Back to Journals » Risk Management and Healthcare Policy » Volume 16
Outpatient Spine Surgery in Poland: A Survey on Popularity, Challenges, and Future Perspectives
Authors Latka K ![]() , Kołodziej W, Rajski R, Pawuś D
, Kołodziej W, Rajski R, Pawuś D ![]() , Chowaniec J, Latka D
, Chowaniec J, Latka D
Received 4 July 2023
Accepted for publication 31 August 2023
Published 12 September 2023 Volume 2023:16 Pages 1839—1848
DOI https://doi.org/10.2147/RMHP.S425465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Kajetan Latka,1,2 Waldemar Kołodziej,2,3 Rafal Rajski,3 Dawid Pawuś,4 Jacek Chowaniec,3 Dariusz Latka2,3
1Department of Neurosurgery, The St. Hedwig’s Regional Specialist Hospital, Opole, Poland; 2Center for Minimally Invasive Spine and Peripheral Nerve Surgery neurochirurg.opole.pl, Opole, Poland; 3Department of Neurosurgery, Institute of Medical Sciences, University of Opole, Opole, Poland; 4Faculty of Electrical Engineering, Automatic Control and Informatics, Opole University of Technology, Opole, Poland
Correspondence: Kajetan Latka, Tel +48609225084, Email [email protected]
Objective: This study aimed to investigate the popularity of outpatient spine surgery in Poland, identify factors influencing its adoption, and assess its benefits, challenges, and impact on patient outcomes and healthcare costs. Additionally, the study proposes strategies to improve outpatient spine surgery adoption and ensure its safe implementation in Poland.
Materials and Methods: An electronic survey was distributed to members of the Polish Spine Surgery Society and the Polish Neurosurgery Society. Data were analyzed using Matlab R2020b statistical software, employing descriptive statistics to summarize the responses.
Results: The survey indicated that 67% of respondents provide spinal procedures commercially, with 58% performing them on an outpatient basis, showing the growing role of the private sector in providing spinal surgery services in Poland. Root nerve blocks and joint blocks were the most common outpatient procedures, followed by microdiscectomy, endoscopic discectomy, and L-S spinal fusion. The public NHF was the most common payer for outpatient procedures.
Conclusion: Outpatient spine surgery in Poland is not yet widespread, but improvements can be made to reduce hospital stays and enhance recovery. Changes in reimbursement systems to cover outpatient procedures and addressing physicians’ liability concerns, particularly by emphasizing the NO-fault system, are essential. With proper support, outpatient spine surgery could become a valuable addition to Poland’s healthcare system.
Keywords: spine surgery, outpatient, endoscopy
Introduction
In recent years, the field of surgery has witnessed a remarkable transformation, thanks to advancements in medical research and the development of evidence-based protocols. Outdated practices that resulted in high perioperative mortality rates, frequent intraoperative infections, and lengthy hospital stays have now become a thing of the past. Modern surgical procedures are designed to be less invasive, more efficient, and with faster recovery times, allowing patients to return to their normal lives as quickly as possible.
One of the most significant developments in surgery has been the introduction of enhanced recovery after surgery (ERAS) protocols. ERAS is a patient-centered, evidence-based approach to perioperative care that emphasizes early mobilization, nutrition, and pain management, and has been shown to improve patient outcomes, reduce hospital stays, and lower healthcare costs.1,2
Another significant advancement in surgical care has been the evolution of anesthesia techniques. Regional anesthesia, such as epidural anesthesia, has been shown to be an effective method for pain control in many surgical procedures.3 Total Intravenous Anesthesia (TIVA) has also gained popularity, offering improved intraoperative hemodynamic stability and faster emergence from anesthesia.4
In the field of spine surgery, advances in surgical techniques, implants, and visualization have led to the development of a range of outpatient procedures. Outpatient spine surgery refers to surgical procedures that can be performed on an outpatient basis, allowing patients to go home on the same day as their surgery.5 Compared to traditional inpatient procedures, outpatient spine surgery has been shown to result in fewer complications, reduced healthcare costs, and faster return to daily activities.6,7
Despite the benefits of outpatient spine surgery, there are still challenges and controversies surrounding its adoption. One of the main obstacles to the widespread adoption of outpatient spine surgery is the reluctance of healthcare providers to perform these procedures due to a lack of awareness and training.8 Additionally, patients may be hesitant to undergo outpatient spine surgery due to concerns about the safety and efficacy of the procedure.
In Poland, healthcare is funded through the National Health Fund (NHF), a public entity financed by compulsory health contributions. Despite the advantages of outpatient spine surgery, the NHF still imposes hospitalization obligations for spinal procedures, leading to increased costs and longer waiting times for patients.9–12 However, private healthcare providers are now offering outpatient spine surgery, providing patients with state-of-The-art methods without the need for artificial hospitalization.13–15
In this study, we aimed to investigate the popularity of outpatient spine surgery among healthcare providers in Poland, and the factors that influence its adoption. We will also examine the benefits and challenges of outpatient spine surgery, and the impact it has on patient outcomes and healthcare costs. Finally, we will propose strategies to improve the adoption of outpatient spine surgery and ensure its safe and effective implementation in Poland.
Materials and Methods
To investigate the popularity of outpatient spine surgery among healthcare providers in Poland, an electronic survey was conducted. The survey consisted of 25 questions (Figure 1) and was distributed to members of the Polish Spine Surgery Society and the Polish Neurosurgery Society over a one-month period from August through September 2022. A unique link was sent to each respondent to prevent multiple responses from a single participant. The survey questions included, among others, the types of procedures performed and their frequency, the form of their provision (private vs public), the time from the procedure to verticalization, and general information such as the place of work and managerial function.
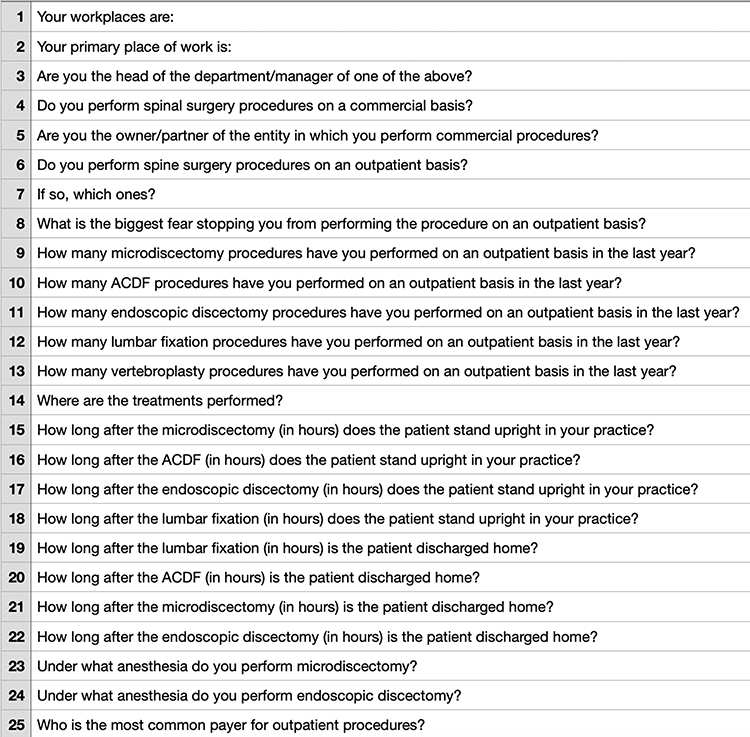 |
Figure 1 English Translation of Survey Questions Used in the Study. |
Data collected from the survey were analyzed using the Matlab R2020b statistical software. Descriptive statistics were used to summarize the responses, including means and standard deviations for continuous variables and frequencies and percentages for categorical variables. To ensure the anonymity and confidentiality of the respondents, the data were de-identified and aggregated.
No sensitive personal data was collected in this survey, and all data were anonymized to maintain the privacy of the participants. As this study did not involve patients, patient data, or interventions, and due to the nature of the data collected, it was deemed by our institution that ethical approval from a Bioethics Committee was not required. However, all aspects of the study were conducted in accordance with the ethical standards of research. This research complies with all relevant national regulations and institutional policies.
Results
A total of 43 respondents from 30 different spine centers in Poland participated in the study, and the results were analyzed and presented in Table 1. In terms of the respondents’ main working place, the majority of them (49%) work in a neurosurgery ward, followed by 37% in an NHF-funded orthopedics ward. Only 2% work in a surgical dispensary (Figure 2). Furthermore, a significant number of respondents (74%) declared that they work in more than one center simultaneously, which may suggest that they have a broad range of experience in different medical settings (Figure 3).
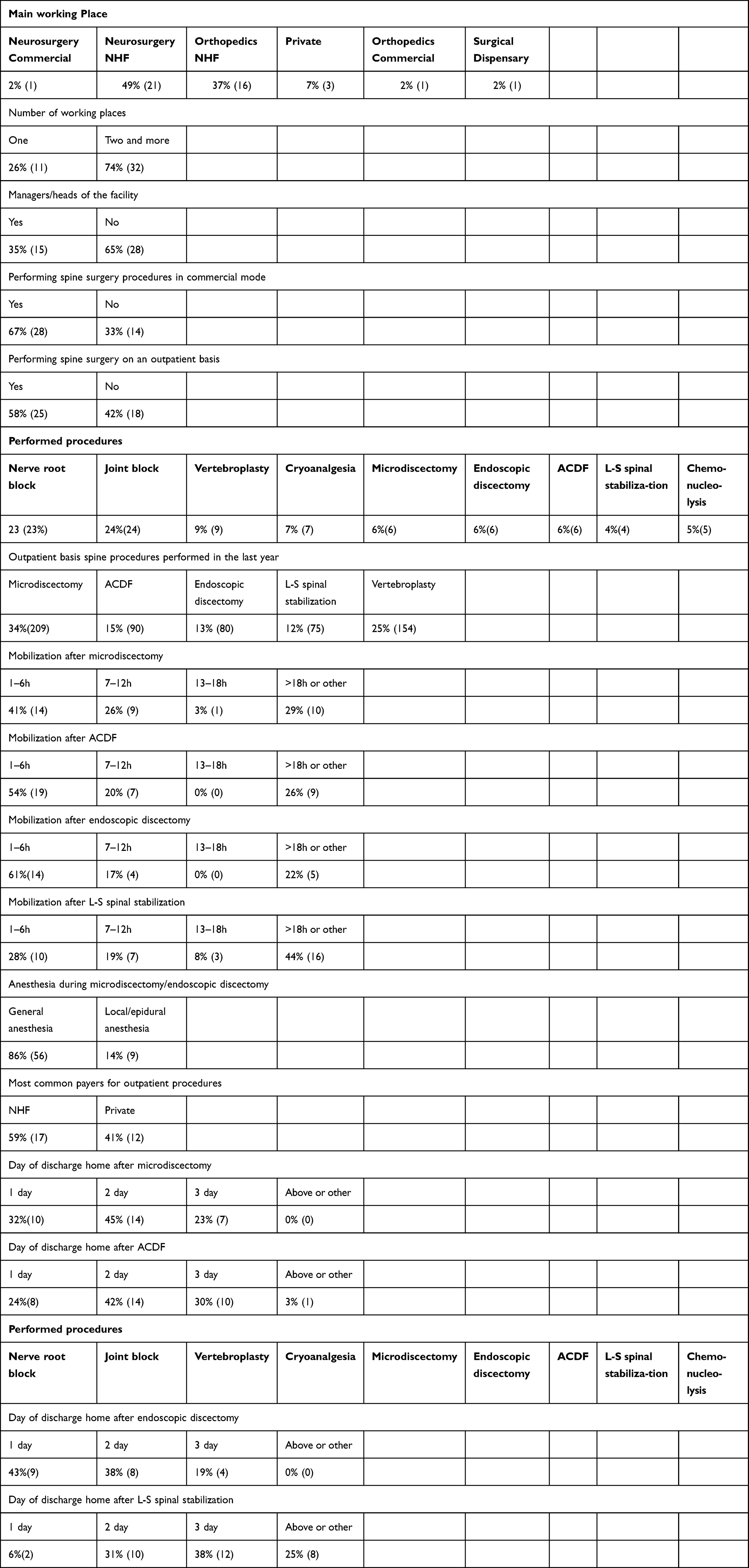 |
Table 1 Detailed Study of the Survey Results |
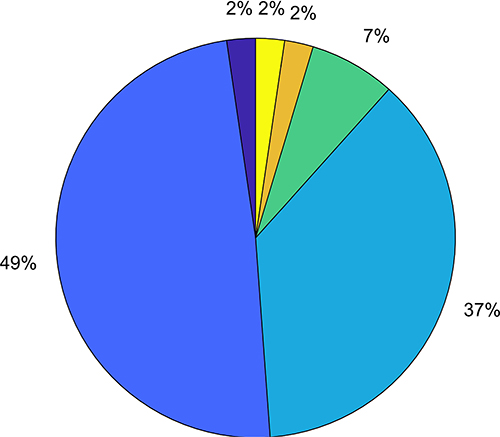 |
Figure 2 Graphical layout of the main workplaces. 2% - Neurosurgery – Commercial, 2% - Surgical dispensary, 2% - Orthopedics – Commercial, 7% - Private, 37% - Orthopedics – NHF, 49% - Neurosurgery – NHF. |
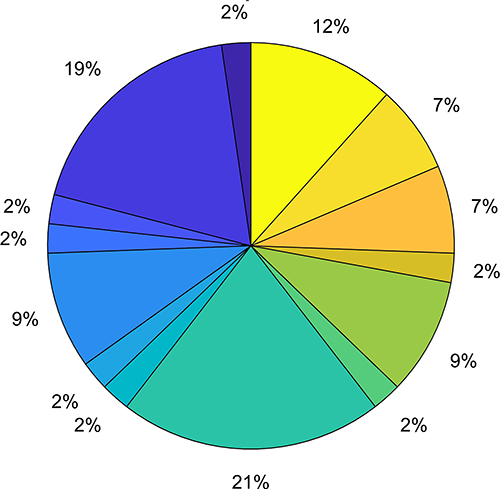 |
Figure 3 Graphical layout of all declared working places. 2% - Neurosurgery - Commercial, Private, 2% - Neurosurgery - NHF, Surgical dispensary, 2% - Neurosurgery - NHF, Neurosurgery – Commercial, 2% - Neurosurgery - NHF, Orthopedics - NHF, Neurosurgery - Commercial, Private, 2% - Neurosurgery - NHF, Orthopedics - NHF, Private, 2% - Orthopedics - Commercial, Private, 2% - Orthopedics - NHF, Neurosurgery - Commercial, Private, 7% - Orthopedics - NHF, Orthopedics - Commercial, Private, 7% - Orthopedics - NHF, Orthopedics – Commercial, 9% - Neurosurgery - NHF, Neurosurgery - Commercial, Private, 9% - Orthopedics –NHF, 12% - Orthopedics- NHF, Private, 19% - Neurosurgery – NHF, 21% - Neurosurgery - NHF, Private. |
Regarding the provision of spinal procedures, 67% of the respondents provide them privately, while 58% of them perform them on an outpatient basis (Figure 4). This suggests that the private sector in Poland plays a significant role in providing spinal surgery services to patients, and that outpatient procedures are becoming increasingly common. Root nerve blocks and joint blocks are the most commonly performed procedures, followed by microdiscectomy, endoscopic discectomy, and L-S spinal stabilization.
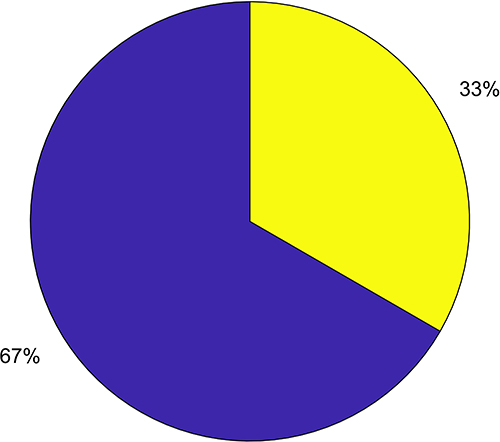 |
Figure 4 Do you performing commercial operations? 67% - YES, 33% - NO. |
When asked about their greatest concerns in performing outpatient procedures, 25% of respondents mentioned early surgical complications, 11% postoperative pain, 8% anesthesiology complications, and 14% fear of prosecution and potential claims. However, almost 30% pointed to organizational issues and weak infrastructure (Figure 5).
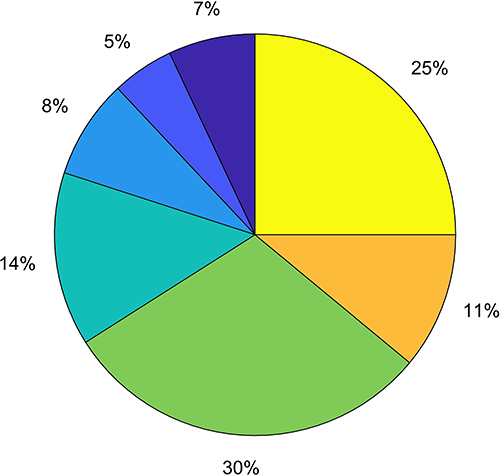 |
Figure 5 What is your biggest concern that prevents you from performing a procedure in an outpatient setting? 5% - Lack of staff, 7% - Other, 8% - Anasthesiological complications, 11% - Post-operative pain, 14% - Fear of potential legal accusations and prosecution, 25% - Early surgical complications, 30% - Facility problems. |
The time from the end of the procedure to the patient’s upright position is an important factor in assessing the effectiveness of spinal surgery procedures. According to the survey results, 41% of respondents declared that patients were verticalized within 6 hours after microdiscectomy, and even 61% after endoscopic surgery. However, after the L-S spinal stabilization operation, only 28% of respondents reported that patients were verticalized within 6 hours. It should be noted that these are self-reported times provided by the respondents and may not necessarily reflect the actual times in practice. Nevertheless, this conclusion suggests that while microdiscectomy and endoscopic discectomy are perceived as minimally invasive procedures and surgeons are increasingly comfortable with early mobilization of their patients, fusion procedures are still perceived as requiring longer mobilization times.
It is important to note that the results reflect the responses of surgeons regarding the expected discharge time for their patients. According to their declarations, the majority of patients were expected to be discharged on the same day after endoscopic discectomy (43%), followed by microdiscectomy (32%). Only 6% of respondents declared that patients after L-S spinal fixation were expected to be discharged on the same day. The most common expected discharge day for each of the surgeries was day 2.
Indeed, it should be noted that the vast majority of respondents (86%) declared that they prefer to perform spinal surgery procedures under general anesthesia, while only 14% preferred local/epidural anesthesia. This finding suggests that general anesthesia is the preferred method of anesthesia for spinal surgery procedures in Poland, according to the surveyed surgeons.
These findings suggest that outpatient spinal procedures are feasible in Poland, but there is still room for improvement in terms of reducing hospital stays and facilitating the recovery process.
Finally, the most common payer for outpatient procedures was the public NHF, which is the dominant entity of financing in Poland. This finding suggests that even though outpatient spinal procedures are becoming more popular, the public healthcare system still plays a significant role in financing them.
Discussion
The dynamic development of medicine and medical technology has created unique opportunities for surgical fields. Gone are the days when patients stayed in the hospital for many days and weeks after surgery.16 The idea of outpatient surgeries has been developed, resulting not only in excellent short and long-term results but also in good mental comfort of the patient, including reducing stress resulting from the need for hospitalization. Injection procedures are now practiced only on an outpatient basis, regardless of whether they cover surface tissues, such as facial injections in aesthetic medicine, or deep, eg, nerve root blocks, joint blocks, etc.17,18
Endoscopy has been a milestone development in increasing the benefits of the procedure, with the smallest possible surgical accesses and with a very high safety threshold.19 Open procedures, such as inguinal hernia surgery, or even very precise procedures, such as cataract correction, have also entered the repertoire of outpatient procedures.20,21
Spine surgery is another field within the scope of one-day surgery, which is particularly noticeable in highly developed countries with a free-market model of health care financing.22 In Poland, outpatient spinal surgeries are an extremely rare phenomenon, and as of the date of preparation of the following study, only three centers in Poland perform them in this format. The reason for this phenomenon is very complex and requires in-depth analysis. Probably the most significant issue is related to the financial aspect of outpatient procedures.23
Public health care in Poland is financed primarily by the National Health Fund (NHF), which determines the amount of reimbursement of drugs, procedures, etc. and sets the conditions necessary to receive them and limits on the permissible number of procedures performed. Currently, the NHF does not reimburse spine surgeries performed in outpatient care and only allows reimbursement of treatment costs in the case of hospitalization lasting several days.24 Furthermore, by applying homogeneous patient groups, the system even stimulates hospitals to artificially prolong hospitalizations to achieve the highest reimbursement level. For instance, the performance of a decompressive spinal operation with a three-day hospitalization cost about 3000 euros, while additional single day in hospital increases the price to 4500 euros. These mechanisms may discourage further adoption of outpatient spine surgery in Poland.
By dividing patients into those qualified for hospitalization and those qualified for outpatient treatment, not only does waiting time decrease significantly, but also the costs associated with unnecessary hospitalization are significantly reduced.24,25 Spinal surgeries are the most expensive procedures, both in Europe and in the United States, and a small group of patients is able to individually finance the costs of treatment in the private sector.2,26
The COVID-19 pandemic has had a significant impact on healthcare systems worldwide, and Poland is no exception.27 The public health crisis caused by the pandemic led to the suspension of elective hospitalizations for several months in overburdened public hospitals. This period was particularly challenging for the healthcare system and demonstrated the potential for outpatient settings to alleviate the strain on hospitals. During this period, the authors observed a record number of outpatient procedures performed in their ambulatory center. The need to reduce hospital stays to minimize patients’ potential exposure to COVID-19 and to free up resources for patients with acute needs provided an unexpected impetus for the expansion of outpatient spine surgery. This experience highlighted the potential resilience and adaptability of outpatient settings during a public health crisis and provided a unique opportunity to assess the feasibility, safety, and efficiency of outpatient spine surgery under such extraordinary circumstances.
One of the significant barriers to the development of outpatient spinal surgeries in Poland is the fear of possible complications and medical lawsuits, which is a concern shared by many medical professionals. The law in Poland is very strict in the case of adjudication of unintentional medical malpractice, and this is a significant issue that requires clarification, particularly in the case of developing rules for public outpatient procedures. The No-Fault system, which would be introduced more and more widely in developed countries, would be particularly beneficial, which would positively affect the comfort of doctors’ work and the treatment of the patient.28,29
The fear of legal consequences is a well-known phenomenon in the medical community, and in Poland, the legal environment has made it challenging for doctors to perform outpatient spinal surgeries. The current legislation is very strict, and doctors are understandably concerned about their potential liability in the event of a medical mistake or malpractice. As a result, many doctors are hesitant to perform outpatient surgeries and prefer to err on the side of caution by performing procedures in a hospital setting, where there is a higher level of supervision and support.
However, it is essential to note that the risk of complications associated with outpatient spinal surgeries is relatively low, and the benefits of these procedures are significant. By introducing a division into patients qualified for hospitalization and patients qualified for outpatient treatment, not only does the waiting time decrease significantly, but also the costs associated with unnecessary hospitalization are significantly reduced.13 In addition to the direct cost reduction, the patient’s recovery time and, as a result, the return to work are shortened, which can have a positive impact on their overall quality of life. It is important to consider that outpatient spinal surgeries have been successfully performed in other countries, including the United States, with good results and high patient satisfaction.12 Furthermore, the development of outpatient spinal surgeries would also have a positive impact on the overall healthcare system in Poland. By reducing hospitalizations, the burden on hospitals and healthcare staff could be decreased, allowing for more resources to be allocated to other areas of healthcare. Additionally, outpatient surgeries could lead to a more efficient use of medical equipment and facilities, reducing costs and improving overall healthcare productivity.13 In conclusion, the development of outpatient spinal surgeries in Poland has the potential to greatly benefit patients and the healthcare system. While there are several barriers to the implementation of these procedures, including financial and legal concerns, it is important to consider the potential benefits and work towards finding solutions to these barriers. With proper support from the government, medical professionals, and the National Health Fund, the implementation of outpatient spinal surgeries in Poland could provide a valuable addition to the country’s healthcare system.
In the authors’ view, the described barriers and difficulties are not limited to outpatient spine surgery but are indeed reflective of many underlying issues present in the healthcare model adopted in Poland. What might seem to be simple legislative solutions may prove to be challenging to implement in such a flawed system. Although it might appear that a patient with insurance, mandatory and provided by the National Health Fund, should have the freedom to choose the facility to perform the medical procedure, which would then be reimbursed by the insurer, the reality is different. In fact, patients can only choose between facilities that have a contract with the insurer. The granting of such contracts can often be influenced by political considerations, particularly when the hospital is governmental or owned by the local authority rather than being a private facility, which adds another layer of complexity to the healthcare landscape. Additionally, seemingly straightforward matters like contracting medical service providers in Poland remain highly opaque. Hospital contracts are often automatically extended, and tenders for new providers appear sporadically. Given such a system, it is hard to imagine that newly established ambulatory centers would effortlessly start providing services for the National Health Fund. These system-wide challenges demand thoughtful analysis and careful planning for sustainable solutions. The experience and insights gained from the focused examination of outpatient spine surgery could serve as a catalyst for broader reforms, promoting more accessible, efficient, and patient-centered healthcare in Poland.
Conclusions
The conducted survey shows that outpatient spine surgery in Poland is still not very popular. Most of the procedures performed are minor procedures such as vertebro- or kyphoplasties, chemonucleolysis, thermo- or cryo- ablations. According to the authors, outpatient surgeries are an extremely effective solution from the point of view of the doctor and the patient, as well as economical from the point of view of the public payer. However, it is necessary to change the reimbursement systems and cover outpatient procedures, and work on changes in the system of physicians’ liability for errors, with particular emphasis on the No-fault system.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Debono B, Wainwright TW, Wang MY, et al. Consensus statement for perioperative care in lumbar spinal fusion: enhanced recovery after surgery (ERAS®) society recommendations. Spine J. 2021;21(5):729–752. PMID: 33444664. doi:10.1016/j.spinee.2021.01.001
2. Dietz N, Sharma M, Adams S, et al. Enhanced recovery after surgery (ERAS) for spine surgery: a systematic review. World Neurosurg. 2019;130:415–426. PMID: 31276851. doi:10.1016/j.wneu.2019.06.181
3. Noba L, Rodgers S, Chandler C, Balfour A, Hariharan D, Yip VS. Enhanced recovery after surgery (ERAS) reduces hospital costs and improve clinical outcomes in liver surgery: a systematic review and meta-analysis. J Gastrointest Surg. 2020;24(4):918–932. PMID: 31900738; PMCID: PMC7165160. doi:10.1007/s11605-019-04499-0
4. Pereira L, Figueiredo-Braga M, Carvalho IP. Preoperative anxiety in ambulatory surgery: the impact of an empathic patient-centered approach on psychological and clinical outcomes. Patient Educ Couns. 2016;99(5):733–738. PMID: 26654958. doi:10.1016/j.pec.2015.11.016
5. Isik O, Kaya E, Dundar HZ, Sarkut P. Surgical site infection: re-assessment of the risk factors. Chirurgia. 2015;110(5):457–461. PMID: 26531790.
6. Ubaldi K. Challenges Facing the Ambulatory Surgery Center Market. AORN J. 2019;109(4):428–430. PMID: 30919418. doi:10.1002/aorn.12656
7. Detmer DE, Gelijns AC. Ambulatory surgery. A more cost-effective treatment strategy? Arch Surg. 1994;129(2):123–127. PMID: 8304823. doi:10.1001/archsurg.1994.01420260009001
8. Friedlander DF, Krimphove MJ, Cole AP, et al. Where Is the Value in Ambulatory Versus Inpatient Surgery? Ann Surg. 2021;273(5):909–916. PMID: 31460878. doi:10.1097/SLA.0000000000003578
9. Torabi SJ, Patel RA, Birkenbeuel J, Nie J, Kasle DA, Manes RP. Ambulatory surgery centers: a 2012 to 2018 analysis on growth in number of centers, utilization, Medicare services, and Medicare reimbursements. Surgery. 2022;172(1):2–8. PMID: 34973814. doi:10.1016/j.surg.2021.11.033
10. Suskind AM, Dunn RL, Zhang Y, Hollingsworth JM, Hollenbeck BK. Ambulatory surgery centers and outpatient urologic surgery among Medicare beneficiaries. Urology. 2014;84(1):57–61. PMID: 24976220; PMCID: PMC4077194. doi:10.1016/j.urology.2014.04.008
11. Pasternak LR, Johns A. Ambulatory gynaecological surgery: risk and assessment. Best Pract Res Clin Obstet Gynaecol. 2005;19(5):663–679. PMID: 16011908. doi:10.1016/j.bpobgyn.2005.06.003
12. Gologorsky Y. Outpatient spine surgery: transition to the ambulatory surgery center. World Neurosurg. 2018;114:369–370. PMID: 29689398. doi:10.1016/j.wneu.2018.04.119
13. Durand WM, Musharbash FN, Ortiz-Babilonia CD, Jain A. Characteristics of spine surgery performed at ambulatory surgical centers. Spine. 2023;48(2):143–145. PMID: 36122294. doi:10.1097/BRS.0000000000004480
14. Rój J, Jankowiak M. Socioeconomic determinants of health and their unequal distribution in Poland. Int J Environ Res Public Health. 2021;18(20):10856. PMID: 34682597; PMCID: PMC8536126. doi:10.3390/ijerph182010856
15. Sowada C, Sagan A, Kowalska-Bobko I, et al. Poland: health System Review. Health Syst Transit. 2019;21(1):1–234. PMID: 31333192.
16. Bellani ML. Psychological aspects in day-case surgery. Int J Surg. 2008;6(1):S44–6. PMID: 19167936. doi:10.1016/j.ijsu.2008.12.019
17. McCartney CJL, McIsaac D. Are peripheral nerve blocks indicated in ambulatory knee surgery? Anesth Analg. 2019;128(1):3–4. PMID: 30550466. doi:10.1213/ANE.0000000000003646
18. Stewart J, Gasanova I, Joshi GP. Spinal anesthesia for ambulatory surgery: current controversies and concerns. Curr Opin Anaesthesiol. 2020;33(6):746–752. PMID: 33002959. doi:10.1097/ACO.0000000000000924
19. Frakes JT. Outpatient endoscopy. The case for the ambulatory surgery center. Gastrointest Endosc Clin N Am. 2002;12(2):215–227. PMID: 12180155. doi:10.1016/s1052-5157(01)00004-6
20. Nordin AB, Shah SR, Kenney BD. Ambulatory pediatric surgery. Semin Pediatr Surg. 2018;27(2):75–78. PMID: 29548355. doi:10.1053/j.sempedsurg.2018.02.003
21. Bigoteau M, Grammatico-Guillon L, Massot M, et al. Ambulatory surgery centers: possible solution to improve cataract healthcare in medical deserts. J Cataract Refract Surg. 2021;47(3):352–357. PMID: 33086293. doi:10.1097/j.jcrs.0000000000000452
22. Gray DT, Deyo RA, Kreuter W, et al. Population-based trends in volumes and rates of ambulatory lumbar spine surgery. Spine. 2006;31(17):1957–1963. PMID: 16924213. doi:10.1097/01.brs.0000229148.63418.c1
23. Ertl G. Medicine in free market economies. J Am Coll Cardiol. 2012;59(17):1566–1567. PMID: 22516448. doi:10.1016/j.jacc.2012.01.027
24. Smarżewska D, Wereda WS, Jończyk JA. Assessment of the health care system in poland and other OECD countries using the hellwig method. Int J Environ Res Public Health. 2022;19(24):16733. PMID: 36554611; PMCID: PMC9779126. doi:10.3390/ijerph192416733
25. Gennari A, Mazas S, Coudert P, Gille O, Vital JM. Outpatient anterior cervical discectomy: a French study and literature review. Orthop Traumatol Surg Res. 2018;104(5):581–584. PMID: 29902639. doi:10.1016/j.otsr.2018.04.014
26. Nieszporska S. Priorities in the Polish health care system. Eur J Health Econ. 2017;18(1):1–5. PMID: 27682073; PMCID: PMC5209398. doi:10.1007/s10198-016-0831-0
27. Korneta P, Kludacz-Alessandri M, Walczak R. The impact of COVID-19 on the performance of primary health care service providers in a capitation payment system: a case study from Poland. Int J Environ Res Public Health. 2021;18(4):1407. PMID: 33546467; PMCID: PMC7913620. doi:10.3390/ijerph18041407
28. Mikos M, Budzowska J, Banaś T, et al. Civil lawsuits as an indicator of adverse outcomes in healthcare. Int J Environ Res Public Health. 2022;19(17):10783. PMID: 36078499; PMCID: PMC9518515. doi:10.3390/ijerph191710783
29. Kassim PN. No-fault compensation for medical injuries: trends and challenges. Med Law. 2014;33(4):21–53. PMID: 27351046.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.