Back to Journals » Clinical Ophthalmology » Volume 20
Outcome of Botox Injection in Partially Accommodative Esotropia Compared to Medial Rectus Recession
Authors Alarfaj G ![]() , Alkharashi A, Aldofyan MZ, Alarfaj M
, Alkharashi A, Aldofyan MZ, Alarfaj M ![]() , Alkharashi M
, Alkharashi M
Received 24 March 2026
Accepted for publication 19 May 2026
Published 11 June 2026 Volume 2026:20 607367
DOI https://doi.org/10.2147/OPTH.S607367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Ghufran Alarfaj,1 Abdulmajeed Alkharashi,1 Munirah Z Aldofyan,1 Motazz Alarfaj,2 Maan Alkharashi1,3,4
1Department of Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2Department of Ophthalmology, College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 3Department of Ophthalmology, Boston Children’s Hospital, Boston, MA, USA; 4Department of Ophthalmology, Harvard Medical School, Boston, MA, USA
Correspondence: Ghufran Alarfaj, Department of Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia, Email [email protected]
Purpose: To compare the effectiveness of botulinum toxin (BTX) injection to bilateral medial rectus recession (BMR) in partially accommodative esotropia (PAET).
Methods: This retrospective study reviewed the medical records of 107 children younger than 15 years of age treated for PAET with BTX injection or bilateral medial rectus recession (BMR) surgery at a single institution between 2015 and 2022. PAET was defined as residual esotropia of at least 14 prism diopters (PD) after six weeks of continuous wear of full cycloplegic refraction. Primary success was defined as a distance alignment of ≤ 10 PD after a single treatment (BTX injection or BMR surgery). Secondary success was defined as achieving this alignment after repeated treatment.
Results: Of 107 patients, 51 received BTX injection and 56 underwent surgery. The surgery group had a significantly higher primary success rate (83.9%) than the BTX injection group (50.9%). No demographic factors correlated with treatment success. After repeat interventions, the cumulative success rate rose to 78.4% in the BTX injection group and 87.5% in the surgery group. Six patients (11.7%) in the BTX injection group eventually required surgical intervention. The complications rate was 4.8% in the BTX injection group (temporary ptosis covering visual axis), and 3.57% in the surgery group (consecutive exotropia necessitating medial rectus advancement).
Conclusion: Surgical intervention (BMR surgery) demonstrated significantly higher primary success rates for PAET than a single BTX injection. However, repeated BTX injections ultimately achieved comparable long-term success rates. While BTX offers less invasiveness and reduced anesthesia time, the potential need for multiple injections should be considered when counseling patients and their families.
Keywords: strabismus, esotropia, partially accommodative esotropia, botulinum toxin type A, bilateral medial rectus recession
Introduction
Strabismus has a global incidence of 1.3–5.7%1 and local incidence of 11.8% in Saudi Arabia.2 This increased local incidence could be attributed to the higher rate of consanguinity in the region.3 Esotropia is the most common type of strabismus that requires surgical intervention in Saudi Arabia (69.3%).4 Among the different types of esotropia in childhood, accommodative esotropia is considered the most common.5 Accommodative esotropia is further categorized into three main subtypes: refractive accommodative esotropia, partially accommodative esotropia (PAET) and non-refractive accommodative esotropia with a high accommodative convergence-to-accommodation (AC/A) ratio. In PAET, despite full cycloplegic correction with cycloplegic refraction, residual esotropia necessitates surgical intervention.6 However, challenges in obtaining accurate angle measurements due to factors such as limited patient cooperation and inconsistent compliance with glasses can hinder surgical decision making.7,8
Botulinum toxin type A, a neurotoxin produced by Clostridium botulinum, offers a less invasive alternative. This potent exotoxin temporarily weakens injected muscles while promoting contracture of the antagonist muscle.9–12 This study aims to evaluate the outcome of BTX injection (BOTOX®, Allergan, Inc., Irvine, CA) in patients with PAET, compared to bilateral medial rectus recession surgery and examining the concordance with previous local studies.
Subjects and Methods
This is a single-center, retrospective, nonrandomized controlled study approved by King Saud University Institutional Review Board with approval number E-25-9838 and adheres to the tenets of the Declaration of Helsinki. The parents or the legal guardians signed the informed consent.
The data were extracted from the electronic medical record system at King Abdulaziz University Hospital, a tertiary eye care center in Riyadh, Saudi Arabia. Data were extracted from January 2015 to December 2022. PAET was defined as residual angle of deviation of 14 prism diopters (PD) or more after six weeks of continuous full cycloplegic refraction, provided hyperopia exceeded +1.50 diopters. Patient demographic data included age at esotropia onset, extraocular muscle movements, preoperative and postoperative angles of deviation, spherical equivalent (SE), visual acuity, amblyopia, number of injections (BTX injection group), number of surgeries (BMR group), and complications. The preoperative angle of deviation was classified as small (≤ 25PD), medium (30PD to 45 PD), or large (> 45PD).
Patients with neurological disease, developmental delay, prior BTX injection or surgery, or were less than six months of follow-up were excluded. A six-month follow-up period ensured that any effects of BTX had dissipated.
The choice of intervention (BTX injection or bilateral medial rectus [BMR] surgery) was determined by physician preference. Specifically, some physicians performed only BMR surgery, using a hang-back technique in 19 patients and a modified hang-back technique in 37 patients, while others preferred BTX injection, which was administered via a transconjunctival approach in all cases. Primary success was defined as orthotropic or an angle of deviation ≤ 10 PD at least six months post primary intervention (single BTX injection or BMR surgery). Secondary success was achieving this angle after repeated BTX injections or additional BMR surgeries.
Statistical Analysis
The normality of data was assessed with Shapiro–Wilk Test. Normally distributed data were compared with independent-samples t-test while non-normally distributed data were compared with Mann–Whitney U-Test. Categorical data were compared with Pearson Chi-Square Test. The odds ratios with their p-values were calculated using binary logistic regression. The gathered data were analyzed using Statistical Package for the Social Sciences (SPSS 20.0) (IBM Corp., New York, USA). Results were considered statistically significant if P value <0.05.
Results
This retrospective study included 107 patients meeting the inclusion criteria: 51 received BTX injections and 56 underwent BMR surgery. Demographics and characteristics of patients in the BTX injection and BMR surgery groups are summarized and compared in Table 1. Statistically significant differences were observed between the two groups in age and angle of deviation, with the surgery group exhibiting both older age and larger angle of deviation (Figure 1). In both groups, the majority had medium angle of deviation.
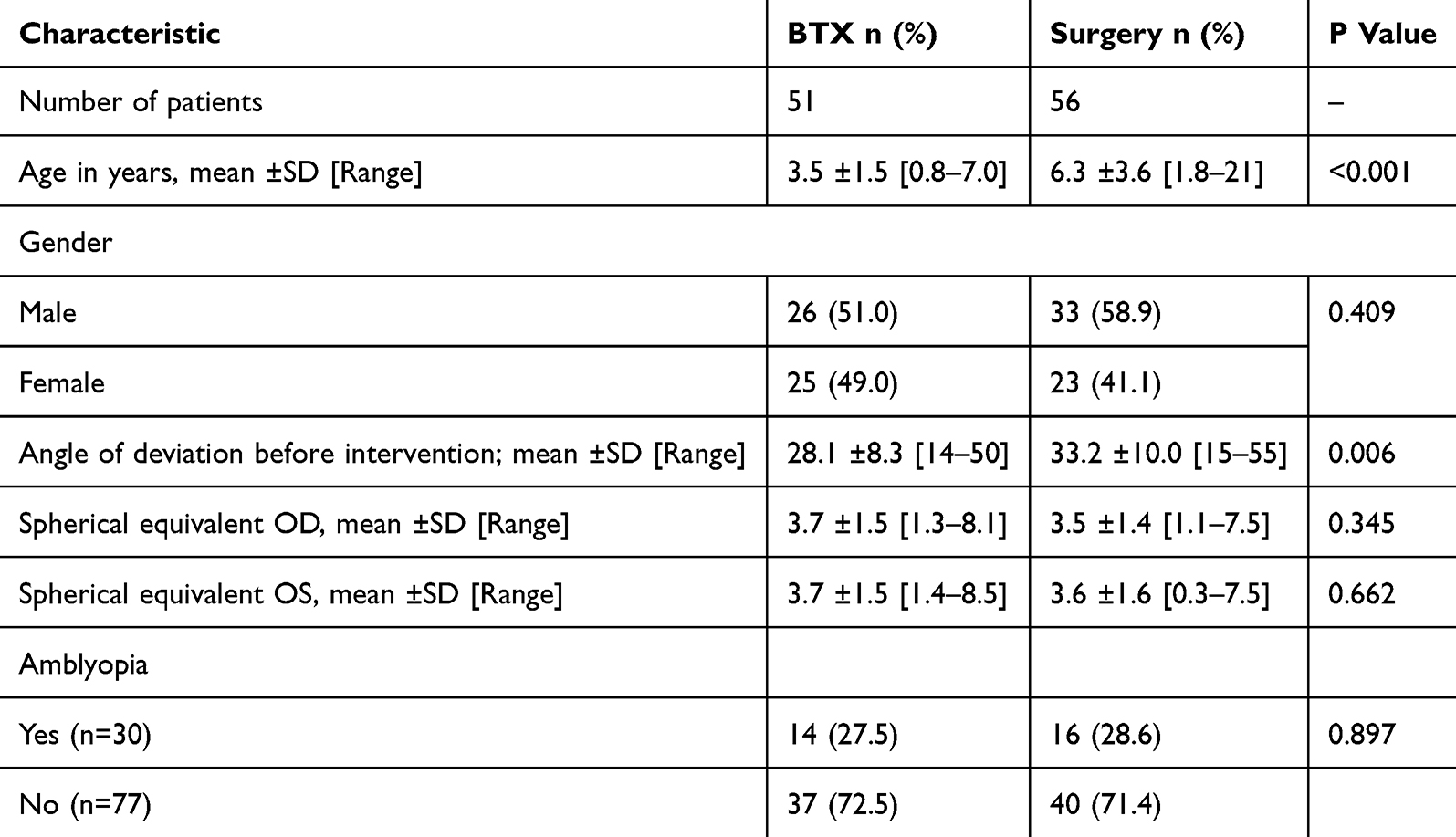 |
Table 1 Demographics and Clinical Characteristics of Patients in the BTX and Surgery Groups |
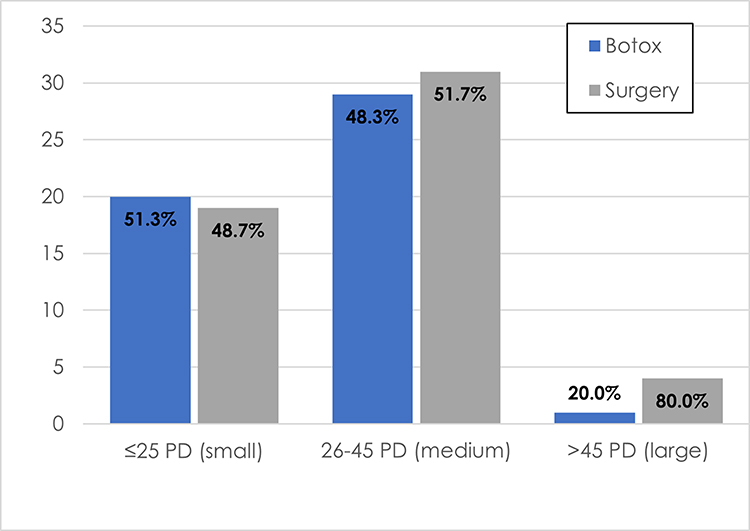 |
Figure 1 Distribution of patients in each group according to preoperative deviation. (small, ≤25 PD, medium, between 26 and 45 PD and large >45 PD) Y axis is the number of patients. |
Within the BTX injection group, 28 patients (56.0%) received 5 international units (IU) per medial rectus muscle, 21 patients (42.0%) received 7.5 IU, one patient received 3 IU, and dosage data were unavailable for one patient. The primary success rate (orthotropia or deviation ≤10 PD at six months post-treatment) was 26/51 (50.9%) in the BTX injection group and 47/56 (83.9%) in the surgery group, with a P value of <0.001. After repeat interventions, the cumulative success rate rose to 78.4% in the BTX injection group and 87.5% in the surgery group. Six patients (11.7%) in the BTX injection group eventually required surgical intervention (Figure 2).
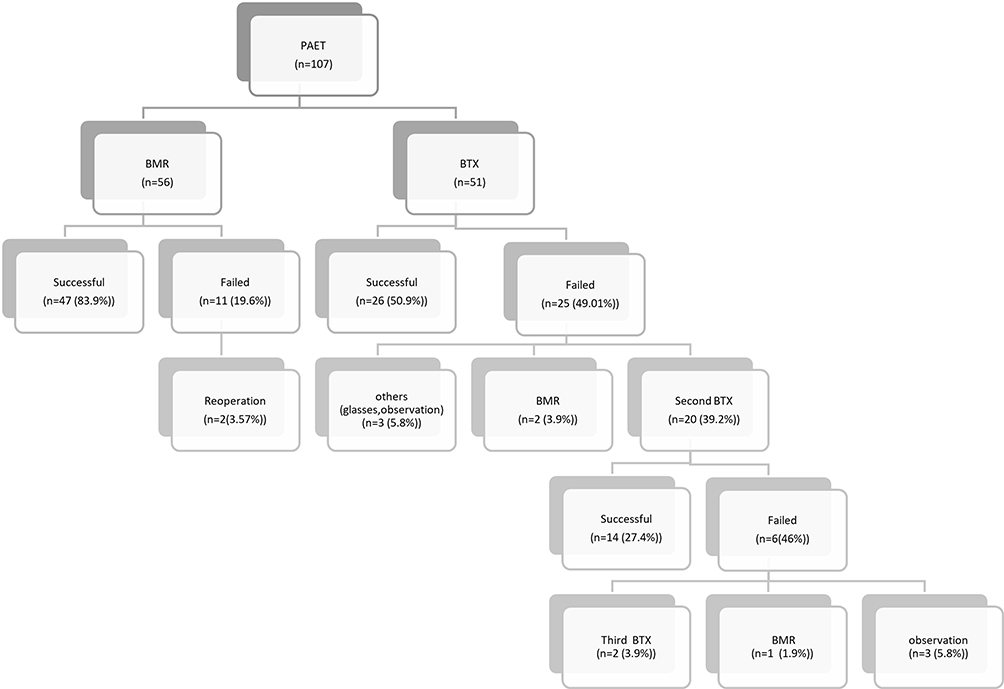 |
Figure 2 Distribution of patients in the study. Abbreviations: PAET, partially accommodative esotropia; BMR, bilateral medial rectus recession. |
Among those in BTX injection group, the majority of patients required one injection 35 (68.6%), 14 (27.5%) required two injections, and 2 (3.9%) required three injections.
The number of patients maintaining successful alignment increased with additional injections: 26 (50.9%) after the first injection, 39 (72.5%) after the second, and 40 (78.4%) after the third.
The overall median follow-up period was 18 months (range: 7–72 months). BTX injection group had a median follow-up of 24 months compared to 14 months in the surgery group.
The complication rate in the BTX injection group was 45%, consisting entirely of transient ptosis. However, it was visually significant, covering the visual axis, in only 3.92% of these cases. In contrast, surgery group had a complication rate of 7.1%, primarily due to consecutive exotropia or vertical deviations, necessitating medial rectus advancement in 2 patients (3.57%).
There was no significant association between BTX dose and success rate (P = 0.155). However, higher doses were significantly associated with an increased risk of ptosis (P = 0.008). Other factors such as age, initial angle of deviation, refractive error, or presence of amblyopia were not significantly associated with treatment failure or the need for additional BTX injections (P = 0.462, 0.594, 0.580, and 0.611, respectively).
Discussion
BTX injection offers several advantages over surgery, including shorter surgery time, reduced exposure to general anesthesia, and lower cost.13 However, success rates vary widely due to differences in sample sizes, follow-up durations, pre-treatment angles of deviation, and success criteria (Table 2). Notably, larger studies tend to report lower success rates.14,15
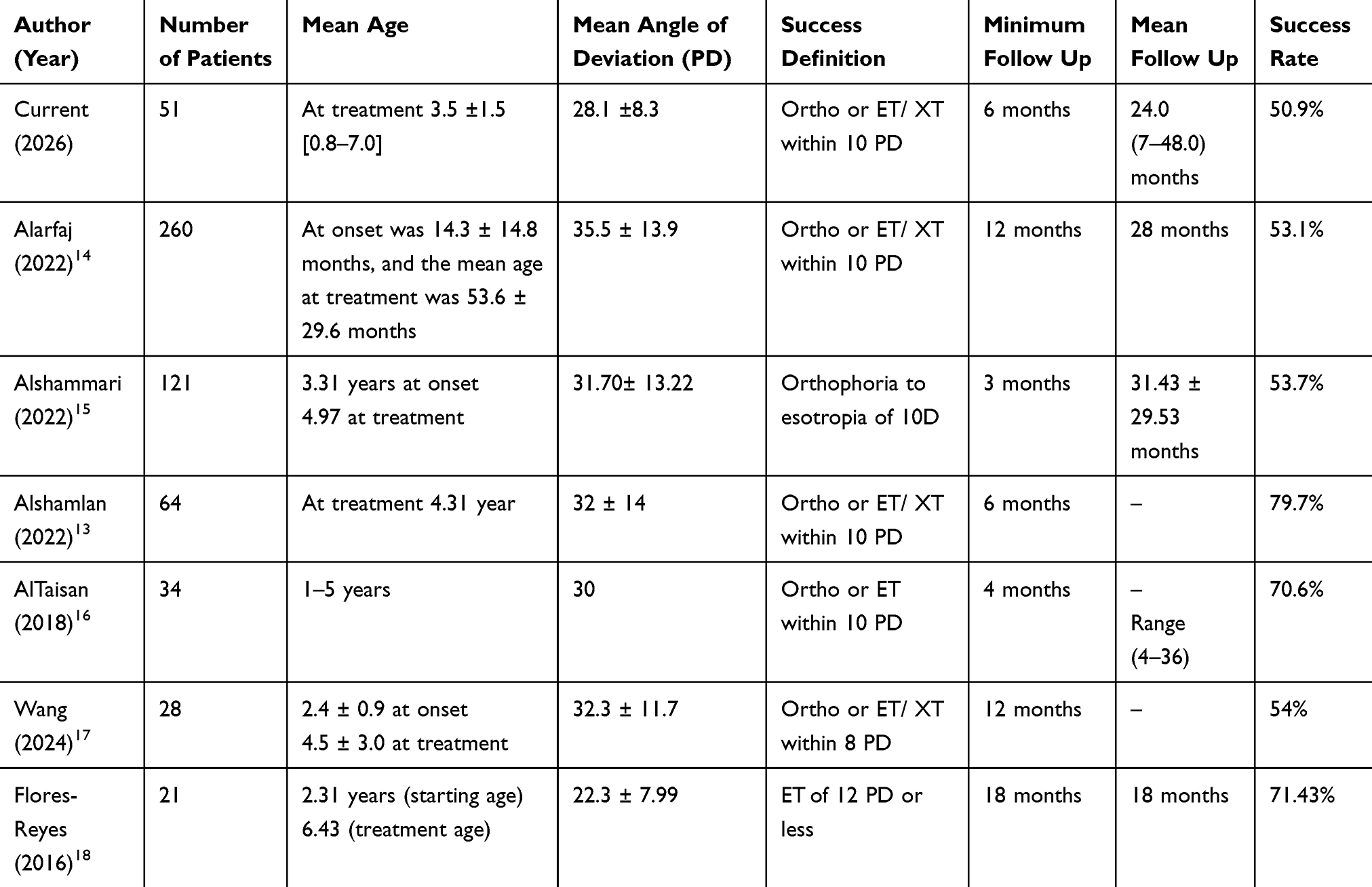 |
Table 2 Success Rate of Botox in PAET in Different Studies |
Contradictory outcomes have been reported in the literature when the success rate of BTX and surgery were compared in partially accommodative esotropia.
In our study, the primary success rate was 50.9% in the BTX injection group compared with 83.9% in the surgery group. This difference may be partly explained by the longer follow-up duration in the BTX group, which had a median follow-up of 24 months versus 14 months in the surgery group. The extended follow-up in the BTX group was necessary because these patients were younger and required closer monitoring for the potential development of amblyopia. With repeated interventions, success rates increased to 78.4% and 81.5% after repeated treatment, respectively. These results are consistent with previous studies. For example, AlShammari et al, reported primary success rates of 47% for the BTX injection group and 709% for the surgery group. Increasing slightly with repeat intervention to 53.7% and 70.9% in both groups, respectively.15
Similarly, a study with longer follow-up done in China by Wang et al, reported a success rate of 50% in the BTX injection group and 72–78% in the surgery group.17
The higher success rate with repeated BTX injections may reflect its use as a less invasive secondary treatment option, especially in younger patients where precise angle measurements for surgical planning can be challenging. Additionally, younger age is associated with improved sensory outcomes, and repeat BTX injections may have a cumulative therapeutic effect.19,20
These considerations align with findings from Scott et al, who reported that secondary injection success rate of 62% versus 35% for primary injections.20
Although BTX injections offer theoretical advantages, such as shorter procedure duration and reduced anesthesia time, these benefits may be offset by the need for repeated interventions. In our study, nearly one-third of patients in the BTX injection group required more than one injection to achieve satisfactory alignment, and 11.7% ultimately underwent surgery. This suggests that, in practice, children may be exposed to anesthesia multiple times, which diminishes the appeal of BTX injection as a less invasive option. Furthermore, while concerns have been raised about potential neurocognitive effects of early childhood anesthesia, repeated exposures may carry similar risks.17,21 Therefore, the decision to pursue BTX injection as a primary treatment should be made cautiously, especially considering the higher and more consistent success rate achieved with surgery after a single intervention.
Our analysis found no significant predictors of BTX treatment success, a finding consistent with studies by Al Taisan et al and Flores-Reyes et al16,18 In contrast, Alarfaj et al and Alshamlan et al, reported higher success rates in patients with smaller initial angles of deviation.13,14
A recent meta-analysis suggested that amblyopia may influence treatment outcomes in partially accommodative esotropia, as stable and symmetrical visual acuity may help maintain ocular alignment after treatment. This may have contributed to the poorer motor outcomes observed with BTX injection. Despite these findings, our analysis did not demonstrate a significant association between amblyopia and treatment failure. This discrepancy may be related to differences in amblyopia severity, treatment compliance, sample size, or the retrospective nature of the study, which may limit the ability to detect subtle associations.22
Regarding complications, our findings are consistent with previous studies showing that botulinum toxin (BTX)-related complications are typically mild and transient. In contrast, surgical intervention is associated with more serious complications, particularly consecutive exotropia, with reported rates ranging from 2–21%. In our cohort, 3.57% of surgical patients required further intervention to address this issue. It is important to note that these figures reflect early to moderate postoperative outcomes; the incidence of such complications is likely to increase with longer follow-up as additional cases become apparent.15,17,23,24
Limitations
The retrospective design of this study precluded randomization and may have introduced selection bias. Specifically, the surgical group had an older mean age and larger baseline deviation angles, and treatment allocation may have been influenced by physician preference. Additionally, binocular vision was not assessed either before or after the intervention.
Despite these limitations, the study has important strengths, including the evaluation of repeated BTX injections and the relatively long follow-up period.
Conclusion
This study demonstrates that surgical intervention resulted in significantly higher primary success rates for treating PAET compared to a single botulinum toxin injection. However, repeated Botox injections ultimately achieved comparable success rates to surgery. While Botox injections offer advantages of less invasiveness and reduced anesthesia time, the potential need for multiple injections should be carefully considered when counseling patients and their families regarding treatment options.
Abbreviations
BTX, botulinum toxin; BMR, bilateral medial rectus recession; PAET, partially accommodative esotropia; IU, international units; PD, prism diopters.
Acknowledgment
The authors would like to thank Priscilla Gikandi for her valuable assistance with the statistical analysis.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Multi-ethnic Pediatric Eye Disease Study Group. Prevalence of amblyopia and strabismus in African American and Hispanic children ages 6 to 72 months the multi-ethnic pediatric eye disease study. Ophthalmology. 2008;115(7):1229–1236.e1. PMID: 17953989; PMCID: PMC4839485. doi:10.1016/j.ophtha.2007.08.001
2. Danish EY, Shaikh RM, Hadrawi T. Pattern of pediatric eye diseases at King Fahad Armed Forces Hospital, Jeddah. Pak J Med Health Sci. 2015;9(3):945–7.
3. Alenezi HM, Abo El-Fetoh NM, Alruwaili AS, et al. Squint in children and adolescents, Arar, Northern Saudi Arabia. Egypt J Hosp Med. 2018;70:298–302. doi:10.12816/0043093
4. Curtis TH, McClatchey M, Wheeler DT. Epidemiology of surgical strabismus in Saudi Arabia. Ophthalmic Epidemiol. 2010;17:307–314. doi:10.3109/09286586.2010.508351
5. Greenberg AE, Mohney BG, Diehl NN, Burke JP. Incidence and types of childhood esotropia: a population-based study. Ophthalmology. 2007;114:170–174. doi:10.1016/j.ophtha.2006.05.072
6. Veneruso PE, Bruzzese D, Magli A. Long-term development of refractive error in refractive, nonrefractive and partially accommodative esotropia. PLoS One. 2018;13:e0204396. doi:10.1371/journal.pone.0204396
7. Pediatric Eye Disease Investigator Group. Inter-observer reliability of the prism and alternate cover test in children with esotropia. Arch Ophthalmol. 2009;127:59. doi:10.1001/archophthalmol.2008.548
8. Wangtiraumnuay N, Surukrattanaskul S, Surakiatchanukul T, Masaya-Anon P, Hiriotappa J. Outcomes of pediatric accommodative esotropia with botulinum toxin A treatment in Thailand. Strabismus. 2021;29:26–33. doi:10.1080/09273972.2020.1871379
9. Münchau A, Bhatia KP. Uses of botulinum toxin injection in medicine today. BMJ. 2000;320(7228):161–165. PMID: 10634738; PMCID: PMC1128745. doi:10.1136/bmj.320.7228.161
10. Ellenhorn MJ, Barceloux DG. Diagnosis and treatment of human poisoning. Med Toxicol. 1988:1185–1187.
11. Scott AB. Botulinum toxin injection into extraocular muscles as an alternative to strabismus surgery. Ophthalmology. 1980;87:1044–1049. doi:10.1016/S0161-6420(80)35127-0
12. Scott AB, Rosenbaum A, Collins CC. Pharmacologic weakening of extraocular muscles. Invest Ophthalmol. 1973;12(12):924–927. PMID: 4203467.
13. Alshamlan FT, Alghazal F. Comparison of dose increments of Botulinum Toxin A with surgery as primary treatment for infantile esotropia and partially accommodative esotropia. Clin Ophthalmol. 2022;16:2843–2849. doi:10.2147/OPTH.S382499
14. Alarfaj MA, Alsarhani WK, Alrashed SH, et al. Factors affecting the efficacy of botulinum toxin injection in the treatment of infantile and partially accommodative esotropia. Middle East Afr J Ophthalmol. 2022;29:122–126. doi:10.4103/meajo.meajo_39_23
15. AlShammari S, Alaam M, Alfreihi S. Conventional surgery versus botulinum toxin injections for partially accommodative esotropia. J Am Assoc Pediatr Ophthalmol Strabismus. 2022;26:16.e1–16.e6. doi:10.1016/j.jaapos.2021.08.308
16. Al Taisan AA, Al Shamlan FT, Al Mulhim AK, Alsomali AI, Al Owaifeer AM. Botulinum toxin; indications, success rates and complications in themanagement of horizontal strabismus in Saudi Arabia. J Clin Ophthalmol. 2018;2. doi:10.35841/clinical-ophthalmology.2.1.32-37
17. Wang Y, Jiang J, Li L. Long-term effects of botulinum Toxin A versus incisional surgery for management of partially accommodative esotropia in children: comparison of three approaches. Am J Ophthalmol. 2024;265:289–295. PMID: 38789085. doi:10.1016/j.ajo.2024.05.024
18. Flores-Reyes EM, Castillo-López MG, Toledo-Silva R, et al. Botulinum toxin type A as treatment of partially accommodative esotropia. Arch Soc Esp Oftalmol. 2016;91:120–124. doi:10.1016/j.oftal.2015.11.007
19. Keith W, McNeer KW, Tucker MG, Spencer RF. Botulinum toxin management of essential infantile esotropia in children. Arch Ophthalmol. 1997;115:1411–1418. doi:10.1001/archopht.1997.01100160581010
20. Scott AB, Magoon EH, McNeer KW, Stager DR. Botulinum treatment of childhood strabismus. Ophthalmology. 1990;97:1434–1438. doi:10.1016/S0161-6420(90)32390-4
21. Backeljauw B, Holland SK, Altaye M, et al. Cognition and brain structure following early childhood surgery with anesthesia. Pediatrics. 2015;136:e1–12. doi:10.1542/peds.2014-3526
22. Hira S, Avilés Covarrubias C, Bravo-Gonzalez A, de Menezes E Souza Filho CE, Tosato Zinher M. Botulinum Toxin A versus bilateral medial rectus recession for partially accommodative esotropia: a systematic review and meta-analysis. J Pediatr Ophthalmol Strabismus. 2025;62(5):314–320. PMID: 40135870. doi:10.3928/01913913-20250227-08
23. Ganesh A, Pirouznia S, Ganguly SS, Fagerholm P, Lithander J. Consecutive exotropia after surgical treatment of childhood esotropia: a 40-year follow-up study. Acta Ophthalmol. 2011;89(7):691–695. PMID: 19925519. doi:10.1111/j.1755-3768.2009.01791.x
24. Folk ER, Miller MT, Chapman L. Consecutive exotropia following surgery. Br J Ophthalmol. 1983;67(8):546–548. PMID: 6871147; PMCID: PMC1040117. doi:10.1136/bjo.67.8.546
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Surgical Outcomes and Factors Related to Their Success of Infantile Esotropia in a Tertiary Hospital: A Retrospective Study
Srimanan W
Clinical Ophthalmology 2024, 18:2627-2635
Published Date: 20 September 2024
Insidious Myopic Comitant Esotropia in a Teenager
Tangtammaruk P, Hieda O
International Medical Case Reports Journal 2024, 17:945-948
Published Date: 11 November 2024