Back to Journals » Biologics: Targets and Therapy » Volume 19
OX40/OX40L as a Therapeutic Target in Atopic Dermatitis: A Scoping Review
Authors Valenzuela F ![]() , Meza V
, Meza V ![]()
Received 9 December 2024
Accepted for publication 11 April 2025
Published 2 May 2025 Volume 2025:19 Pages 281—288
DOI https://doi.org/10.2147/BTT.S511125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Shein-Chung Chow
Fernando Valenzuela,1,2 Victor Meza1
1Department of Dermatology, Universidad de Los Andes, Santiago, Chile; 2Department of Dermatology, Universidad de Chile, Santiago, Chile
Correspondence: Fernando Valenzuela, Department of Dermatology, Universidad de Los Andes, Santiago, Chile, Monseñor Álvaro del Portillo, Santiago, 12455, Chile, Email [email protected]
Abstract: Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disease, whose pathophysiology involves a complex interplay of genetic and environmental factors that lead to dysregulated T-cell-mediated inflammatory pathways and a compromised skin barrier. Despite the recent introduction of novel targeted therapies for moderate-to-severe AD, many patients still fail to achieve or maintain treatment goals, or experience treatment-emergent adverse events, which continue to burden their disease management. Recently, the role of T cell co-stimulatory molecule OX40 and its ligand OX40L, which is mainly expressed on professional antigen-presenting cells such as dendritic cells, has attracted widespread research attention as a potential therapeutic target in T cell-mediated skin diseases. Moreover, early basic and clinical research has shown encouraging results regarding the efficacy and safety of therapies targeting the OX40-OX40L axis in moderate-to-severe AD. Therefore, herein we aim to summarize the current evidence regarding the efficacy and safety of inhibiting the OX40/OX40L signaling axis in patients with moderate-to-severe AD.
Keywords: atopic dermatitis, eczema, OX40, OX40L, amlitelimab, rocatinlimab, telazorlimab, targeted therapies
Introduction
Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin condition that affects approximately 15–20% of children and 2–10% of adults worldwide.1–3 Clinically, it is characterized by pruritic eczematous lesions and is often associated with sleep disturbances, as well as allergic, cardiovascular, and neuropsychiatric comorbidities, significantly impacting patients’ overall quality of life.2
The pathophysiology of AD involves a complex interplay of genetic and environmental factors, leading to a compromised skin barrier and dysregulation of inflammatory pathways mediated predominantly by T helper (Th)2 cells.2 This inflammation is triggered by antigen stimulation of T-cell receptors and the engagement of costimulatory molecules, particularly those in the tumor necrosis factor (TNF) receptor superfamily, such as OX40.4 OX40 is an inducible costimulatory receptor predominantly expressed on activated T cells, especially Th2 cells, but also on Th1,4,5 Th17, and Th22 cells that may play roles in the later stages of the disease.3,5 Notably, OX40 is not expressed on naive CD4+ or CD8+ T cells.3
Upon antigen stimulation, OX40 is rapidly and transiently expressed on effector and memory T cells, where it binds to OX40 ligand (OX40L), primarily found on antigen-presenting cells (APCs) such as Langerhans cells, dendritic cells, B cells, type 2 innate lymphoid cells (ILC2), fibroblasts, endothelial cells, and mast cells.3,6 This interaction facilitates the trimerization of OX40 monomers, the recruitment of TNF receptor-associated factor (TRAF) proteins, and the activation of downstream signaling pathways, including nuclear factor kappa B (NF-κB) and phosphoinositide 3-kinase (PI3K)/Akt.3,6 These processes enhance effector T cell proliferation and survival, promote the generation of memory T cells, and increase the production of pro-inflammatory cytokines, which perpetuate the inflammatory cycle and contribute to chronic itch and skin barrier dysfunction—two key features of AD.3,7,8 Among these pro-inflammatory cytokines, interleukins (IL) produced by Th2 cells, ILC2 and basophils (IL-4, IL-5, IL-13, IL-31), as well as those keratinocyte-derived (IL-25, IL-33 and thymic stromal lymphopoietin) are predominant, with Th1-, Th17- and Th22-derived cytokines becoming subsequently involved as disease progresses.3,6–8
Given the critical role of the OX40/OX40L signaling pathway in both effector and memory T cells, its blockade may offer sustained inhibition of T-cell-mediated inflammation.3,7,8 Recent clinical trials have investigated the effects of antibodies targeting OX40 (Rocatinlimab or Telazorlimab) or OX40L (Amlitelimab) in patients with moderate-to-severe AD, a population for whom effective long-term treatment options remain limited. This review aims to summarize the current evidence regarding the efficacy and safety of inhibiting the OX40/OX40L signaling axis in these patients.
Materials and Methods
A comprehensive search for relevant studies was conducted in the PubMed and ClinicalTrials.gov databases. The search terms included (“OX40” OR “OX40L” OR “Amlitelimab” OR “KY1005” OR “Rocatinlimab” OR “AMG451” OR “KHK4083” OR “Telazorlimab” OR “GBR 830” OR “ISB830”) AND (“Atopic dermatitis” OR “eczema” OR “xerosis” OR “eczematous skin diseases”). We included articles published in the last 20 years that were available in full text in English or Spanish and focused on the OX40/OX40L axis in AD. Animal studies were excluded from the review. Additionally, the references of the included articles were screened for further relevant studies.
Results
Amlitelimab (KY1005)
Amlitelimab is a non-depleting human IgG4 monoclonal antibody (mAb) that binds to OX40L, effectively blocking OX40 stimulation and subsequently impeding T-cell-mediated inflammatory responses9–11 (Figure 1). Its effects on AD have been investigated in phase 1, phase 2a, and phase 2b trials (Table 1).
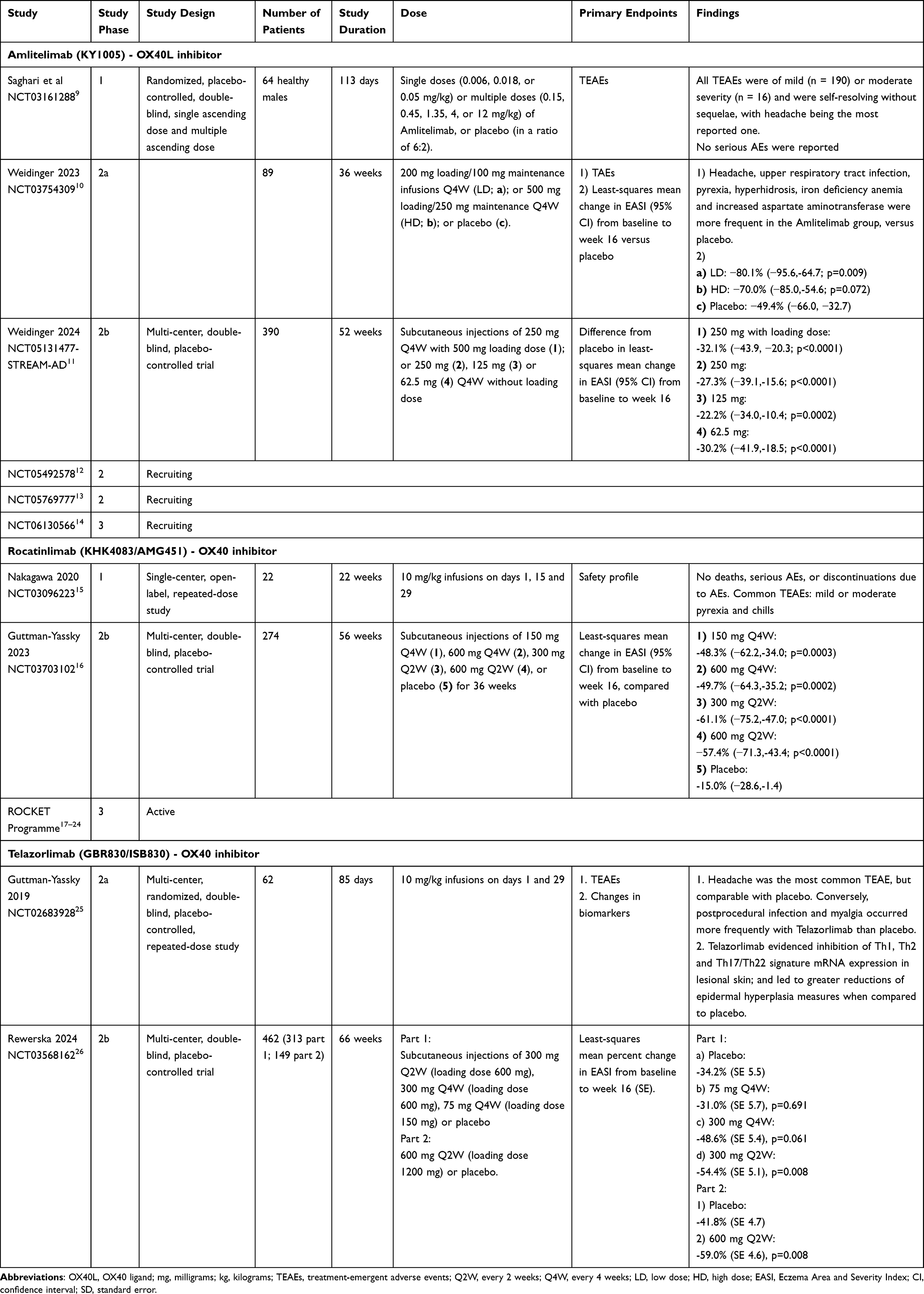 |
Table 1 Summary of Clinical Trials Targeting OX40/OX40L Signaling in Patients with Moderate-to-Severe Atopic Dermatitis |
 |
Figure 1 Novel therapies targeting the OX40/OX40L costimulatory signaling pathway include monoclonal antibodies against OX40 (telazorlimab and rocatinlimab) and OX40L (amlitelimab). Abbreviations: APC, Antigen-presenting cell; Th, T-helper; IL, interleukin; OX40L, OX40 ligand. |
The phase 1 trial conducted by Saghari et al9 assessed the safety, tolerability, and immunogenicity of Amlitelimab. This study randomized 64 healthy male subjects (mean age 26.5 ± 6.0 years) to receive single doses (0.006, 0.018, or 0.05 mg/kg) or multiple doses (0.15, 0.45, 1.35, 4, or 12 mg/kg) of Amlitelimab or placebo (in a 6:2 ratio). All treatment-emergent adverse events (TEAEs) were classified as mild (n = 190) or moderate (n = 16), resolving without complications, with headaches being the most frequently reported. No serious adverse events were observed.
Following this, a phase 2a double-blind, randomized, controlled trial by Weidinger et al10 included 89 patients with moderate-to-severe AD who were intolerant or had inadequate responses to topical treatments. Participants were randomized in a 1:1:1 ratio to receive intravenous Amlitelimab at low dose (LD, 200 mg loading/100 mg maintenance every 4 weeks [Q4W], n = 29), high dose (HD, 500 mg loading/250 mg maintenance Q4W, n = 30), or placebo (n = 29). At week 16, the LD and HD Amlitelimab groups demonstrated mean percentage changes from baseline in Eczema Area and Severity Index (EASI) scores of 80% and 70%, respectively, compared to 49% in the placebo group. Additionally, 44% and 37% of patients receiving LD or HD Amlitelimab achieved Investigator Global Assessment (IGA) scores of 0/1, while only 8% of those on placebo did. Patients treated with Amlitelimab also showed reductions in serum levels of pro-inflammatory cytokines IL-13 and IL-22. Common TEAEs included headache (10% vs 3% with placebo), upper respiratory tract infection (10% vs 3%), hyperhidrosis (7% vs 0%), pyrexia (7% vs 0%), iron-deficiency anemia (7% vs 0%), and increased aspartate aminotransferase (7% vs 0%).
Recently, Weidinger et al published data from the first part of their phase 2b study (STREAM-AD, NCT05131477),11 a 52-week, randomized, double-blind, placebo-controlled trial. In this study, 390 adults with moderate-to-severe AD were randomized in a 1:1:1:1:1 ratio to receive subcutaneous Amlitelimab Q4W (250 mg with 500 mg loading dose, n=77; 250 mg without loading dose, n=78; 125 mg without loading dose, n=77; or 62.5 mg without loading dose, n=79) or placebo Q4W (n=79). During the initial 24-week treatment period, Amlitelimab demonstrated statistically significant improvements in percentage change in EASI from baseline to week 16 compared to placebo for all four doses studied (difference from placebo in least squares mean change from baseline: 250 mg with loading dose, −32.1%; 250 mg, −27.3%; 125 mg, −22.2%; 62.5 mg, −30.2%), with improvements sustained through week 24. Amlitelimab was well tolerated across all dose groups, although specific details on TEAEs were not reported.
The second part of this study is ongoing and will further evaluate the effects of Amlitelimab up to week 52.11 Additionally, phase 2 long-term extension studies (NCT05492578, NCT05769777)12,13 and a phase 3 study (NCT06130566)14 are currently in development to better define the role of this drug in moderate-to-severe AD.
Rocatinlimab (KHK4083/AMG451)
Rocatinlimab is a non-fucosylated IgG1 anti-OX40 mAb that inhibits and reduces the number of OX40+ T cells15,16 (Figure 1). Its efficacy in AD has been evaluated in both phase 1 and phase 2b trials (Table 1).
In a single-arm phase 1 trial conducted by Nakagawa et al15 22 patients with moderate-to-severe AD received infusions of Rocatinlimab at a dose of 10 mg/kg on days 1, 15, and 29. This treatment resulted in a 74% reduction in the EASI score from baseline to week 22, with 35% of patients achieving an IGA score of clear (0) or almost clear (1), indicating at least a two-grade improvement.
A subsequent multi-center, double-blind, placebo-controlled phase 2b trial by Guttman-Yassky et al16 included 274 patients with moderate-to-severe AD, who were randomized to receive various subcutaneous doses of Rocatinlimab (150 mg Q4W, 300 mg every 2 weeks [Q2W], 600 mg Q2W, or 600 mg Q4W) or a placebo. Consistent with Nakagawa et al’s findings,18 the least squares mean percent reduction in EASI score from baseline to week 16 was significantly greater across all Rocatinlimab dose groups compared to placebo (48–61% vs 15%, respectively). The 300 mg Q2W group demonstrated the most substantial improvements at week 16, with 31% of patients achieving an IGA score of 0/1 and 54% achieving a 75% improvement in EASI score (EASI75), compared to only 2% and 11% in the placebo group, respectively. By week 36, the 300 mg Q2W group showed an 88% least squares mean percent reduction in EASI score from baseline, with IGA 0/1 and EASI75 responses increasing to 52% and 64%, respectively. Notably, after treatment discontinuation at week 36, only 4–27% of patients who achieved EASI75 at that time experienced any relapse by week 56.
Moreover, biomarker analysis indicated that Rocatinlimab led to sustained reductions in mean serum concentrations of both TARC and IL-22 up to week 56, suggesting its potential to modulate Th2 and Th17/Th22 immune signatures.16
Throughout the trial, Rocatinlimab was well tolerated, with the most common adverse events being pyrexia (17% vs 4% in the placebo group), nasopharyngitis (14% vs 16%), chills (11% vs 0%), headache (9% vs 2%), aphthous ulcers (7% vs 0%), and nausea (6% vs 2%).16
The role of Rocatinlimab in moderate-to-severe AD is currently under further investigation in the comprehensive phase 3 ROCKET program (NCT05899816; NCT05651711; NCT05704738; NCT05398445; NCT05633355; NCT05724199; NCT06224192; NCT05882877),17–24 which aims to enhance our understanding of the effects of this drug.
Telazorlimab (GBR830/ISB830)
Telazorlimab is a humanized IgG1 neutralizing mAb targeting OX40 (Figure 1), investigated in both phase 2a and phase 2b clinical trials (Table 1).25,26
In the phase 2a trial led by Guttman-Yassky et al25 62 patients with moderate-to-severe AD were randomized 3:1 to receive either 10 mg/kg intravenous Telazorlimab or placebo on days 1 (baseline) and 29. Skin biopsies were obtained on days 1, 29, and 71. The primary endpoints included TEAEs and changes in biomarkers (epidermal hyperplasia/cytokines) at days 29 and 71. Secondary endpoints included the proportion of patients achieving at least a 50% improvement in the EASI score (EASI50). Results showed that TEAEs were comparable between groups (Telazorlimab: 63%, placebo: 63%). Headache was the most common adverse event in both groups, while post-procedural infection and myalgia occurred more frequently in the Telazorlimab group (9% vs 0% and 7% vs 0%, respectively). Additionally, a higher proportion of patients receiving Telazorlimab achieved EASI50 compared to placebo (76.9% vs 37.5%). Telazorlimab also inhibited Th1, Th2, and Th17/Th22 mRNA expression in lesional skin, reduced measures of skin hyperplasia, and decreased the presence of OX40+ T cells and OX40L+ dendritic cells, with effects sustained until day 71, 42 days after the last dose.25
In contrast, the phase 2b trial conducted by Rewerska et al26 involved a two-part study with 462 adults with moderate-to-severe AD randomized to different subcutaneous dosing regimens of Telazorlimab or placebo over 16 weeks of blinded treatment, followed by 38 weeks of open-label treatment and a 12-week drug-free follow-up. In part 1 (n=313), patients were assigned to receive 300 mg Q2W, 300 mg Q4W, or 75 mg Q4W, with a loading dose of 600 mg for the first two groups and 150 mg for the latter. In part 2 (n=149), patients received a loading dose of 1200 mg followed by 600 mg Q2W. The primary endpoint was the percentage change from baseline in the EASI score at week 16, while safety assessments focused on the incidence of TEAEs. At week 16, the least squares mean percentage change from baseline in EASI was significantly greater for patients receiving Telazorlimab 300 mg Q2W (part 1) and 600 mg Q2W (part 2) compared to placebo (−54.4% vs −34.2% for part 1; −59.0% vs −41.8% for part 2, P= 0.008 for both). TEAEs were similarly distributed between groups (Telazorlimab: 66%, placebo: 61.7%), with nasopharyngitis, upper respiratory tract infections, and headache being the most common adverse events.26
To our best knowledge, no ongoing trials are investigating the use of Telazorlimab in AD.
Discussion
Despite the recent introduction of novel targeted therapies for moderate-to-severe AD—including Dupilumab (an IL-4/IL-13 receptor alpha subunit inhibitor), Tralokinumab (an IL-13 inhibitor), and Janus kinase inhibitors—many patients still fail to achieve or maintain treatment goals or experience TEAEs, which continue to burden their disease management.3
This highlights the persistent need for new therapeutic options that are not only effective but also safe, durable, and capable of providing sustained relief for moderate-to-severe AD patients.3,7,8
Studies have demonstrated that AD patients exhibit increased OX40 expression in circulating CD4+ T cells, particularly in activated, skin-homing CD4+ T cells.27 Additionally, both OX40+ T cells and OX40L+ dendritic cells are elevated in the lesional skin of AD patients compared to non-lesional and psoriatic skin.28,29
Given these findings, and the positive outcomes observed in the aforementioned clinical studies,9–11,15,16,25,26 targeting the OX40/OX40L costimulatory pathway presents a promising therapeutic approach. This pathway not only modulates pathogenic effector T cells but also influences the generation and survival of memory T cells, offering the potential for sustained disease control.3,9–11,15,16,25,26,30
The unique, transient expression of OX40 on activated T cells makes it an appealing treatment target. By selectively blocking antigen-specific T cells implicated in AD pathophysiology, therapies could mitigate the risk of generalized immunosuppression.3,31–33 Moreover, the involvement of OX40/OX40L in not only Th2 but also Th1, Th17, and Th22 inflammatory pathways suggests it could provide broader, longer-lasting control of the disease.3,31–33
Nonetheless, while these findings indicate the potential for OX40/OX40L inhibitors to modify the course of AD, further investigation is needed. Phase 3 trials with larger patient populations and extended follow-up periods are essential to fully assess their long-term efficacy, safety, tolerability, and to determine optimal dosing regimens and routes of administration.
Moreover, a potential therapeutic role in other diseases such as psoriasis, alopecia areata, pemphigus, asthma, ulcerative colitis, Crohn’s disease and graft-versus-host disease has been suggested and should be further researched.34–36
Finally, regarding long-term safety concerns, the authors believe that potential immuno-oncology implications should be ruled out in future studies, as OX40 agonists are currently being tested in early phase cancer clinical trials.37
Conclusion
Blocking the OX40/OX40L costimulatory signaling pathway represents a promising and innovative therapeutic approach for patients with moderate-to-severe AD. This strategy offers the potential to target multiple stages of the inflammatory process that drive the disease, delivering more precise and sustained treatment effects.
While early basic and clinical research has shown encouraging results regarding the efficacy and safety of therapies targeting this pathway, larger phase 3 and beyond studies are still necessary. These trials will be crucial in defining the long-term role of OX40/OX40L inhibitors in the management of AD, helping to optimize treatment outcomes for these patients.
Consent
All authors consent to publication.
Funding
There is no funding to report.
Disclosure
FV has served as advisor and/or paid speaker for and/or participated in clinical trials sponsored by AbbVie, Amgen, Beiersdorf, Biogen, Bristol-Myers Squibb, Boehringer Ingelheim, Incyte, Janssen-Cilag, LEO, Lilly, Loreal, Merck, Novartis, Pfizer, Priovant, Sanofi and UCB. VM has no conflicts of interest to report for this work.
References
1. Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab. 2015;66(Suppl 1):8–16. doi:10.1159/000370220
2. Bieber T. Atopic dermatitis: an expanding therapeutic pipeline for a complex disease. Nat Rev Drug Discov. 2022;21(1):21–40. doi:10.1038/s41573-021-00266-6
3. Croft M, Esfandiari E, Chong C, et al. OX40 in the pathogenesis of atopic dermatitis—a new therapeutic target. Am J Clin Dermatol. 2024;25(3):447–461. doi:10.1007/s40257-023-00838-9
4. Croft M. Co-stimulatory members of the TNFR family: keys to effective T-cell immunity? Nat Rev Immunol. 2003;3(8):609–620. doi:10.1038/nri1148
5. Croft M, So T, Duan W, Soroosh P. The significance of OX40 and OX40L to T-cell biology and immune disease. Immunol Rev. 2009;229(1):173–191. doi:10.1111/j.1600-065X.2009.00766.x
6. Halim TYF, Rana BMJ, Walker JA, et al. Tissue-restricted adaptive type 2 immunity is orchestrated by Expression of the costimulatory molecule OX40L on group 2 innate lymphoid cells. Immunity. 2018;48(6):1195–1207.e6. doi:10.1016/j.immuni.2018.05.003
7. Gramaglia I, Jember A, Pippig SD, Weinberg AD, Killeen N, Croft M. The OX40 costimulatory receptor determines the development of CD4 memory by regulating primary clonal expansion. J Immunol. 2000;165(6):3043–3050. doi:10.4049/jimmunol.165.6.3043
8. Furue M, Furue M. OX40L-OX40 signaling in atopic dermatitis. J Clin Med Res. 2021;10(12). doi:10.3390/jcm10122578
9. Saghari M, Gal P, Gilbert S, et al. OX40L inhibition suppresses KLH-driven immune responses in healthy volunteers: a randomized controlled trial demonstrating proof-of-pharmacology for KY1005. Clin Pharmacol Ther. 2022;111(5):1121–1132. doi:10.1002/cpt.2539
10. Weidinger S, Bieber T, Cork MJ, et al. Safety and efficacy of amlitelimab, a fully human nondepleting, noncytotoxic anti-OX40 ligand monoclonal antibody, in atopic dermatitis: results of a phase IIa randomized placebo-controlled trial. Br J Dermatol. 2023;189(5):531–539. doi:10.1093/bjd/ljad240
11. Weidinger S, Blauvelt A, Papp K, et al. 523 - Efficacy and safety of amlitelimab (an anti-OX40 ligand antibody) in patients with moderate-to-severe atopic dermatitis: 24-week results from a phase 2b trial (STREAM-AD). Br J Dermatol. 2024;190(Supplement_2):ii24–ii26. doi:10.1093/bjd/ljad498.028
12. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05492578.
13. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05769777?id=NCT05769777&limit=10&rank=1.
14. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT06130566?id=NCT06130566&limit=10&rank=1.
15. Nakagawa H, Iizuka H, Nemoto O, et al. Safety, tolerability and efficacy of repeated intravenous infusions of KHK4083, a fully human anti-OX40 monoclonal antibody, in Japanese patients with moderate to severe atopic dermatitis. J Dermatol Sci. 2020;99(2):82–89. doi:10.1016/j.jdermsci.2020.06.005
16. Guttman-Yassky E, Simpson EL, Reich K, et al. An anti-OX40 antibody to treat moderate-to-severe atopic dermatitis: a multicentre, double-blind, placebo-controlled phase 2b study. Lancet. 2023;401(10372):204–214. doi:10.1016/S0140-6736(22)02037-2
17. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05899816?id=NCT05899816&limit=10&rank=1.
18. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05651711?id=NCT05651711&limit=10&rank=1.
19. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05704738?id=NCT05704738&limit=10&rank=1.
20. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05398445?id=NCT05398445&limit=10&rank=1.
21. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05633355?id=NCT05633355&limit=10&rank=1.
22. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT06224192?id=NCT06224192&limit=10&rank=1.
23. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05882877?id=NCT05882877&limit=10&rank=1.
24. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/study/NCT05724199?id=NCT05724199&limit=10&rank=1.
25. Guttman-Yassky E, Pavel AB, Zhou L, et al. GBR 830, an anti-OX40, improves skin gene signatures and clinical scores in patients with atopic dermatitis. J Allergy Clin Immunol. 2019;144(2):482–493.e7. doi:10.1016/j.jaci.2018.11.053
26. Rewerska B, Sher LD, Alpizar S, et al. Phase 2b randomized trial of OX40 inhibitor telazorlimab for moderate-to-severe atopic dermatitis. J Allergy Clin Immunol Glob. 2024;3(1):100195. doi:10.1016/j.jacig.2023.100195
27. Elsner JS, Carlsson M, Stougaard JK, et al. The OX40 axis is associated with both systemic and local involvement in atopic dermatitis. Acta Derm Venereol. 2020;100(6):adv00099. doi:10.2340/00015555-3452
28. Ilves T, Harvima IT. OX40 ligand and OX40 are increased in atopic dermatitis lesions but do not correlate with clinical severity. J Eur Acad Dermatol Venereol. 2013;27(2):e197–e205. doi:10.1111/j.1468-3083.2012.04587.x
29. Fujita H, Shemer A, Suárez-Fariñas M, et al. Lesional dendritic cells in patients with chronic atopic dermatitis and psoriasis exhibit parallel ability to activate T-cell subsets. J Allergy Clin Immunol. 2011;128(3):574–582.e1–e12. doi:10.1016/j.jaci.2011.05.016
30. Sher L, Rewerska B, Acocella A, et al. 472 Telazorlimab in atopic dermatitis: phase 2b study shows improvement at 16 weeks. J Invest Dermatol. 2021;141(5):S82. doi:10.1016/j.jid.2021.02.496
31. Sadrolashrafi K, Guo L, Kikuchi R, et al. An OX-tra’ordinary tale: the role of OX40 and OX40L in atopic dermatitis. Cells. 2024;13(7):587. doi:10.3390/cells13070587
32. Guttman-Yassky E, Croft M, Geng B, et al. The role of OX40 ligand/OX40 axis signalling in atopic dermatitis. Br J Dermatol. 2024;191(4):488–496. doi:10.1093/bjd/ljae230
33. Lé AM, Torres T. OX40-OX40L inhibition for the treatment of atopic dermatitis-focus on rocatinlimab and amlitelimab. Pharmaceutics. 2022;14(12):2753. doi:10.3390/pharmaceutics14122753
34. Riki H, Takahashi H, Amagai M. Diverse role of OX40 on T cells as a therapeutic target for skin diseases. J Invest Dermatol. 2023;143(4):545–553. doi:10.1016/j.jid.2022.11.009
35. Papp KA, Gooderham MJ, Girard G, Raman M, Strout V. Phase I randomized study of KHK 4083, an anti‐OX 40 monoclonal antibody, in patients with mild to moderate plaque psoriasis. J Eur Acad Dermatol Venereol. 2017;31(8):1324–1332. doi:10.1111/jdv.14313
36. Willoughby J, Griffiths J, Tews I, Cragg MS. OX40: structure and function–what questions remain? Mol Immunol. 2017;83:13–22. doi:10.1016/j.molimm.2017.01.006
37. Thapa B, Kato S, Nishizaki D, et al. OX40/OX40 ligand and its role in precision immune oncology. Cancer Metastasis Rev. 2024;25:1–3.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.