Back to Journals » Integrated Pharmacy Research and Practice » Volume 12
Outcomes of Pharmacist-Led Pharmaceutical Care Interventions Within Community Pharmacies: Narrative Review
Authors Eldooma I ![]() , Maatoug M, Yousif M
, Maatoug M, Yousif M
Received 12 February 2023
Accepted for publication 1 May 2023
Published 15 May 2023 Volume 2023:12 Pages 113—126
DOI https://doi.org/10.2147/IPRP.S408340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Ismaeil Eldooma,1,2 Maha Maatoug,2 Mirghani Yousif2
1Department of Planning, Research, and Information; National Health Insurance Fund, Wad-Medani, Sudan; 2Department of Clinical Pharmacy and Pharmacy Practice, University of Gezira, Wad-Medani, Sudan
Correspondence: Ismaeil Eldooma, National Health Insurance Fund, Department of Planning, Research, and Information, Wad-Medani, Sudan, Tel +249123162135, Email [email protected]
Abstract: Pharmaceutical care (PhC) services interventions led by pharmacists within community pharmacies (CPs) are essential in achieving optimal medication use outcomes. PhC is a concept related to medication use goals optimization through the reduction and prevention of drug-related problems (DRPs). This review paper summarized the literature on pharmacist-led PhC interventions within CPs. PubMed and Google Scholar publications were searched, identified, and summarized. Results showed that some studies handled community pharmacists’ roles, and some talked about PhC interventions. However, some studies reviewed the use of medicines, adherence, and follow-up, while other groups were on counseling, patient education, and health promotion. Pharmacists integrated some studies concerning diagnosis and disease screening into community pharmacy services. Besides these studies, there were studies on system design and installation of PhC service models. Most of the identified research results showed pharmacist-led intervention benefits for patients. These benefits include reduced DRPs, clinical, economical, humane, education and knowledge, disease prevention and immunization, identification of practice process problems, and the need for current practice redesigning. In conclusion, pharmacists can help patients achieve optimal outcomes through pharmacist-led interventions. Despite mentioned results, We recommend researching comprehensively applied PhC services provision models within CPs for more pharmacists-led interventions and role activation.
Keywords: pharmaceutical care, pharmacist-led interventions, community pharmacies, narrative, outcomes
Introduction
Background
Pharmacist-led pharmaceutical care (PhC) services interventions within community pharmacies (CPs) are vital in achieving optimal clinical, economic, and humanistic outcomes of medication use.1,2 PhC emerged as a new philosophy of Pharmacy Practice (PP). This new philosophy aims to provide patients with a social pharmacy role by reducing and preventing drug-related problems (DRPs), thus achieving optimal outcomes. After Helper and Strand introduced the new concept of PP in the 1990s, pharmaceutical services began to evolve towards focusing on patients rather than pharmaceutical products (patient-centered). The first definition of the PhC concept discussed the provision of medicines to achieve specific outcomes, which reflect obtaining patients’ desired quality of life.3 However, European countries introduced the PhC concept to optimize medication use outcomes.4 Both resources mentioned the outcomes of the new pharmacy role as the primary objective.
After introducing the PhC concept into an actual PP, initiatives continued emerging. Pharmacists worldwide undertook the new pharmacy philosophy as a vital goal in the pharmacy practice profession in developed countries.5–8 Pharmacists conducted many interventional studies concerning PhC services; however, interventions within CPs could be considered valuable. These interventions have been shown to improve adherence and disease control, clinical outcomes in many chronic diseases, pregnant women’s health, tobacco and smoking cessation, disease identification through screening, and health-related quality of life of the patients through good education, counseling, and knowledge dissemination.9–16 Nevertheless, according to our knowledge, little was known about pharmacist-led interventions within CPs’ addressing comprehensive PhC services provision. Interventions conducted by pharmacists were clinical and counseling activities, services, education, training, and system structure design within CPs.
The Role of Community Pharmacists Towards Pharmaceutical Care Services
Community pharmacists’ interventions to provide education, training, and medication management can help people benefit from the new community pharmacy practice models through PhC services provision. Traditionally, CPs are often known as retail pharmacies or retail drug outlets in which medicines are stored, dispensed, supplied, or sold to pharmacy encounters (patients and co-patients).17,18 CPs are considered the most easily accessed healthcare facilities for society individuals since the pharmacist does not recommend the previous appointment to meet care seekers.19,20 However, in this century, CPs evolved to have new roles due to the spread of the PhC concept into the PP domain.21 Many articles showed the newly evolved roles of community pharmacists in the context of PhC services. These roles can be summarized as expanding access to care to improve patient outcomes, reproductive health services, mental health, oral healthcare services, chronic diabetic management, immunization, and weight management.22–28 Despite the evolving roles, outcomes of PhC services provision within CPs varied between countries regarding models adopted.
This review briefly explored the outcomes of pharmacist-led interventions and provided care to patients within CPs in the scope of PhC services. Moreover, this article reviewed and summarized the results of the implemented PhC intervention programs, PP activities, and services or care provided. Specifically, we explored outcomes of pharmacist-led PhC services provision within the CPs rather than in hospitals or clinics since this is essential and represents the first step towards professional services provision. Regarding previous initiatives, many kinds of care provided in the PhC context within CPs as advanced pharmacists’ roles illustrated the new PP philosophy (pharmaceutical care) (Table 1).
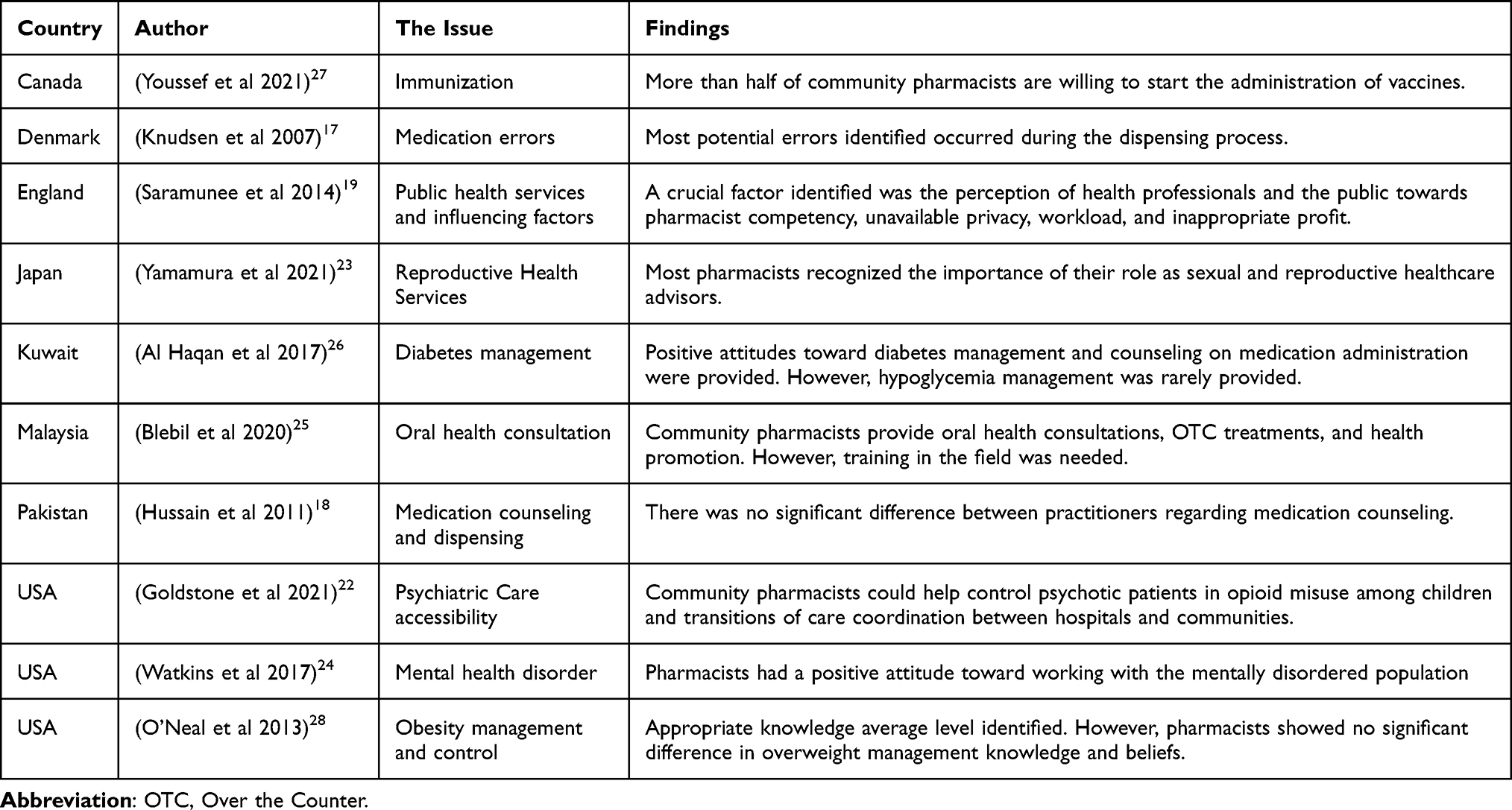 |
Table 1 The Role of Community Pharmacists Toward Pharmaceutical Care Services |
Methods
We searched semi-systematically through the PubMed and Google Scholar electronic databases and summarized the literature on outcomes of pharmacist-led PhC interventions within CPs. Results were limited to the period between 1996 to 2022. The search words for each database included: “pharmacist-led”, “outcomes or impact”, “pharmaceutical care”, “community pharmacy or pharmacies”, “interventions”, and “pharmacist.” References from identified journal articles, documents, and books formed the relevant information in this paper. We included studies that assessed the pharmacists-led interventions and the outcomes achieved (clinical, economical, humanistic, educational, knowledge, medication review, counseling, follow-ups, and health promotion). All services included must be in the context of PhC services within CPs and pharmacist-led scope only (inclusion criteria).
Results and Discussion
Pharmaceutical Care Interventions Within Community Pharmacies
In the past centuries, the roles of community pharmacists were limited to compounding and pharmaceutical product provision.29 However, in the late years, the position of a community pharmacist in the healthcare system has evolved and changed substantially.30 Pharmacists took on several roles that emerged from the PhC concept as a pharmacy practice philosophy. Pharmacists can provide PhC services within various pharmacy settings, but in this paper, we explored the published literature concerning the service provided by CPs. The roles and activities of community pharmacists in delivering PhC services, regarding the explored published literature, were multiple and diverse. The pharmacist-led PhC services interventions are executed activities and roles in the context of PhC services to optimize patient care. PhC services involve patient-centered, pharmacist-led activities and interventions to improve medicines management to achieve determined outcomes that can improve patients’ quality of life.8 Pharmacists conducted PhC service within the CPs in the past years after the new PP philosophy emerged in the 90th. The PhC services within CPs included medication reviews, adherence improvement, follow-ups, counseling, assessment, and screening of diseases, referring to hospitals or clinics, health promotion and education, immunization, and even diagnostic measures of some specific conditions.29
Medication Review, Adherence, and Follow-Up
A medication review (MR) is the complete check of the prescribed medicines used by a specific patient. The purpose is to identify any DRP that may require urgent intervention.31 The Pharmaceutical Care Network Europe (PCNE) stated the most popular definition of MR;
Medication review is a structured evaluation of a patient’s medicines to optimize medicines use and improve health outcomes, and this entails detecting drug-related problems and recommending interventions.32
According to this definition, MR as a pharmacist-led intervention could optimize medication use outcomes. Many studies in the published literature showed pharmacist-led medication reviews and interventions conducted in the context of PhC services within CPs worldwide. However, MR requires follow-up integration to evaluate the outcomes of the patient-provided interventions. The pharmacists should offer coaching and technical follow-up for these patients (Table 2).33 The purpose of follow-up is to document all results and activities integrated into the evaluation or review of medication use of the provided service.
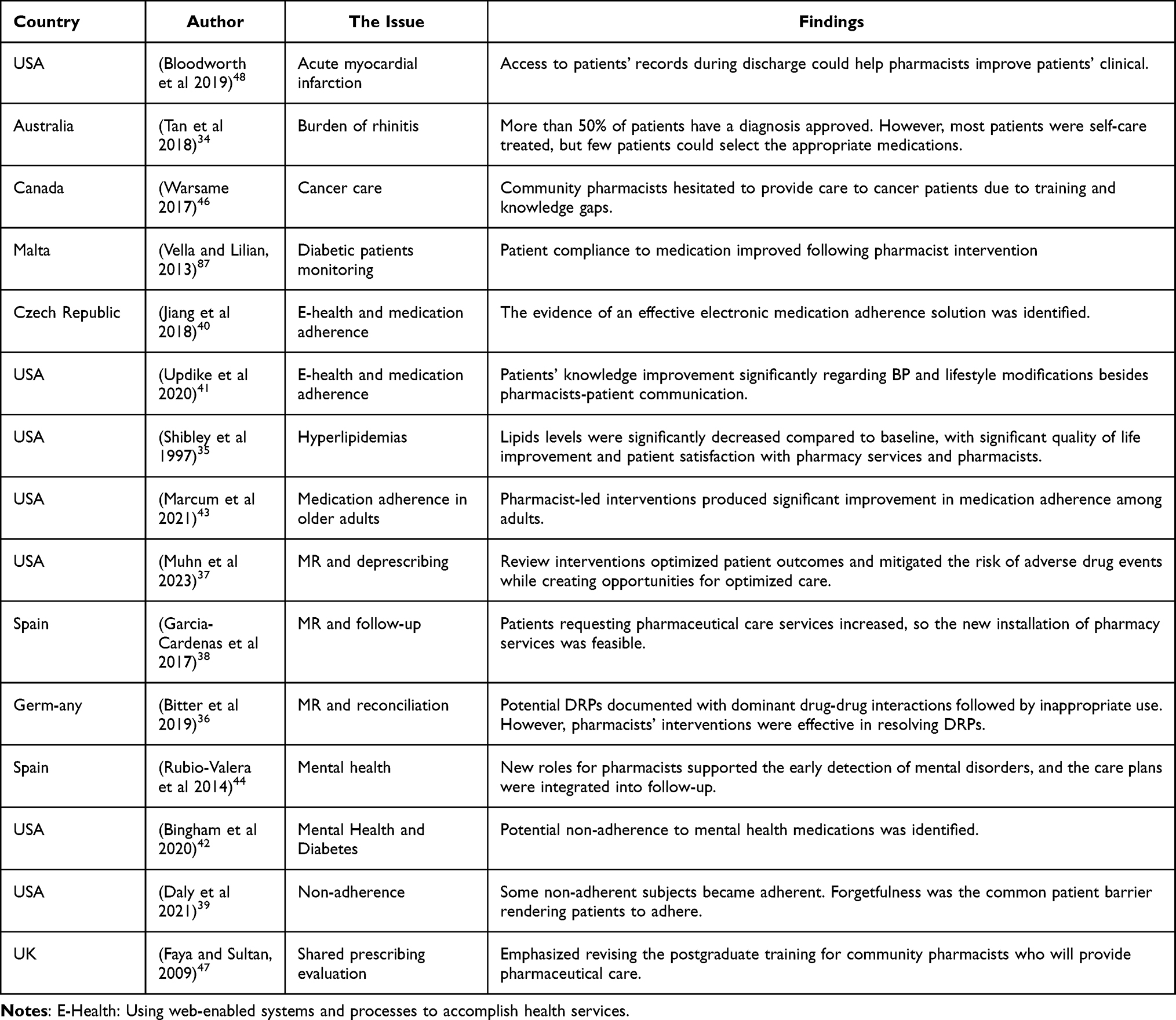 |
Table 2 Findings Summary of Medication Review, Adherence, and Follow-Up Interventions |
Community pharmacists have conducted studies concerning MR and follow-ups in the context of PhC services in Germany, Spain, and Belgium. Most of these Studies assessed the pharmacist-led interventions on clinical outcomes concerning MR and follow-up for patients. Conducted studies aimed at reviewing chronic or acute medication supported with follow-up activities. The MR purposes of most conducted studies were to optimize medication use, improve the quality of life for patients and identify any DRPs to achieve the required outcomes. These studies illustrated that pharmacists could contribute to managing chronic illnesses such as rhinitis, hypertension, diabetes, and hyperlipidemia through medication reviews and follow-up interventions.34–37 It is evident that pharmacist-led interventions concerning MR and follow-up are effective in chronic medication use and outcomes optimization. Also, in some MR studies, pharmacists have investigated adherence and compliance with medication use instructions and dose regimens.38–41 Pharmacists also conducted adherence assessments to the medication regimen and interventions regarding mental health.42,43 Towards mental health, community pharmacists’ interventions were summarized in a narrative review by Rubio-Valera et al in Spain. The author mentioned that community pharmacist was a part of the healthcare team to deal with mental health problems and shared in decision making, screened risk assessment of mental health, improved quality medicines use, reviewed medication use, and improved adherence with reduction of antipsychotic poly-pharmacy.44 A single study identified by Bingham et al, USA, addressed pharmacist-led interventions on psychotropic medication adherence in patients with diabetes. This study revealed that community pharmacist-led interventions significantly improved adherence to psychotropic medications. A meta-analysis review article by Zachary et al, USA, addressed pharmacist-led interventions to improve adherence in older patients. The authors concluded that there was a significant improvement in medication adherence among geriatrics receiving pharmacist-led interventions, which Medicare (Insurance system) payments can support (Table 2).
One study by Vella and Azzopardi (2013) in Malta illustrated the pharmacist-led intervention’s effectiveness in monitoring diabetic patients blood glucose control. The researcher observed and compared the patient’s compliance with medication and blood glucose self-monitoring and evaluated the efficacy of patients’ therapeutic plans. The pharmacist interventions included educating and distributing a Diabetes Patient published Information Leaflets (DPIL). The conclusion was that pharmacist-led MR and follow-ups could improve medication therapy use and control of blood glucose bio-markers.45 The second study found in the literature was conducted in Canada by Warsame (2017) as a pharmacy student’s perspective case study paper concerning the primary care of cancer patients at the CP. This study emphasized that pharmacists in the community have duties as primary care providers to provide comprehensive PhC services to cancer patients. The author recommended that follow-up be necessary for assessing common toxicities and providing recommendations within CPs or referrals. This study illustrated the feasibility of this program implementation within CPs in the context of PhC services.46 A third study was conducted in the UK by Faya (2009) concerning older people’s prescription follow-up and executing the required pharmacist-led interventions to avoid and reduce DRPs. This study concluded that community pharmacists could become general practitioners in advancing practice in the specialist clinical area of older people.47 A unique study conducted in the US by Bloodworth et al discussed the pharmacist linkage in care transitions between hospitals and the community. The study revealed that pharmacists’ access to hospital records could positively affect medication use outcomes for patients discharged from hospitals through MR and management.48 Regarding this published literature,
pharmacist-led interventions in the context of MR and patient follow-up could improve medication use and outcomes optimization, especially for older people and chronic medication users. The medication review integrated into follow-up requires effective counseling to achieve desired outcomes. All these identified studies in MR were within chronic illness and specific ailments. There is an opportunity for comprehensive PhC services for many acute diseases that were not conducted yet (Table 2).
Counseling and Patient Education Within Community Pharmacies
Good counseling is essential to the PhC services provision since it influences patients’ perceptions and adherence behaviors. The purpose of counseling and patient education is to optimize medication use outcomes. Adequate counseling requires good communication and strong relationships with patients to provide the best care and knowledge. Through good counseling, pharmacists aim to cooperate with patients to identify essential information and motivate them towards medication adherence to achieve the desired outcomes.49 Counseling is usually related and integrated into patient education and information. Sometimes, some articles mentioned counseling as pharmacist-conducted patient education.50 (Table 3).
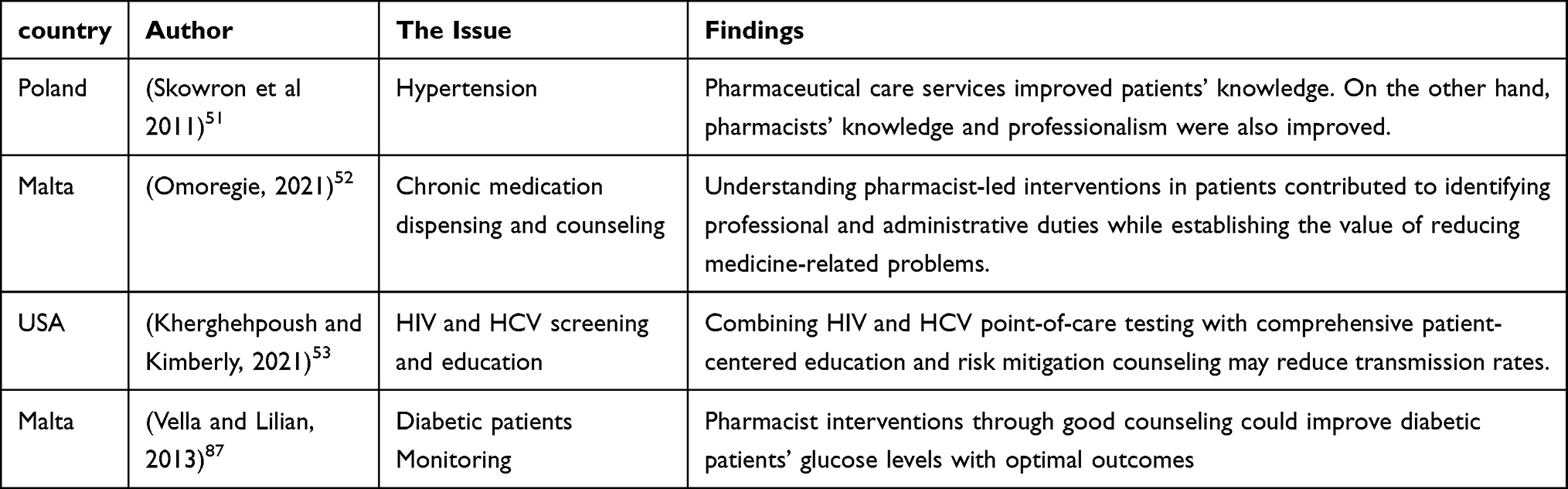 |
Table 3 Findings Summary of Community Pharmacies’ Counseling and Patient Education Services |
Practical interventions within CPs to achieve optimal medication use outcomes are good counseling, patient education, and advice within the context of the PhC philosophy. The literature contains many studies illustrating the significant outcomes of the PhC service provision with good counseling and patient education. For example, one study in Poland by Skowron et al assessed the impact of PhC education and good counseling services on patients with hypertension and their pharmacists. This study concluded that there were good outcomes for both patients and pharmacists represented in controlled patients’ blood pressure, pharmacist satisfaction (with pharmacotherapy and professional knowledge), and improved knowledge about hypertension for both.51 The study by Fayain (2009) in the UK aimed to assess the impact of pharmacist counseling intervention on diabetic patients’ compliance with medication and blood glucose self-monitoring. This study evaluated glycated hemoglobin (HbA1c) levels. The study revealed significant results and concluded that pharmacist-led MR and good counseling have vital outcomes in lower HbA1c levels and diabetic patients’ medication adherence more effectively to achieve optimal treatment benefits.45 Another study by Omoregie in Malta (2012) illustrated the importance of pharmacists’ good counseling and provision of blood glucose testing within CPs to identify new diabetic patients. During chronic medication dispensing at the CP, blood glucose testing can help patients to use their medicines more seriously. The outcome was good clinical benefits for blood glucose levels due to pharmacists’ motivation and well-informed patients towards pharmacy glycemia monitoring PhC services52 (Table 3).
A unique study in the context of pharmacist-led PhC services intervention concerning patient education and counseling was undertaken in a CP by Kherghehpoush and Keirnan (2021) in the US. The study linked patients’ education with laboratory screening of hepatitis C and immunodeficiency viruses (HCV and HIV). The pharmacist in this research coupled comprehensive education with viral transmission risk mitigation counseling. This study showed that participants complied with pharmacist-provided screening point-of-care services within a CP. This study concluded that comprehensive patient-centered PhC education and risk mitigation counseling might lower virus transmission rates among community individuals53 (Table 3).
Regarding these research-mentioned results regarding good counseling and patient education, pharmacists within CPs can conduct more comprehensive interventions in the context of PhC. Pharmacists can deliver professional pharmacy interventions through good counseling and effective patient education. Various medical conditions can be improved when pharmacist-led interventions convey good counseling and education of patients to improve awareness of their illness. Good counseling and effective patient education could make possible optimal outcomes from medicines. These outcomes are usually clinical, humanistic, or economic so that the overall benefit will appear in suitable patients’ quality of life. Good quality of life can be usual for patients when more expanded pharmacists’ roles are integrated into health promotion and preventive immunization.
Health Promotion and Immunization
CPs can play a vital role in health promotion, disease prevention, and immunization programs as advanced and expanded PhC services. Through collaboration with other healthcare providers, pharmacists can improve population health and increase immunization levels in developing countries where health systems still lack many medical providers.54 Pharmacist-led immunization interventions for better health were conducted for various vaccination programs. For example, in the USA, there are PhC services in HIV, and HCV viral diseases, older adults influenza vaccination, pharmacist authorization to administer vaccines, and pharmacists facilitating vaccination in older adults. Many studies and documents supported pharmacist-led immunization interventions in CPs to improve vaccination for most populations55–57 (Table 4).
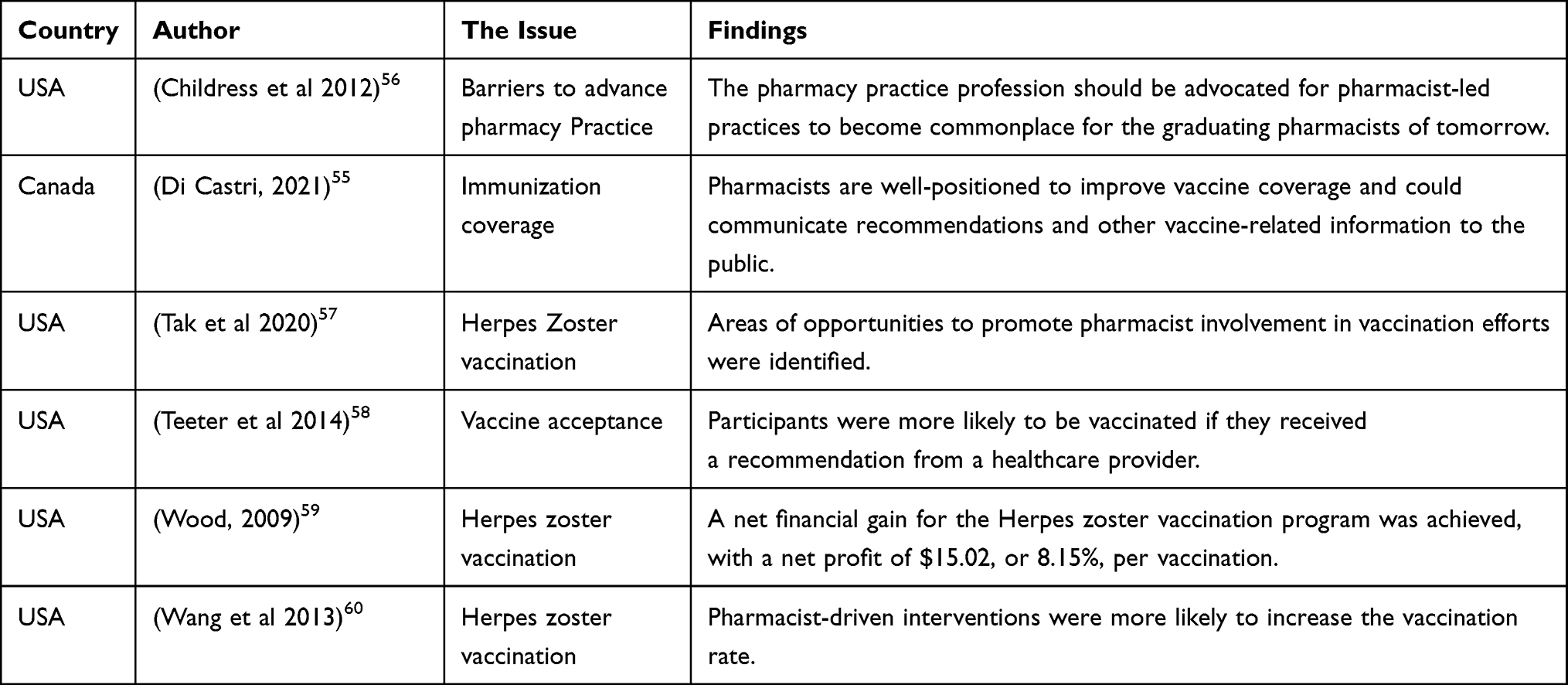 |
Table 4 Findings Summary of Health Promotion and Immunization |
Vaccination is a national priority in many developed countries. A critical study conducted by Childress et al in the USA assessed the essential role of pharmacists within CPs in facilitating vaccination and promoting health in older adults. Since older adults face many barriers to vaccination, the researcher identified that community pharmacists could overcome these barriers by offering convenient access points, building confidence in vaccination, and actively increasing awareness through health promotion programs within CPs. The study concluded that pharmacists who engage in vaccination and disease prevention could achieve better vaccination coverage and prevention of many microbial diseases.57 Similar studies addressed factors related to herpes zoster vaccination status and the extent of vaccine recommendation acceptance within community pharmacies, financial analysis of a herpes zoster immunization program from a community pharmacy perspective, and the effect of pharmacist intervention on herpes zoster immunization within community pharmacies58–60 (Table 4).
Patient Assessment, Disease Screening, Diagnosis, and Referring
PhC services provided by pharmacists within CPs require initial patient assessment, screening of DRPs, symptomatic diagnosis, and finally referring to other health care providers coupled with documentation as vital activity as stated in the PhC services cycle61–63 (Table 5).
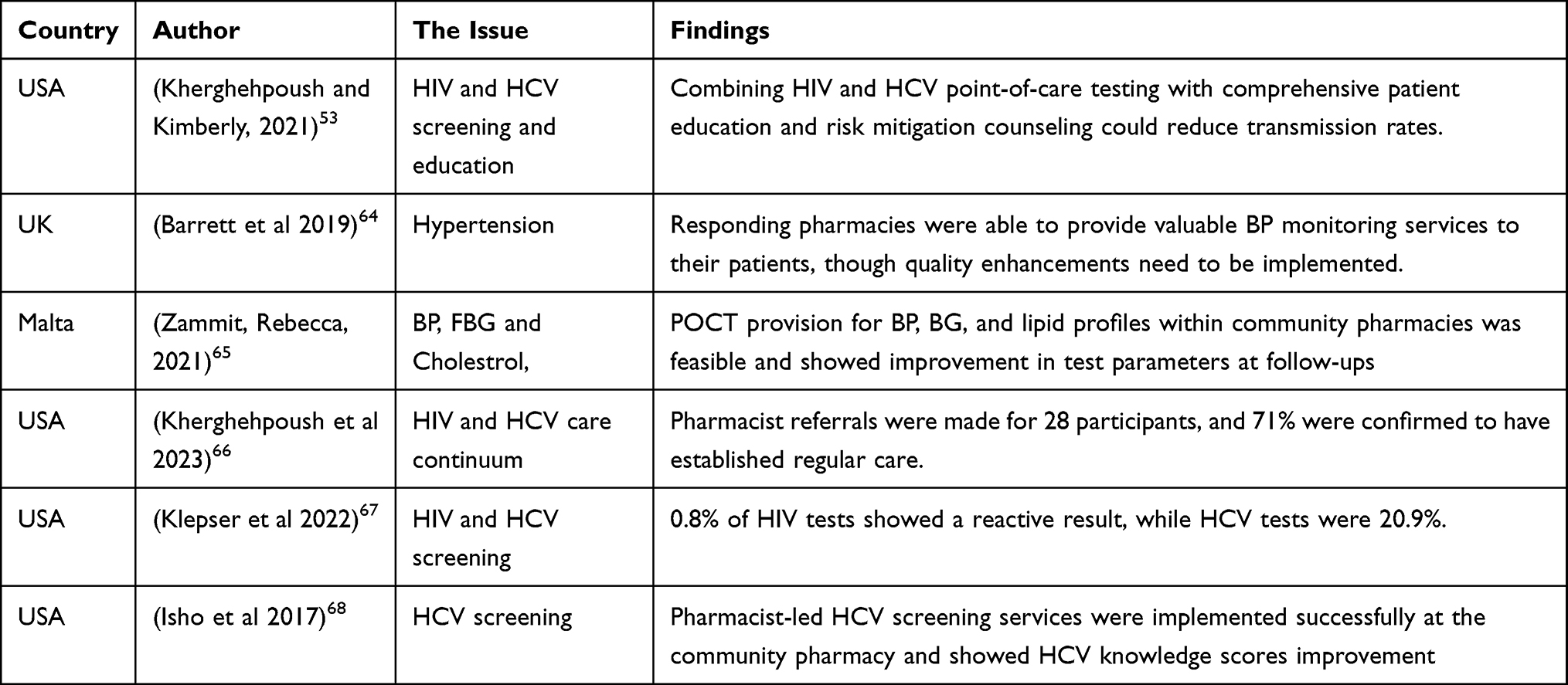 |
Table 5 Findings Summary of the Patient Assessment, Disease Screening, Diagnosis, and Referring |
Community pharmacists could contribute substantially to preventing, identifying, and managing high BP via routine assessment, public health promotion, and medicine optimization services as expanded and advanced PhC services.64 Many studies have been conducted concerning patient status assessment, disease screening, pre-diagnosis, and referring. A UK study by Barrett and Hodgkinson (2019) assessed the quality of digital blood pressure (BP) devices used to provide follow-up and hypertension screening services. Providing free BP checks to patients showed valuable service provision outcomes.64 Zammit conducted the second study (2021) in Australia, showing pharmacist-led interventions focusing on medication review services provided within a community pharmacy. The community pharmacy in this study was designed to be point-of-care testing (POCT). The POCT provided rapid testing for biomarkers within direct patient care services. This intervention facilitated disease diagnosis, monitoring, and management by the community pharmacist. The study concluded that significant positive outcomes were achieved. The service proved sustainable during the Coronavirus Pandemic Disease (COVID-19) when the healthcare system was not functioning at its standard capacity (Table 5).65 Another POCT study was conducted by Kherghehpoush and McKeirnan (2021) in the USA within a community pharmacy specializing in mental health services and serving people experiencing homelessness. The study assessed the health impacts of pharmacist-led HIV and HCV screening linked with education and risk mitigation counseling. This study concluded HIV and HCV POCT within CPs providing patient education and risk mitigation counseling may lower transmission, improve adherence care and encounters retention with these specialized pharmacies.53 Similar studies were conducted regarding the role of CPs in the HIV and HCV care, evaluation of pharmacy-based HCV and HIV screening program and pharmacist-initiated HCV screening within CPs to improve awareness linked to care at the medical center (Table 5).66–68 These results showed evidence of the feasibility of vital roles of community pharmacists in conducting PhC services within CPs regarding assessment, screening, and treatment of mild ailments, even in the absence of other healthcare providers. The influential roles of community pharmacists can be optimized when the traditional PP system and structure are redesigned to comply with these newly expanded roles.
System and Structure Redesigning Interventions
CP services differ between countries. After the evolution of PP and the emerging PhC services concept, the service provision varied from more specific services like MR to more complex services requiring interprofessional collaboration.69 However, PhC services require changing practices from traditional to evolved ones. The change requires redesigning the current practice systems and CP structure to comply with the new PP concept and roles.
There have been many studies concerning structural and transformational changes within CPs. These interventional studies are either operational, structural redesigning, or referring for resupply of medications. Pharmacist-led interventions for the CP system and structure designing are to improve safe over-the-counter medication, expand pharmacy roles for urgent care medication service models, electronically enhanced prescriptions, and create a medication safety culture.70–75 All systems and changing structural studies supported the PhC services providers within the CP. The most updated and vital study was titled “Structural and Operational Redesigning of Patient-centered Ambulatory Care Pharmacy Services and its Effectiveness during the COVID-19 Pandemic”.70 Thorakkattil et al conducted this study in Saudi Arabia aimed CP practice redesigning through pharmacist-led interventions in the context of PhC services. The author concluded that access to pharmacy services during the COVID-19 pandemic was executed through home medication delivery, remote area pickup locations, pharmacy call-center counseling, prescription refilling, and online pharmacy services. The intervention outcomes were influential in reducing physical contact and virus transmission between society and individuals (Table 6).
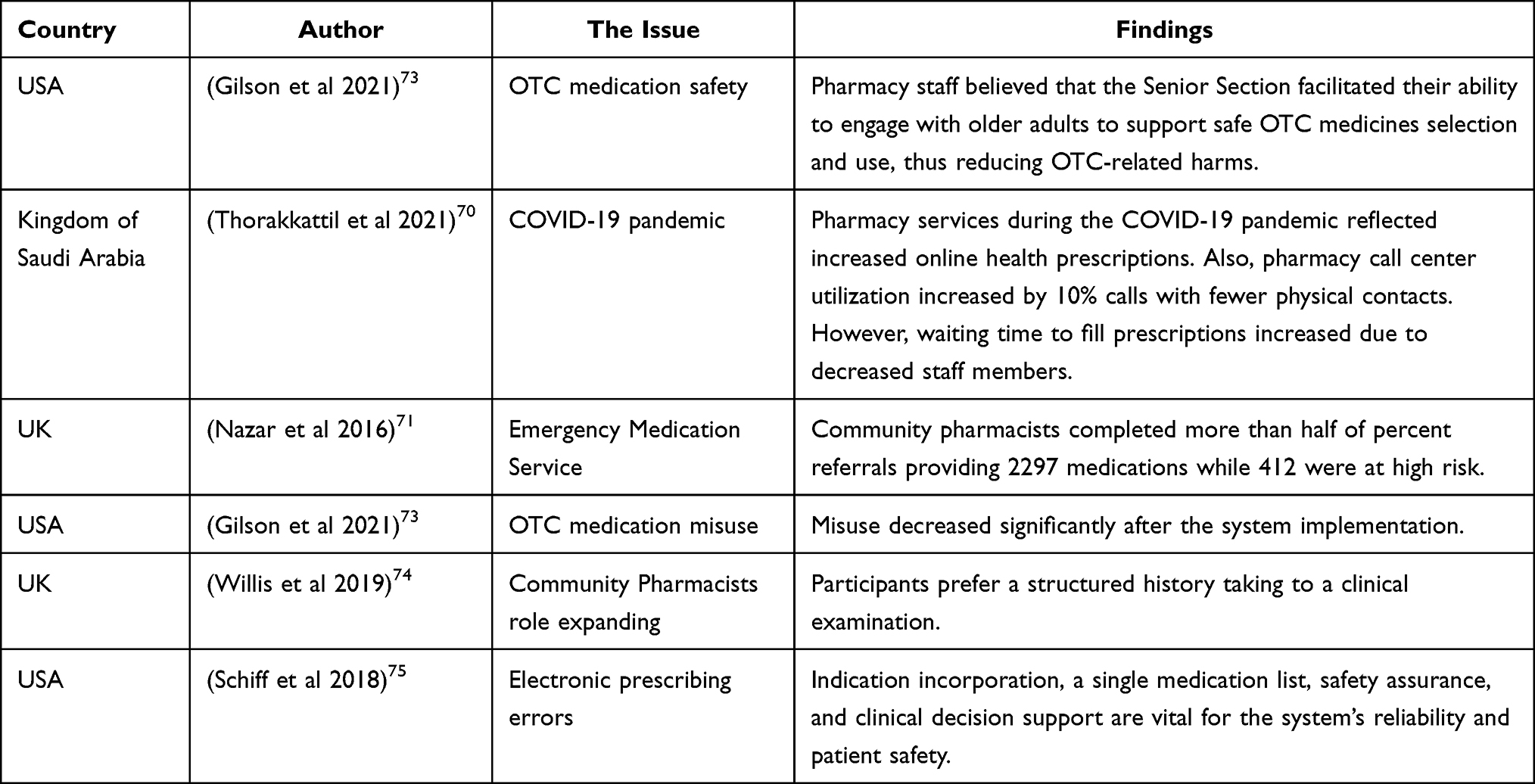 |
Table 6 Findings Summary of System and Structure Redesigning Interventions |
All efforts used to conduct studies concerning pharmacist-led interventions within CPs revealed effective outcomes and improved health benefits. However, many studies were published on the outcomes of pharmacist-led interventions in the context of PhC services within CPs.
Outcomes of Pharmacist-Led Pharmaceutical Care Interventions
Pharmacist-led intervention outcomes in the context of PhC services provision regarding the patient quality of life can be in the form of disease cure, elimination or reduction of symptoms, arresting and slowing of a disease prognosis, or disease prevention3. The patient care process steps illustrate the therapeutic relationship, assessment, identification of MRPs, and development of a care plan coupled with follow-up. Many studies evaluated the care process implementation of PhC services and the outcomes or benefits achieved. These outcomes were measured and stated in many published literature. A systematic review paper titled “community pharmacist-led interventions and their effects on patient medication adherence and other health outcomes” was conducted by Milosavljevic et al and published in the International Journal of Pharmacy Practice. The researcher concluded that community pharmacist-led interventions could significantly improve compliance and disease control. Future research should understand better which intervention component contributed substantially to improving adherence and health outcomes for patients with various medical conditions.9 Also, Newman et al conducted A second study, published in 2020; the study aimed to evaluate the effect of community pharmacist-led interventions on chronic disease management, clinical utilization, and economic outcomes. The study was an umbrella review paper designed; the conclusion was that community pharmacists could improve clinical outcomes in various chronic diseases, including diabetes, hyperlipidemia, HIV, and cardiovascular and respiratory diseases.10 Since many developed countries adopted it, results showed promising outcomes, improved quality of life, and patient satisfaction. These outcomes are within the domain of the health intervention outcomes regarding the PhC services and concept. The PhC services outcomes are either clinical, economic, or humanistic outcomes (ECHO).76
The identified studies of pharmacist-led PhC interventions and clinical outcomes in this review paper illustrated the investigation and evaluation of either cure of illness, symptoms elimination or reduction of, arresting or slowing of a disease prognosis, and prevention of diseases. Studies concerned with disease cure or symptom elimination and reduction identified were many. Reflections of the pharmacist-led interventions for chronic disease symptoms control and removal were conducted for hypertension, diabetes, hyperlipidemia, Asthma, and chronic or acute pain (systematic review paper).51,77 Also, studies for disease prevention have shown acceptable outcomes; for example, a Saudi Arabian study conducted by Thorakkattil et al, in which COVID-19 prevention within CP services provided during the pandemic was a vital outcome.70 (Table 7).
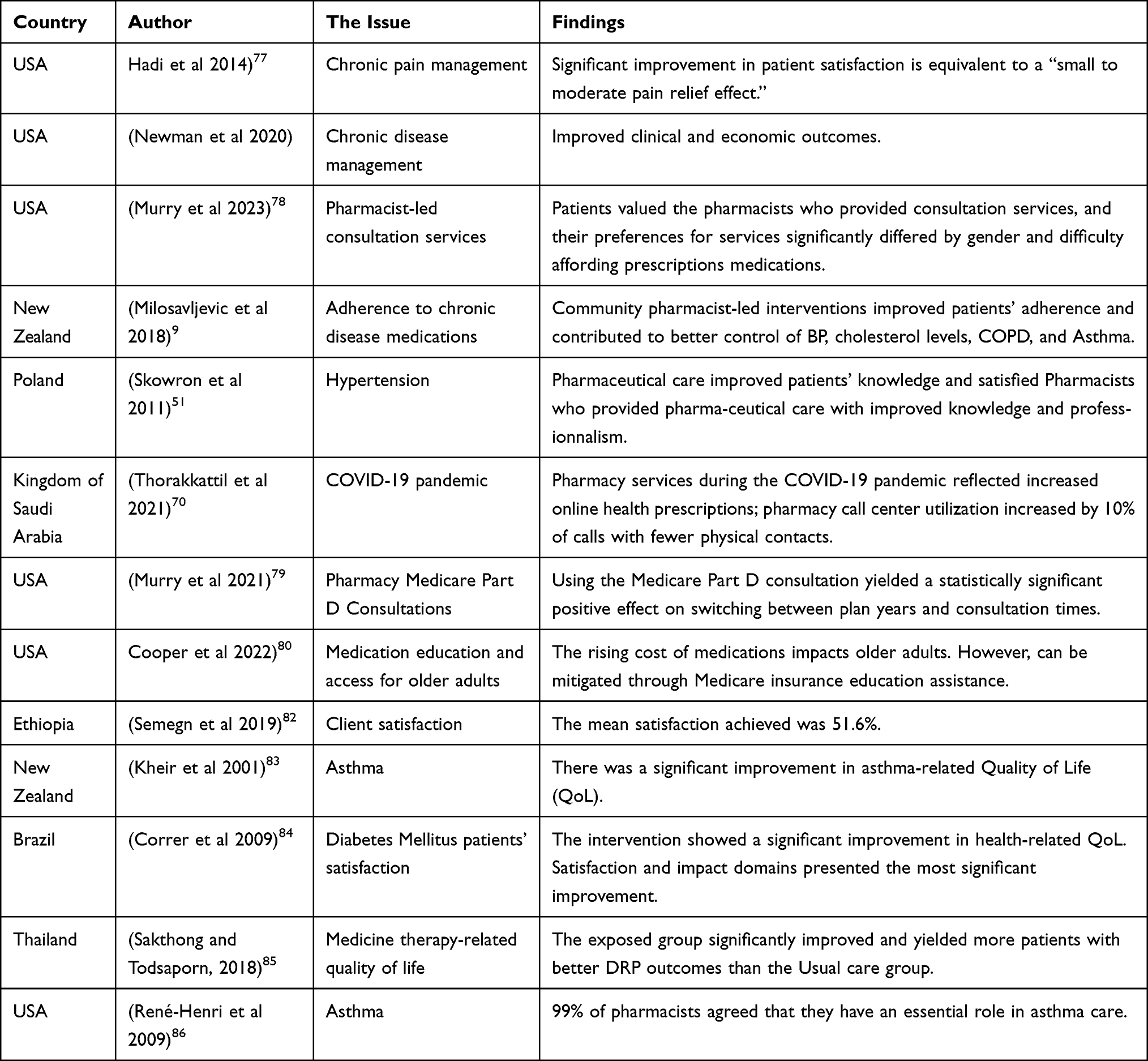 |
Table 7 Findings Summary for Outcomes of Pharmacist-Led Pharmaceutical Care Interventions |
The economic outcomes achieved from pharmacist-led interventions within CPs for chronic diseases were evaluated in 15 references that complied with inclusion criteria in systematic review research conducted by Newman et al. Pharmacists impacted the treatment outcomes of chronic ailments such as Asthma, Diabetes Mellitus, Chronic Obstructive Pulmonary disease (COPD), Heart failure, Hypertension, Hyperlipidemia, and HIV. Community pharmacist-led interventions are mostly executed through patient consultations and education. The specific economic outcomes reported were limited and primarily focused on pharmacy interventions in diabetes only. In some cases, a decrease in medical and healthcare costs in patients with diabetes was identified.10 The Medicare Part D (An insurance system in the USA for voluntary outpatient prescription drug benefits for people provided through a private contract with the government) consultation is one of the critical domains for pharmacist-led care interventions within community pharmacies in the USA.78–80 CPs for Medicare Part D provide free consultation services with MRs to improve adherence and appropriate and rational medication use at a reasonable cost. The pharmacist-led Medicare Part D consultation outcomes showed better plan-changing interventions and adherence to chronic medication utilization (Table 7).
Pharmacist-led PhC services interventions also achieved educational outcomes. These educational outcomes improved knowledge for students, pharmacists, and patients. Usually, patient education in the identified studies was conducted through written information document provision, such as printed leaflets or good counseling. However, pharmacists’ and pharmacy students’ education interventions were found to be through training programs.50,80,81 These educational interventions in pharmaceutical care were to achieve optimal patient health outcomes, in most cases, due to improved knowledge and adherence (Table 7).
One of the essential outcomes of pharmacist-led interventions in the PhC services context within CPs is to achieve excellent patient satisfaction when their quality of life improves since satisfied patients are most likely appropriate on their medication intake and comply with instructions they received. Also, clients’ satisfaction with CPs is important for PhC service provision and implementation.82 The need for a better quality of life is usually vital for those who have chronic diseases. Quality of life improvement for patients using regular medications was conducted in many previous studies, such as hypertension, diabetes, hyperlipidemia, chronic pain, and cancer. For example, some studies addressed pharmacist-led PhC Interventions within CPs for research purposes concerning patients’ quality of life, such as the impact of PhC programs on patients’ quality of life and satisfaction with the provided pharmacy services in patients with type 2 diabetes mellitus, the effects of PhC interventions in discovering and resolving of DRPs problems on the quality of life in a group of elderly patients. The pharmacists’ influence on asthmatic patients’ health-related quality of life was published as New Zealand PhC services experience.83–86 These studies illustrated the value of pharmacist-led interventions on the quality of life improvement for patients with acceptable satisfaction levels (Table 7).
Conclusion
The roles of community pharmacists in providing comprehensive PhC services are still evolving, especially in developed countries. Globally conducted studies concerning pharmacist-led PhC services interventions within CPs showed good benefits for patients, especially those with chronic diseases. Regarding developing countries, there is a need to improve pharmacists’ practice and knowledge regarding the PhC services philosophy. This review paper explored previously conducted studies in the context of PhC services within CPs regarding pharmacist-led interventions to reflect these interventions outcomes that can inform pharmacy professionals of the identified gaps that require further research.
Regarding the published literature, it is evident that pharmacist-led PhC interventions within community pharmacy settings are effective and could result in optimized medication use (objective PhC services), improving patients’ quality of life. By default, the most dominant pharmacist-led interventions identified were conducted on chronic medication use and illness; this may be due to the high burden of chronic diseases on people and pharmacists worldwide; on the other hand, this population is vulnerable and in need of comprehensive PhC services provision. So it is expected that in upcoming years there will be demands for more comprehensive pharmacist-led intervention service provision within community pharmacy settings, so studies that can help broaden and expand pharmacists’ roles will be strongly recommended. The expanding role of community pharmacists complies with the new PP philosophy. Many studies in this review conducted screening and testing studies in the context of expanded roles and showed positive outcomes. It is now the time to change the patient’s perception that pharmacists are just drug handlers to become professionals of trustworthiness and experts in medication.
The PP scope needs research covering the pharmacist-led interventions within the community pharmacy settings, which deal with all community pharmacy encounters in the context of comprehensive PhC services rather than a specific or narrow scope. Pharmacists must conduct research concerning complete and comprehensive PhC services provided through pharmacist-led interventions. After the pandemic of COVI-19, societies worldwide accessed pharmacists at CPs easily and received their medication and pharmaceutical care services. At the same time, most healthcare providers were unavailable, so pharmacists at CPs should raise their readiness to face health disasters in the future. Effective PhC services require further research to fill the gap between the conceptual frame and the current community pharmacy practice domains.
Abbreviations
PhC, Pharmaceutical Care; CPs, Community Pharmacies; DRPs, Drug Related Problems; PP, Pharmacy Practice; MR, Medication Review; HCV, Hepatitis C Virus; HBV, Hepatitis B Virus; HIV, Human Immunodeficiency Virus; POCT, Point of Care Testing; COVID-19, Corona Virus Disease; UK, United Kingdom; USA, United States of America.
Acknowledgment
Full appreciation to the Co-authors for their substantial contribution to this work concerning orientation, reviewing, corrections, and all the great scientific efforts they have provided.
Author Contributions
All authors contributed to this research work significantly, represented in the conceptualization, study design, execution, data collection, analysis, and interpretation of results. They also contributed to drafting, revising, and critically reviewing this article; gave the final approval of the revised version to be published; agreed on the journal submitted to; and agreed to be accountable for all aspects of this work.
Disclosure
All authors declared that they have no competing interests.
References
1. Adunlin G, Mahdavian S. The effectiveness of pharmacist interventions on asthma management: a systematic review. J Asthma Allergy Educ. 2012;3(6):264–273. doi:10.1177/2150129712464775
2. Apikoglu-Rabus S, Yesilyaprak G, Izzettin FV. Drug-related problems and pharmacist interventions in a cohort of patients with asthma and chronic obstructive pulmonary disease. Respir Med. 2016;120:109–115. doi:10.1016/j.rmed.2016.10.006
3. Helper C, Strand LJ. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533–543.
4. Abrahamsen B, Burghle AH, Rossing C. Pharmaceutical care services available in Danish community pharmacies. Int J Clin Pharm. 2020;42(2):315–320. doi:10.1007/s11096-020-00985-7
5. Jones EJ, MacKinnon NJ, Tsuyuki RT. Pharmaceutical care in community pharmacies: practice and research in Canada. Ann Pharmacother. 2005;39(9):1527–1533. doi:10.1345/aph.1E456
6. Westerlund LT, Björk HT. Pharmaceutical care in community pharmacies: practice and research in Sweden. Ann Pharmacother. 2006;40(6):1162–1169. doi:10.1345/aph.1G680
7. Eickhoff C, Schulz MJ. Pharmaceutical care in community pharmacies: practice and research in Germany. Ann Pharmacother. 2006;40(4):729–735. doi:10.1345/aph.1G458
8. Costa FA, Scullin C, Al‐Taani G, et al. Provision of pharmaceutical care by community pharmacists across E urope: is it developing and spreading? J Eval Clin Pract. 2017;23(6):1336–1347. doi:10.1111/jep.12783
9. Milosavljevic A, Aspden T, Harrison J. Community pharmacist-led interventions and their impact on patients’ medication adherence and other health outcomes: a systematic review. Int J Pharm Pract. 2018;26(5):387–397. doi:10.1111/ijpp.12462
10. Newman TV, San-Juan-Rodriguez A, Parekh N, et al. Impact of community pharmacist-led interventions in chronic disease management on clinical, utilization, and economic outcomes: an umbrella review. Res Social Adm Pharm. 2020;16(9):1155–1165. doi:10.1016/j.sapharm.2019.12.016
11. Ayogu EE, Yahaya RI, Isah A, Ubaka CM. Effectiveness of a pharmacist-led educational intervention on health outcomes in hypertension management at community pharmacies in Nigeria: a two-arm parallel single-blind randomized controlled trial. Br J Clin Pharmacol. 2023;89(2):649–659. doi:10.1111/bcp.15514
12. Al Aqeel S, Abanmy N, AlShaya H, Almeshari AJS. Interventions for improving pharmacist-led patient counselling in the community setting: a systematic review. Syst Rev. 2018;7(1):1–13.
13. Scott PA, Quotah OF, Dalrymple KV, et al. Community pharmacist-led interventions to improve preconception and pregnancy health: a systematic review. Pharmacy. 2021;9(4):171. doi:10.3390/pharmacy9040171
14. O’Reilly E, Frederick E, Palmer E. Models for pharmacist-delivered tobacco cessation services: a systematic review. J Am Pharm Assoc. 2019;59(5):742–752. doi:10.1016/j.japh.2019.05.022
15. Fuller JM, Wong KK, Krass I, Grunstein R, Saini B. Sleep disorders screening, sleep health awareness, and patient follow-up by community pharmacists in Australia. Patient Educ Couns. 2011;83(3):325–335. doi:10.1016/j.pec.2011.05.004
16. Shen X, Bachyrycz A, Anderson JR, Tinker D, Raisch DW. Quitting patterns and predictors of success among participants in a tobacco cessation program provided by pharmacists in New Mexico. J Manag Care Spec Pharm. 2014;20(6):579–587. doi:10.18553/jmcp.2014.20.6.579
17. Knudsen P, Herborg H, Mortensen A, Knudsen M, Hellebek AJBQ. Safety. Preventing medication errors in community pharmacy: frequency and seriousness of medication errors. BMJ Qual Saf. 2007;16(4):291–296. doi:10.1136/qshc.2006.018770
18. Hussain A, Ibrahim MI. Medication counselling and dispensing practices at community pharmacies: a comparative cross sectional study from Pakistan. Int J Clin Pharm. 2011;33(5):859–867. doi:10.1007/s11096-011-9554-6
19. Saramunee K, Krska J, Mackridge A, et al. How to enhance public health service utilization in community pharmacy?: general public and health providers’ perspectives. Res Social Adm Pharm. 2014;10(2):272–284. doi:10.1016/j.sapharm.2012.05.006
20. Kelling SE. Exploring accessibility of community pharmacy services. Inov Pharm. 2015;6(3). doi:10.24926/iip.v6i3.392
21. Dolovich L, Austin Z, Waite N, et al. Pharmacy in the 21st century: enhancing the impact of the profession of pharmacy on people’s lives in the context of health care trends, evidence and policies. Can Pharm J. 2019;152(1):45–53. doi:10.1177/1715163518815717
22. Goldstone LW, DiPaula BA, Werremeyer A, et al. The role of board-certified psychiatric pharmacists in expanding access to care and improving patient outcomes. Psychiatr Serv. 2021;72(7):794–801. doi:10.1176/appi.ps.202000066
23. Yamamura S, Terajima T, Navarrete J, et al. Reproductive health services: attitudes and practice of Japanese community pharmacists. Healthcare. 2021;9(10):1336. doi:10.3390/healthcare9101336
24. Watkins A, McKee J, Hughes C, Pfeiffenberger T. Community pharmacists’ attitudes toward providing care and services to patients with severe and persistent mental illness. J Am Pharm Assoc. 2017;57(3s):S217–S224.e212. doi:10.1016/j.japh.2017.02.020
25. Blebil A, Dujaili J, Elkalmi R, Tan HLK, Tai MS, Khan TM. Community pharmacist’s role in providing oral health-care services: findings from Malaysia. J Pharm Bioallied Sci. 2020;12(1):64–71. doi:10.4103/jpbs.JPBS_152_19
26. Al Haqan AA, Al-Taweel DM, Awad A, Wake DJ. Pharmacists’ attitudes and role in diabetes management in Kuwait. Med Princ Pract. 2017;26(3):273–279. doi:10.1159/000456088
27. Youssef D, Abou-Abbas L, Farhat S, Hassan H. Pharmacists as immunizers in Lebanon: a national survey of community pharmacists’ willingness and readiness to administer adult immunization. Hum Resour Health. 2021;19(1):131. doi:10.1186/s12960-021-00673-1
28. O’Neal KS, Crosby KM. Patients’ perceptions of a pharmacist-managed weight management clinic in a community setting. Res Social Adm Pharm. 2013;9(1):129–136. doi:10.1016/j.sapharm.2012.04.002
29. Bobbins AC, Burton S, Fogarty TL. Different models of pharmaceutical services and care in primary healthcare clinics in the Eastern Cape, South Africa: challenges and opportunities for pharmacy practice. Afr J Prim Health Care Fam Med. 2020;12(1):e1–e11. doi:10.4102/phcfm.v12i1.2323
30. Farris KB, Fernandez-Llimos F, Benrimoj SI. Pharmaceutical care in community pharmacies: practice and research from around the world. Ann Pharmacother. 2005;39:1539–1541. doi:10.1345/aph.1G049
31. Griese-Mammen N, Schulz M, Böni F, Hersberger KE. Medication review and medication reconciliation. In: Alves da Costa F, van Mil JWF, Alvarez-Risco A, editors. The Pharmacist Guide to Implementing Pharmaceutical Care. Cham: Springer International Publishing; 2019:69–87.
32. Griese-Mammen N, Hersberger KE, Messerli M, et al. PCNE definition of medication review: reaching agreement. Int J Clin Pharm. 2018;40(5):1199–1208. doi:10.1007/s11096-018-0696-7
33. Liekens S, Foulon V. Pharmaceutical care and the role of the patient. In: Alves da Costa F, van Mil JWF, Alvarez-Risco A, editors. The Pharmacist Guide to Implementing Pharmaceutical Care. Cham: Springer International Publishing; 2019:25–31.
34. Tan R, Cvetkovski B, Kritikos V, et al. The burden of rhinitis and the impact of medication management within the community pharmacy setting. J Allergy Clin Immunol. 2018;6(5):1717–1725. doi:10.1016/j.jaip.2018.01.028
35. Shibley MC, Pugh CB. Implementation of pharmaceutical care services for patients with hyperlipidemias by independent community pharmacy practitioners. Ann Pharmacother. 1997;31(6):713–719. doi:10.1177/106002809703100608
36. Bitter K, Pehe C, Krüger M, Heuer G, Quinke R, Jaehde U. Pharmacist-led medication reviews for geriatric residents in German long-term care facilities. BMC Geriatr. 2019;19(1):1–8. doi:10.1186/s12877-019-1052-z
37. Muhn S, Amin NS, Bardolia C, et al. Pharmacist’s comprehensive medication review in deprescribing chronic medications at the end of life. Arch Clin Med Case Rep. 2023;7(95–100). doi:10.26502/acmcr.96550580
38. Garcia-Cardenas V, Benrimoj SI, Ocampo CC, et al. Evaluation of the implementation process and outcomes of a professional pharmacy service in a community pharmacy setting. A case report. Res Social Adm Pharm. 2017;13(3):614–627. doi:10.1016/j.sapharm.2016.05.048
39. Daly CJ, Verrall K, Jacobs DM. Impact of community pharmacist interventions with managed care to improve medication adherence. J Pharm Pract. 2021;34(5):694–702. doi:10.1177/0897190019896505
40. Jiang C, Zhang H, Liu K, et al. A mobile health solution for medication adherence intervention and its real world evidence.
41. Updike WH, Pane O, Hanna K, Chevasco RM, Kelly WN, Sneed KB. Pharmacists interventions using Bluetooth technology and telehealth to improve blood pressure—A pilot study. J Am Pharm Assoc. 2020;60(4):e100–e108. doi:10.1016/j.japh.2020.01.008
42. Bingham J, Silva-Almodóvar A, Lee H, et al. Reprint of: the role of the pharmacist in mental health: an investigation of the impact of pharmacist-led interventions on psychotropic medication adherence in patients with diabetes. J Am Pharm Assoc. 2020;60(5):S78–S83. doi:10.1016/j.japh.2020.08.030
43. Marcum ZA, Jiang S, Bacci JL, Ruppar TM. Pharmacist-led interventions to improve medication adherence in older adults: a meta-analysis. J Am Geriatr Soc. 2021;69(11):3301–3311. doi:10.1111/jgs.17373
44. Rubio-Valera M, Chen TF, O’Reilly CL. New roles for pharmacists in community mental health care: a narrative review. Int J Environ Res Public Health. 2014;11(10):10967–10990. doi:10.3390/ijerph111010967
45. Vella J, Azzopardi LM. Pharmacist-led diabetic patient monitoring. J Euromed Pharm. 2013;3:21–24.
46. Warsame L. Primary care of cancer patients: a pharmacy student’s perspective. Can Pharm J. 2017;150(6):351. doi:10.1177/1715163517734237
47. Faya S. Pharmaceutical Care For Elderly Patients in Community Pharmacy: analysis and Evaluation of Community Pharmacist Interventions in the Randomised Evaluation of Shared Prescribing for Elderly People in the Community over Time (RESPECT) Study [PhD]: School of Pharmacy, University of Bradford; 2009.
48. Bloodworth LS, Malinowski SS, Lirette ST, Ross LA. Pharmacist linkage in care transitions: from academic medical center to community. J Am Pharm Assoc. 2019;59(6):896–904. doi:10.1016/j.japh.2019.08.011
49. Cavaco A. Pharmaceutical care and patient counseling. In: Alves da Costa F, van Mil JWF, Alvarez-Risco A, editors. The Pharmacist Guide to Implementing Pharmaceutical Care. Cham: Springer International Publishing; 2019:33–40.
50. American Society of Health-System P. ASHP guidelines on pharmacist-conducted patient education and counseling. Am J Health Syst Pharm. 1997;54(4):431–434. doi:10.1093/ajhp/54.4.431
51. Skowron A, Polak S, Brandys J. The impact of pharmaceutical care on patients with hypertension and their pharmacists. Pharm Pract. 2011;9(2):110–115. doi:10.4321/S1886-36552011000200009
52. Omoregie B. Pharmacist Interventions in POYC Patients [M.pharm. (Melit.)]. Malta: Faculty of Medicine and Surgery, Department of Pharmacy, University of Malta; 2021.
53. Kherghehpoush S, McKeirnan KC. Pharmacist-led HIV and hepatitis C point-of-care testing and risk mitigation counseling in individuals experiencing homelessness. Explor Res Clin Soc Pharm. 2021;1:100007. doi:10.1016/j.rcsop.2021.100007
54. Azhar S, Hassali MA, Ibrahim MIM, Ahmad M, Masood I, Shafie AA. The role of pharmacists in developing countries: the current scenario in Pakistan. Hum Resour Health. 2009;7(1):1–6. doi:10.1186/1478-4491-7-54
55. Di Castri AM, Halperin DM, Ye L, et al. Public awareness, attitudes, beliefs, and behaviors regarding the role of pharmacists as immunizers. Hum Vaccin Immunother. 2021;17(9):3052–3065. doi:10.1080/21645515.2021.1913963
56. Childress BC, Tran HT, Bosler J. Breaking down barriers to advanced pharmacy practice. J Manag Care Pharm. 2012;18(5):395–396. doi:10.18553/jmcp.2012.18.5.395
57. Tak CR, Marciniak MW, Savage A, Ozawa S. The essential role of pharmacists facilitating vaccination in older adults: the case of Herpes Zoster. Hum Vaccin Immunother. 2020;16(1):70–75. doi:10.1080/21645515.2019.1637218
58. Teeter BS, Garza KB, Stevenson TL, Williamson MA, Zeek ML, Westrick SC. Factors associated with herpes zoster vaccination status and acceptance of vaccine recommendation in community pharmacies. Vaccine. 2014;32(43):5749–5754. doi:10.1016/j.vaccine.2014.08.040
59. Wood HM, McDonough RP, Doucette WR. Retrospective financial analysis of a herpes zoster vaccination program from an independent community pharmacy perspective. J Am Pharm Assoc. 2009;49(1):12–17. doi:10.1331/JAPhA.2009.08030
60. Wang J, Ford LJ, Wingate L, et al. Effect of pharmacist intervention on herpes zoster vaccination in community pharmacies. J Am Pharm Assoc. 2013;53(1):46–53. doi:10.1331/JAPhA.2013.12019
61. Griese-Mammen N, Schulz M, Böni F, Hersberger KE. Medication review and medication reconciliation; 2019.
62. Brown L, Seoane-Vazquez E. Pharmaceutical care in North America. In: The Pharmacist Guide to Implementing Pharmaceutical Care. Springer; 2018:145–158.
63. Nunes-da-cunha I, Fernandez-Llimos FJ. Teaching pharmaceutical care at university level. 2019.
64. Barrett R, Hodgkinson J. Quality evaluation of community pharmacy blood pressure (BP) screening services: an English cross-sectional survey with geospatial analysis. BMJ open. 2019;9(12):e032342. doi:10.1136/bmjopen-2019-032342
65. Zammit R. Point of Care Testing in Community Pharmacy Practice [Doctorate in Pharmacy]. University of Malta; 2021.
66. Kherghehpoush S, McKeirnan KC. The role of community pharmacies in the HIV and HCV care continuum. Explor Res Clin Soc Pharm. 2023;9:100215. doi:10.1016/j.rcsop.2022.100215
67. Klepser DG, Klepser ME, Peters PJ, Hoover KW, Weidle PJ. Implementation and evaluation of a collaborative, pharmacy-based hepatitis C and HIV screening program. Prev Chronic Dis. 2022;19:E83. doi:10.5888/pcd19.220129
68. Isho NY, Kachlic MD, Marcelo JC, Martin MT. Pharmacist-initiated hepatitis C virus screening in a community pharmacy to increase awareness and link to care at the medical center. J Am Pharm Assoc. 2017;57(3s):S259–s264. doi:10.1016/j.japh.2017.03.006
69. Alves da Costa F. Pharmaceutical Care in Europe. In: Alves da Costa F, van Mil JWF, Alvarez-Risco A, editors. The Pharmacist Guide to Implementing Pharmaceutical Care. Cham: Springer International Publishing; 2019:159–171.
70. Thorakkattil SA, Nemr HS, Al-Ghamdi FH, Jabbour RJ, Al-Qaaneh AM. Structural and operational redesigning of patient-centered ambulatory care pharmacy services and its effectiveness during the COVID-19 pandemic. Res Social Adm Pharm. 2021;17(1):1838–1844. doi:10.1016/j.sapharm.2020.06.017
71. Nazar H, Nazar Z, Simpson J, Yeung A, Whittlesea C. Use of a service evaluation and lean thinking transformation to redesign an NHS 111 refer to community Pharmacy for Emergency Repeat Medication Supply Service (PERMSS). BMJ Open. 2016;6(8):e011269. doi:10.1136/bmjopen-2016-011269
72. Gilson AM, Stone JA, Morris AO, et al. Impact of a pilot community pharmacy system redesign on reducing over-the-counter medication misuse in older adults. J Am Pharm Assoc. 2021;61(5):555–564. doi:10.1016/j.japh.2021.04.007
73. Gilson AM, Xiong KZ, Stone JA, Jacobson N, Chui MA. A pharmacy-based intervention to improve safe over-the-counter medication use in older adults. Res Social Adm Pharm. 2021;17(3):578–587. doi:10.1016/j.sapharm.2020.05.008
74. Willis SC, Seston EM, Family H, White S, Cutts C. Extending the scope of community pharmacists’ practice to patients requiring urgent care - An evaluation of a training programme using the theoretical domains framework. Health Soc Care Community. 2019;27(4):999–1010. doi:10.1111/hsc.12717
75. Schiff G, Mirica MM, Dhavle AA, Galanter WL, Lambert B, Wright A. A prescription for enhancing electronic prescribing safety. Health Aff. 2018;37(11):1877–1883. doi:10.1377/hlthaff.2018.0725
76. Teichert M. Structure, Process, and outcome, and their indicators. In: Alves da Costa F, van Mil JWF, Alvarez-Risco A, editors. The Pharmacist Guide to Implementing Pharmaceutical Care. Cham: Springer International Publishing; 2019:107–117.
77. Hadi MA, Alldred DP, Briggs M, Munyombwe T, Closs SJ. Effectiveness of pharmacist-led medication review in chronic pain management: systematic review and meta-analysis. Clin J Pain. 2014;30(11):1006–1014. doi:10.1097/AJP.0000000000000063
78. Murry LT, Viyurri B, Chapman CG, et al. Patient preferences and willingness-to-pay for community pharmacy-led medicare Part D consultation services: a discrete choice experiment; 2023.
79. Murry LT, Murry RC, Deng H, Viyyuri B, Gerleman BL, Urmie JJ. Community pharmacy medicare part d consultations: plan-switching decisions and chronic medication adherence. Journal of Pharmacy Practice. 2021;34(5):727–733. doi:10.1177/0897190020903852
80. Cooper JB, Scotti A, Carr ML, Pharmacy A. Implementing medicare education for medication access: a review of the literature using the RE-AIM framework; 2022.
81. Lloyd-Williams FJPE. counseling. The effect of an intervention programme to improve health education leaflet uptake and distribution in community pharmacies. Patient Educ Couns. 2003;49(1):27–33. doi:10.1016/S0738-3991(02)00034-4
82. Semegn S, Alemkere GJ. Assessment of client satisfaction with pharmacist services at outpatient pharmacy of Tikur Anbessa specialized hospital. PLoS One. 2019;14(10):e0224400. doi:10.1371/journal.pone.0224400
83. Kheir N, Emmerton L, Shaw J. Can pharmacists influence the health-related quality of life of patients with asthma?: the New Zealand pharmaceutical care experience. Sultan Qaboos Univ Med J. 2001;3(2):69–75.
84. Correr CJ, Pontarolo R, Venson R, Melchiors AC, Wiens A, Wiens A. Effect of a pharmaceutical care program on quality of life and satisfaction with pharmacy services in patients with type 2 diabetes mellitus. Braz J Pharm Sci. 2009;45:809–817. doi:10.1590/S1984-82502009000400027
85. Sakthong P, Sangthonganotai T. A randomized controlled trial of the impact of pharmacist-led patient-centered pharmaceutical care on patients’ medicine therapy-related quality of life. Res Social Adm Pharm. 2018;14(4):332–339. doi:10.1016/j.sapharm.2017.05.001
86. René-Henri N, Khamla Y, Nadaira N, et al. Community pharmacists’ interventions in asthma care: a descriptive study. Ann Pharmacother. 2009;43(1):104–111. doi:10.1345/aph.1L308
87. Vella J, Azzopardi LM. Pharmacist-led diabetic patient monitoring; 2013.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pharmaceutical Care Services in Community Pharmacies: An Umbrella Review of Global Evidence with Insights from Polish and Spanish Practices
Żuk A, Machuca M
Integrated Pharmacy Research and Practice 2025, 14:113-136
Published Date: 2 September 2025