")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
Overview of the Active Ingredients in Cosmetic Products for the Care of Skin That Has Been Exposed to Ionizing Radiation – Analysis of Their Effectiveness in Breast Cancer Radiotherapy
Authors Kondziołka J , Wilczyński S
Received 6 June 2021
Accepted for publication 16 July 2021
Published 26 August 2021 Volume 2021:14 Pages 1065—1076
DOI https://doi.org/10.2147/CCID.S322228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Joanna Kondziołka, Sławomir Wilczyński
Department of Basic Biomedical Science, Faculty of Pharmaceutical Sciences in Sosnowiec, Medical University of Silesia, Katowice, Poland
Correspondence: Sławomir Wilczyński Email [email protected]
Abstract: Treatment that uses ionizing radiation is one of the most common therapeutic methods in case of breast cancer. However, it often results in radiation dermatitis, which manifests itself, among others, as erythema, burning, itching and pain as well as dry or moist desquamation of the epidermis in the irradiated areas. The intensity of these symptoms significantly reduces the patient’s quality of life, which could affect the effectiveness of the entire therapy. There are more and more cosmetic preparations on the market for daily care of skin that has been exposed to radiation. The composition of the active ingredients in these preparations is designed to support the protective functions of the skin, delay the occurrence of the side effects of ionizing radiation, reduce their intensity, and accelerate the regeneration of the irradiated areas. Unfortunately, there is little scientific evidence of the effectiveness of the active ingredients that are contained in these preparations. This paper presents a narrative review of the most commonly used ingredients and compares them with the current state of knowledge on their effectiveness in preventing radiodermatitis.
Keywords: active substances, breast cancer, prevention, radiation dermatitis, radiotherapy
Introduction
In 2020 breast cancer was the most commonly diagnosed cancer in the entire population of patients (ca.11.7%). When only the female population is considered, breast cancer constitutes ca. 24.5%, which translates into almost 2.3 million new cases per year.1,2 Radiotherapy has been very important in the treatment of this disease for many years. It uses ionizing radiation to destroy cancer cells. Despite its undeniable advantages such as its high degree of effectiveness, high safety profile and local action, it is accompanied by various side effects. Over 95% of patients that are exposed to ionizing radiation report adverse effects such as erythema, edema and dryness of the skin, itching, dry or moist desquamation, soreness, and, in extreme cases, skin necrosis.3–5 These symptoms are known as radiation dermatitis.5 This skin inflammation is divided into acute radiation dermatitis, which appears within the first four weeks of treatment and chronic radiation dermatitis, which can be observed even years after radiation.6
The pathogenesis of radiodermatitis is a complex process and involves a combination of direct radiation injuries and inflammatory reaction of epidermis, dermis, and vasculature. First, tissue damage, which is the beginning of acute radiodermatitis, appears during initial dose of ionizing radiation when secondary electrons and reactive oxygen species (ROS), responsible for cellular structure damage, are formed.7 Each following fraction of radiation increases inflammatory reaction which causes changes in skin pigmentation, hair loss and damage of dermis, and leads to a disruption of the normal process of self-renewal of the skin. As a response to higher doses of radiation, skin starts to produce novel cells by increasing the rate of mitosis in the basal keratinocyte cell layer. Because this process is faster than shedding of the old cells, it leads to thickened and dry desquamation. During subsequent doses the basal cells are unable to recover and exudate appears which leads to moist desquamation, broken epidermis, and pain. Depending on immune function and degrees of tissue injury, there is an increased risk of infection in the irradiated area.8
The mechanism of this inflammatory reaction is not yet completely understood, but keratinocytes, fibroblasts, and endothelial cells stimulate resident as well as circulating immune cells, which produce ranks of cytokines and chemokines (eg, interleukin (IL)-1α, IL-1β, tumor necrosis factor (TNF)-α, TGF- β, IL-6, IL-8, C-C motif chemokine ligand (CCL)-4, C-X-C motif chemokine ligand (CXCL)-10 and CCL-2). The presence of these molecules results in upregulation of the expression of adhesion molecules and plays a very important role in the transendothelial migration of immune cells from circulation to the irradiated skin.7,8
Chronic radiodermatitis mechanism is based also on extended inflammatory reaction which starts during initial dose of ionizing radiation and is prolonged even for months or years after the last radiotherapy session. In case of acute effect, the inflammatory cytokines responsible for this reaction are IL-6, (TNF)-α, (IL)-1 α, TGF- β which enhance tissue fibrosis and induce synthesis of extracellular matrix proteins and metalloproteinases and form telangiectasia. Accumulation and activation of leucocytes at the irradiated area leads to skin atrophy and necrosis.7
All radiation dermatitis can significantly reduce a patient’s quality of life, and its intensification with each subsequent exposure could be the reason for dose reduction or even unplanned interruptions of the therapy, which could affect the effectiveness of the treatment.4,9,10 The intensity of the reaction depends on many factors such as the total dose and how it is fractioned, concurrent chemotherapy, the condition of the skin, and any other comorbidities.11 The severity of reactions is evaluated using one of two grading systems shown in Table 1. Depending on the institute, medical staff either use classification according to the Radiation Therapy Oncology Group (RTOG) or the Common Terminology Criteria for Adverse Events (CTCAE). Because of the frequency of the occurrence of an acute reaction and the consequences that result from its presence, an effective skin care procedure during radiation therapy needs to be determined and the effectiveness of the active ingredients in preventing and treating radiodermatitis should be confirmed. According to Multinational Association of Supportive Care in Cancer (MASCC) there is only a few recommended active ingredients for skin care during radiotherapy. First of all, gentle washing with or without mild soap is recommend as skin care procedure. Positive effect in reducing the maximum toxicity grade is also observed in case of topical prophylactic steroids which are also recommended by MASCC as prophylaxis. Additionally, silver sulfadiazine cream could be used as a treatment to reduce intensity of radiodermatitis.13
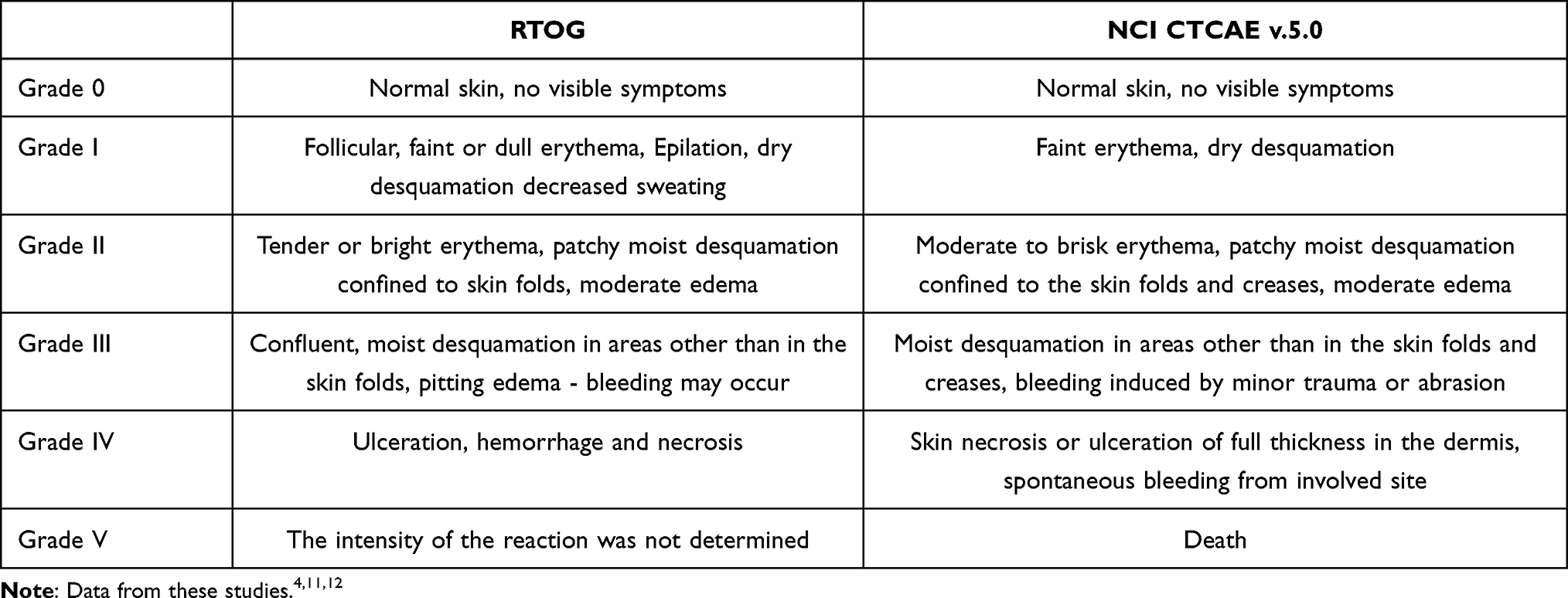 |
Table 1 Comparison of the Scoring of Acute Toxicity in RTOG and CTCAE |
Currently, many preparations are available on the market, whose manufacturers declare that they are effective in soothing or preventing inflammation and protecting skin that has been exposed to ionizing radiation. Some of these are medicinal products such as over-the-counter drugs (OTC), but the main and most common group is cosmetic preparations or so-called dermocosmetics, which include skin care creams and balms, as well as mouthwashes, gels and ointments. Owing to their carefully selected compositions, these products are designed to improve skin hydration and lubrication by rebuilding the hydrolipidic film, regenerating the epidermis, to neutralize the effects of free radicals and to support the protective functions of the skin. Their action is based on a wide variety of active ingredients such as hyaluronic acid, allantoin, panthenol (provitamin B5), ectoine, natural oils (linseed, argan, macadamia), and plant extracts (chamomile, oats, pot marigold). In addition to the main active ingredients, these cosmetics differ significantly in their base, and, as a result, there are water-in-oil or oil-in-water emulsions, petrolatum-based ointments or cream gels.
Materials and Methods
In order to analyze the effectiveness of the active ingredients in reducing the intensity of radiation dermatitis, the research was conducted in the electronic database PubMed, which was searched for articles that were published between 1991 and 2020. The search was conducted up to July 5, 2021. The language of the articles was limited to English and the databases that were used supplied the appropriate filters. The following keywords were searched in various conjunctions to optimize the search results in accordance with the topic of this article: radiation dermatitis, breast cancer, hyaluronic acid, panthenol, Aloe Vera, Calendula officinalis, prevention. All articles that were cited in this narrative review were also screened in order to identify other potential studies in their reference lists. Once again only English articles were reviewed.
Results
During the online search, the articles were screened by their titles and abstracts. A total of 31 articles were considered to be relevant and were selected for full-text reading. A scan of literature and citations of the included studies yielded 17 more articles for full-text reading. Among the 48 papers that were considered for the present review, ten did not have any relevant data for the planned narrative review and were excluded. For the remaining 38 articles, among which were reviews, case studies, randomized controlled trials, contents were evaluated and selected for data analysis. A summary of this analysis, including name of the active ingredient, type of test and reference products, name of the investigator conducting the study, size of the test group and the result of the study, is shown in Table 2.
 |  | 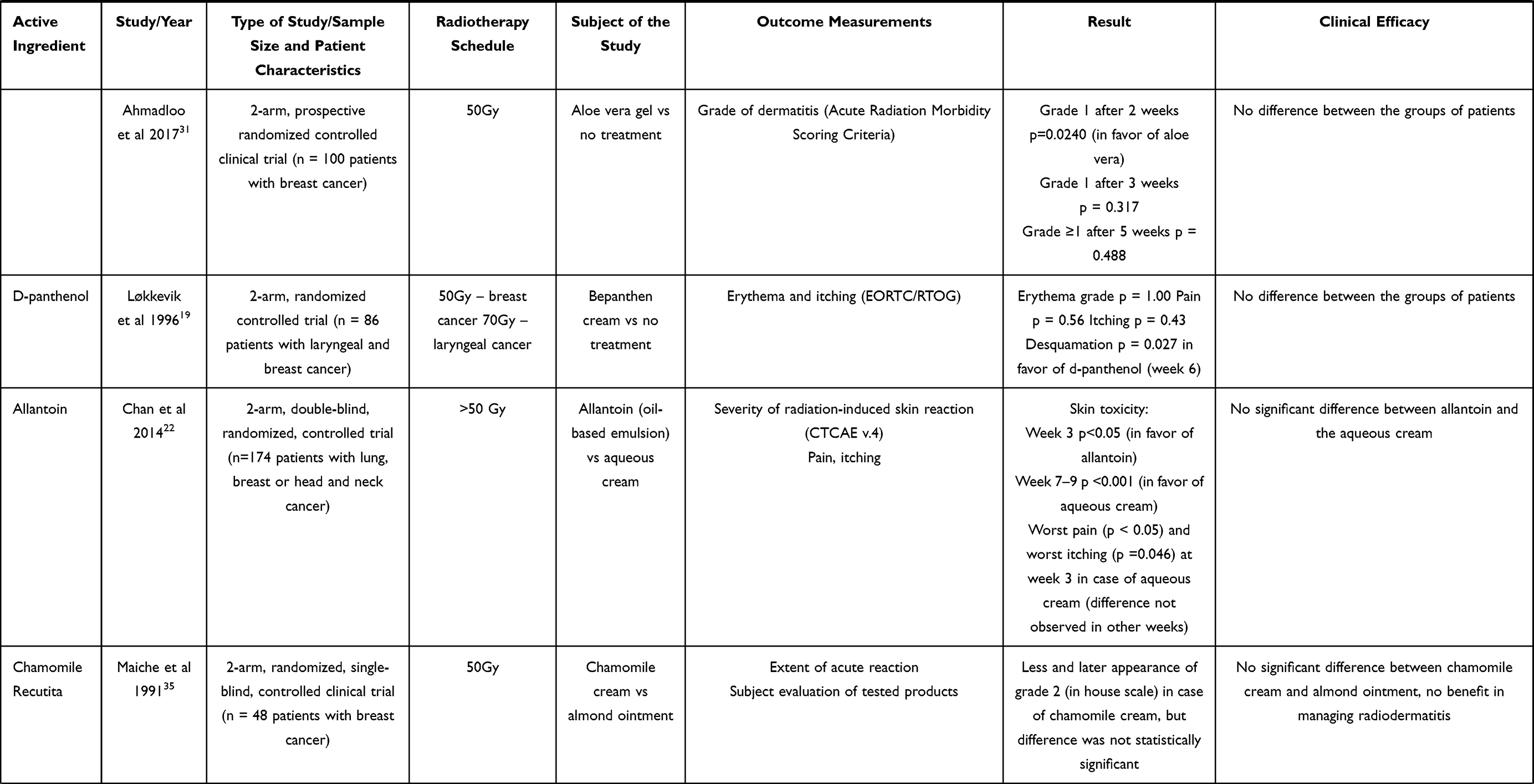 | 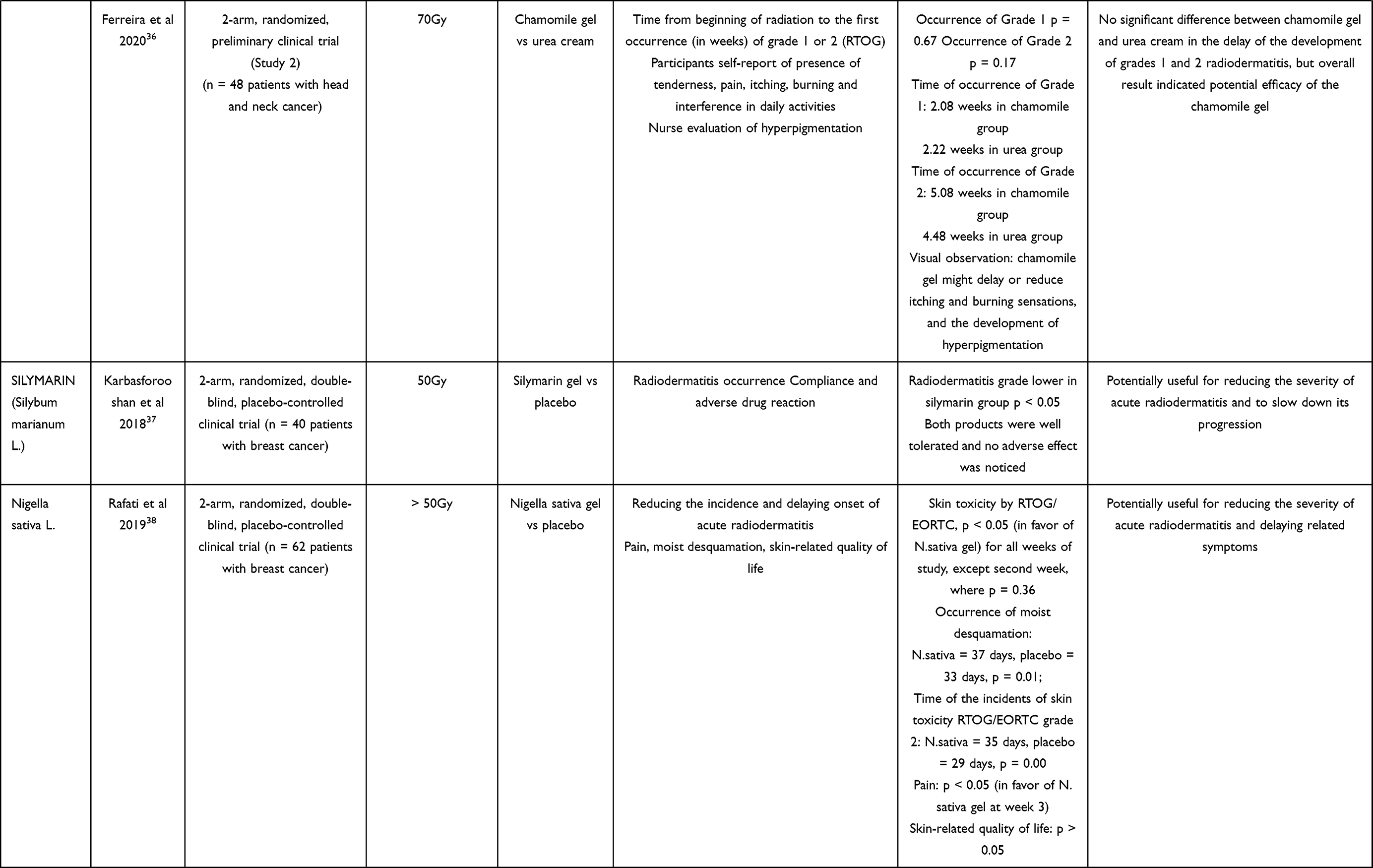 |
Table 2 Summary of the Research on the Active Ingredients |
Discussion
Hyaluronic Acid
One of the most common ingredients that is used in irradiated skin care products is hyaluronic acid, which is a natural biopolymer from the family of glycosaminoglycans that are found in many tissues, which accelerates wound healing by affecting the development of fibroblasts and fibrin.14 Because of these properties, it has been subjected to several clinical trials that were designed to prove its importance in the skin care preparations that are used during radiation therapy. An analysis of literature data did not unequivocally confirm the effectiveness of hyaluronic acid in preventing radiation dermatitis. A study published in 1997 by Liguori et al showed that a preparation containing 0.2% sodium hyaluronate significantly delayed the occurrence of the first signs of radiodermatitis and also reduced its intensity compared to the placebo (p <0.01). The most significant differences in severity of skin reaction scores (scale created for the purpose of the study) between hyaluronic acid and placebo were noticed from week 3 (score > 1: hyaluronic a. = 4.4% vs placebo = 31.3%) until week 7 (score > 1: hyaluronic a. = 20.4% vs placebo = 44.5%). A shorter healing time of irritated skin after the therapy was also observed in a group of patients who were using a preparation containing hyaluronic acid.15 However, research that was conducted by Kirova et al from 2005–2008 showed that there was no significant difference in alleviating the symptoms of negative effects of ionizing radiation between the 0.2% sodium hyaluronate preparation tested by Liguori’s team and a simple emollient containing 2% urea and 9.5% glycerol. However, in the group of patients that were using the preparation with hyaluronic acid, there was a decrease in the level pain sensation (hyaluronic a. +7.0 vs emollient +13,7; p = 0.053) and less erythema in the irradiated area (the relative reduction of colorimetric value: hyaluronic a. = 20.4%, emollient = 13.0%; p = 0.46) compared to the control group, although it should be noted that other studies have not confirmed the effectiveness of hyaluronic acid in the care of skin that has been exposed to ionizing radiation.16 A study by Pinnix et al showed that significantly better results, and thus less severe radiodermatitis, were observed in patients who were using the petrolatum-based gel compared to the hyaluronic acid-based gel (≥ Grade 2 according CTCAE v.3: hyaluronic a. = 61.5%, petrolatum gel = 47.7%; p = 0.027).17
D-Panthenol
The second most frequent active ingredient in the commercially available skin care preparations that are used during radiotherapy is D-panthenol or provitamin B5. It is a polyhydroxy alcohol that is present in the skin, hair and nails, and plays an important role in the metabolic processes of proteins, carbohydrates, and fats. It participates in tissue regeneration and accelerates wound healing. When applied to the skin, it soothes irritation and redness and also improves the lipid barrier of the epidermis, which is why it is often used in cosmetics for irritated skin and after-sun lotions.18 A study by Løkkevik et al that was conducted in a group of 86 patients showed that the application of a cream containing 5% d-panthenol to skin that had been subjected to radiotherapy significantly reduced epidermal peeling (p = 0.027), but if only grades 3 and 4 are considered – no significant difference was found (p = 0.83). However, an overall assessment did not reveal any significant differences in skin condition compared to the areas to which no care product had been applied.19 Another study was conducted by Censabella et al to compare the effectiveness of a hydroactive colloidal gel containing arginine versus two historical groups using cream with 5% d-panthenol in preventing moist desquamation after radiotherapy. The first historical group applied cream for the duration of radiotherapy, the second group applied cream with d-panthenol during the first 11–14 days of radiotherapy, than replaced it with hydroactive colloidal gel. The test results proved that the product with d-panthenol exhibited weaker effects in the tested range (incidents of moist desquamation: hydroactive colloidal gel = 6.9%, first historical group (d-panthenol) = 35.1%, second historical group (d-panthenol and hydroactive colloidal gel) = 12.6%; p < 0.0001). In addition, the gel had an advantage in terms of its functional aspects such as quick absorption without leaving an adhesive layer, a cooling effect and less skin irritation during application.10 In the absence of sufficient evidence for the effectiveness of provitamin B5, this component is not recommended by the Multinational Association of Supportive Care of Cancer (MASCC).13 Nevertheless, it is still one of the most common ingredients in the discussed products that are available on the market.
Allantoin
Allantoin is another common ingredient that is used in preparations recommended for the care of skin that has been exposed to ionizing radiation. It is a heterocyclic urea derivative that has soothing, protecting, skin conditioning and moisturizing effects in cosmetic products and also affects skin regeneration by stimulating cell reconstruction and acting as anti-inflammatory.20,21 In this case, there is also insufficient evidence that this component has a positive effect on minimizing radiation dermatitis. The aim of the research that was conducted by Chan et al at the turn of 2012 and 2013, was to compare the effectiveness of an emulsion containing natural oils and allantoin with a reference cream in preventing and treating radiation-induced skin inflammation. Patients who received aqueous cream had significantly higher average level of worse pain (p < 0.05) and itching (p = 0.046) up to the third week. However, the obtained results showed that there were no significant differences between the tested preparations in reducing pain or itching at other weeks. Similar relation was noticed in case of skin toxicity analysis. Patients from allantoin-cream group had significantly lower average level of skin toxicity (CTCAE) at week three (p < 0.05) but at week seven, eight, and nine, level of skin toxicity was statistically higher in this group (p < 0.001). Despite the initial similar or even better results, it finally turned out that the allantoin-containing cream was much less effective in relieving inflammation symptoms after six weeks of radiation and after the radiotherapy had been completed.22
Extract of Pot Marigold (Calendula officinalis L.)
Among the natural active ingredients that are used in preparations for skin care after radiotherapy, there is also pot marigold (Calendula officinalis L.). The raw material that is obtained from its flowers is rich in essential oils, flavonoids, triterpene alcohols, phenolic acids, saponins, carotenoids, and sterols. This extract has moisturizing and anti-inflammatory effects, which is why it is recommended for cosmetics for dry, irritated, and sensitive skin. However, its widest application is to accelerate wound healing and epidermal reconstruction. Research that was conducted by Patrick et al in 1996 proved that the flavonoids that are contained in the extract stimulate the process of hyaluronan deposition and accelerate the formation of blood vessels, which would confirm the theory of its effect on wound healing.23 Research conducted by Pommier et al in a group of 254 patients confirmed that an ointment containing the marigold extract reduced the number of cases of grade 2 and 3 dermatitis (occurrence of acute dermatitis: calendula = 41%, trolamine = 63%, p = 0.001) and significantly reduced the pain sensation in this group of patients compared to the group that was using a trolamine cream (pain evaluated on visual analog scale (VAS): calendula = 1.54, trolamine = 2.10, p = 0.03). The largest differences were observed in problem areas such as skin folds, armpits, and thin skin.24,25 Another study that compared the effectiveness of a cream with marigold with a reference cream was conducted by Sharp et al in 2013. The results that were obtained confirmed that there were no significant differences between the tested products (≥ grade 2 according RTOG/EORTC scale during follow-up visit: calendula: 23%, reference cream: 19%) and, what is more, the marigold cream was rated worse in terms of its application (p < 0.001) and absorption (p < 0.001).25,26 Promising results were obtained by Schneider et al during evaluation in a group of 51 patients with head and neck cancer – efficacy of Calendula Officinalis cream with 4% Calendula oil versus Essential Fatty Acid cream (EFA) with sunflower oil. The obtained results showed a statistically significant difference between the occurrence of grade 2 and 3 (RTOG) reactions in the studied groups (week 7, ≥ grade 2: calendula = 22.22%, EFA = 42.86%).27 However, in reference to the research that has been conducted to date, this component has not been recommended by the Multinational Association of Supportive Care of Cancer (MASCC).13
Aloe Vera L. Gel
The results of the effectiveness of a very common ingredient, namely aloe vera gel, in the care of radiation-damaged skin may seem surprising. Aloe vera gel, which mainly contains polysaccharides, is one of the more popular soothing ingredients used in cosmetics. Because of its antibacterial, antiviral, anti-ulcer, and antioxidant effects, it is also used in many specialized preparations that are designed to treat skin problems and wounds, including burns.28,29 The healing effect of aloe vera gel was confirmed by Somboonwong et al in a study in rats that was conducted in 2000. After the results were analyzed, it was found that the wound-healing process was significantly faster in the group of animals treated with the aloe vera gel than in the control group.28,30 Nevertheless, a number of studies have not proven the effectiveness of this raw material in preventing and treating radiation dermatitis.31–34 Research conducted by Heggie et al in a group of 225 patients confirmed that Aqueous cream was significantly better in reducing dry desquamation and pain than Aloe vera gel (dry desquamation ≥ 1%: Aloe vera = 70%, aqueous cream = 41%, p < 0.001; cumulative probability of ≥ grade 2 of pain: Aloe vera = 26%, aqueous cream = 17%, p = 0.03).32 Moreover, according to a study conducted by Hoopfer et al, compared to dusting powder, the cream containing aloe vera gel and the placebo, which was the base of the tested cream, it was found that there was an increase in radiodermatitis for both emulsions compared to the third group of patients who were using the dusting powder.33 However, it should be taken into account that in this case the base itself could have had a crucial impact on the final results of the effectiveness of these creams.
Extract of Chamomile (Chamomile recutita)
Chamomile is a medical plant common because of its anti-inflammatory properties and effectiveness against candida and gram-positive organism. It contains many substances among which bisaboloids, flavonoids, levomenthol, and chamazulene.35 Because of its anti-inflammatory properties, chamomile was considered as treatment during radiotherapy. A study conducted by Maiche et al on a group of 48 women with breast cancer confirmed that there was no statistically significant difference between chamomile cream and almond ointment, however most of the skin reactions appeared later in case of chamomile cream.35 During another clinical trial, conducted by Ferreira et al, chamomile gel containing 8.35% chamomile (Chamomile Recutita), was compared with urea cream. No statistical difference was observed in case of the delay in the development of grade 1 (p = 0.67) and grade 2 (p = 0.17) radiodermatitis. However the figures showed that gel with chamomile might be helpful in delaying or reducing itching, burning sensation or development of hyperpigmentation.36
Silymarin (Silybum marianum L.)
In 2016–2018, Karbasforooshan et al conducted a trial to prove effectiveness of an extract from milk thistle (Silybum marianum L.), which is well-known because of its liver protecting properties. During the research, a 1% silymarin gel that was applied once a day was evaluated. The obtained results indicated a statistically significant difference in the frequency and severity of radiodermatitis based on the RTOG and NCI-CTCAE scores. In the fifth week, 100% of patients in silymarin group developed grade 1, while in the placebo group also grades 2 and 3 were reported (grade 1 = 55%, grade 2 = 40%, grade 3 = 5%). Although the results showed that this active ingredient reduced the grade of acute radiodermatitis and delayed its occurrence, the group included only 50 patients and therefore a larger clinical study is required to confirm these initial results.37
Extract of Black Cumin (Nigella sativa L.)
Additionally, there was a clinical trial with another plant extract – Nigella Sativa L. in 2018. This medicinal plant, which is commonly known as black cumin, has been used as a remedy for many ailments such as headache, fever, inflammation, cough or metabolic disorders. The oil from black cumin has been used in the form of ointment for treating wounds and skin irritations or inflammation. For their research, Rafati et al used a gel with a Nigella sativa extract. The obtained results showed that this active ingredient was more effective than a placebo gel in preventing acute radiation dermatitis (skin toxicity by RTOG/EORTC, p < 0.05 for all weeks of study, except the second week, where p = 0.36). There was a significant difference between the N. sativa gel and the placebo for the severity of moist desquamation at weeks five and six (p = 0.01) as well as in the time in which the related symptoms appeared (time of occurrence of moist desquamation: N. sativa = 37 days, placebo = 33 days, p = 0.01; time of the incidents of skin toxicity RTOG/EORTC grade 2: N. sativa = 35 days, placebo = 29 days, p = 0.00). Moreover, for this research, the group of patients was also small and therefore a larger study is required to confirm the initial results and effectiveness of N. sativa in preventing radiodermatitis.38
Conclusion
There are many products on the market for the care of skin that has been exposed to ionizing radiation. These are primarily cosmetics that include common active ingredients. According to the literature review, only a few of them have undergone clinical trials (Table 2), thus there is no scientific evidence for their effectiveness in preventing radiation dermatitis. The MASCC guidelines only recommend topical steroids, silver sulfadiazine and care that is based on gentle washing using a mild soap for preventing radiodermatitis. For the hyaluronic acid, sucralfate and petrolatum-based ointments, there is insufficient evidence of their effectiveness, but there is no reason to completely remove them from further research.13
However, it should be noted that in most studies which aimed to confirm the effectiveness of a given active substance in delaying, minimizing and assisting in the treatment of the side effects of radiotherapy, a preparation with a completely different composition, not a placebo, was used for the comparisons. This may have affected the observed differences between the products and the final results, because various bases affect the skin and its hydration, lipid barrier or absorption of active ingredients differently.10,33 At the same time, it should be noted that the analysis of the effectiveness of the preparations that are used in the care of radiation-damaged skin is only provable using qualitative methods. This limits the unambiguous and independent assessment of the clinical usefulness of individual ingredients or preparations of a researcher. Therefore, it is first necessary to develop a methodology for the quantitative assessment of the skin during the course of radiation therapy using skin measurement. All of the previously-mentioned methods have been used in dermatological distribution and concentration of chromophores such as melanin and hemoglobin in the skin.40,41
Thermographic analysis allows to determine the temperature gradient of irradiated areas and intact skin. This parameter, together with information on the number of chromophores in a given area, can be used to determine the severity of skin inflammation. At the same time, taking into account the number of cases of breast cancer per year and the frequency of the side effects of radiotherapy, research should be continued to identify preparations that are effective for irradiated skin care. To improve the quality of life of treated patients, these products should delay the occurrence of side effects, minimize them, and accelerate recovery. The application itself and the form of the preparation also play a very important role, because even when a very effective preparation is administered in the form of a hard-to-spread cream or ointment, it can intensify the pain of areas that have been irritated by radiation and will not be used by patients.
Funding
This study has been financially supported by Medical University of Silesia, grants no. PCN-1-013/K/0/O and PCN-2-114/N/0/O.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization [homepage on the Internet] Fact sheets: breast cancer; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/breast-cancer.
2. World Health Organization [homepage on the Internet] Fact sheets: cancer; 2021. Available from: https://gco.iarc.fr/today/data/factsheets/cancers/20-Breast-fact-sheet.pdf.
3. Kišonas J, Venius J, Sevriukova O, et al. Application of reflectance confocal microscopy for early diagnosis of radiation-induced acute dermatitis in radiosensitive patient: case study. Radiat Prot Dosimetry. 2018;182(1):93–97.
4. White J, Joiner MC. Toxicity from radiation in breast cancer. In: Small W, Woloschak GE, editors. Radiation Toxicity: A Practical Guide. (Cancer Treatment and Research V.128). New York: Springer Science + Media Business; 2006:65–110.
5. Lee J, Park W, Choi DH, et al. Patient-reported symptoms of radiation dermatitis during breast cancer radiotherapy: a pilot study. Qual Life Res. 2017;26:1713–1719. doi:10.1007/s11136-017-1526-4
6. Spałek M. Chronic radiation – induced dermatitis: challenges and solution. Clin Cosmet Investig Dermatol. 2016;9:473–482. doi:10.2147/CCID.S94320
7. Singh M, Alavi A, Wong R, Akita S. Radiodermatitis: a review of our current understanding. Am J Clin Dermatol. 2016;17(3):277–292. doi:10.1007/s40257-016-0186-4
8. Robijns J, Laubach HJ. Acute and chronic radiodermatitis: clinical signs, pathophysiology, risk factors and management options. J Egypt Women Dermatol Soc. 2018;15:2–9. doi:10.1097/01.EWX.0000529960.52517.4c
9. McQuestion M. Evidence-based skin care management in radiation therapy: clinical update. Semin Oncol Nurs. 2011;27(2):e1–e17. doi:10.1016/j.soncn.2011.02.009
10. Censabella S, Claes S, Orlandini M, Braekers R, Bulens P. Efficacy of a hydroactive colloid gel versus historical controls for the prevention of radiotherapy-induced moist desquamation in breast cancer patients. Eur J Oncol Nurs. 2017;29:1–7. doi:10.1016/j.ejon.2017.04.003
11. Rosenthal A, Israilevich R, Moy R. Managment of acute radiation dermatitis: a review of the literature and proposalfor treatment algorithm. J Am Acad Dermatol. 2019;81:558–567. doi:10.1016/j.jaad.2019.02.047
12. Kitajma M, Noto K, Itaki C, et al. Quantitative assessment of radiodermatitis through a non-invasive objective procedure in patients with breast cancer. Mol Clin Oncol. 2019. doi:10.3892/mco.2019.1948
13. Wong RKS, Bensadoun RJ, Boers-Doets CB, et al. Clinical practice guidelines for the prevention and treatment of acute and late radiation reactions from the MASCC Skin Toxicity Study Group. Support Care Cancer. 2013;21:2933–2948. doi:10.1007/s00520-013-1896-2
14. Salwowska NM, Bebenek KA, Żądło DA, Wcisło-Dziadecka DL. Physiochemical properties and application of hyaluronic acid: a systematic review. J Cosmet Dermatol. 2016;15:520–526. doi:10.1111/jocd.12237
15. Liguori V, Guillemin C, Pesce GF, Mirimanoff RO, Bernier J. Double-blind, randomized clinical study comparing hyaluronic acid cream to placebo in patients treated with radiotherapy. Radiother Oncol. 1997;42(2):155–161. doi:10.1016/S0167-8140(96)01882-8
16. Kirova YM, Fromantin I, De Rycke Y, et al. Can we decrease the skin reaction in breast cancer patients using hyaluronic acid during radiation therapy? Results of phase III randomised trial. Radiother Oncol. 2011;100:205–209. doi:10.1016/j.radonc.2011.05.014
17. Pinnix C, Perkins GH, Strom EA, et al. Topical hyaluronic acid vs. standard of care for the prevention of radiation dermatitis after adjuvant radiotherapy for breast cancer: single-blind randomized phase III clinical trial. Int J Radiat Oncol Biol Phys. 2011;83(4):1089–1094.
18. Pavlačková J, Egner P, Sedláček T, Mokrejš P, Sedlaříková J, Polášková J. In vivo efficacy and properties of semisolid formulations containing panthenol. J Cosmet Dermatol. 2018;18(1):346–354.
19. Løkkevik E, Skovlund E, Reitan JB, Hannisdal E, Tanum G. Skin treatment with Bepanthen Cream versus no cream during radiotherapy: a randomized controlled trial. Acta Oncol. 1996;35(8):1021–1026. doi:10.3109/02841869609100721
20. Becker LC, Bergfeld QF, Belsito DV, et al. Final report of the safety assessment of allantoin and its related complexes. Int J Toxicol. 2010;29(3_suppl):84S–97S. doi:10.1177/1091581810362805
21. Araújo LU, Grabe-Guimarães A, Mosqueira VC, Carneiro CM, Silva-Barcellos NM. Profile of wound healing process induced by allantoin. Acta Cir Bras. 2010;25(5):460–466. doi:10.1590/S0102-86502010000500014
22. Chan RJ, Mann J, Tripcony L, et al. Natural oil-based emulsion containing allantoin versus aqueous cream for managing radiation-induced skin reactions in patients with cancer: a Phase 3, double-blind, randomized, controlled trial. Int J Radiat Oncol Biol Phys. 2014;90(4):756–764.
23. Patrick KF, Kumar S, Edwardson PA, Hutchinson JJ. Induction of vascularisation by an aqueous extract of the flowers of Calendula officinalis L. the European marigold. Phytomedicine. 1996;3(1):11–18. doi:10.1016/S0944-7113(96)80004-3
24. Pommier P, Gomez F, Sunyach MP, D’Hombres A, Carrie C, Montbarbon X. Phase III randomized trial of Calendula officinalis compared with Trolamine for the prevention of acute dermatitis during irradiation of breast cancer. J Clin Oncol. 2004;22(8):1447–1453. doi:10.1200/JCO.2004.07.063
25. Kodiyan J, Amber KT. A Review of the Use of Topical Calendula in the Prevention and Treatment of Radiotherapy-Induced Skin Reactions. Antioxidants (Basel). 2015;4(2):293–303. doi:10.3390/antiox4020293
26. Sharp L, Finnilä K, Johansson H, Abrahamsson M, Hatschek T, Bergenmar M. No differences between Calendula cream and aqueous cream in the prevention of acute radiation skin reactions—results from a randomised blinded trial. Eur J Oncol Nurs. 2012;17(4):429–435.
27. Schneider F, Danski MT, Vayego SA. Usage of Calendula officinalis in the prevention and treatment of radiodermatitis: a randomized double-blind controlled clinical trial. Rev Esc Enferm USP. 2015;49(2):221–228. doi:10.1590/S0080-623420150000200006
28. Hashemi SA, Madani SA, Abediankenari S. The Review on properties of Aloe Vera in healing of cutaneous wounds. Biomed Res Int. 2015;2015:1–6. doi:10.1155/2015/714216
29. Radha MH, Laxmipriya NP. Evaluation of biological properties and clinical effectiveness of Aloe vera: a systematic review. J Tradit Complement Med. 2014;5(1):21–26. doi:10.1016/j.jtcme.2014.10.006
30. Somboonwong J, Thanamittramanee S, Jariyapongskul A, Patumraj S. Therapeutic effects of Aloe vera on cutaneous microcirculation and wound healing in second degree burn model in rats. J Med Assoc Thai. 2000;83(4):417–425.
31. Ahmadloo N, Kadkhodaei B, Omidvari S, et al. Lack of prophylactic effects of aloe vera gel on radiation induced dermatitis in breast cancer patients. Asian Pac J Cancer Prev. 2017;18(4):1139–1143.
32. Heggie S, Bryant GP, Tripcony L, et al. A phase III study on the efficacy of topica aloe vera gel on irradiated breast tissue. Cancer Nurs. 2002;25(6):442–451. doi:10.1097/00002820-200212000-00007
33. Hoopfer D, Holloway C, Gabos Z, et al. Three-arm randomized phase III trial: quality aloe and placebo cream versus powder as skin treatment during breast cancer radiation therapy. Clin Breast Cancer. 2014;15(3):181–190.
34. Farrugia CJ, Burke ES, Haley ME, Bedi KT, Gandhi MA. The use of aloe vera in cancer radiation: an updated comprehensive review. Complement Ther Clin Pract. 2019;35:126–130. doi:10.1016/j.ctcp.2019.01.013
35. Maiche AG, Grӧhn P, Mӓki-Hokkonen H. Effect of chamomile cream and almond ointment on acute radiation skin reaction (1991) correspondence and short communications. Acta Oncol. 1991;30(3):395–397.
36. Ferreira EB, Ciol MA, de Meneses AG, Bontempo PSM, Hoffman JM, Reis PEDD. Chamomile gel versus urea cream to prevent acute radiation dermatitis in head and neck cancer patients: results from a preliminary clinical trial. Integr Cancer Ther. 2020;19:1534735420962174. doi:10.1177/1534735420962174
37. Karbasforooshan H, Hosseini S, Elyasi S, et al. Topical silymarin administration for prevention of acute radiodermatitis in breast cancer patients: a randomize double-blind, placebo-controlled clinical trial. Phytother Res. 2018;33(2):379–386.
38. Rafati M, Ghasemi A, Saeedi M, et al. Nigella sativa L. for prevention of acute radiation dermatitis in breast cancer: a randomized, double-blind, placebo-controlled, clinical trial. Complement Ther Med. 2019;47:102205. doi:10.1016/j.ctim.2019.102205
39. Kumar S, Juresic E, Barton M, Shafiq J. Management of skin toxicity during radiation therapy: a review of the evidence. J Med Imaging Radiat Oncol. 2010;54:264–279. doi:10.1111/j.1754-9485.2010.02170.x
40. Yudovsky D, Pilon L. Retrieving skin properties from in vivo spectra reflectance measurements. J Biophotonics. 2010;4(5):305–314.
41. Yudovsky D, Nouvong A, Pilon L. Hyperspectral imaging in diabetic foot wound care. J Diabetes Sci Technol. 2010;4(5):1099–1111. doi:10.1177/193229681000400508
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.