Back to Journals » Patient Preference and Adherence » Volume 19
Outpatient Process Transformation and Patient Satisfaction Under New Public Service Theory
Authors Cai Z, Wu A, Wang X, Xie H
Received 4 June 2025
Accepted for publication 14 October 2025
Published 29 October 2025 Volume 2025:19 Pages 3349—3361
DOI https://doi.org/10.2147/PPA.S544684
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Zejun Cai,1 Ali Wu,1 Xiaofeng Wang,1 Haofen Xie2
1Department of Gastroenterology Surgery, First Affiliated Hospital of Ningbo University, Ningbo, Zhejiang, 315010, People’s Republic of China; 2Department of Outpatient, First Affiliated Hospital of Ningbo University, Ningbo, Zhejiang, 315010, People’s Republic of China
Correspondence: Haofen Xie, Department of Outpatient, First Affiliated Hospital of Ningbo University, No. 59 of Liuting Street, Haishu District, Ningbo, Zhejiang, 315010, People’s Republic of China, Tel +8613867889859, Email [email protected]
Objective: To explore the impact of outpatient process transformation guided by new public service (NPS) theory on patient satisfaction.
Methods: A total of 600 outpatients were randomly selected for satisfaction surveys before and after the process transformation, which was designed and implemented based on the principles of NPS theory. The transformation targeted areas with satisfaction scores below 9 points. Data were collected in June–August 2023 (pre-transformation) and June–August 2024 (post-transformation).
Results: After the process transformation, patient satisfaction scores significantly improved across all dimensions, including the medical environment, treatment procedures, service quality, respect for patients, privacy protection, responsiveness to complaints and overall evaluation (all P < 0.05).
Conclusion: The application of NPS theory in outpatient process management effectively enhances patient satisfaction and service quality. This study provides empirical support for the value of patient-centred reforms and offers practical insights for healthcare institutions seeking to improve outpatient services through theory-guided interventions.
Keywords: new public service theory, outpatient service, process transformation, degree of satisfaction
Introduction
New public service (NPS) theory, proposed by renowned American public administration scholars Denhardt and Denhardt through their critical analysis of new public management theory, emphasises that public services should prioritise citizens’ needs and stress civic engagement and social responsibility.1 In recent years, patient satisfaction has become a key metric for evaluating hospital service quality.2,3 As the frontline of healthcare delivery, outpatient services reflect a hospital’s management efficacy, partly evidenced by patient satisfaction levels. However, common issues such as prolonged waiting times, inadequate doctor–patient communication and insufficient environmental cleanliness persist in outpatient settings, negatively impacting the patient experience and satisfaction.
The adoption of NPS theory is particularly relevant for outpatient care reform for several reasons. First, unlike traditional new public management approaches that emphasise efficiency and cost control, NPS theory prioritises citizen-centred values, dialogue and participatory governance.1,4 This aligns perfectly with the need to improve patient-centred care in outpatient settings, where service quality depends heavily on effective communication, respect for patient needs and a responsive service design. Second, NPS theory’s principles of “serving rather than steering” and “valuing people, not just productivity” provide a framework for transforming outpatient processes from administrative-driven to patient-driven workflows. This is critical in addressing widespread patient dissatisfaction related to impersonal care, bureaucratic inefficiencies and the lack of empathy in medical interactions. Furthermore, NPS theory improves upon other management frameworks, such as lean or total quality management, by explicitly emphasising democratic participation, transparency and public value creation. Although other approaches may focus narrowly on process efficiency, NPS theory incorporates broader social and ethical dimensions, making it especially suitable for public healthcare systems where equity and accountability are paramount.
The principle of “serving rather than steering” in NPS theory requires hospital managers to shift from traditional control-oriented roles to becoming service providers, placing greater emphasis on addressing patients’ individual needs, and to provide more convenient and efficient medical services through optimised outpatient procedures. The principle of “emphasising citizenship” is reflected in medical practice by respecting patients’ rights to information, participation and choice. By involving patients in the design and improvement of outpatient processes, hospitals can enhance patients’ sense of engagement and satisfaction. However, previous evaluations of outpatient service quality often focused on technical efficiency and cost control while overlooking the quality of the interactive experience and service delivery from the patient’s perspective.5,6
This study adopts a pre- and post-control design, randomly selecting 600 outpatients to form two groups for satisfaction surveys and evaluating them before and after the process transformation. The specific objectives of this study are the following: (1) to design and implement an outpatient process transformation based on the principles of NPS theory; (2) to evaluate the impact of this transformation on patient satisfaction across multiple dimensions, including the medical environment, treatment process, service attitude and feedback mechanisms; and (3) to provide evidence-based recommendations for healthcare institutions seeking to apply NPS theory in outpatient service reform. Moreover, this research aims to apply NPS theory to the transformation of the outpatient process, improve overall service quality by improving doctor–patient interaction and patient participation, compensate for the shortcomings of previous research and provide medical management departments and medical institutions with practical experience to learn from and promote improvements in outpatient service quality and the optimal allocation of medical resources.
Participants and Methods
Study Design
This study employed a quasi-experimental, pre–post comparison design to evaluate the impact of outpatient process transformation guided by NPS theory.
Research Participants
Patients who visited the outpatient clinic of our hospital between June and August 2023 and June and August 2024 were randomly selected each month for participation in this study, with all patient satisfaction assessments completed by specific personnel from third-party assessment agencies. Before the study began, all patients were informed of the value and purpose of the study and signed an informed consent form. Inclusion criteria: any outpatient who was willing to participate and understood the value of the study. Exclusion criteria: patients <18 years, patients who were unable to communicate effectively and those who were unwilling to participate.
Investigation Tools
Based on the survey results from the hospital quality management department on outpatient satisfaction, a questionnaire was designed. The instrument demonstrated good internal consistency, with a reliability coefficient of 0.872 and a content validity index of 0.891. The questionnaire contained 16 items covering the outpatient consultation environment, medical procedures, healthcare services and feedback evaluation. Except for the overall evaluation item, all items were scored using a Likert scale based on satisfaction: 5 points for “satisfied”, 4 for “relatively satisfied”, 3 for “basically satisfied”, 2 for “dissatisfied” and 1 for “very dissatisfied”. The overall evaluation was scored directly by patients on a scale from 1 to 10, where 1 is the lowest and 10 is the highest (see Table 1 for details).
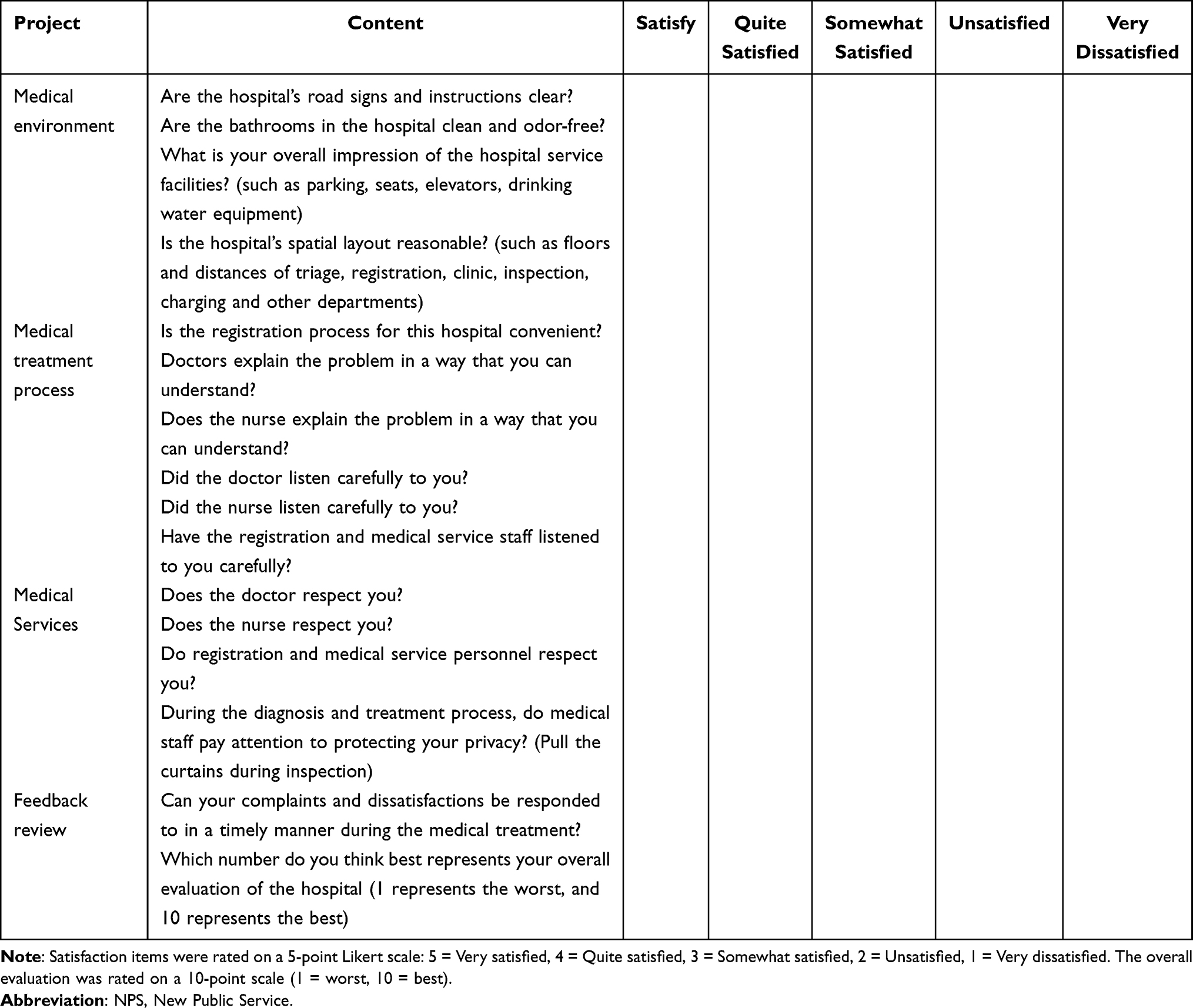 |
Table 1 Outpatient Patient Satisfaction Survey Items and Rating Scale (N = 600) |
Investigation Method
This study employed a random sampling method. Each month, all eligible outpatients were assigned numbers based on their visit records to establish a sampling frame. A computer-generated random number table was used to select a starting point; numbers were then read sequentially, and those within the range were selected until 200 patients were identified. Drawn numbers were checked against the inclusion criteria. Numbers that did not meet the criteria were excluded and replaced through additional draws until the required sample size of 200 was reached. The same sampling procedure was applied both before and after the process improvement to ensure the balance and comparability of the data.
The strength of this methodology lies in the use of random sampling, validated questionnaires and third-party data collection, which enhance the objectivity and reliability of the findings.
Prior to the redesign of the outpatient process, patient scores regarding the medical environment, procedures, services and feedback evaluation were collected. Process improvements then targeted items with average scores below 4.5. All transformations were guided by the principles of NPS theory, adopting a patient-centred approach that is responsive to their needs and people oriented. The objectives were to address issues identified within the outpatient process, implement corrective measures, deliver higher-quality medical services and experiences and enhance the capacity of public hospitals to deliver public services.
Based on experience in process improvement research, 6 months was selected as the observation period.7,8 This time period is long enough to observe major changes without being so long that the research is affected by external factors, such as changes in hospital policies, seasonal variations, or shifts in patient demographics. After the transformation, the outpatients were evaluated again in terms of the outpatient clinic environment, medical procedures, medical quality, service convenience and overall evaluation, and statistical analysis was performed.
Specific Methods for Transforming the Outpatient Process Under the Guidance of New Public Service Theory
Creating a Positive Medical Environment
The outpatient clinic operates ventilation systems throughout the year to improve air quality in the diagnostic and treatment areas. In accordance with the standards for third-class public toilets set by the National Housing and Urban–Rural Development Commission, the clinic has accelerated the renovation of toilet facilities. Sanitation supervisors conduct daily inspections, and cleaning staff perform regular maintenance to ensure a ventilated, dry, clean and odour-free environment while also providing complimentary toilet paper.
The clinic has collaborated with professional advertising firms to create highly visible and diverse medical guidance signage. Outpatient managers have enhanced dynamic management practices, encouraging triage and pre-examination nurses to provide proactive guidance to patients. Additionally, social volunteers and hospital staff volunteers have been recruited, trained and assigned to appropriate roles, ensuring that patients receive timely assistance whenever needed.
Optimising the Medical Treatment Process
Research indicates that outpatient traffic is unevenly distributed, with substantial disparities between peak and trough periods. This leads to severe queues during peak hours and underutilisation of service windows during off-peak times.9 To address these issues, operational rules have been formulated for appointment-based diagnosis and treatment. The developed smart outpatient operation system is employed to balance physicians’ workload, prevent both underutilisation (“windows”) and overcrowding (“full”) and establish an effective management mechanism.
Publicity efforts are conducted through multiple channels to encourage patients to book appointments in different periods. Increased placement of appointment guidelines within the clinic, combined with active promotion by medical staff, helps amplify outreach and supports the continued implementation of tiered diagnosis and treatment.
Pre-examination and medical guidance personnel proactively direct each patient in an orderly manner, maintaining a quiet clinical environment. They monitor the waiting area dynamics and actively remind patients of relevant procedures, such as check-in, queueing systems and follow-up steps.
Medical and technical departments adopt flexible scheduling and increase examination capacity based on patient volume. The laboratory department has expanded the blood collection area and utilises adaptive shift arrangements to shorten patient waiting times. Additionally, test appointment times and preparatory instructions are communicated via text message to the patient’s mobile phone.
Improving the Quality of Medical Services
Efforts have been made to strengthen the use of standardised, courteous language at service counters and to enhance the overall quality of window services, working collectively to foster an orderly treatment environment. Guided by the “one visit at most” principle, staff at the registration counters provide direct, face-to-face assistance to patients. The medicine dispensing window follows a standardised operational process to ensure accurate distribution of medications, with clear communication to patients regarding usage. For special medications, additional explanations are provided to ensure full patient understanding.
Outpatient medical staff adhere to the “one patient per clinic” rule to protect patient privacy. Pre-examination nurses utilise patients’ waiting time to offer guided instruction and facilitate medical appointments. In addition, health education lectures are conducted twice weekly in the waiting area, covering the prevention, treatment and management of common and frequently occurring diseases.
Deepening Service Convenience
A one-stop comprehensive service centre has been established, staffed with full-time nursing personnel, to provide over 30 types of assistance, including medical inquiries, processing of two-way referrals, printing of outpatient and external prescriptions, review and stamping of medical certificates, convenience services, receipt and delivery of test reports, wheelchair rental, handling of outpatient complaints, and lost and found services. To alleviate parking shortages, the hospital is maximising the availability of parking spaces. Staff are instructed not to occupy parking areas, thereby freeing up above-ground parking resources and improving spatial efficiency. The promotion of time-slot appointments is actively encouraged to reduce patients’ time in the hospital and increase parking turnover. Patients are encouraged to use green transportation options. Information regarding subway and bus routes is communicated through WeChat messages, video displays in waiting areas and other channels to facilitate easy access to the hospital.
Quality Control
The outpatient satisfaction survey was administered and collected by staff from a third-party evaluation agency. All agency personnel received training prior to the survey to ensure data quality. A standardised script was used to explain the purpose, value and precautions of the survey to patients. For patients with visual impairments or those unable to write, the data collectors read each item aloud and recorded the responses on their behalf. To minimise psychological concerns and prevent potential bias resulting from the presence of healthcare personnel, medical staff were not present during the survey. Investigators maintained original records onsite, checked for completeness and collected questionnaires immediately to ensure a high response and recovery rate.
Data Analysis
EpiData version 3.0 (EpiData Association, Odense, Denmark) was used for data entry and validation to ensure data accuracy. Statistical analysis was performed using SPSS version 21.0 (IBM, Armonk, NY, USA). Categorical data are presented as numbers and percentages, and intergroup comparisons were conducted using the chi-square test. Continuous data are expressed as the mean ± standard deviation, and the t-test was applied for comparisons between and within groups. To account for multiple comparisons, the Bonferroni method was used during intergroup analyses to reduce type I errors, and P < 0.05 was considered statistically significant.
Results
Comparison of General Patient Information Before and After the Process Transformation
A total of 600 outpatients were included in both the pre- and post-transformation groups. There were no statistically significant differences in the general information, including age, gender, education level, occupation and medical insurance information, between the two groups (all P > 0.05), indicating that the two groups were comparable at baseline. The detailed data are presented in Table 2.
 |
Table 2 Comparison of General Patient Characteristics Before and After Process Transformation (N = 600 per Group) |
Comparison of Patient Satisfaction Scores Before and After the Process Transformation
Patient satisfaction scores were compared across multiple dimensions, including the medical environment, treatment process, medical services and evaluation feedback. The results demonstrated significant improvements in all satisfaction items after the process transformation (all P < 0.05). The specific scores (mean ± standard deviation) and statistical results are summarised in Table 3. Additionally, a visual comparison of satisfaction scores before and after the transformation is provided in Figure 1.
 |
Table 3 Comparison of Patient Satisfaction Scores Before and After New Public Service (NPS)-Guided Process Transformation (N = 600 per Group) |
 |
Figure 1 Comparison of patient satisfaction scores before and after New Public Service (NPS theory)-guided process transformation across key dimensions (N = 600 per group). Notes: Satisfaction scores were measured on a 5-point Likert scale (1 = Very dissatisfied to 5 = Very satisfied). Error bars represent standard deviations. All pre-post differences were statistically significant (P < 0.05, t-test). |
Discussion
The efficiency, quality and environment, among other aspects, of outpatient medical services directly reflect the overall medical level and comprehensive service capabilities of the hospital. When choosing a hospital, patients not only consider the hospital’s technical level but also pay great attention to the hospital’s service quality.10,11 The development of various outpatient workstreams is a key link in demonstrating the service quality and medical capabilities of tertiary hospitals.12,13 Our hospital’s outpatient management has implemented a number of measures to improve patient satisfaction with outpatient services.
Information Helps Outpatient Satisfaction: A Service-Oriented New Public Service Approach
Health informatization is a key strategy for hospitals to enhance and modernize their management practices.14 The Internet and information technology are continuously changing, with information technology no longer limited to data processing.15 Major hospitals have made innovations in the development of outpatient information, optimised the medical treatment process and service model with a patient-centred approach, shortened the waiting time for patient visits, improved the quality of outpatient services and achieved positive economic and social benefits.16,17 These improvements directly align with the NPS theory principle of being service oriented, shifting the focus from administrative control to enabling efficient and accessible service delivery. Hospital publicity in the new media era relates to the dissemination and interaction of information between hospitals, society and patients.18,19 To improve the satisfaction of outpatients, outpatient managers and the Information Department have worked together to transform the process based on patients’ opinions and suggestions and have introduced measures such as appointment registration, timed appointments for examinations, personalised payment plans, mobile phone payment, implementation of a medical insurance card and intelligent medical guidance to provide the patient with accurate medical treatment within minutes.20,21 This participatory design process, where patient feedback directly informs system changes, embodies the NPS theory emphasis on citizen participation and a responsive service. Patient satisfaction with the convenience of registration and outpatient service staff has improved considerably, but some problems still exist. For example, some patients did not make an appointment for medical treatment, elderly patients were accustomed to start queueing early and patients had to wait a long time at their first visit, which led to some patients still feeling that the waiting time for medical treatment was too long. In particular, the waiting time for ultrasound was excessive, and the listening score for ultrasound doctors indicated that they failed to communicate or listen.
In response to these problems, the hospital once again promoted appointment registration and timed medical treatment slots through WeChat official accounts and TV stations; outpatient managers communicated with multiple departments to ensure patients received treatment on time, improve compliance with appointment examinations, explore clinic space and flexible scheduling in ultrasound rooms and strengthen communication with elderly patients. These ongoing adjustments reflect a citizen-centred commitment to continuously adapt services to meet evolving patient needs, a core tenet of NPS theory. Additionally, the hospital uses SMS reminders to notify and guide patients through subsequent treatment steps, alongside offering convenient services such as online consultations and self-service booking, thereby enabling patients to independently schedule their examinations and tests. Patient satisfaction with the medical treatment process has improved considerably, but further improvements to the information system to improve the patient medical treatment experience and improve service levels is still the focus of follow-up work.
“One Visit at Most” Helps Outpatient Satisfaction: Embodying Citizen-Centred Values
Based on information development, this study further explores the impact of the concept of “one visit at most” on outpatient satisfaction. According to the “Action Plan for Deepening ‘One-time’ Reform in the Medical and Health Services Field in Zhejiang Province”, relevant measures must be conscientiously implemented, such as fewer queues for medical treatment, more convenient payment, less processes for examinations and more considerate service provision, so that patients can spend the shortest time possible in the hospital when seeing a doctor, they no longer have long detours on entering the hospital and they have a better medical experience.22 The core idea of reducing the patient burden aligns perfectly with the NPS theory goal of creating public value and prioritising citizen needs over bureaucratic efficiency. The hospital’s outpatient management has adopted the principle of “one visit at most” and introduced multiple patient-centred strategies. These include appointment-based registration (via phone, WeChat official accounts, in clinic, community referral and self-service kiosks) and self-service options to reduce waiting times. Additional measures such as self-service machines, password-free payment, facial recognition payment, QR code payment and instant settlement have been implemented to minimise repeated queueing. Clinic-appointed examinations help reduce unnecessary patient movement, whereas intelligent medical guidance and online report viewing contribute to continuous process optimisation. The appointment cancellation system has been improved to further standardise outpatient services. Multichannel patient education enhances public awareness of informed healthcare-seeking behavior, effectively increasing real-name registration and appointment rates while reducing waiting times and cancellation rates. Initiatives such as city-wide services for drugs covered under the Major Disease Insurance scheme (a supplementary public health insurance program), precision medicine and a first-consult responsibility system have been introduced. As a result, the overall patient satisfaction score increased from 8.66 ± 1.156 before process improvement to 9.12 ± 0.857 afterwards, a difference that was statistically significant. This holistic, patient-centric redesign demonstrates the NPS theory principle of serving citizens by fundamentally reengineering processes around their experience. Multiple physicians collaboratively conduct objective assessments of patients, negotiate treatment plans, enhance diagnostic and therapeutic efficiency, and improve medical service quality.23 The hospital has implemented a first-consultation responsibility system and established integrated outpatient services, multidisciplinary team clinics and specialised consultations for complex cases and multi-departmental joint clinics. Physicians in each clinic consider patient needs and strive to reduce unnecessary visits by enabling same-day settlement and follow-up appointment arrangements. As a result, patient satisfaction scores regarding respect within the diagnostic process increased from 4.43 ± 0.711 before the intervention to 4.69 ± 0.638 afterwards. The role of pre-examination nurses has evolved from simple inquiry to guided education. Utilising patients’ waiting time, these nurses now deliver instructional talks and promote the use of QR codes posted outside each clinic, which provide reminders covering processes such as secondary check-in, treatment procedures and the importance of individualised care. Patient satisfaction scores regarding respect for outpatient nurses improved from 4.55 ± 0.617 pre-intervention to 4.74 ± 0.525 post-intervention. Each service window actively assists patients under the “Youth Civilised Service Units” initiative at various levels, leading to a significant increase in patient satisfaction with window staff. Satisfaction scores related to medical quality also rose markedly, indicating strong patient approval of the hospital’s “one visit at most” initiative. The improvement in scores related to respect and communication underscores the success of applying NPS theory’s human-centred values, valuing the citizen–patient interaction as much as the clinical outcome. Outpatient management will better support outpatient clinics in the practice of “one visit at most” in the future, further improving patients’ medical experience and satisfaction.
Detailed Services Help Outpatient Satisfaction: Participatory and Value-Driven Care
In addition to increased information provision and “one visit at most”, detailed services are also key factors in improving patient satisfaction. Detail management is a new management method that divides a complete set of management processes into multiple management details, quantifies the management process step by step, completes each detail within a certain time and continuously quantifies and improves each detail, ultimately optimising the entire management process.24–26 Detailed services are integrated into outpatient management to create an atmosphere of caring for, respecting and helping outpatients. This meticulous attention to the patient journey reflects the NPS theory commitment to dignity and respect for citizens accessing public services. Outpatient managers and the Logistics Support Department provide patients with convenient services, such as shared wheelchairs, caring power banks, free rental of umbrellas and free breakfast for patients undergoing fasting tests. The hospital has established a comprehensive outpatient service centre. This centre is equipped with full-time personnel to provide medical consultation, a two-way referral, outpatient prescription printing, external prescription printing, medical certificate review and stamping, convenient services, test form delivery, wheelchair loan, outpatient complaint collection, and lost and found services. The establishment of this “one-stop” centre is a practical manifestation of the NPS theory service-oriented principle, designed for citizen convenience rather than administrative silos. The establishment of this centre has increased the patient satisfaction score for outpatient registration and the service window from 4.35 ± 0.723 before the transformation to 4.77 ± 0.524 after the transformation. The satisfaction score for service facilities, particularly regarding the medical environment, was the lowest among all categories. Parking facilities were the primary concern raised by patients, with a score of only 4.16 ± 0.971 prior to process restructuring. The reasons for this are as follows: 1) the hospital is located on an old campus in the city centre, where physical space for expansion is limited; 2) as a municipal-level comprehensive tertiary hospital, it attracts patients from districts and counties seeking higher-quality medical resources, many of whom commute by car. Within these spatial constraints, hospital management has taken measures to maximise parking availability, including prohibiting employees from occupying patient parking spots. Furthermore, the hospital continues to optimise parking resource use by developing above-ground parking areas and rationalising spatial allocation. Additional efforts include coordinating with Metro Line 2 to establish dedicated hospital access points and special medical channels. Patients are also encouraged to use green transportation options; subway and bus route information is disseminated through WeChat messages and videos in waiting areas. Following the implementation of these measures, the satisfaction score for parking facilities increased to 4.52 ± 0.772. The proactive and creative approach to solving the parking dilemma, despite spatial constraints, demonstrates a core NPS theory mindset: public servants should seek innovative solutions to serve citizens rather than citing constraints. Although there is still room for improvement in satisfaction scores, hospitals and outpatient managers continue to identify solutions with the goal of facilitating the process of seeking medical treatment.
Continuously enriching the concept of medical services based on patient needs can improve the hospital’s internal management level, enhance the hospital’s brand influence and continuously enhance the hospital’s core competitiveness in the fiercely competitive medical market.27 The implementation of outpatient business process transformation is based on NPS theory. The significant improvements in satisfaction scores across all dimensions provide strong empirical evidence for the value of applying NPS theory in healthcare settings. The findings demonstrate that its core principles – citizen centred, participatory and service oriented – effectively translate into tangible service quality improvements. The “patient-centred” value concept will gradually be reflected. The outpatient business process will provide patients with more scientific, standardised and convenient one-stop services so that patients can greatly improve the efficiency and quality of outpatient medical treatment. This study considerably improved patient satisfaction through specific measures such as optimising the appointment system and strengthening medical guidance. In addition, process transformation based on patient feedback can help hospitals understand patient needs and expectations in a timely manner, identify problems and shortcomings in the services provided and implement targeted improvement measures. This iterative feedback loop is a hallmark of the participatory governance model advocated by NPS theory. This study not only provides practical process transformation suggestions for hospital managers but also emphasises the key role of patient feedback in improving medical services, providing a useful reference, including for other medical institutions.
Broader Implications for Healthcare Management Practices
The findings from this study offer several actionable insights for healthcare management practices beyond our institutional context. First, our results demonstrate that systematic process transformation guided by a coherent theoretical framework – specifically, NPS theory – can produce substantial improvements in patient satisfaction. This suggests that healthcare managers should move beyond isolated quality improvement projects and instead embrace comprehensive, theory-driven reform approaches that simultaneously address multiple service dimensions (environment, process, service attitude and feedback mechanisms). In addition, our study provides a replicable model for implementing patient-centred care in practical terms. The specific interventions we implemented, such as optimising appointment systems, creating one-stop service centres, improving signage and training staff in communication skills, represent concrete strategies that can be adapted to various healthcare settings. Healthcare managers can prioritise similar evidence-based interventions that directly address common patient pain points, particularly those related to communication, waiting times and administrative burdens. Moreover, our findings highlight the importance of measuring and responding to patient feedback in a structured manner. The systematic collection and analysis of satisfaction data enabled us to identify specific areas for improvement and evaluate the effectiveness of our interventions. This suggests that healthcare organisations should invest in robust feedback systems that capture patient experiences in real time and facilitate continuous service improvement. Finally, our successful application of NPS theory principles demonstrates the value of importing management frameworks from other public sectors into healthcare. Healthcare managers might explore other governance and management theories from public administration that emphasise service quality, citizen engagement and continuous improvement, adapting them to the specific context of healthcare delivery.
Policy Implications and Generalisability of Findings
The substantial improvements in patient satisfaction demonstrated in this study have important implications for healthcare policy and management. The successful application of NPS theory in our outpatient process transformation offers a replicable model for other healthcare institutions seeking to enhance service quality. Specifically, our findings suggest that policymakers and hospital administrators should (1) prioritise patient-centred design in service delivery systems, moving beyond efficiency metrics to incorporate humanistic care values; (2) implement structured feedback mechanisms that enable genuine patient participation in service improvement, as advocated by NPS principles; and (3) allocate resources towards both technological solutions (eg informatisation) and human-centred interventions (eg staff training in communication and empathy).
The generalisability of our findings, however, requires careful consideration. Although the core principles of NPS theory are universally applicable, the specific implementation strategies may need adaptation to different healthcare contexts. The improvements observed in our study, such as the 0.46-point increase in overall satisfaction (from 8.66 to 9.12), were achieved within a tertiary hospital setting in China with specific organisational characteristics and resource availability. Other settings, such as community health centres or hospitals in different healthcare systems, might experience different magnitudes of effect or require modified approaches. Nevertheless, the theoretical framework of focusing reforms on citizen needs, the participatory design and service orientation remains broadly transferable.
Limitations and Future Research Directions
Despite the promising results, this study has several limitations that should be acknowledged. First, the reliance on self-reported satisfaction scores introduces the potential for social desirability bias, where patients might provide overly positive responses. Although we mitigated this by using third-party survey administrators and ensuring anonymity, future studies could incorporate more objective measures of service quality (eg time metrics, clinical outcomes) to triangulate findings. Second, the single-hospital setting limits the external validity of our findings. Although we demonstrated considerable improvements within our institution, the results may not be fully generalisable to hospitals with different sizes, funding structures or patient demographics. Multi-centre studies across diverse healthcare settings are needed to confirm the broader applicability of NPS theory-guided reforms. Third, the 6-month observation period post-transformation represents only short-term follow-up. Although this timeframe was sufficient to detect initial improvements, it remains unclear whether these gains will be sustained over the long term. The Hawthorne effect, where behaviour temporarily improves due to awareness of being studied, might have contributed to our results. Future research should include longer follow-up periods (eg 1–2 years) to assess the sustainability of satisfaction improvements and identify potential decay effects. Additional limitations include the focus on a specific regional context and the inability to fully account for all confounding variables that might influence patient satisfaction. Future studies should employ more robust designs, such as randomised controlled trials across multiple institutions, and explore the differential effectiveness of NPS theory-based interventions across various patient subgroups (eg by age, socioeconomic status or medical condition).
Despite these limitations, our study provides compelling evidence for the value of NPS theory in guiding outpatient process reform. The consistent improvements across all satisfaction domains suggest that a principled approach focused on citizenship, participation and service can effectively enhance the healthcare experience. Future efforts should build on this foundation to develop more nuanced implementation frameworks and evaluate their long-term impact on both patient satisfaction and clinical outcomes.
Conclusion
The transformation of outpatient processes, designed and implemented under the guidance of NPS theory, was associated with significant improvements in patient satisfaction scores across all surveyed dimensions, including the medical environment, treatment procedures, service quality, respect for patients, privacy protection, responsiveness to complaints and overall evaluation. This quasi-experimental study suggests that the application of NPS theory principles, such as being citizen centred, participatory and service oriented, can be an effective approach to enhancing outpatient service quality and the patient experience. Based on our findings, we recommend that hospital managers and policymakers consider implementing a patient-centred process redesign informed by similar theoretical frameworks, establishing structured mechanisms for collecting and responding to real-time patient feedback to guide continuous improvement, investing in informatisation and smart systems to streamline patient flow and reduce waiting times, enhancing staff training in communication and empathy to align with humanistic care values and optimising resource allocation to address common patient pain points, such as parking limitations, through innovative and multi-faceted solutions. Future research should focus on evaluating the long-term sustainability of these improvements and assessing the generalisability of this approach across diverse healthcare settings through more robust, multi-centre study designs.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki.This study was conducted with approval from the Ethics Committee of First Affiliated Hospital of Ningbo University (ID: 2020-R259). Written informed consent was obtained from all participants.
Consent for Publication
The manuscript is not submitted for publication or consideration elsewhere.
Acknowledgments
No funding or sponsorship was received for this study or publication of this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any funding support.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Flagg AJ. The role of patient-centered care in nursing. Nurs Clin North Am. 2015;50(1):75–86.
2. Davidson KW, Shaffer J, Ye S, et al. Interventions to improve hospital patient satisfaction with healthcare providers and systems:a systematic review. BMJ Qual Saf. 2016;26(7):596–606. doi:10.1136/bmjqs-2015-004758
3. Expert group on technical specifications for the evaluation of emergency patients in public hospitals. Expert consensus on technical specifications for the evaluation of emergency patients in public hospitals. Chin J Emerg Med. 2023;32(9):1158–1162.
4. Lowe D, Ryan R, Schonfeld L, et al. Effects of consumers and health providers working in partnership on health services planning, delivery and evaluation. Cochrane Database Syst Rev. 2021;9(9):CD013373. doi:10.1002/14651858.CD013373.pub2
5. Xiong J, Yang S, Xu P, et al. Analysis of pain points of hospital outpatient services based on online patient reviews. Chinese J Hospital Manag. 2021;37(4):317–321.
6. Davidson SRE, Haskins R, Ingham B, et al. Service redesign for outpatient services: strategies to improve the wait. Public Health. 2025;242:214–219. doi:10.1016/j.puhe.2025.03.011
7. Yang H, Chen J, Pan Y, et al. Application and practice of lean management in the transformation of outpatient inspection process of large hospitals. China Hospital Manage. 2010;30(07):27–28.
8. Kim CS, Spahlinger DA, Kin JM, Coffey RJ, Billi JE. Implementation of lean thinking: one health system’s journey. Jt Comm J Qual Patient Saf. 2009;35(8):406–413. doi:10.1016/s1553-7250(09)35057-6
9. Zheng P, Xie H, Ma J, et al. Application and research of outpatient information system in the analysis of the cause of withdrawal. Chinese Hospital. 2019;23(11):68–70.
10. Chen S, Wang Y, Yang Z, et al. Practice and effect of applying lean management to optimize outpatient procedures. Chinese J Hospital Manag. 2013;29(6):430–432.
11. Papp C, Harsanyi S, Gesztelyi R, Emri M, Zsuga J. Assessment of patient flow and optimized use of lean thinking transformation from the perspective of graph theory and spectral graph theory: a case study. Technol Health Care. 2021;29(2):199–211. doi:10.3233/THC-191782
12. Bai J, Liu J, Shi W, et al. Application of PDCA cycle management in outpatient management of tertiary hospitals. J Hospital Manage People’s Liberation Army. 2018;25(7):644–646.
13. Zhao J, Liu X, Gu G, Gu H, Yan Y, Li M. Application of the cycle management model in improving outpatient appointment services. Inquiry. 2022;59:46958022108140.
14. Ma J, Yan R, Tong Z, et al. System architecture and practice based on Internet + assisted tiered diagnosis and treatment. China Digital Med. 2017;12(7):48–50.
15. Mi Y, Zhao Y, Li W, et al. A preliminary study on real-time monitoring management of outpatient clinics based on the concept of “managing cockpits”. China Hospital Manage. 2019;23(8):5–7.
16. Wu H, Li J, Zhang H. Design and implementation of two-way referral service model based on tiered diagnosis and treatment. China Digital Med. 2018;13(6):16–18.
17. Wen X, Song Q, OuYang S, Yao Z, Luo Y. Novel use of structural equation modeling to examine the development of a framework of patient-centered two-way referral systems for building digital subjective well-being healthcare: a cross-sectional survey in Central China. Digit Health. 2024;10:20552076241253079. doi:10.1177/20552076241253079
18. Yang HL, Luan XR, Zhao LL, Wang JW, Chen YY. Design and application of health education apps based on wechat for self-management among patients. Iran J Public Health. 2022;51(5):1020–1029. doi:10.18502/ijph.v51i5.9417
19. Huang X, Wang Y, Yang X, Jiang R, Liu Y, Wang H. Patient-centric mobile medical services accessed through smartphones in the top 100 Chinese public hospitals: cross-sectional survey study. JMIR Form Res. 2024;8:e45763. doi:10.2196/45763
20. Song T, Zhang N, Chen M. The application effect of quality control circle in improving the satisfaction of patients visiting the multidisciplinary joint outpatient department nursing. 2024;13(2):181–185.
21. Chu Z, Li N, Yue M, et al. Optimization and thoughts on outpatient process under the background of “internet + healthcare”. China Health Quality Manage. 2018;25(4):109–111.
22. Zheng P, Xie H, Ma J. The application effect of quality control circle in improving the satisfaction of patients visiting the multidisciplinary joint outpatient department. Chinese Hospital. 2019;23(8):72–74.
23. Yao Z, Liu D, Zhang Y, et al. Give full play to the role of advantageous disciplines in improving outpatient medical services. Chinese Hospital. 2017;21(5):67–69.
24. Shan N, Zhang Y, Wang J. Application of details management in pipeline nursing management in NICU premature babies. Qilu Nurs J. 2018;24(13):46–48.
25. Newborn Brain Society Guidelines and Publications Committee, Molloy EJ, El-Dib M, Soul J, et al. Neuroprotective therapies in the NICU in preterm infants: present and future (neonatal neurocritical care series). Pediatr Res. 2024;95(5):1224–1236. doi:10.1038/s41390-023-02895-6
26. Wu J, Han Y, Lu L, et al. Comprehensively optimize outpatient management and continuously improve medical services. China Hospital. 2016;20(4):6–8.
27. Jin Y. Research on the impact of detail management on doctor-patient relationship in outpatient nursing work of children’s hospitalschinese science and technology journal database (full-text version. Med Health. 2023.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.