")
Back to Journals » Clinical Ophthalmology » Volume 9
Outcome of therapeutic penetrating keratoplasty in a tertiary eye care center in Nepal
Authors Bajracharya L , Gurung R
Received 10 July 2015
Accepted for publication 9 October 2015
Published 7 December 2015 Volume 2015:9 Pages 2299—2304
DOI https://doi.org/10.2147/OPTH.S92176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Leena Bajracharya, Reeta Gurung
Department of Cornea, Tilganga Institute of Ophthalmology, Kathmandu, Nepal
Background: Corneal ulcer is an important cause of blindness in developing countries. Therapeutic keratoplasty for infective keratitis is a frequently performed surgery in these countries.
Objective: To find out the outcome of therapeutic keratoplasty for infective keratitis.
Methods: Records of 5 years were reviewed of patients who underwent therapeutic keratoplasty from 2006 to 2010. Data collected included demographic parameters, indications for surgery, microbiology of the ulcers, type of surgery performed, and donor tissue details. In the follow-up period, ocular status was evaluated in terms of eradication of disease, anatomic success, graft clarity, visual acuity, and development of glaucoma and cataract.
Results: In all, 180 eyes of 180 patients were enrolled in the study; 59.4% of the patients were male. Average age was 44.4±16.7 years. Overall, 71% of infective keratitis was perforated. A total of 101 (56%) eyes were positive for organisms of which 49 showed pure fungus and 49 showed pure bacteria. The commonest fungus and bacteria isolated were Aspergillus and Streptococcus, respectively. Average follow-up period was 29±23 months. Overall cure rate of infection was 88.8%, anatomical success rate was 89.5%, and graft clarity was 37.2%. Overall, 43.4% had secondary glaucoma. In the postoperative course, 65.8% of phakic eyes had developed cataract. In all, 38.6% of graft had endothelial failure and 24% of the graft failed due to late infective keratitis. Overall functional success with a visual acuity above 6/60 was 25.4%. Bacterial keratitis had a significantly higher cure rate, anatomical success, and graft clarity compared to fungal keratitis.
Conclusion: Therapeutic keratoplasty is an important procedure to save the eye and preserve vision in severe infective keratitis. There is a high incidence of postoperative glaucoma, cataract, and graft failure in such a surgery. Bacterial keratitis has a better outcome than fungal keratitis.
Keywords: therapeutic penetrating keratoplasty, infective keratitis, Nepal, corneal ulcer
Introduction
In developing countries, corneal ulcer is the major cause of visual impairment and blindness.1 Lack of accessibility of eye care, delayed or inappropriate treatment, and microbes not responding to antimicrobial therapy may result in a large or perforated ulcer which will necessitate therapeutic penetrating keratoplasty (TPK). The procedure is meant to terminate or reduce an actively infectious corneal disease or repair an anatomic defect in the cornea.2 It is generally performed in an emergency or semi-emergency basis, and its primary goal is to reestablish globe integrity. Visual rehabilitation is a secondary consideration.
TPK constitutes a significant proportion of keratoplasty performed in Asian and other developing countries.2 In the Tilganga Institute of Ophthalmology, which is a tertiary center for cornea service in Nepal, TPK accounts for 41% of all grafts performed.3 TPK carries a risk of recurrence of infection and also has a higher risk of graft rejection and graft failure compared to optical keratoplasty. It has a higher incidence of postoperative uveitis, glaucoma, synechia, and cataract.4 This study is intended to find out the outcome of TPK. This will provide baseline information for further prospective studies which in turn will help to identify the changes that need to be done to improve the outcome.
Materials and methods
This is a retrospective study of all consecutive cases that underwent TPK for active infective keratitis in the Tilganga Institute of Ophthalmology from January 2006 to December 2010. Data were collected about demographic parameters, indications for TPK, microbiology of the ulcers, type of surgical procedure performed, details of donor tissue in terms of donor age, graft size, and endothelial density, duration of follow-up, and any significant events happening in the postoperative period. The outcome of TPK was measured in terms of anatomic stability, eradication of disease, visual acuity, graft clarity, and development of cataract and glaucoma. Comparison was made between the outcome of bacterial and fungal ulcer undergoing TPK. Cases which had follow-up of less than 2 months were not analyzed for outcome. In those cases that had undergone TPK more than once, only the first TPK was considered for outcome assessment. A P-value of more than 0.05 was considered significant. Since this is a retrospective study ethical approval was not required from our institute, and patient consent was not necessary.
Surgical technique and postoperative management
The TPK was performed under peribulbar block, except in children. The criteria for quality of the donor tissue may not be as stringent as for optical penetrating keratoplasty. So, even very old, aged cornea or with low endothelial cell count was used. In all cases, the donor size was exceeded by 0.5 mm. The recipient cornea was incised using either a handheld or a vacuum trephine. Care was taken to avoid pressure on the globe. In case of a large perforation and sloughing ulcer, freehand dissection of the host bed was performed, after initial marking with a trephine. The entire infiltrated area along with 1 mm of healthy corneal tissue was removed in most of the cases except when the whole of the cornea was infiltrated. The excised corneal specimen was sent for microbial investigations.
Purulent material was irrigated from the anterior chamber (AC). Inflammatory membranes over the iris and pupil were mechanically removed with forceps. Anterior and posterior synechia were released. One or two iridectomies were performed to prevent pupillary block glaucoma. Cataract extraction was done when there was infection extending to the lens, presence of white swollen lens with probability of pupillary block, iatrogenic trauma to lens, or when lens was extruded itself. Intravitreal injection of antimicrobial and/or anterior vitrectomy was done in cases of suspected endophthalmitis and spontaneous lens extrusion. 10-0 Nylon interrupted sutures were used to close the graft host junction.
Postoperatively, the duration of antimicrobial treatment as well as initiation and frequency of steroids were titrated based on severity of infection, type of infection, associated epithelial defect, and postoperative inflammation. Fungal keratitis requires longer treatment than bacterial. Steroids were started almost immediately in bacterial keratitis but in fungal, it was delayed by 1 to 2 weeks postoperatively. In case of recurrence of the infection, steroids were avoided. Other postoperative problems including formation of synechia, shallowing of AC, secondary glaucoma, non-healing epithelial defect, and loose sutures were managed with supportive medications and/or with procedures such as AC reformation, synechiolysis, tarsorrhaphy, and resuturing of the wound.
Results
Demographic parameters
Overall, 180 eyes of 180 patients had undergone TPK for infective keratitis; 59.4% were male. Average age of the patients was 44.4±16.7 years (range 1.25 to 82 years). Eight patients had undergone TPK more than once in the same eye. In all, 26 patients were from the urban area, 16 were from India, and the remaining 138 (76.6%) patients were from rural districts of Nepal.
Donor cornea details
Average waiting time of patients for TPK was 4.7±4.52 days. Average age of donor cornea and endothelial cell count was 67.5±17.1 years (range 7 to 98 years) and 2,321.5±471.4 cells/mm2 (range 1,173 to 3,875 cells/mm2), respectively. Mean recipient rim size was 8.02±0.48 mm.
Indications for TPK
A total of 128 cases (71.1%) were perforated corneal ulcers and the remaining were non-healing ulcers or ulcers impending to perforate.
Out of 180 eyes of TPK, 101 (56.1%) were positive for organisms of which 49 showed pure fungus, 49 showed pure bacteria, and three showed mixed bacteria and fungus (Table 1). Culture-negative cases were treated according to the clinical diagnosis. In the culture-negative group, the presumed etiology of 20 cases was virus. There is no facility of polymerase chain reaction test for virus in our institute.
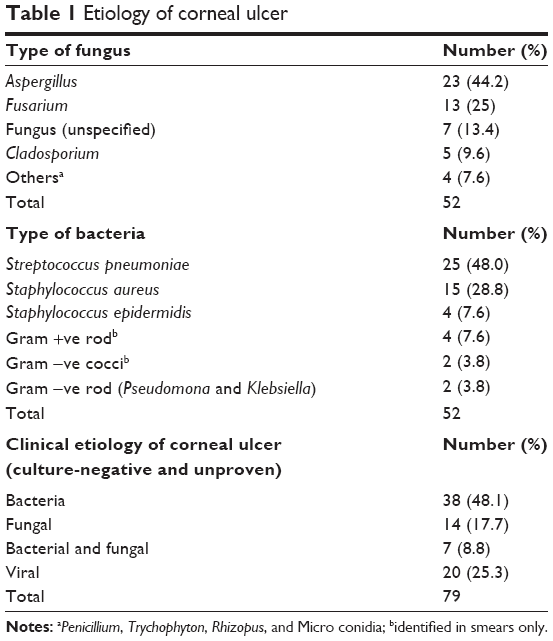 | Table 1 Etiology of corneal ulcer |
Procedure
All patients had undergone full thickness keratoplasty. Out of 180 TPK, 33 surgeries (18.3%) were combined with extracapsular cataract extraction with (n=18) or without (n=13) posterior chamber intraocular lens.
In the early postoperative period of 2 weeks, 49 out of 180 patients underwent synechiolysis and AC deepening procedure. In five cases, AC reformation was combined with extracapsular cataract extraction with or without posterior chamber intraocular lens. Resuturing was done in 25 eyes. Other postoperative procedures performed were tarsorrhaphy, injection of intracameral antifungal, and intravitreal antibiotics.
Overall cure rate (eradication of infection after primary TPK) was 160/180 (88.8%) (Table 2). Recurrence of infection occurred within 2 weeks in bacterial keratitis and within 1 month in fungal. Five eyes with fungal recurrence were eviscerated, two underwent second TPK, and two cases became anterior staphyloma (blind eye). One bacterial recurrence underwent second TPK and one became phthisical due to endophthalmitis. All three second TPKs were successful in eradication of infection. All three recurrences in the culture-negative cases had to be eviscerated due to extension of infection in the sclera or due to endophthalmitis (Tables 2 and 3). Only six out of 20 recurrences healed with structural integrity of eye. Not included in Table 2 are viral recurrences in the culture-negative group. Twelve out of 20 clinical viral ulcers in this group had recurrence of viral one or more times in course of follow-up.
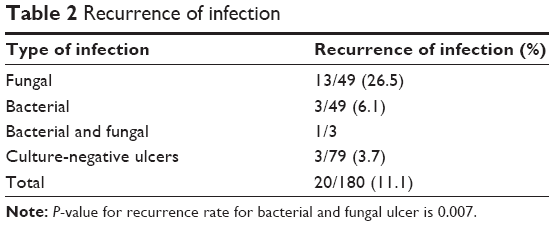 | Table 2 Recurrence of infection |
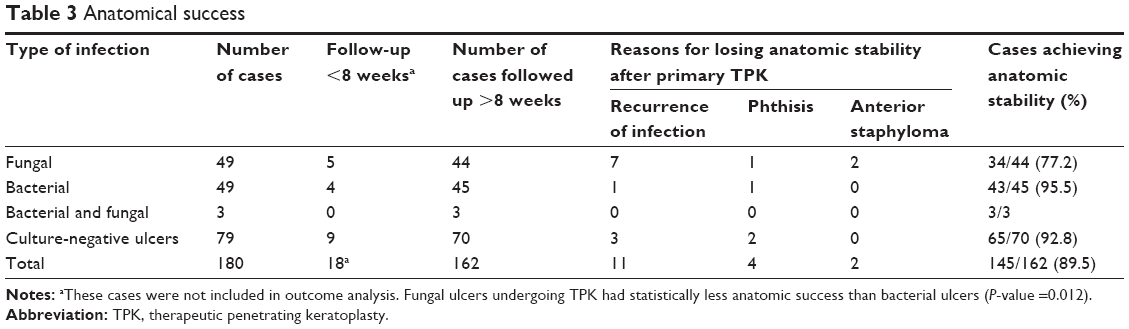 | Table 3 Anatomical success |
The average follow-up duration of 145 eyes having anatomical success was 29±23 months (2–86 months). These eyes were further analyzed for graft clarity, functional success (visual acuity), and development of secondary glaucoma and cataract.
Causes of graft failure
Late infective keratitis in the graft
In 35 eyes of 35 patients, the graft was complicated by development of late microbial keratitis after eradication of initial infection (Table 4). Five of them had to undergo TPK again for structural integrity.
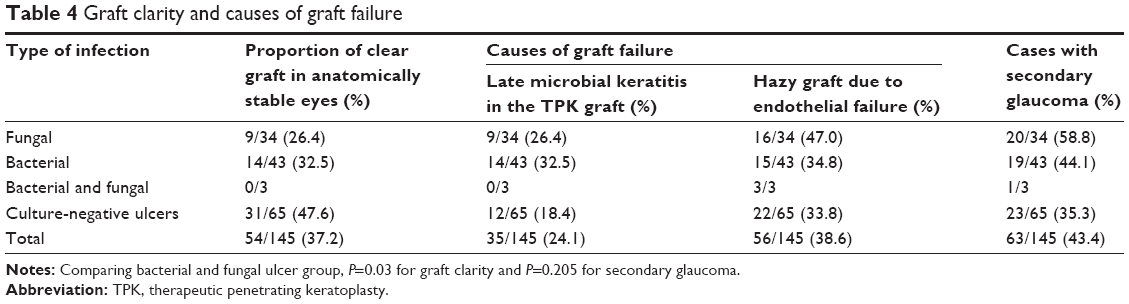 | Table 4 Graft clarity and causes of graft failure |
Cause of endothelial failure
There was graft rejection in 20 cases, out of which 16 grafts failed despite treatment because they presented late. In our study, 26 cases had edematous decompensated graft, the cause of which could be either late endothelial decompensation or graft rejection which could have happened at the time when patients had not followed up. Other causes of endothelial failure were secondary glaucoma (n=4), primary graft failure (n=3), re-procedures (n=4), and recurrent viral keratouveitis (n=3). (To mention, eleven failed grafts underwent regraft surgery. Outcome of regraft was not analyzed in our study).
Overall functional success with a visual acuity above 6/60 was 25.4% (Table 5). Causes of a visual acuity below 6/60 were hazy graft (n=51), scarred graft (n=28), cataract (n=42), glaucoma (n=21), and clear graft with high astigmatism (n=1) (cases have more than one cause).
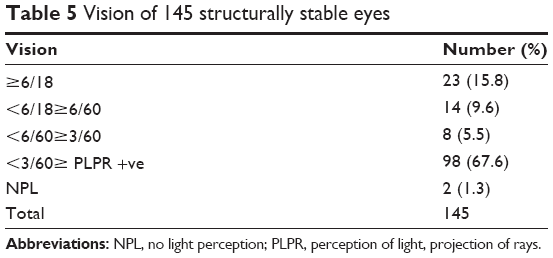 | Table 5 Vision of 145 structurally stable eyes |
In all, 21/54 (38.8%) patients, despite having clear grafts, had a visual acuity below 6/18 which was because of or a combination of cataract, high astigmatism, secondary glaucoma, aphakia, and maculopathy.
Late complications
Cataract
On follow-up of 117 phakic eyes, 65.8% had documentation of variable grades of cataract. In all, 22 of them had undergone cataract extraction with posterior chamber intraocular lens in the later postoperative period.
Secondary glaucoma
Overall, ten out of 63 cases of glaucoma needed interventional treatment. Among these ten cases, seven underwent transscleral cyclophotocoagulation, two underwent valve implant, and one underwent trabeculectomy. Six out of ten interventions were performed in fungal group, and two each in the bacterial and culture-negative groups.
Discussion
The mean age group of our patients, 44 years, is similar to that in Northern India and Iran, but varies with other Asian countries where the mean age is >55 years.5–8 Male preponderance of the patients is also seen in India, Singapore, and Iran.5,6,8 This could be because more men work outside home and are prone to work-related trauma. There could also be gender bias in health care in a male-dominant society like ours.
Corneal ulcers presenting in the Tilganga Institute of Ophthalmology are severe, already perforated, or impending to perforate. That is why 71% of TPKs were done for perforated corneal ulcers. Sedghipour et al and Sukhija and Jain reported even greater proportion of perforated ulcers, 76%–88%.6,9
Bacterial and fungal organisms isolated in our study are in fact the commonest organisms causing infective keratitis in the country (Table 1).10–12 We had a large number of culture-negative cases. This could be because patients were already treated with various antimicrobials before they came to our institute. In our study, the ratio of fungal to bacterial ulcers undergoing TPK was 1:1. In other studies done in Asia, this ratio ranges from 1:0.7 to 1.3:1.5,7,8 Aspergillus is the commonest fungus needing TPK in North India and Taiwan but in Singapore, it is Fusarium. In Taiwan and Singapore, the commonest bacterium isolated in TPK cases is Pseudomonas, in which the predisposing factor for ulcer is contact lens but in India, it is Staphylococcus.5,7,8 Only culture-proven pure fungal and -pure bacterial ulcers are compared to avoid bias.
Cataract surgery was the commonest procedure combined with TPK. Other reports mention TPK combined with cataract surgery in 3%–50% of TPK.4
Postoperatively, TPK has a high incidence of severe AC reaction, shallow AC, synechia, and high intraocular pressure. Sony et al mentioned a range of postoperative AC shallowing as 9% to 31% in various studies.4 In our study, 27% needed AC reformation. Some cases required cataract extraction for deepening of AC and prevention of synechia. There is a high chance of primary graft failure on repeated intervention.
Recurrence of infection is a very undesirable complication which may again stake the structural integrity of the operated eye. Our study shows fungal ulcers undergoing TPK have higher chances of recurrence than bacterial ulcers with statistical significance (P-value =0.007) (Table 2). Other reports mention recurrence rate of fungus after TPK to be 7.3%–10%.4 Sharma et al mentioned cure rate (absence of recurrence) in fungus as 69%–90%.2 Our high recurrence rate of 26% could be because of residual infection in the recipient rim in three cases, associated fungal endophthalmitis in one case, and because many fungal corneal ulcers presenting in our institute were advanced with extensive invasion of anterior segment structures. Sharma et al quoted the cure rate of bacterial ulcers as 90%–100% and our bacterial cure rate also lies within this range.2 Although we have no evidence to support with a polymerase chain reaction test, in our study, 12 out of 20 (60%) viral keratitis undergoing TPK in culture-negative group had recurrent viral keratitis later in the postoperative period. Recurrence of herpetic keratitis varies widely among different studies from 8.8%–75%.4
In our study, overall anatomic stability after primary TPK was 89.5% (Table 3), which is similar to that reported by Cristol et al and Sukhija and Jain.9,13 Anatomic stability was more in TPK performed for bacterial ulcers than for fungal ulcers (P-value =0.012). Sharma et al and Chen et al reported 90%–92% anatomical success rate for bacterial and 84.6%–88.5% for fungal ulcer.5,7 Low anatomical stability in fungal ulcer in our study was due to a high rate of recurrence of fungus as already described earlier.
Graft clarity was less in the case of fungal than bacterial ulcers (P=0.03) (Table 4). Sharma et al mentioned that the range of clear graft at 1-year follow-up varied from 69%–100% in bacterial ulcers and varied from 51%–84% in fungal ulcers.2 Graft clarity also depends on follow-up time. In our study, with an average follow-up period of 29 months, graft clarity was 37.2%. The majority of patients, 76.6%, were from far rural areas and did not regularly follow up, and this had an implication in the graft survival.
Late postoperative keratitis is quite common in patients who had undergone keratoplasty surgery. Risk factors have been loose sutures, topical steroid, and decreased sensation.14 In our series, 24% of 145 eyes, who had achieved eradication of initial infection, developed late microbial keratitis (Table 4). The course of microbial keratitis in corneal graft progresses rapidly due to compromised ocular surface and use of topical steroids. Five of them needed therapeutic keratoplasty to save the eyeball. Vajapayee et al mentioned the rate of infective keratitis after keratoplasty as 1.46%–11.9%.14 High incidence and more severe form of late keratitis in our study could be due to patients not being able to come timely for follow-up care.
In total, 25.2% had a visual acuity above 6/60 after achieving anatomic success (Table 5). Sharma et al reported 14.8% patients with a visual acuity above 6/60 at 1-year follow-up.5 In our study, 22 patients had undergone cataract surgery at various times. This could be the reason for better vision in our study. Full visual rehabilitation such as cataract surgery, regraft, and correction of astigmatism was not performed for many patients as most of our unilateral blind patients were not willing to undergo a second surgery.
Cataract is a common complication of corneal ulcer, surgical procedure, inflammation, and topical steroids. In our study, presence of cataract in phakic TPK eyes was 65.8%. There is reporting of 51%–77.7% incidence of cataract in TPK done for active viral keratitis.4
Graft rejection was present in 20/145 (13.7%) cases who followed up. Sony et al reported that rejection rates in TPK varied from 14.6% to 52.1%.4 In our study, 26 cases were edematous decompensated graft. In this group, it was clinically difficult to distinguish whether edema resulted due to late decompensation or rejection which happened at the time patient did not follow-up. This could be the reason why graft rejection was reported less in our study. We had only 20% of rejections being reversed with treatment whereas Sedghipour et al report reversal of graft rejection in 66.6% of cases.6 Low rate of reversal could be due to patients not able to present timely.
Secondary glaucoma is mostly due to extensive peripheral anterior synechia and may lead to graft failure and blind eye. We noted a high incidence of secondary glaucoma of 43.4% (Table 4) compared to that reported by Sharma et al and Sukhija and Jain who mentioned 25% and 22%, respectively.5,9 Although presence of secondary glaucoma is not significant statistically, medically uncontrolled glaucoma was found more in fungal group than bacterial. In our study, up to 58.8% of cases in fungal group developed glaucoma. This could be because of controlled use of steroids in fungal keratitis in early postoperative period. Other reports show 2%–50% incidence of secondary glaucoma in fungal TPK.4,15
A limitation of our study is the wide range of follow-up as well as variation in donor tissue quality. There is a large group of culture-negative cases which included viral keratitis. Outcome of viral ulcer cannot be commented because we lack polymerase chain reaction for definite diagnosis.
Conclusion
Therapeutic keratoplasty has a definite role in the management of perforated and/or severe infective keratitis. TPK provides structural stability, ambulatory vision, and can preserve potentiality of vision. Presence of infection and inflammatory status of the eye at the time of TPK makes the postoperative course challenging. Bacterial ulcers undergoing TPK have a better outcome in comparison to fungal ulcers.
Disclosure
The authors report no conflicts of interest in this work.
References
Whitcher JP, Srinivasan M. Corneal ulceration in the developing world – a silent epidemic. Br J Ophthalmol. 1997;81(8):622–623. | ||
Sharma N, Sachdev R, Jhanji V, Titiyal JS, Vajpayee RB. Therapeutic keratoplasty for microbial keratitis. Curr Opin Ophthalmol. 2010;21(4):293–300. | ||
Bajracharya L, Gurung R, Demarchis EH, Oliva M, Ruit S, Tabin G. Indications for keratoplasty in Nepal: 2005–2010. Nepal J Ophthalmol. 2013;5(2):207–214. | ||
Sony P, Sharma N, Vajpayee RB, Ray M. Therapeutic keratoplasty for infectious keratitis: a review of the literature. CLAO J. 2002;28(3):111–118. | ||
Sharma N, Jain M, Sehra SV, et al. Outcomes of therapeutic penetrating keratoplasty from a tertiary eye care centre in northern India. Cornea. 2014;33(2):114–118. | ||
Sedghipour MR, Sorkhabi R, Shenasi A, Dehghan H. Outcome of penetrating keratoplasty in corneal ulcer: a single-center experience. Clin Ophthalmol. 2011;5:1265–1268. | ||
Chen WL, Wu CY, Hu FR, Wang IJ. Therapeutic penetrating keratoplasty for microbial keratitis in Taiwan from 1987 to 2001. Am J Ophthalmol. 2004;137(4):736–743. | ||
Ti SE, Scott JA, Janardhanan P, Tan DT. Therapeutic keratoplasty for advanced suppurative keratitis. Am J Ophthalmol. 2007;143(5):755–762. | ||
Sukhija J, Jain AK. Outcome of therapeutic penetrating keratoplasty in infectious keratitis. Ophthalmic Surg Lasers Imaging. 2005;36(4):303–309. | ||
Feilmeier MR, Sivaraman KR, Oliva M, Tabin GC, Gurung R. Etiologic diagnosis of corneal ulceration at a tertiary eye center in Kathmandu, Nepal. Cornea. 2010;29(12):1380–1385. | ||
Upadhyay MP, Karmacharya PC, Koirala S, et al. Epidemiologic characteristics, predisposing factors, and etiologic diagnosis of corneal ulceration in Nepal. Am J Ophthalmol. 1991;111(1):92–99. | ||
Amatya R, Shrestha S, Khanal B, et al. Etiological agents of corneal ulcer: a five year prospective study in eastern Nepal. Nepal Med Coll J. 2012;14(3):219–222. | ||
Cristol SM, Alfonso EC, Guildford JH, Roussel TJ, Culbertson WW. Results of large penetrating keratoplasty in microbial keratitis. Cornea. 1996;15(6):571–576. | ||
Vajpayee RB, Sharma N, Sinha R, Agarwa T, Singhvi A. Infectious keratitis following keratoplasty. Surv Ophthalmol. 2007;52(1):1–12. | ||
Xie L, Dong X, Shi W. Treatment of fungal keratitis by penetrating keratoplasty. Br J Ophthalmol. 2001;85:10701074. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.