early/moderate Parkinson’s disease. Parkinsonism Relat Disord. 2018;56:27–32. doi:10.1016/j.parkreldis.2018.06.001
10. Buhmann C, Kassubek J, Jost WH. Management of pain in Parkinson’s disease. J Parkinsons Dis. 2020;10:S37–S48. doi:10.3233/JPD-202069
11. Taghizadeh G, Joghataei MT, Goudarzi S, Bakhsheshi M, Habibi SAH, Mehdizadeh M. King’s Parkinson’s disease pain scale cut-off points for detection of pain severity levels: a reliability and validity study. Neurosci Lett. 2021;745:135620. doi:10.1016/j.neulet.2020.135620
12. Chaudhuri KR, Rizos A, Trenkwalder C, et al. King’s Parkinson’s disease pain scale, the first scale for pain in PD: an international validation. Mov Disord. 2015;30:1623–1631. doi:10.1002/mds.26270
13. Kim HJ, Ruscheweyh R, Yeo JH, et al. Translation, cross-cultural adaptation, and validity of the Korean version of the pain sensitivity questionnaire in chronic pain patients. Pain Pract. 2014;14:745–751. doi:10.1111/papr.12123
14. Behari M, Srivastava A, Achtani R, Nandal N, Dutta RB. Pain assessment in Indian Parkinson’s disease patients using King’s Parkinson’s disease pain scale. Ann Indian Acad Neurol. 2020;23:774–780. doi:10.4103/aian.AIAN_449_20
15. Stoyanova-Piroth G, Milanov I, Stambolieva K. Translation, adaptation and validation of the Bulgarian version of the King’s Parkinson’s Disease Pain Scale. BMC Neurol. 2021;21:357. doi:10.1186/s12883-021-02392-5
16. Jost WH, Rizos A, Odin P, Lohle M, Storch A. King’s Parkinson’s disease pain scale: intercultural adaptation in the German language. Nervenarzt. 2018;89:178–183. doi:10.1007/s00115-017-0333-z
17. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30:1591–1601. doi:10.1002/mds.26424
18. Broen MP, Braaksma MM, Patijn J, Weber WE. Prevalence of pain in Parkinson’s disease: a systematic review using the modified QUADAS tool. Mov Disord. 2012;27:480–484. doi:10.1002/mds.24054
19. Lin XJ, Yu N, Lin XG, et al. A clinical survey of pain in Parkinson’s disease in Eastern China. Int Psychogeriatr. 2016;28:283–289. doi:10.1017/S1041610215001659
20. Wasner G, Deuschl G. Pains in Parkinson disease–many syndromes under one umbrella. Nat Rev Neurol. 2012;8:284–294. doi:10.1038/nrneurol.2012.54
21. Kubo S, Hamada S, Maeda T, et al. A Japanese multicenter survey characterizing pain in Parkinson’s disease. J Neurol Sci. 2016;365:162–166. doi:10.1016/j.jns.2016.04.015
22. Rodriguez-Violante M, Alvarado-Bolanos A, Cervantes-Arriaga A, Martinez-Martin P, Rizos A, Chaudhuri KR. Clinical determinants of Parkinson’s disease-associated pain using the King’s Parkinson’s disease pain scale. Mov Disord Clin Pract. 2017;4:545–551. doi:10.1002/mdc3.12469
23. Martinez-Martin P, Manuel Rojo-Abuin J, Rizos A, et al. Distribution and impact on quality of life of the pain modalities assessed by the King’s Parkinson’s disease pain scale. NPJ Parkinson's Dis. 2017;3:8. doi:10.1038/s41531-017-0009-1
24. Adewusi JK, Hadjivassiliou M, Vinagre-Aragon A, et al. Peripheral neuropathic pain in idiopathic Parkinson’s disease: prevalence and impact on quality of life; a case controlled study. J Neurol Sci. 2018;392:3–7. doi:10.1016/j.jns.2018.06.022
25. de Mattos DC, Meziat Filho NA, Pedron CA, et al. Their relationship with motor dysfunction in individuals with Parkinson disease-a cross-sectional study. Pain Pract. 2019;19:732–739. doi:10.1111/papr.12803
26. Young Blood MR, Ferro MM, Munhoz RP, Teive HA, Camargo CH. Classification and characteristics of pain associated with Parkinson’s disease. Parkinsons Dis. 2016;2016:6067132. doi:10.1155/2016/6067132
27. Defazio G, Antonini A, Tinazzi M, et al. Relationship between pain and motor and non-motor symptoms in Parkinson’s disease. Eur J Neurol. 2017;24:974–980. doi:10.1111/ene.13323
28. Vila-Cha N, Cavaco S, Mendes A, et al. Unveiling the relationship between central parkinsonian pain and motor symptoms in Parkinson’s disease. Eur J Pain. 2019;23:1475–1485. doi:10.1002/ejp.1413
29. Ozturk EA, Gundogdu I, Kocer B, Comoglu S, Cakci A. Chronic pain in Parkinson’s disease: frequency, characteristics, independent factors, and relationship with health-related quality of life. J Back Musculoskelet Rehabil. 2017;30:101–108. doi:10.3233/BMR-160720
30. Rana AQ, Qureshi ARM, Haris A, et al. Negative impact of severity of pain on mood, social life and general activity in Parkinson’s disease. Neurol Res. 2018;40:1054–1059. doi:10.1080/01616412.2018.1517852
31. Rana AQ, Qureshi ARM, Rahman N, Mohammed A, Sarfraz Z, Rana R. Disability from pain directly correlated with depression in Parkinson’s disease. Clin Neurol Neurosurg. 2017;160:1–4. doi:10.1016/j.clineuro.2017.05.022
32. Rana AQ, Qureshi ARM, Kachhvi HB, Rana MA, Chou KL. Increased likelihood of anxiety and poor sleep quality in Parkinson’s disease patients with pain. J Neurol Sci. 2016;369:212–215. doi:10.1016/j.jns.2016.07.064
33. Fu YT, Mao CJ, Ma LJ, et al. Pain correlates with sleep disturbances in Parkinson’s disease patients. Pain Pract. 2018;18:29–37. doi:10.1111/papr.12578
34. Tessitore A, Russo A, De Micco R, et al. Central pain processing in “drug-naive” pain-free patients with Parkinson’s disease. Hum Brain Mapp. 2017;39:932–940. doi:10.1002/hbm.23892
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.