Back to Journals » Drug Design, Development and Therapy » Volume 20
Oxycodone versus Sufentanil for Postoperative Analgesia and Early Recovery After Radical Gastrectomy: A Propensity Score-Matched Study
Authors Wang Y ![]() , Hu L, Chen Z, Tao X, Zhou M, Bian Q, Liu H
, Hu L, Chen Z, Tao X, Zhou M, Bian Q, Liu H
Received 2 March 2026
Accepted for publication 20 May 2026
Published 28 May 2026 Volume 2026:20 606394
DOI https://doi.org/10.2147/DDDT.S606394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Yudong Wang,1,2,* Lei Hu,1,* Zeng Chen,3,* Xirong Tao,1 Miao Zhou,3 Qingming Bian,3 Hui Liu1
1School of Anesthesiology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Faculty of Medicine, Yangzhou University, Yangzhou, Jiangsu, People’s Republic of China; 3Department of Anesthesiology, The Affiliated Cancer Hospital of Nanjing Medical University, Jiangsu Cancer Hospital, Jiangsu Institute of Cancer Research, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingming Bian, Department of Anesthesiology, The Affiliated Cancer Hospital of Nanjing Medical University, Jiangsu Cancer Hospital, Jiangsu Institute of Cancer Prevention and Treatment, No. 42 Baiziting, Nanjing, Jiangsu, 210009, People’s Republic of China, Email [email protected] Hui Liu, School of Anesthesiology, Xuzhou Medical University, No. 209 Tongshan Road, Xuzhou, Jiangsu, 221004, People’s Republic of China, Tel +86 13813043213, Email [email protected]
Background: Radical gastrectomy is associated with trauma and severe pain. We examined whether oxycodone could improve postoperative analgesia and early recovery compared with sufentanil in patients undergoing radical gastrectomy.
Methods: Patients who underwent radical gastrectomy with patient-controlled intravenous analgesia (PCIA) based on sufentanil or oxycodone for postoperative pain management from January 2022 to December 2023 were included in this study. We used a 1:1 ratio propensity score matching (PSM) in our study to adjust for confounding factors and differences between groups. Patient demographics, surgical and anesthesia details, analgesic effects, and recovery profiles were recorded and analyzed.
Results: After PSM, 224 patients were included in each group. Oxycodone treatment was associated with improved pain scores at rest and during movement at 2 h postoperatively (P< 0.001), fewer rescue analgesics (P=0.005), shorter time to first flatus and defecation (P=0.030; P=0.016), reduced indwelling nasogastric tube time (P=0.043), shorter length of hospital stay (P=0.031), and lower incidence of nausea in the matched cohort (P=0.049). There were significantly higher lymphocytes (POD1 and POD3: all P< 0.001), CD4+ T cells (POD1: P=0.003; POD3: P< 0.001) and CD4+/CD8+ T cell ratio (POD1 and POD3: all P< 0.001), and lower CD8+ T cells (POD1: P=0.001; POD3: P< 0.001). Subgroup analysis stratified by age, surgical technique, and resection extent demonstrated no significant interaction effects across all variables (P-interaction > 0.05).
Conclusion: Compared with sufentanil, oxycodone-based PCIA was associated with lower early postoperative pain scores, reduced immune suppression and fewer adverse reactions, and faster gastrointestinal function recovery.
Keywords: oxycodone, sufentanil, analgesia, postoperative recovery, immune function, gastrointestinal function
Introduction
Gastric cancer (GC) is the fifth most common cancer and the fifth most common cause of cancer death globally.1 Surgery significantly improves prognosis in GC patients,2 but radical gastrectomy involves a variety of complex procedures—including extensive exploration, lymph node dissection, and digestive tract reconstruction, which is a severe trauma to the body. Patients undergoing radical gastrectomy often experience moderate to severe postoperative pain, particularly visceral pain, which can significantly impact their recovery and quality of life.3,4
Patient-controlled intravenous analgesia (PCIA) is widely utilized for its efficacy in tailoring pain relief to individual needs. Oxycodone and sufentanil are commonly used opioids in PCIA for postoperative analgesia. Although these two drugs have been compared in various postsurgical settings, with variable efficacy and adverse effects being reported, the clinical relevance of these differences remains debated.5–7 Previous studies have largely focused on the simple comparison of the analgesic efficacy.7,8 However, there is a lack of comprehensive research on their effects on various perioperative indicators, which are of great significance for patients’ overall recovery and prognosis.
Patients with GC are an immunologically heterogeneous group with varying degrees of immunosuppression.9 The use of opioids may further exacerbate the suppression of immune function in these patients.10 Clinical evidence supports this concern: in 60 patients undergoing surgery for GC, morphine-treated patients showed decreased T and NK cell numbers at 2 h after incision, and NK cell numbers had not returned to baseline at 5 days after surgery. In contrast, patients in the flurbiprofen group exhibited higher NK cell numbers at 2 h and higher T and NK cell numbers at 1 day, despite similar levels of analgesia.11 Similarly, in a randomized controlled trial of 25 patients undergoing neck surgery, fentanyl suppressed NK cell cytotoxicity more than flurbiprofen on day 1.12 An impaired immune function following surgery can adversely affect patients by increasing the survival rate of tumor cells, elevating the rates of recurrence and metastasis, raising the incidence of systemic and wound infections, and sepsis, as well as delaying wound healing.13 Postoperative gastrointestinal dysfunction (POGD) is also a frequent occurrence after abdominal surgery, which contributes to patient discomfort and increased healthcare costs.14 Opioid use may exacerbate POGD by activation of gastrointestinal opioid receptors.15 Additionally, given that opioids undergo hepatic metabolism and renal excretion, understanding their effects on liver and renal function is essential.
All commonly used traditional opioid analgesic drugs have effects on these functions to a different extent.16 In this retrospective study, we compared the analgesic efficacy of oxycodone versus sufentanil for postoperative analgesia and evaluated their impacts on cellular immune function, gastrointestinal function, and liver and renal function in patients undergoing radical gastrectomy, aiming to provide evidence for optimizing postoperative analgesia and enhancing early recovery.
Materials and Methods
Study Design and Setting
This was a single-center, retrospective cohort study. The study was approved by the Ethics Committee of Jiangsu Cancer Hospital (KY-2024-007) and registered in the Chinese Clinical Trial Registry (www.Chictr.org.cn; ChiCTR2400080651). The ethics committee granted a waiver of written consent because of the retrospective nature of the study. All patient data were de-identified and handled in strict compliance with confidentiality requirements. This study was conducted in accordance with the principles of the Declaration of Helsinki.
All patients were enrolled from the database of Jiangsu Cancer Hospital. From January 2022 to December 2023, patients who underwent radical gastrectomy with PCIA based on sufentanil or oxycodone for postoperative pain management were included using the same inclusion and exclusion criteria. All gastrectomies were performed by the same surgical team according to the standard of radical gastrectomy of the latest edition of Japanese gastric cancer treatment guidelines.17 Exclusion criteria were defined as follows: (1) a history of severe heart, liver, or kidney insufficiency; (2) chronic pain syndromes or a history of analgesic use within the past 6 months; (3) immunosuppressive therapy or immunosuppressive disorders; (4) patients with benign gastric tumors, gastrointestinal stromal tumors, or combined with other organ malignancies, and residual GC; (5) intraoperative bleeding>1000 mL or duration of surgery>6 h; (6) analgesic pumps with different parameters; (7) receipt of regional blocks or adjunct anesthetic techniques. According to the formula of the pump, patients were allocated to two groups: the oxycodone group (oxycodone 1 mg/kg + tropisetron 8 mg + saline to 100 mL), sufentanil group (sufentanil 1 μg/kg + tropisetron 8 mg + saline to 100 mL). The dose ratio (1 mg: 1 μg) of oxycodone to sufentanil was selected based on previously reported equianalgesic ratios.8,18
Anesthesia Method
All patients received standardized general anesthesia induced with 0.04~0.06 mg/kg midazolam, 1.0~2.0 mg/kg propofol, 2~3 μg/kg fentanyl, and 0.6 mg/kg rocuronium. Subsequently, their trachea was intubated, and the patient was positioned in the supine position. Anesthesia was maintained with continuous propofol, remifentanil, rocuronium, and dexmedetomidine. Vasoactive medication (phenylephrine, ephedrine, or norepinephrine) and fluid administration were given at the discretion of the attending anesthesiologist. Once the abdomen was closed, the oxycodone group was given 8 mg tropisetron and 0.1 mg/kg oxycodone. The sufentanil group was administered 8 mg tropisetron and 0.1 μg/kg sufentanil.
All patients were managed by the acute pain service (APS). After the end of surgery, patients were transferred to the post-anesthesia care unit where PCIA was initiated. Postoperative pain was evaluated on the numerical rating scale (NRS) by the APS staff of the hospital in the range of 0–10, 0 was no pain and 10 was the maximum possible pain at rest and during movement at 2 h, 24 h, and 48 h after surgery. When patients had an NRS score of more than 4, 50 mg of tramadol was injected by the APS staff. The degree of sedation was evaluated with the Ramsay sedation scale (RSS) by the APS staff of the hospital at 2 h, 24 h, and 48 h after surgery.19 The activities of daily living (ADL) were evaluated with the Barthel Index (BI, the higher the score, the greater the activities of daily living) by the nursing staff before surgery, and 0 to 5 days after surgery.20 Venous blood was drawn from all patients before surgery and on postoperative day 1 (POD1) and postoperative day 3 (POD3) for the assessment of lymphocyte counts, liver and kidney function. All data were recorded on the hospital’s electronic patient record (EPR) system and electronic anesthesia record-keeping system, which are both standard documentation tools in our institute.
Data Collection
Data related to postoperative analgesia were extracted from the AI-PCA system (Jiangsu Rehn Medical Instruments Technology Co., Ltd.) database of Jiangsu Cancer Hospital. Other data were retrospectively extracted from the hospital’s EPR system and electronic anesthesia record-keeping system and consisted of baseline characteristics (sex, age, weight, height, medical history and ASA physical status), surgical characteristics (surgical technique, resection extent, extent of lymph node dissection, pathological stage, duration of surgery), anesthesia characteristics (type and specifics of analgesic method, intraoperative medication administration, blood loss, blood transfusion, urine output, fluid input), postoperative characteristics (occurrence of postoperative adverse reactions, RSS scores, first day of defecation, first day of flatus, time of indwelling nasogastric tube, time of indwelling nasojejunal tube, length of hospital stay after surgery, immune function (counts of lymphocyte subsets), liver and renal function (serum creatinine [SCR], blood urea nitrogen [BUN], albumin [ALB], alanine aminotransferase [ALT], aspartate aminotransferase [AST], lactate dehydrogenase [LDH]) and ADL. Postoperative pain characteristics consisted of the use of rescue analgesics, the number of PCIA presses, and NRS pain scores. For exploratory post‑hoc analysis, 2-year survival data were collected via telephone follow‑up. All patients or their family members were contacted to ascertain survival status, date of death (if applicable), and cause of death. The primary outcome was the NRS pain scores during movement at 2 h postoperatively.
Statistical Analysis
SPSS 26 (IBM Corp., Armonk, NY, USA) was used to perform statistical analysis of the demographic and clinical data. All figures were prepared using GraphPad Prism version 10.3 (GraphPad Inc., Salt Lake City, UT, USA). Missing data were largely assumed to be missing at random. There were no missing data for the primary outcome, and missing data for all secondary outcomes were less than 5%, so we did not perform an imputation of missing data.
To reduce bias related to the non-randomized and observational study design, we applied propensity score matching (PSM) analysis to the oxycodone and sufentanil groups. Propensity scores were estimated using a logistic regression model based on the following preoperative characteristics: age, sex, body mass index (BMI), ASA physical status, surgical technique, resection extent, extent of lymph node dissection, pathological stage, duration of surgery, medical history, fluid input, patients requiring transfusion, blood loss, and urine output. A 1:1 nearest neighbor matching without replacement was applied with a caliper width of 0.02 standard deviations of the logit propensity score.
The Shapiro–Wilk test was performed to analyze the normality of the measurement data. Normally distributed measurement data are presented as mean±standard deviation (SD). The differences between the two groups were compared using the t-test, and repeated-measures data were analyzed using generalized estimating equations. The treatment × time interaction was tested first. If significant, between-group differences at each time point were tested at α=0.05. If not significant, the treatment main effect was tested next. If significant, then between-group differences at each time point were tested at α=0.05. Otherwise, the Bonferroni correction was applied at each time point.21 Counting data are expressed as frequencies and rates, and categorical variables were tested using the chi-square test or Fisher’s test. Measurement data that show a nonnormal distribution are presented as the median (quartile) [M (Q25, Q75)], and the Mann–Whitney U-test was applied. To elucidate the underlying heterogeneity in the influence of oxycodone and sufentanil on postoperative analgesia, we conducted prespecified subgroup analysis stratified by age (< 65 vs ≥ 65), surgical technique (laparoscopy vs open), and resection extent (distal vs total). Interaction effects were formally tested by calculating interaction P-values (P-interaction) through regression models incorporating multiplicative interaction terms. Forest plots were used to visualize the predictive effects within these subgroups and the consistency of treatment effects across variables. In the exploratory analysis, overall survival (OS) and 1‑year mortality were assessed. All patients had a minimum potential follow‑up of 2 years, ensuring complete observation of the 1‑year and 2‑year time windows without informative censoring. OS was defined as the time from surgery to death from any cause, with surviving patients censored at the date of last follow‑up. OS curves were estimated using the Kaplan‑Meier method and compared between groups with the log‑rank test. One‑year mortality was calculated as the proportion of patients who died within 1 year after surgery and compared using the chi‑square test or Fisher’s test. All statistical tests were two-sided and statistical significance was set at P<0.05.
Results
Patient Characteristics of the Pooled and Matched Cohorts
A total of 709 patients were assessed for eligibility from January 2022 to December 2023. But following the exclusion criteria, only 600 cases were included in our original cohort, and after PSM, the matched cohort was divided into two groups: oxycodone group (224 cases) and sufentanil group (224 cases). The study design and process are described in the diagram below (Figure 1).
 |
Figure 1 Flow chart of the study. |
The demographic and intraoperative characteristics of the original cohort and matched cohort are shown in Table 1. In the original cohort, the mean BMI of the patients in the sufentanil group was higher than that in the oxycodone group (mean in kg/m2 24.4 vs 23.2, P=0.002). The frequency of hypertension was significantly higher in the oxycodone group than the sufentanil group (41.6% vs 29.1%, P=0.026). After PSM, there were no significant differences in the mean age, sex, ASA physical status, surgical technique, resection extent, extent of lymph node dissection, pathological stage, duration of surgery, frequency of hypertension, diabetes mellitus, neurological disease, anemia, cardiovascular diseases, and fluid input, patients requiring transfusion, blood loss and urine output between the two groups.
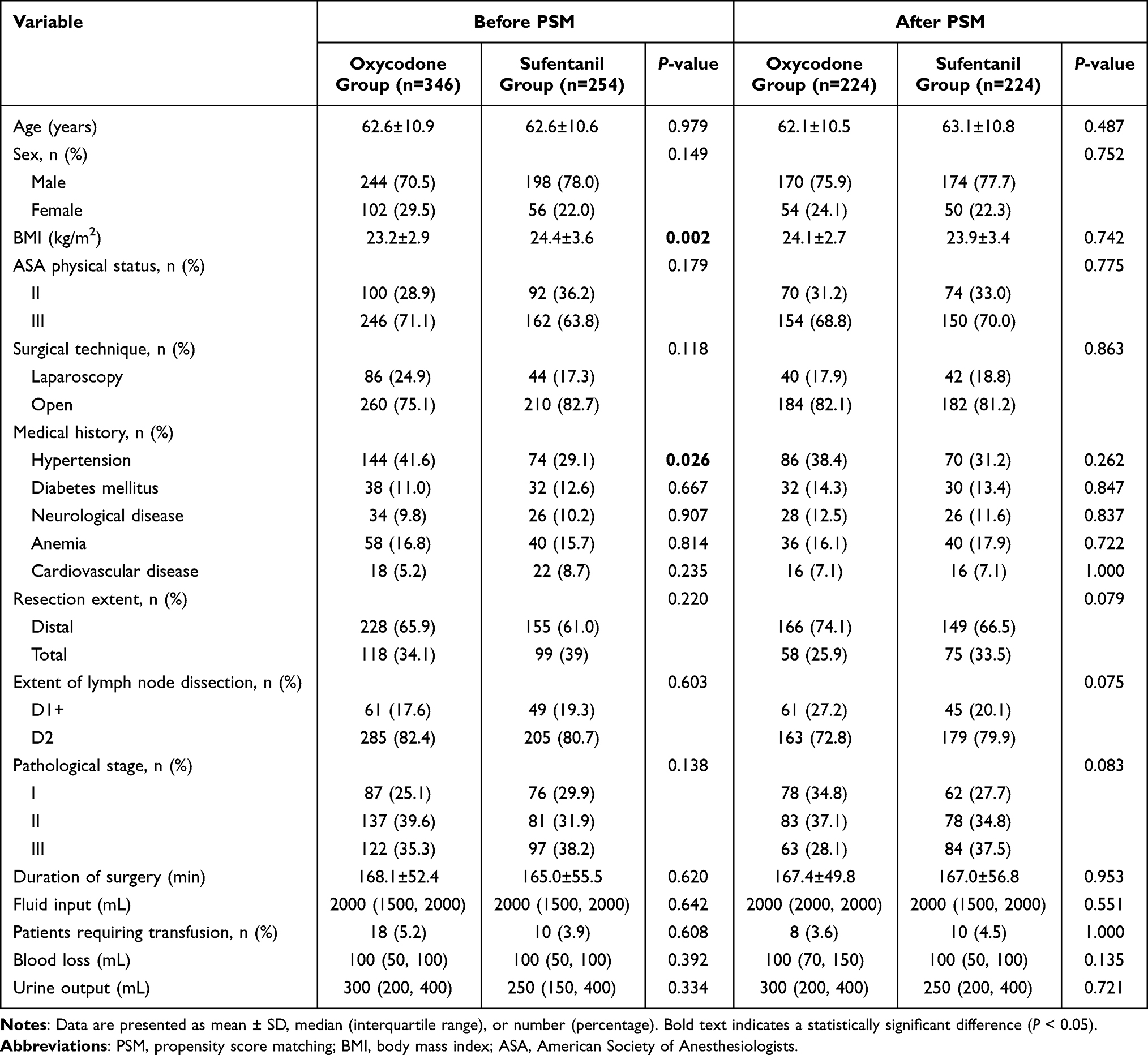 |
Table 1 Baseline Characteristics of the Patients Before and After PSM |
Analgesic Effects and Adverse Reactions
Repeated measurements results showed that the main effects of group and time between the two groups were significant regarding pain scores at rest and during movement. Trends in pain scores at rest and during movement decreased over time in both groups. Compared with sufentanil, oxycodone reduced pain scores at rest and during movement. Patients in the oxycodone group showed lower mean NRS scores at rest at 2 h postoperatively than sufentanil patients (1.94±0.82 vs 2.95±0.97, P<0.001). Similar differences were observed in pain scores during movement at the same time point (3.13±0.94 vs 4.04±0.84, P<0.001). In contrast, the two groups had similar NRS pain scores at 24 and 48 h postoperatively (Figure 2 and Table 2).
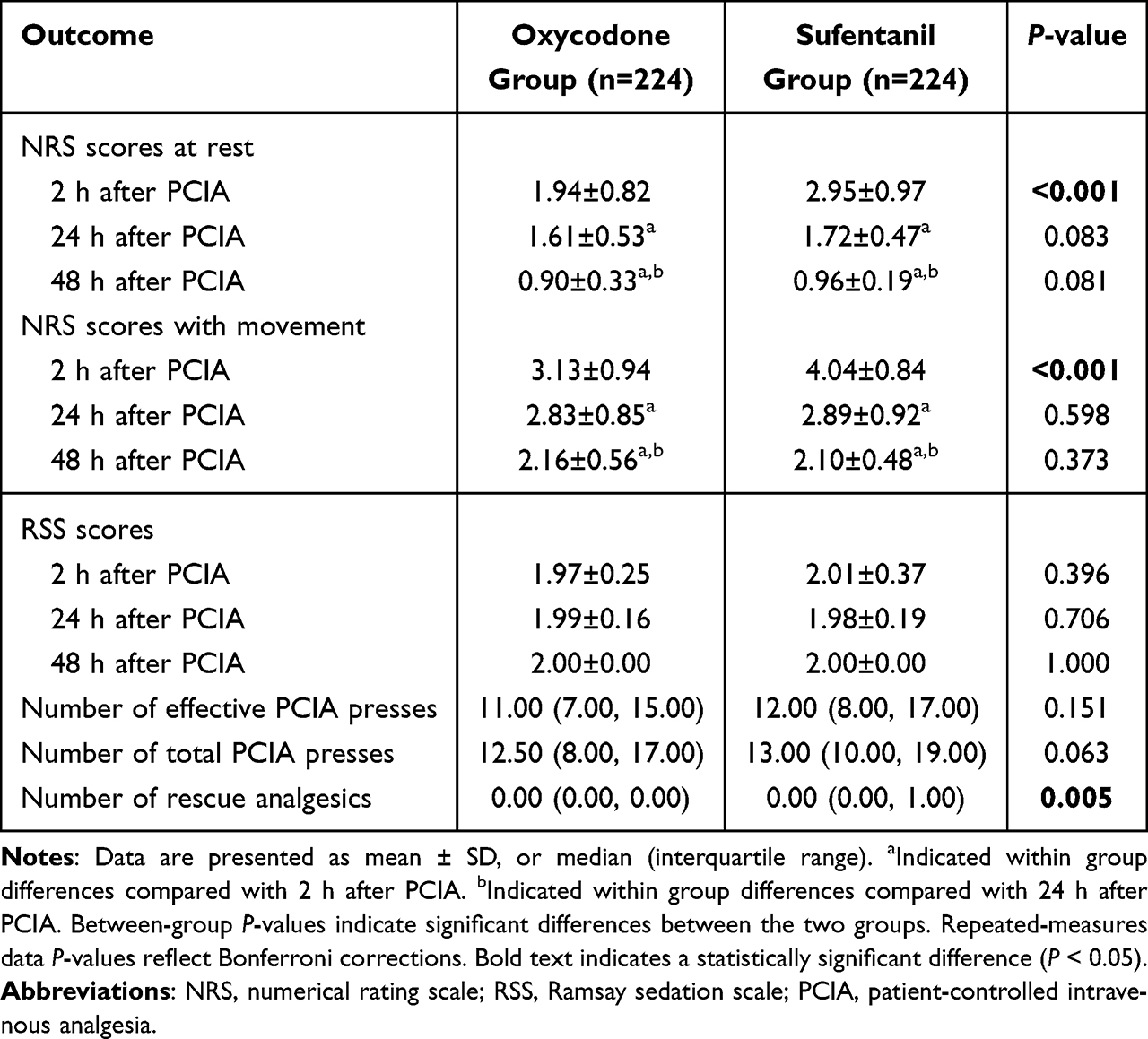 |
Table 2 Comparison of Analgesic Effects and RSS Scores Between the Two Groups |
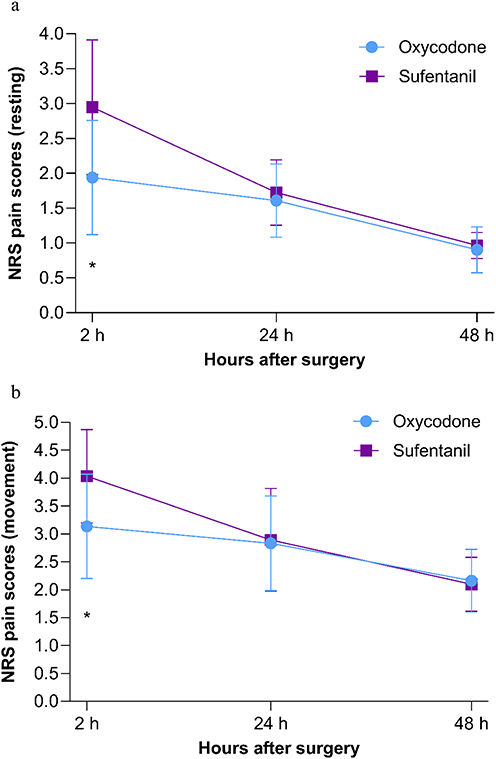 |
Figure 2 Comparison of NRS pain scores (a) at rest and (b) during movement between groups. *P<0.05. Abbreviation: NRS, numeric rating scale. |
The number of effective PCIA presses and total PCIA presses were similar between the two groups (all P > 0.05). However, the number of required rescue analgesics postoperatively was lower in patients in the oxycodone group (0.00 [0.00, 0.00] vs 0.00 [0.00, 1.00], P=0.005; Table 2).
Postoperative incidence of vomiting, dizziness, and other adverse reactions was similar between the oxycodone and sufentanil groups. However, oxycodone treatment was associated with a lower incidence of nausea compared with sufentanil (10 [4.5] vs 26 [11.6], P=0.049; Table 3).
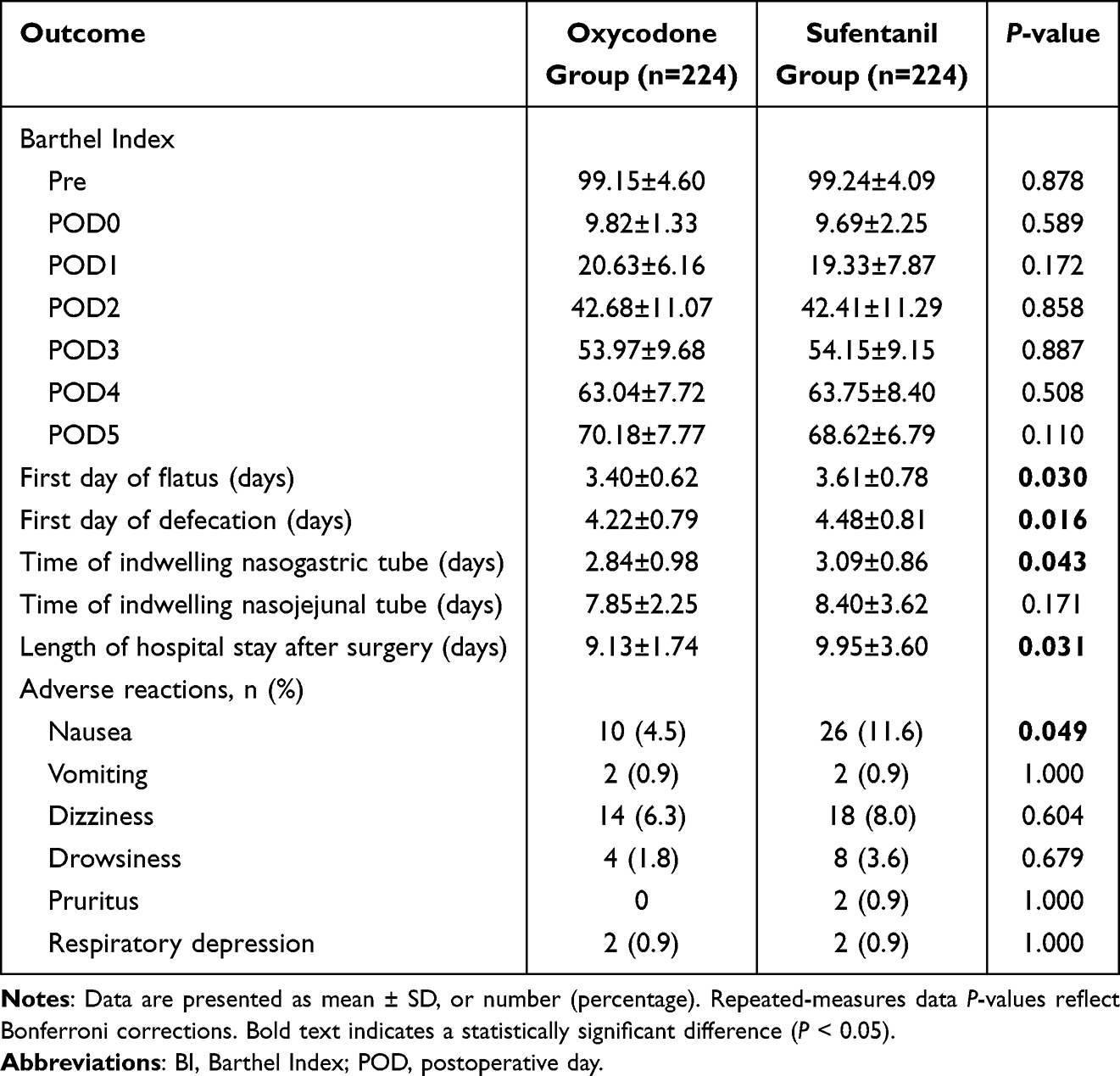 |
Table 3 BI Scores, Postoperative Gastrointestinal Function, Length of Hospital Stay After Surgery, and Adverse Reactions Related to Analgesic Procedures Between the Two Groups |
Lymphocyte Subsets, Liver Function, and Renal Function
Before surgery, all measured variables were within their reference range and did not significantly differ between groups (Table 4 and Supplementary Figure S1).
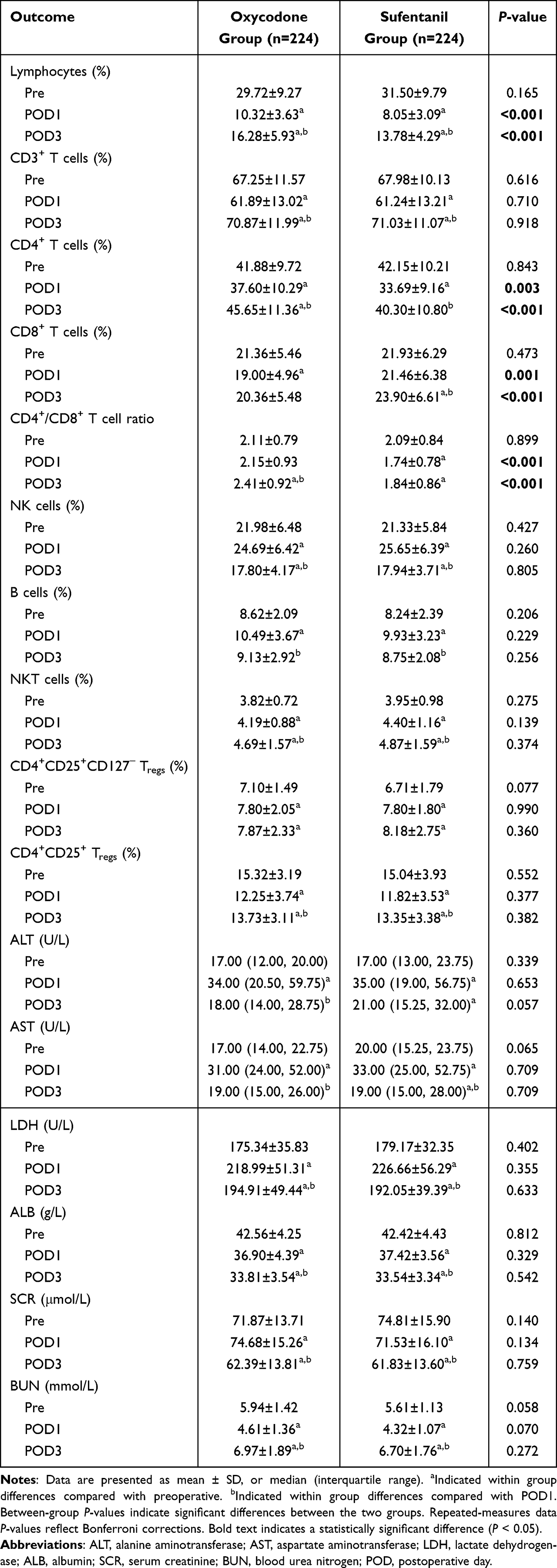 |
Table 4 Lymphocyte Subsets, Liver Function, and Renal Function Between the Two Groups |
Compared with the preoperative levels in all groups, lymphocytes and CD4+CD25+ Tregs significantly decreased on POD1 and POD3. The CD3+ T cells and CD4+ T cells showed a downward trend on POD1 and an upward trend on POD3. The NK cells and B cells showed an upward trend on POD1 and a downward trend on POD3. The NKT cells and the CD4+CD25+CD127− Tregs significantly increased on POD1 and POD3 compared with the preoperative levels. The levels of CD8+ T cells in the oxycodone group decreased after POD1, while the sufentanil group increased significantly at POD3 compared with the preoperative levels. The CD4+/CD8+ T cell ratio in the oxycodone group increased on POD3, while the sufentanil group decreased significantly at POD1 and POD3 compared with the preoperative levels (Table 4 and Supplementary Figure S1).
Lymphocytes (POD1: 10.32±3.63 vs 8.05±3.09, P<0.001; POD3: 16.28±5.93 vs 13.78±4.29, P<0.001), CD4+ T cells (POD1: 37.60±10.29 vs 33.69±9.16, P=0.003; POD3: 45.65±11.36 vs 40.30±10.80, P<0.001) and CD4+/CD8+ T cell ratio (POD1: 2.15±0.9 vs 1.74±0.78, P<0.001; POD3: 2.41±0.92 vs 1.84±0.86, P<0.001) on POD1 and POD3 were higher in the oxycodone group compared with the sufentanil group. The CD8+ T cells on POD1 and POD3 were lower in the oxycodone group compared with the sufentanil group (POD1: 19.00±4.96 vs 21.46±6.38, P=0.001; POD3: 20.36±5.48 vs 23.90±6.61, P<0.001). The CD3+ T cells, NK cells, B cells, NKT cells, CD4+CD25+CD127− Tregs, and CD4+CD25+ Tregs among the two groups at each time point demonstrated no significant differences (Table 4 and Supplementary Figure S1).
The levels of ALT, AST, LDH, ALB, SCR, and BUN did not significantly differ between groups. Postoperative changes in ALT, AST, LDH, ALB, SCR, and BUN levels relative to baseline are shown in Table 4.
Gastrointestinal Function
The mean time to first flatus (3.40±0.62 vs 3.61±0.78, P=0.030), time to first defecation (4.22±0.79 vs 4.48±0.81, P=0.016), and time of indwelling nasogastric tube (2.84±0.98 vs 3.09±0.86, P=0.043) were significantly shorter in the oxycodone group than in the sufentanil group. There was no statistically significant difference between groups in the time of indwelling nasojejunal tube (Table 3).
BI Scores, RSS Scores, and the Length of Hospital Stay After Surgery
The oxycodone and sufentanil groups showed no significant differences in mean BI scores and RSS scores at each time point (Table 2 and Table 3). Oxycodone treatment reduced the length of hospital stay after surgery compared with sufentanil (9.13±1.74 vs 9.95±3.60, P=0.031; Table 3).
Subgroup Analysis
This study demonstrated a consistent association between oxycodone and reduced pain scores at rest and during movement at 2 h postoperatively across all patient subgroups, with no significant interaction effects detected (all P-interaction >0.05), suggesting homogeneity in the correlation of oxycodone with pain scores at rest and during movement at 2 h postoperatively reduction among patients with varying clinical characteristics (Figure 3).
 |
Figure 3 Forest plot of the subgroup analysis for the primary outcome. |
Exploratory Survival Outcomes
In the exploratory analysis, 182 patients in the oxycodone group and 193 patients in the sufentanil group were successfully followed for at least 2 years. The 2‑year OS rate was 87.4% (159/182) in the oxycodone group and 90.2% (174/193) in the sufentanil group. Kaplan‑Meier analysis showed no statistically significant difference in OS between the two groups (P = 0.426; Supplementary Figure S2). One‑year mortality was 3.8% (7/182) in the oxycodone group and 4.1% (8/193) in the sufentanil group, with no significant difference detected (P = 0.883).
Discussion
This retrospective cohort study suggests that oxycodone-based PCIA was associated with improved early postoperative analgesia and reduced immune suppression compared with sufentanil-based PCIA in patients undergoing radical gastrectomy. In addition, oxycodone was associated with a lower incidence of nausea, a shorter length of hospital stay after surgery, and faster recovery of gastrointestinal function.
Although oxycodone and sufentanil significantly reduced pain scores at rest and during movement at 2–48 h postoperatively, oxycodone was associated with lower pain scores at rest and during movement at 2 h postoperatively, lower use of postoperative rescue analgesia, and fewer adverse reactions. Our results suggest that oxycodone provided better analgesia than sufentanil after radical gastrectomy in the early period. Sufentanil is a Mu-opioid receptor (MOR)-specific agonist with powerful analgesic effects, but the analgesic effect of pure MOR agonism is unsatisfactory for relieving visceral pain, limiting its efficacy in gastrointestinal surgery. Oxycodone not only activates the MOR but also occupies the kappa-opioid receptor (KOR).22 KORs located within the gastrointestinal tract are significant factors for anti-nociception in the visceral pain system.23 Oxycodone produces effective postoperative analgesia by acting on both MOR and KOR. Additionally, oxycodone penetrates the blood brain barrier well, likely with the help of active transport,24 resulting in a fast onset of action, which compensates for its lower affinity for the MOR. These are possible explanations for the results. The lower incidence of nausea may be attributable to the weaker μ-receptor affinity of oxycodone compared with sufentanil,25 which mitigates the adverse reactions related to μ-receptor agonists. The subgroup analysis confirmed that these analgesic benefits were consistent across patient age, surgical technique, and extent of resection, supporting the generalizability of the findings.
Improving patient immune function in the perioperative period has been a focus of clinical research. In this study, we found that surgery significantly decreased the levels of lymphocytes, CD3+ T cells, and CD4+ T cells. The results obtained clearly confirm that a relevant suppression of cellular immune responses happens after surgery as in previous studies.26,27 Other important results derived from our study are that lymphocytes, CD4+ T cells, and CD4+/CD8+ T cell ratio on POD1 and POD3 were higher in the oxycodone group, and the CD8+ T cells on POD1 and POD3 were lower in the oxycodone group. These results suggest that oxycodone, rather than sufentanil, can accelerate the alleviation of postoperative immune suppression. Three possible explanations may account for the results. First, in vitro studies suggest that molecular structures which have a hydroxyl group at both C3 and C6 have the greatest immunosuppressive properties, while those opioids which have a carbonyl substitution at C6, a single bond between C7 and C8, and preferably a hydroxyl group at C14 (as in oxycodone) do not exhibit immunosuppressive effects, thereby conferring a potential advantage over other opioids.11 Second, oxycodone has much weaker μ-receptor affinity than sufentanil,23 which may mitigate the immune suppression related to μ-receptor agonism. The last possible explanation is that oxycodone provided better analgesia than sufentanil after radical gastrectomy in the early period. Adequate postoperative analgesia reduces the immunosuppressive effects of postoperative pain and stress responses.
POGD is a prevalent surgical complication of gastrointestinal surgery characterized by a transient impairment of gastrointestinal function.28 The etiology of POGD is multifactorial, with factors such as opioid usage, previous gastrointestinal surgery, nausea, vomiting, and increased postoperative pain.29,30 POGD has been consistently associated with prolonged hospital stay and delayed recovery,9,30 making its prevention a key objective of the enhanced recovery after surgery (ERAS) protocols. In this study, we found that patients in the oxycodone group had shorter time to first postoperative flatus and defecation, and shorter indwelling nasogastric tube time, showing a benefit in terms of improved recovery of gastrointestinal function as in previous study.31 Opioid medications have been associated with impairment of gastrointestinal motility.32 This is due to their overarching impact on the enteric nervous system via MOR, which can, for instance, result in prolonged gastrointestinal transit times.33 Oxycodone’s weaker MOR affinity relative to sufentanil would be expected to have a less pronounced inhibitory effect on gastrointestinal function. Furthermore, the better early analgesia and lower incidence of nausea observed in the oxycodone group may also have contributed to earlier mobilization and faster gastrointestinal recovery. Patients in the oxycodone group had a significantly shorter indwelling nasogastric tube time and a shorter indwelling nasojejunal tube time (although not statistically significant). The presence of tubes may cause discomfort and hinder patients’ mobility; it might also contribute to increasing patients’ anxiety and fear of accidents, thus delaying the recovery of gastrointestinal function further. In China, one of the major hospital discharge criteria after gastrointestinal surgery is the restoration of gastrointestinal function.34 In this study, a reduction was found in the length of hospital stay after surgery in patients in the oxycodone group, possibly because of fewer postoperative adverse reactions and faster recovery of gastrointestinal function. Therefore, oxycodone instead of sufentanil applied for PCIA may be useful for enhanced recovery after gastrectomy.
Opioid analgesics are primarily metabolized by the liver and primarily eliminated via the kidneys.35 Therefore, patients with liver or renal impairment are expected to have altered pharmacokinetics and safety of analgesics. The results of this study showed that the differences in liver and renal function between the two groups at different time points were not statistically significant, and failed to detect an advantage of oxycodone in terms of liver and renal function. Previous studies have found that oxycodone can be safely used in patients with mild to moderate liver injury, and oxycodone pretreatment significantly reduces postoperative serum creatinine levels and delivers renal protection.36,37 The absence of such differences in this study may reflect the inclusion of patients with normal baseline organ function, the short duration of postoperative analgesic exposure, and the limited follow‑up period for assessing long‑term changes.
In the exploratory analysis, no significant difference in OS or 1‑year mortality was observed between the oxycodone and sufentanil groups. These findings should be interpreted with caution because the survival endpoints were not prespecified, the study was not powered for survival comparisons, and the number of events was small. Moreover, although all patients had 2 years of follow‑up, this duration remains relatively short for GC. Therefore, these results should be regarded as hypothesis‑generating, and prospective trials with survival as a primary endpoint and longer follow‑up are warranted.
There are several limitations to this study. First, as a retrospective study, prospective sample size estimation was impractical. However, post-hoc power analysis confirmed adequate statistical power (> 80%) to detect clinically relevant effect sizes; residual risks of bias and unmeasured confounders persist in observational designs, even though the observed confounders were adjusted to an acceptable level using the PSM method. Second, the duration of follow‑up was relatively short, which precludes assessment of long‑term clinical outcomes. These outcomes are essential for evaluating patients’ long‑term postoperative recovery and prognosis. To partially address this, we conducted telephone follow‑up and performed an exploratory analysis of OS and 1‑year mortality, recognizing that these endpoints were not prespecified and the study was not powered for survival comparisons. Third, we conducted this study at a single center, which may limit the generalizability of our findings to patients with different populations or perioperative management. Multi-center, prospective, randomized controlled trials with longer follow‑up are needed to confirm our results. Additionally, more research could be done to investigate the effects of oxycodone with different dosages and multimodal analgesia strategies.
Conclusion
In conclusion, this study provides evidence that oxycodone-based PCIA was associated with lower postoperative pain in the early postoperative period, reduced immune suppression and fewer adverse reactions, and faster gastrointestinal function recovery compared with sufentanil-based PCIA in patients undergoing radical gastrectomy. These findings suggest that oxycodone may be a useful alternative to traditional opioids for PCIA as part of enhanced recovery protocols after gastrectomy, but prospective randomized controlled trials with longer follow‑up are required to confirm these observations and evaluate long‑term clinical outcomes.
Data Sharing Statement
Beginning six months after publication for a period of three years, the datasets used or analyzed during the present study will be available from the corresponding author (Hui Liu, [email protected]) upon reasonable request.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–14. doi:10.3322/caac.21834
2. Kakeji Y, Ishikawa T, Suzuki S, et al. A retrospective 5-year survival analysis of surgically resected gastric cancer cases from the Japanese Gastric Cancer Association nationwide registry (2001–2013). Gastric Cancer. 2022;25(6):1082–1093. doi:10.1007/s10120-022-01317-6
3. Rivas E, Cohen B, Pu X, et al. Pain and opioid consumption and mobilization after surgery: post Hoc analysis of two randomized trials. Anesthesiology. 2022;136(1):115–126. doi:10.1097/ALN.0000000000004037
4. Rollins KE, Lobo DN, Joshi GP. Enhanced recovery after surgery: current status and future progress. Best Pract Res Clin Anaesthesiol. 2021;35(4):479–489. doi:10.1016/j.bpa.2020.10.001
5. Feng X, Yang P, Liao Z, Zhou R, Chen L, Ye L. Comparison of oxycodone and sufentanil in patient-controlled intravenous analgesia for postoperative patients: a meta-analysis of randomized controlled trials. Chin Med J. 2023;136(1):45–52. doi:10.1097/CM9.0000000000002259
6. Li Y, Dou Z, Yang L, Wang Q, Ni J, Ma J. Oxycodone versus other opioid analgesics after laparoscopic surgery: a meta-analysis. Eur J Med Res. 2021;26(1):4. doi:10.1186/s40001-020-00463-w
7. Yu H, Tian W, Xu Z, et al. Patient-controlled intravenous analgesia with opioids after thoracoscopic lung surgery: a randomized clinical trial. BMC Anesthesiol. 2022;22(1):253. doi:10.1186/s12871-022-01785-4
8. Yang GW, Cheng H, Song XY, et al. Effect of oxycodone-based multimodal analgesia on visceral pain after major laparoscopic gastrointestinal surgery: a randomised, double-blind, controlled trial. Drug Des Devel Ther. 2024;18:1799–1810. doi:10.2147/DDDT.S464518
9. Hao X, Shen Y, Chen N, et al. Osteoprogenitor-GMP crosstalk underpins solid tumor-induced systemic immunosuppression and persists after tumor removal. Cell Stem Cell. 2023;30(5):648–664.e648. doi:10.1016/j.stem.2023.04.005
10. Kim R. Effects of surgery and anesthetic choice on immunosuppression and cancer recurrence. J Transl Med. 2018;16(1):8. doi:10.1186/s12967-018-1389-7
11. Shen JC, Sun HL, Zhang MQ, Liu XY, Wang Z, Yang JJ. Flurbiprofen improves dysfunction of T-lymphocyte subsets and natural killer cells in cancer patients receiving post-operative morphine analgesia. Int J Clin Pharmacol Ther. 2014;52(8):669–675. doi:10.5414/CP202027
12. Narahara H, Kadoi Y, Hinohara H, Kunimoto F, Saito S. Comparative effects of flurbiprofen and fentanyl on natural killer cell cytotoxicity, lymphocyte subsets and cytokine concentrations in post-surgical intensive care unit patients: prospective, randomized study. J Anesth. 2013;27(5):676–683. doi:10.1007/s00540-013-1597-5
13. Ackerman RS, Luddy KA, Icard BE, Piñeiro Fernández J, Gatenby RA, Muncey AR. The effects of anesthetics and perioperative medications on immune function: a narrative review. Anesth Analg. 2021;133(3):676–689. doi:10.1213/ANE.0000000000005607
14. Lu Y, Fang -P-P, Yu Y-Q, et al. Effect of intraoperative dexmedetomidine on recovery of gastrointestinal function after abdominal surgery in older adults. JAMA Network Open. 2021;4(10):e2128886. doi:10.1001/jamanetworkopen.2021.28886
15. Thomas KR, watt J, Wu CMJ, et al. Pain and Opioid-Induced Gut Microbial Dysbiosis. Biomedicines. 2022;10(8):1815. doi:10.3390/biomedicines10081815
16. Wodehouse T, Demopoulos M, Petty R, et al. A randomized pilot study to investigate the effect of opioids on immunomarkers using gene expression profiling during surgery. Pain. 2019;160(12):2691–2698. doi:10.1097/j.pain.0000000000001677
17. Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition). Gastric Cancer. 2023;26(1):1–25. doi:10.1007/s10120-022-01331-8
18. Quan Z, Luo C, Chi P, Wang L, He H. Analgesic effects of oxycodone relative to those of sufentanil, in the presence of midazolam, during endoscopic injection sclerotherapy for patients with cirrhosis and esophageal varices. Anesth Analg. 2018;127(2):382–386. doi:10.1213/ANE.0000000000003305
19. Ramsay MA, Savege TM, Simpson BR, Goodwin R. Controlled sedation with alphaxalone-alphadolone. Br Med J. 1974;2(5920):656–659. doi:10.1136/bmj.2.5920.656
20. Mahoney FI, Barthel DW. Functional evaluation: the barthel index. Md State Med J. 1965;14:61–65.
21. Kraus WE, Bhapkar M, Huffman KM, et al. 2 years of calorie restriction and cardiometabolic risk (CALERIE): exploratory outcomes of a multicentre, Phase 2, randomised controlled trial. Lancet Diabetes Endocrinol. 2019;7(9):673–683. doi:10.1016/S2213-8587(19)30151-2
22. Marie N, Noble F. Oxycodone, an opioid like the others? Front Psychiatry. 2023;14:1229439. doi:10.3389/fpsyt.2023.1229439
23. Muratspahić E, Deibler K, Han J, et al. Design and structural validation of peptide-drug conjugate ligands of the kappa-opioid receptor. Nat Commun. 2023;14(1):8064. doi:10.1038/s41467-023-43718-w
24. Olkkola KT, Kontinen VK, Saari TI, Kalso EA. Does the pharmacology of oxycodone justify its increasing use as an analgesic? Trends Pharmacol Sci. 2013;34(4):206–214. doi:10.1016/j.tips.2013.02.001
25. Zhang J, Tu Q, Gan J, et al. Preemptive anti-stress response effects of oxycodone versus sufentanil for patients undergoing cardiac valve replacement-a randomized controlled trial. Clin Pharmacol Drug Dev. 2020;9(3):321–329. doi:10.1002/cpdd.764
26. Xu Q, Cheng X, Sun H, et al. Effect of remimazolam- vs propofol-based intravenous anesthesia on surgical stress response and post-operative immune function in patients with gastric radical surgery. Drug Des Devel Ther. 2024;18:5183–5192. doi:10.2147/DDDT.S489167
27. Oh CS, Park HJ, Piao L, et al. Expression profiles of immune cells after propofol or sevoflurane anesthesia for colorectal cancer surgery: a prospective double-blind randomized trial. Anesthesiology. 2022;136(3):448–458. doi:10.1097/ALN.0000000000004119
28. Boeckxstaens G, Ayad S, Dukes G, et al. A randomized phase 2 study of the 5-HT4 receptor agonist felcisetrag for postoperative gastrointestinal dysfunction after bowel surgery. Am J Surg. 2024;234:162–171. doi:10.1016/j.amjsurg.2024.04.030
29. Zhu Q, Li X, Tan F, et al. Prevalence and risk factors for hypokalemia in patients scheduled for laparoscopic colorectal resection and its association with post-operative recovery. BMC Gastroenterol. 2018;18(1):152. doi:10.1186/s12876-018-0876-x
30. Wang B, Han D, Hu X, Chen J, Liu Y, Wu J. Perioperative liberal drinking management promotes postoperative gastrointestinal function recovery after gynecological laparoscopic surgery: a randomized controlled trial. J Clin Anesth. 2024;97:111539. doi:10.1016/j.jclinane.2024.111539
31. Guo M, Liu S, Gao J, Han C, Yang C, Liu C. The effects of fentanyl, oxycodone, and butorphanol on gastrointestinal function in patients undergoing laparoscopic hysterectomy: a prospective, double-blind, randomized controlled trial. BMC Anesthesiol. 2022;22(1):53. doi:10.1186/s12871-022-01594-9
32. Barletta JF, Asgeirsson T, Senagore AJ. Influence of intravenous opioid dose on postoperative ileus. Ann Pharmacother. 2011;45(7–8):916–923. doi:10.1345/aph.1Q041
33. Mark EB, Okdahl T, Kahlke DG, et al. Effects of opium tincture on gastrointestinal function and motility in healthy volunteers: a magnetic resonance imaging study. Neurogastroenterol Motil. 2024;36(12):e14941. doi:10.1111/nmo.14941
34. Guo J, Xu A, Sun X, et al. Combined surgery and extensive intraoperative peritoneal lavage vs surgery alone for treatment of locally advanced gastric cancer: the SEIPLUS randomized clinical trial. JAMA Surg. 2019;154(7):610–616. doi:10.1001/jamasurg.2019.0153
35. Malhotra BK, Schoenhard GL, de Kater AW, Friedmann N. The pharmacokinetics of oxycodone and its metabolites following single oral doses of Remoxy®, an abuse-deterrent formulation of extended-release oxycodone, in patients with hepatic or renal impairment. J Opioid Manag. 2015;11(2):157–169. doi:10.5055/jom.2015.0265
36. Tovoli F, De Lorenzo S, Samolsky Dekel BG, et al. Oral oxycodone/naloxone for pain control in cirrhosis: observational study in patients with symptomatic metastatic hepatocellular carcinoma. Liver Int. 2018;38(2):278–284. doi:10.1111/liv.13546
37. Gao S, He Q. Opioids and the kidney: two sides of the same coin. Front Pharmacol. 2024;15:1421248. doi:10.3389/fphar.2024.1421248
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Intrathecal Sufentanil at Different Doses on Postoperative Pain Relief and Opioid Consumption in Elderly Patients Undergoing Lower Limb Orthopedic Surgery: A Randomized Controlled Trial
Li Y, Gu Y, Liu W, Liu X, Wang F, Tian B, Zhou W, Ye Q
Journal of Pain Research 2025, 18:2439-2451
Published Date: 15 May 2025