Back to Journals » OncoTargets and Therapy » Volume 7
Outcomes analysis of an alternative formulation of PEGylated liposomal doxorubicin in recurrent epithelial ovarian carcinoma during the drug shortage era
Authors Berger J, Smith A, Zorn K, Sukumvanich P, Olawaiye A, Kelley J, Krivak T
Received 22 February 2014
Accepted for publication 7 April 2014
Published 8 August 2014 Volume 2014:7 Pages 1409—1413
DOI https://doi.org/10.2147/OTT.S62881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Jessica L Berger, Ashlee Smith, Kristin K Zorn, Paniti Sukumvanich, Alexander B Olawaiye, Joseph Kelley, Thomas C Krivak
Magee-Womens Hospital, University of Pittsburgh Medical Center, Division of Gynecologic Oncology, Pittsburgh, PA, USA
Corrigendum for this paper has been published
A Letter to the Editor has been received and published for this article
Introduction
Epithelial ovarian cancer (EOC) is the leading cause of death from gynecologic cancer in the USA, with an expected 22,240 new diagnoses and 14,030 deaths in 2013.1 Despite high rates of initial remission with aggressive cytoreductive surgery and platinum-based combination chemotherapy, approximately 75% of patients will progress or have recurrence. Response rates to second-line therapy in these patients generally range from 10% to 78%, with median overall survival ranging from 6 to 14 months for platinum-resistant patients to 20–33 months for those with platinum-sensitive disease.2–11
Doxorubicin is considered an active agent in the treatment of EOC, but its use is limited by cumulative dose-dependent cardiac toxicity and myelosuppression. Liposomal encapsulation and PEGylation of doxorubicin maintains efficacy while improving the toxicity profile by limiting hematologic and cardiac toxicity; however, palmar-plantar erythrodysesthesia remains the dose-limiting toxicity. PEGylated liposomal doxorubicin (PLD) has emerged as an effective and well tolerated chemotherapeutic agent for recurrent EOC, with response rates of 8%–26%.2,4–6
In November 2011, manufacturing issues resulted in a national shortage of Doxil® (Ben Venue Laboratories, Bedford, OH, USA), ie, the PLD formulation used in the USA. In response to the national drug shortage, the US Food and Drug Administration (FDA) used enforcement discretion to allow temporary importation of Lipo-Dox® (Sun Pharma, Gujarat, India), ie, the second-generation PLD commonly used in Asian countries. While these agents contain the same active ingredient, they utilize different liposomal particles with different phase transition temperatures and pharmacokinetic properties. While enforcement discretion requires inspection of foreign manufacturing plants, it does not require clinical testing of the substitute drug. No study to date, has investigated the efficacy of Lipo-Dox in a North American population, despite its widespread use during the Doxil shortage.
The objective of this study was to retrospectively evaluate the clinical outcomes and tolerability of Lipo-Dox in patients with recurrent EOC treated during the drug shortage period.
Materials and methods
After obtaining institutional review board approval from the University of Pittsburgh, patients treated at Magee-Womens Hospital, University of Pittsburgh Medical Center, with Lipo-Dox from January 2012 through until December 2012 were identified from chemotherapy administration records. Eligibility criteria included recurrent or progressive EOC, measurable disease on imaging, or evaluable disease based on an elevated CA-125 level, and treatment with at least one cycle of Lipo-Dox during the study period.
Demographic and clinicopathologic data were abstracted retrospectively from the medical records. Outcome data of interest included response rates, time to progression, progression-free survival, overall survival, and toxicity. Response rates were defined by RECIST (Response Evaluation Criteria in Solid Tumors) or by CA-125 levels if measurable disease was not present. Evaluable disease response, measured by CA-125, was defined as complete if the CA-125 level normalized for one month or longer, and partial if a 50% reduction was observed. Progression was defined either by RECIST or a doubling of CA-125, while stable disease was defined as those not falling into partial response or progressive disease. Time to progression, progression-free survival, and overall survival were defined from the first cycle of Lipo-Dox to the first documented progression or death, respectively. Toxicity was defined by the Gynecologic Oncology Group common toxicity criteria.12 Descriptive statistics were used for this observational study.
Results
Eighteen patients with recurrent EOC who received Lipo-Dox were identified. Demographic and clinicopathologic variables are listed in Table 1. All women were Caucasian and their median age was 62 (range 44–72) years. One patient had a performance status of 2; the remainder had a performance status of 0. The majority had stage III/IV high-grade serous EOC and 15 were optimally cytoreduced at initial debulking surgery. Two patients had neoadjuvant chemotherapy with optimal interval debulking. The median primary platinum-free interval was 7 (range 0–39) months, and eight patients (44%) had platinum-resistant or refractory disease. Eight of the ten patients who were platinum-sensitive at first recurrence received platinum-based, second-line chemotherapy. The median number of prior treatment regimens was three (range 1–6). All patients had measurable disease at initiation of Lipo-Dox.
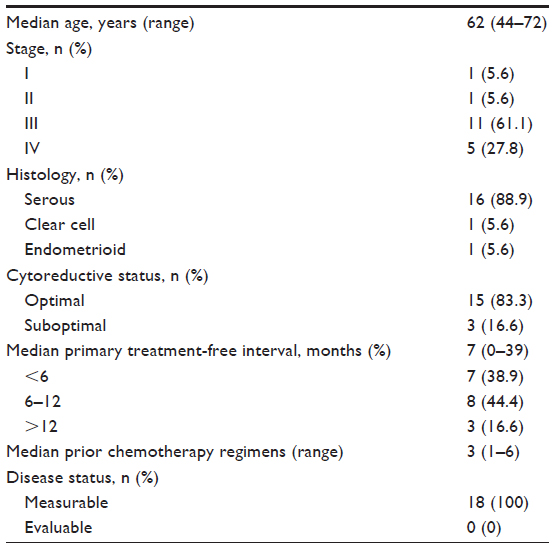 | Table 1 Patient demographic and clinicopathologic characteristics |
Treatment characteristics and clinical outcomes are shown in Table 2. A median of 3.5 (range 1–8) cycles of Lipo-Dox was given. Six patients received combination chemotherapy with the addition of carboplatin (n=2), bevacizumab (n=2), or both agents (n=2). Patients receiving Lipo-Dox in combination with carboplatin were dosed at 30 mg/m2; all others received a dose of 40 mg/m2, ie, the same dosing schedule that is used for Doxil at Magee-Womens Hospital. Two patients received only one cycle of Lipo-Dox. The first patient had a hypersensitivity reaction, therefore, was switched to gemcitabine and bevacizumab, and experienced disease progression. The second patient had a decline in performance status, therefore, was treated with the best supportive measures, and died approximately 2 months later without an evaluation of her disease status.
 | Table 2 Treatment characteristics and patient outcomes |
No patient had a complete or partial response during the treatment period. Two patients had stable disease at a follow-up at 114 and 175 days, indicating a disease control rate of 11%. One patient with stable disease was treated with concurrent carboplatin for her first recurrence after a 6-month progression-free interval. The other patient with stable disease received single-agent Lipo-Dox after four prior regimens. Progression was based on RECIST in ten patients and CA-125 levels in four patients. The median progression-free survival was 83 (range 25–175) days. Median overall survival has not been reached as only nine patients died during the study period. All died from their disease, with survival ranging from 69 to 223 days.
Grade 3 or 4 toxicity as defined by Gynecologic Oncology Group common toxicity criteria was observed in three patients.12 One patient had a hypersensitivity reaction during her first cycle and was not rechallenged. Another patient had grade 3 leukopenia requiring growth factor support. A third patient developed palmar-plantar erythrodysesthesia and required dose reduction.
Discussion
Liposomal doxorubicin has become an important therapeutic agent in recurrent EOC due to its efficacy and tolerability. Liposomal encapsulation and surface PEGylation have extended the half-life of doxorubicin by reducing recognition by the reticuloendothelial system and slowing drug clearance at a smaller volume of distribution. PEGylated liposomes have also demonstrated a passive targeting effect, leading to preferential accumulation in tumor tissue. The pharmacokinetic behavior of PLD reduces myelosuppression and cardiotoxicity without compromising efficacy.13
The lipid bilayer of the FDA-approved PLD, Doxil, is composed of hydrogenated soybean phosphatidylcholine and coated with poly-(ethylene glycol)-distearoylphosphatidylethanolamine (HSPC/PEG-DPSE). In the fall of 2011, manufacturing issues resulted in a critical shortage of Doxil. In response, the FDA exercised temporary enforcement discretion for the importation of an alternative formulation of PLD, Lipo-Dox, which utilizes a distearoylphosphatidylcholine (DSPC)/PEG-DSPE liposome with a slightly higher phase transition temperature than HSPC, and therefore higher stability and a longer half-life.14 Lipo-Dox, while not FDA-approved, utilizes the same active ingredient, dosage, strength, and route of administration as Doxil, and is produced in a facility inspected by the FDA and found to be in compliance with Good Manufacturing Practice.
Lipo-Dox has been evaluated in Asian populations, with response rates comparable with studies of Doxil in North American populations; however, no study has compared these two agents. Fukuda et al retrospectively evaluated 19 patients with platinum-resistant or refractory EOC in Japan and demonstrated a 26.3% response rate with five partial responses. Six additional patients had stable disease indicating a disease control rate of 58.9%. Median progression-free survival and overall survival were 188 days and 381 days, respectively.15 Lipo-Dox was prospectively evaluated in a Phase II trial of 29 patients with platinum-resistant or refractory EOC in Taiwan. The overall response rate was 23.1%, with one complete response, five partial responses, and nine patients with stable disease. The median progression-free survival and overall survival was 5.4 and 13.8 months, respectively.14
The current study is the first to evaluate the use of Lipo-Dox in a North American population. Although this represents a small pretreated population, there were no clinical responses to Lipo-Dox, with a disease control rate of 11% and median progression-free survival of 83 days. While these results are disappointing, previous US studies evaluating PLD have also had variable outcomes, and European data on Doxil initially showed no objective responses in 30 patients when presented to the FDA. Initially, a Phase II study reported by Muggia et al, of single-agent PLD in a North American population, reported a 25.7% response rate.6 Gordon et al reported on a Phase III trial comparing PLD with topotecan in recurrent EOC, with an overall response rate of 19.7% for PLD and a disease control rate of 51.9%.2 However, a Phase III trial comparing gemcitabine with PLD in a platinum-resistant population reported a median progression-free survival of 3.1 months, a response rate to PLD of 8.3%, and a disease control rate of 46.9%.5 A retrospective report, similar to the current study, on the use of PLD in 17 heavily pretreated patients, with recurrent EOC, in Turkey demonstrated a 17% response rate and a disease control rate of 28%.16 Despite the current study population having less platinum-resistant disease than the aforementioned European and US PLD studies, disease response and control was less than expected.
Several possible explanations exist to account for the apparent inferior clinical outcomes of Lipo-Dox in our study. First, our population of patients was more heavily pretreated, receiving a median of three prior chemotherapeutic regimens compared with two prior lines of therapy in the studies by Chou et al14 and Fukuda et al.15 Second, the patients in our study received a lower average dose of Lipo-Dox, ie, 40 mg/m,2 compared with 45 mg/m2 in the Japanese study and 50 mg/m2 in the Taiwanese study. Despite these limitations and the selection bias inherent in retrospective studies, these results raise the question as to whether this formulation of PLD has equivalent efficacy in a North American population when compared with Asian populations, or when compared with Doxil. The small sample size does not allow for definitive conclusions to be drawn, but does raise the question of equivalency. One can only speculate on the reasons for this potential difference, which may include pharmacologic differences between the drugs, or differences in the histologic distribution, or disease biology of ovarian cancer in Asian and North American populations. Evaluation of the outcomes at other centers affected by the Doxil shortage should be encouraged, because prospective evaluation is unlikely to be conducted with the restoration of the FDA-approved drug supply, and the outcomes could affect future drug shortage policy and management.
Temporary importation of foreign drugs has been a successful strategy for several drug shortages in the recent past, when manufacturing issues regarding FDA-approved products cannot be proximately resolved. Manufacturing of Doxil was resumed in November 2012, and an FDA-approved generic form of Doxil was introduced onto the market in March 2012, effectively restoring the domestic drug supply. Nonetheless, further investigation into the clinical outcomes of the patients treated with Lipo-Dox during the critical Doxil shortage is warranted.
Conclusion
Drug shortages are expected to become more frequent in the future, and strategies including mandated reporting of manufacturing issues, and incentivizing generic drug production are underway.17 Our findings require further evaluation, but call into question the prudence of using pharmacologically similar, but clinically untested imported drugs. Confirmation of our findings would impact the use of current stocks of Lipo-Dox remaining from the drug shortage period, but more importantly, provide regulatory guidance on foreign pharmaceutical importation in the management of future drug shortages. Ongoing investigation at the institutional level should be encouraged to ensure equivalent clinical outcomes and patient safety.
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer Clin. 2013;63(1):11–30. | |
Gordon AN, Fleagle JT, Guthrie D, Parkin DE, Gore ME, Lacave AJ. Recurrent epithelial ovarian carcinoma: a randomized phase III study of PEGylated liposomal doxorubicin versus topotecan. J Clin Oncol. 2001;19(14):3312–3322. | |
ten Bokkel Huinink W, Gore M, Carmichael J, et al. Topotecan versus paclitaxel for the treatment of recurrent epithelial ovarian cancer. J Clin Oncol. 1997;15(6):2183–2193. | |
O’Byrne KJ, Bliss P, Graham JD, et al. A Phase III study of Doxil/Caylex versus paclitaxel in platinum treated taxane naive relapsed ovarian cancer. Proc Am Soc Clin Oncol. 2002;21(Suppl; abstract 808):203a. | |
Mutch DG, Orlando M, Goss T, et al. Randomized phase III trial of gemcitabine compared with pegylated liposomal doxorubicin in patients with platinum-resistant ovarian cancer. J Clin Oncol. 2007;25(19):2811–2818. | |
Muggia FM, Hainsworth JD, Jeffers S, et al. Phase II study of liposomal doxorubicin in refractory ovarian cancer: antitumor activity and toxicity modification by liposomal encapsulation. J Clin Oncol. 1997;15(3):987–993. | |
Gore M, Oza A, Rustin G, et al. A randomised trial of oral versus intravenous topotecan in patients with relapsed epithelial ovarian cancer. Eur J Cancer. 2002;38(1):57–63. | |
Aghajanian C, Blank SV, Goff BA, et al. OCEANS: a randomized, double-blind, placebo-controlled Phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J Clin Oncol. 2012;30(17):2039–2045. | |
Wagner U, Marth C, Largillier R, et al. Final overall survival results of phase III GCIG CALYPSO trial of pegylated liposomal doxorubicin and carboplatin vs paclitaxel and carboplatin in platinum-sensitive ovarian cancer patients. Br J Cancer. 2012;107(4):588–591. | |
Markman M, Rothman R, Hakes T, et al. Second-line platinum therapy in patients with ovarian cancer previously treated with cisplatin. J Clin Oncol. 1991;9(3):389–393. | |
Monk BJ, Herzog TJ, Kaye SB, et al. Trabectedin plus PEGylated liposomal doxorubicin (PLD) versus PLD in recurrent ovarian cancer: overall survival analysis. Eur J Cancer. 2012;48(15):2361–2368. | |
Rubin SC, editor. Chemotherapy of Gynecologic Cancers. 2nd ed. Philadelphia, PA, USA: Lippincott Williams & Wilkins; 2004. | |
Immordino ML, Dosio F, Cattel L. Stealth liposomes: review of the basic science, rationale, and clinical applications, existing and potential. Int J Nanomedicine. 2006;1(3):297–315. | |
Chou HH, Wang KL, Chen CA, et al. Pegylated liposomal doxorubicin (Lipo-Dox) for platinum-resistant or refractory epithelial ovarian carcinoma: a Taiwanese gynecologic oncology group study with long-term follow-up. Gynecol Oncol. 2006;101(3):423–428. | |
Fukuda T, Sumi T, Teramae M, et al. PEGylated liposomal doxorubicin for platinum-resistant or refractory Mullerian carcinoma (epithelial ovarian carcinoma, primary carcinoma of Fallopian tube and peritoneal carcinoma): a single-institutional experience. Oncol Lett. 2013;5(1):35–38. | |
Gorumlu G, Kucukzeybek Y, Kemal-Gul M. Pegylated liposomal doxorubicin in heavily pretreated epithelial ovarian cancer patients. J BUON. 2008;13(3):349–352. | |
Chabner BA. Drug shortages – a critical challenge for the generic drug market. N Engl J Med. 2011;365(12):2147–2149. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.