Back to Journals » Clinical Ophthalmology » Volume 14
Outcome and Complications of Combined Modified Deep Sclerectomy and Trabeculectomy for Surgical Management of Glaucoma: A Pilot Study
Authors Sangtam T ![]() , Roy S, Mermoud A
, Roy S, Mermoud A
Received 6 January 2020
Accepted for publication 11 February 2020
Published 12 March 2020 Volume 2020:14 Pages 795—803
DOI https://doi.org/10.2147/OPTH.S244945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract of 'Combined mDST for glaucoma [ID 244945]'.
Views: 230
Tiakumzuk Sangtam,1,2 Sylvain Roy,1,3 André Mermoud1
1Glaucoma Center Montchoisi Clinic, Lausanne, Switzerland; 2Department of Ophthalmology & Visual Sciences, Khoo Teck Puat Hospital, Singapore; 3Laboratory of Hemodynamics and Cardiovascular Technology, Swiss Federal Institute of Technology, Lausanne, Switzerland
Correspondence: Tiakumzuk Sangtam Email [email protected]
Purpose: To report the outcome and complications of a combined surgical technique of modified deep sclerectomy and trabeculectomy (mDST) for glaucoma.
Patients and Methods: Retrospective study of 44 eyes of 43 patients with open and closed angle glaucoma who underwent mDST. Outcome measures were: Surgical Success with 3 criteria - (i) criterion 1 = intraocular pressure (IOP) ≤ 21 mmHg or reduced by ≥ 20% of pre-operative IOP or IOP ≥ 6 mmHg on 2 consecutive time points after 3 months; (ii) criterion 2 = IOP ≤ 18 mmHg or reduced by ≥ 30% of pre-operative IOP or IOP ≥ 6 mmHg on 2 consecutive time points after 3 months and (iii) criterion 3 = IOP ≤ 15 mmHg or reduced by ≥ 40% of pre-operative IOP or IOP ≥ 6 mmHg on 2 consecutive time points after 3 months; IOP Reduction; Use of Anti-glaucoma Medication; Complications; Visual Acuity and Postoperative Interventions.
Results: Median follow-up was 40 months (range 24– 77 months). At the final follow-up visit, the mean postoperative IOP was 11.5 ± 4.7 mmHg (p< 0.0001). Mean number of anti-glaucoma medications decreased from 2.45 ± 1.21 to 0.54 ± 0.95 (p< 0.0001). Surgical success in terms of IOP reduction was 50%; 43.2%; 36.4% for the 3 criteria respectively (complete success) and 70.5%; 56.8%; 47.7% for the 3 criteria respectively (qualified success). The complications noted were shallow/flat anterior chamber in 2 (4.54%), hyphema & bleb leak in 3 (6.81%), aqueous misdirection in 1 (2.27%), hypotonic maculopathy in 2 (4.45%) and hypotony requiring intervention in 6 (13.63%) eyes.
Conclusion: Combined mDST was found to be an effective surgical procedure in reducing IOP. It was associated with complications commonly encountered in glaucoma filtering surgery. The use of intra-scleral space maintainer may help lower the risk of flat or shallow anterior chamber during the early postoperative period.
Keywords: outcome and complications, combined modified deep sclerectomy and trabeculectomy
Introduction
Trabeculectomy was introduced in 1968 by Cairns1 that has become the most commonly performed surgery for glaucoma management.2 The initiation of anti-fibrotic usage improved surgical results.3,4 However, this was associated with significant complications including hypotony and endophthalmitis.5 In an attempt to reduce complications associated with trabeculectomy, non-penetrating deep sclerectomy (NPDS) - by creating an intact trabeculo-Descemetic membrane (TDM) - was popularized as an alternative procedure in the late eighties by Fyodorov and Kozlov.6,7 NPDS also provides additional aqueous drainage pathways through the intra-scleral lake and suprachoroidal space.8,9 Nonetheless, a recent meta-analysis10 showed NPDS to be less effective in reducing IOP than trabeculectomy for patients with open-angle glaucoma. Moreover, NPDS is a technically more challenging procedure to perform than trabeculectomy. The quest for better and safer surgical techniques continues. We are interested to know whether combining two surgical procedures could provide certain benefits. Herein, we report a pilot study on the surgical outcome and complications of a novel technique combining modified deep sclerectomy and trabeculectomy (mDST) for surgical treatment of glaucoma.
Patients and Methods
Patients
Patients who underwent mDST from 2007 to 2012 in Glaucoma Center Montchoisi Clinic, Lausanne, Switzerland were included. Eligibility criteria were: (1) Age ≥ 21 years (2) Diagnosis of primary or secondary open and closed angle glaucoma (3) Minimum of 2 years follow-up. Informed written consents were obtained before surgery from all the patients and the study was approved by Institutional Review Board and adhered to the tenets of the Declaration of Helsinki.
Pre-Operative Data
Pre-operative data consisted of patient demographics, the Snellen distance best-corrected visual acuity (BCVA), the highest intraocular pressure (IOP) before surgery measured using a Goldmann applanation tonometer, the number of IOP-lowering medications used at the time of listing for surgery. For patients using topical combinations, the medications were counted according to the number of active drugs. If systemic acetazolamide was used, it was counted as one drug.
Operative Procedures
One experienced surgeon (AM) performed all the surgeries under retrobulbar anesthesia. A superior corneal traction suture (6–0 Silk, Alcon® Inc) was applied to mobilize the globe for better exposure of the surgical site. Employing a fornix-based approach, limbal peritomy was made for about 3–4 clock hours followed by a proper dissection under the conjunctiva and Tenon’s capsule to create a sub-Tenon pouch. Hemostasis was maintained using a mild wet field bipolar cautery. Polyvinyl alcohol sponges soaked in 0.2 mg/mL Mitomycin-C (MMC) were placed in the pouch, the duration of application depended on the age of the patient and the status of the conjunctiva. The pouch was then thoroughly irrigated with 20 to 30 mL of balanced salt solution. A 5x5 mm limbus-based scleral incision was made and a superficial flap of about one-third scleral thickness was fashioned using Crystal-Red sclerectomy knife (Huco® Vision Switzerland). The dissection of the superficial flap was extended 1 mm further into the clear cornea. A deeper scleral incision of 4x5 mm with a margin of 0.5 mm on each side was made with a 25° Diamond knife (Huco® Vision Switzerland) that was dissected leaving only a very thin layer of deep sclera over the uveal tissue. The deeper dissection was also carefully extended onto the clear corneal stroma to expose the TDM, then the deeper scleral flap was excised. Thereafter, the TDM was punctured and partially excised followed by iridectomy. Intra-operative materials were placed under the flap to act as a space maintainer and offer some resistance to the aqueous flow. The flap was then secured using 10–0 Nylon (Mani® Inc. Japan) with several interrupted sutures to achieve only minimal aqueous ooze. The conjunctiva and Tenon’s capsule were closed watertight with one or two running 8–0 Polysorb (Covidien™ USA).
Intra-Operative Materials
Different intra-scleral space maintainer used were ophthalmic viscoelastic devices (OVD) such as HealaFlow® (2.25% cross-linked sodium hyaluronate), Healon® (1% sodium hyaluronate) and collagen implants such as Aquaflow® (lyophilized porcine scleral collagen), Ologen® (cross-linked lyophilized porcine type I atelocollagen and glycosaminoglycans). The selection for the type of space maintainer was based on the experience and at the discretion of the surgeon (AM).
Perioperative Data
The perioperative data obtained were the concentration and duration of MMC application, the type of space maintainer used, the type and method of sutures used to close the scleral flap and the type of anesthesia. Any perioperative complications were noted.
Post-Operative Follow-Up
Post-operative data included IOP, BCVA and use of IOP lowering medication at 1 day, 1 month, 3 months, 6 months, 12 months, 2 years, and yearly thereafter. Post-operative complications such as bleb leak, hyphema, flat/shallow anterior chamber, hypotony, choroidal detachment, hypotonic maculopathy, encysted bleb, blebitis, endophthalmitis or others (described in free text) were recorded. Any post-operative interventions such as ocular massage, injection of OVD, conjunctiva re-suturing, needling, antimetabolite injection, compression sutures, autologous blood injection, revision for hypotony, and others (described in free text) were also noted.
Outcomes
The outcome measures were based on the outcome criteria proposed in the World Glaucoma Association Guidelines.11 The main outcome measure was the rate of success as defined by the following criteria: (i) criterion 1 = IOP ≤21 mmHg or reduced by ≥20% of pre-operative IOP or IOP ≥6 mmHg on 2 consecutive time points after 3 months; (ii) criterion 2 = IOP ≤18 mmHg or reduced by ≥30% of pre-operative IOP or IOP ≥6 mmHg on 2 consecutive time points after 3 months and (iii) criterion 3 = IOP ≤15 mmHg or reduced by ≥40% of pre-operative IOP or IOP ≥6 mmHg on 2 consecutive time points after 3 months. A minimum follow-up of 2 years was included. Surgical success was categorized according to IOP control and the percentage of IOP reduction as detailed above. Due to the retrospective nature of this study, a single IOP measurement was used. Success was further characterized as complete success for those without ocular hypotensive medications and qualified success with ocular hypotensive medications. Failure was defined as (1) IOP measured above the upper limit or below the lower limit (6 mmHg) on 2 consecutive follow-up visits after 3 months (the second consecutive visit was counted as the time of failure). (2) Repeat glaucoma surgery. (3) Loss of light perception vision. However, the use of sub-conjunctival antimetabolite injection, bleb needling, and re-suturing or surgical revision for hypotony was not counted as failures.
Statistical Analysis
Data were recorded as mean values ± standard deviation (SD) and ranges (minimum to maximum). Kaplan-Meier survival curve was used to analyze the cumulative probability of success. Student’s paired t-test was used to assess differences in quantitative variables before and after surgery. A p-value of <0.05 was considered statistically significant. The data were analyzed using Microsoft Office: mac Excel 2011 and TIBCO Spotfire SPlus 8.1 software.
Results
Patient Demographics
There were a total of 44 eyes from 43 patients with 26 females and 17 males. The mean age was 69 ± 12 years (range 35–92). The median follow-up was 40 months (range 24–77 months). The demographics of the overall data are shown in Table 1.
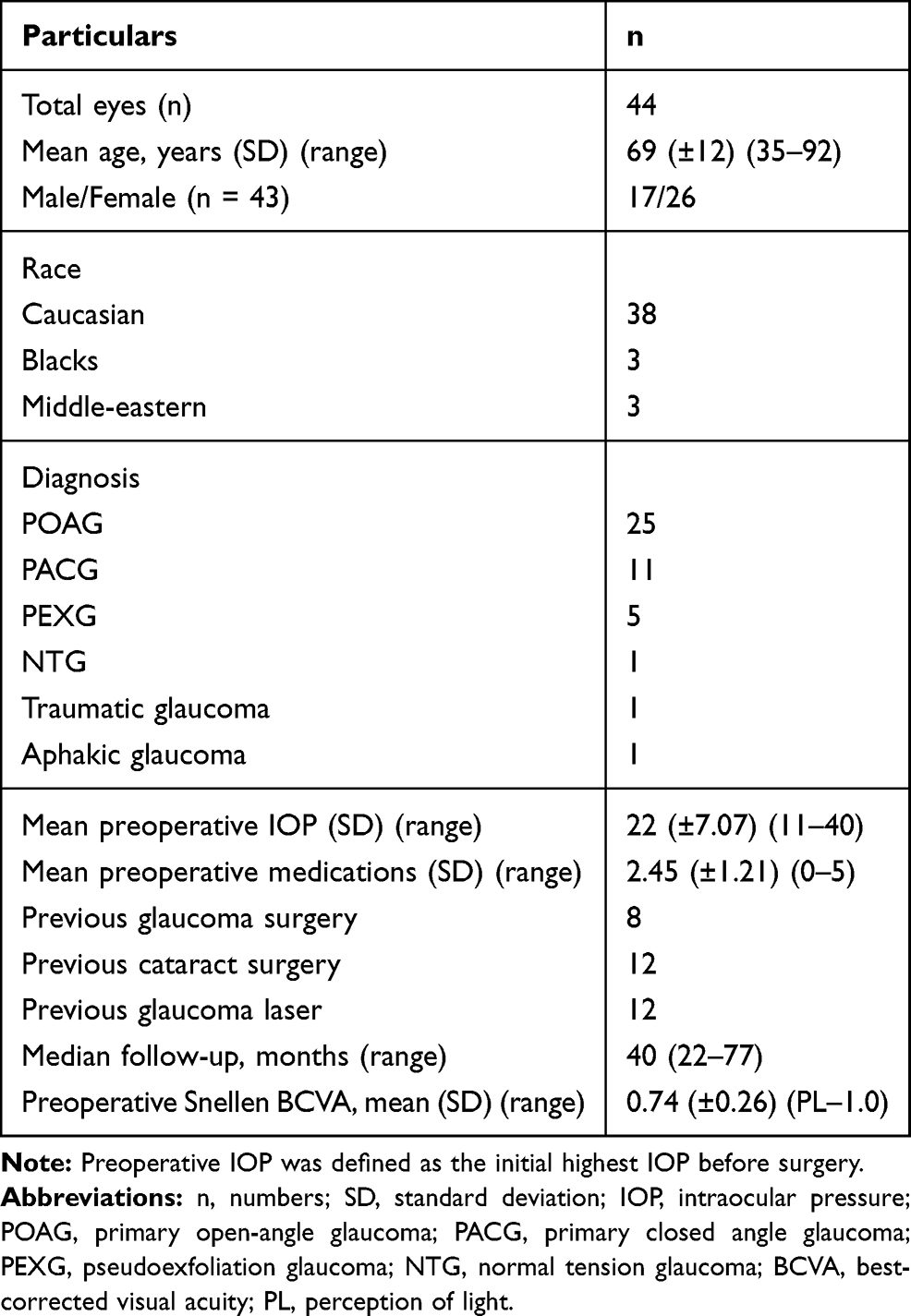 |
Table 1 Patient Demographics |
Thirty-eight (86.4%) eyes received MMC except 1 (2.3%) who did not get any type of antimetabolite. The concentration of MMC was 0.2mg/mL having a mean exposure time of 1.55 ± 0.82 mins. The application of the first sponge was counted as the start of MMC exposure time. There was no information on antimetabolite use in 5 (11.4%) eyes.
Thirty-two (72.7%) eyes received 2.25% cross-linked sodium hyaluronate, 6 (13.6%) eyes received 1% sodium hyaluronate, 2 (4.5%) eyes received lyophilized porcine scleral collagen, 1 (2.3%) eye received 2.25% cross-linked sodium hyaluronate + lyophilized porcine scleral collagen, and 1 (2.3%) eye received cross-linked lyophilized porcine type I atelocollagen and glycosaminoglycans. Two (4.5%) eyes did not receive any intra-scleral space maintainer.
For all eyes having a scleral flap closed with interrupted Nylon® suture, 16 (36.4%) eyes had 8 sutures, 14 (31.8%) had 6 sutures, 5 (11.4%) had 9 sutures, 3 (6.8%) had 7 sutures, 2 (4.5%) had 10 sutures, 1 (2.3%) had 2 sutures, 1 (2.3%) had 4 sutures, 1 (2.3%) had 12 sutures and 1 (2.3%) had 8 sutures plus 1 additional releasable suture. None of the eyes had any adjustable sutures.
Intraocular Pressure & Anti-Glaucoma Medications
The mean pre-operative IOP was 22.0 ± 7.1 mmHg (range 11–40). Forty-two (95.5%) eyes were on anti-glaucoma medications before the surgery. The mean pre-operative number of anti-glaucoma medications was 2.45 ± 1.21 (range 0–5). At the final follow-up visit, the mean IOP was 11.5 ± 4.7 mmHg (range 3–25), representing a decrease of 10.5 mmHg (- 47.9%; p<0.0001) between the pre-operative and post-operative IOP. The IOP outcome of eyes at the final follow-up is given in Table 2. The Kaplan-Meier survival curve for the eyes achieving IOP < 21 mmHg and 20% pre-operative IOP is shown in Figure 1. The mean IOP of eyes over time is depicted as a box-and-whisker plot in Figure 2. A scatter plot comparing pre-operative IOP and post-operative IOP is shown in Figure 3. The mean number of anti-glaucoma medications per patient decreased from 2.45 ± 1.21 to 0.54 ± 0.95 (range 0–3; p<0.0001) at the final follow-up visit. Thirteen eyes (29.5%) required 1–3 anti-glaucoma medications to control IOP (Figure 4).
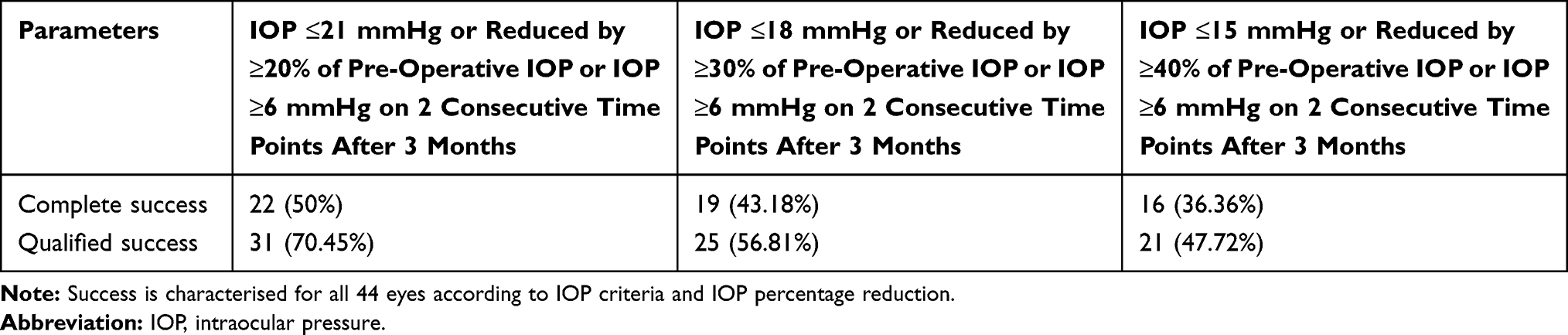 |
Table 2 Outcomes for Success at the Final Follow-Up |
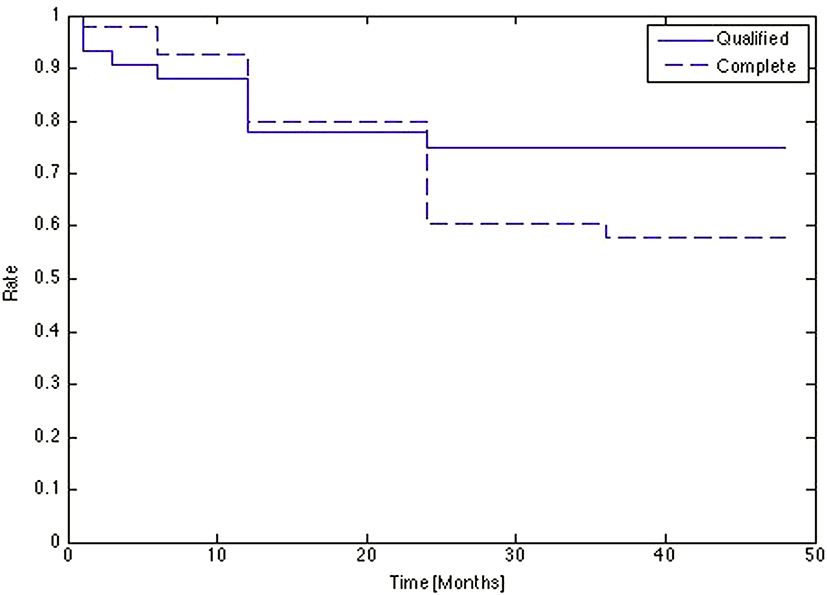 |
Figure 1 Kaplan-Meier survival curve showing the cumulative probability of success at 48 months follow-up. |
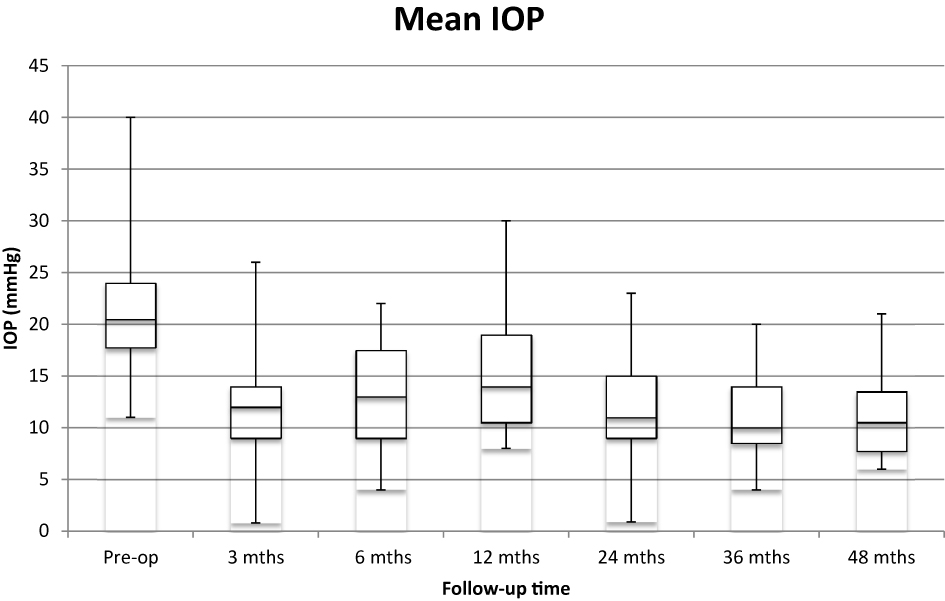 |
Figure 2 Box-and-whisker plot showing the changes in mean IOP over time post-operatively. |
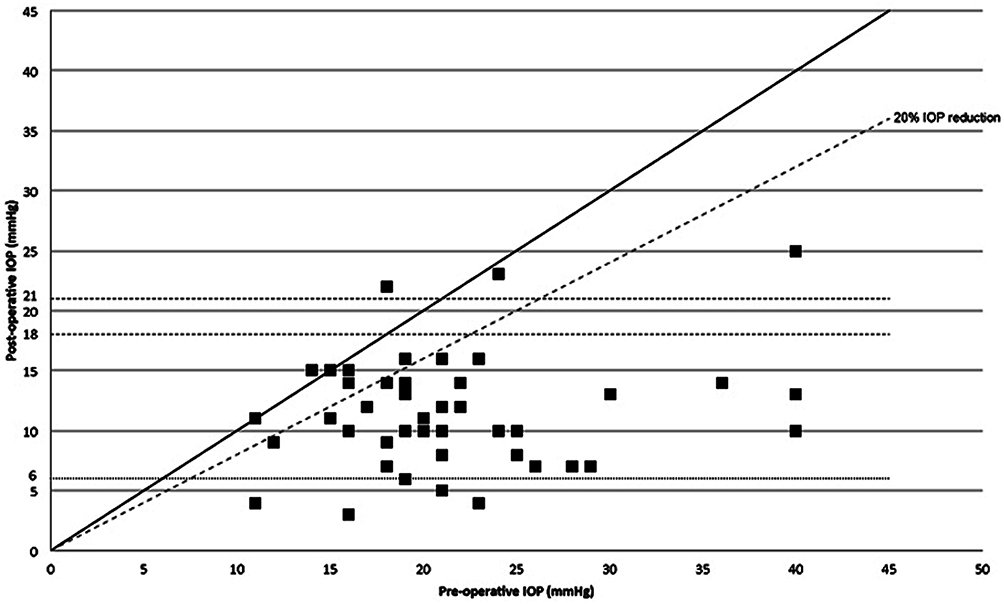 |
Figure 3 Scatter graph of pre-operative versus post-operative IOP. |
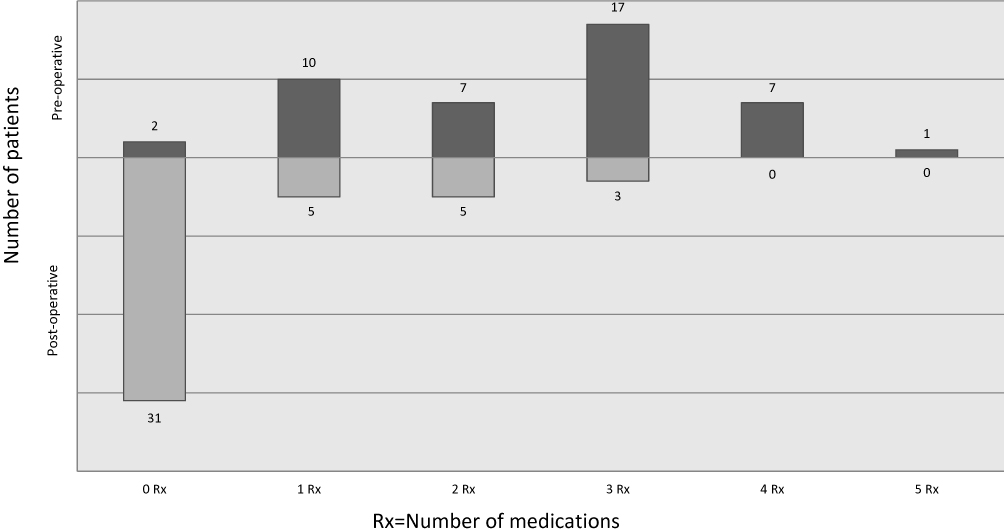 |
Figure 4 Graph showing number of anti-glaucoma medications per patient before and after surgery. |
There were a total of 27 (61.4%) eyes that had pre-operative IOP <22 mmHg. At the final follow-up, 20 (74.1%) of these eyes had an IOP reduction of ≥20% or more and 14 (51.9%) had IOP reduction of ≥30% or more. Eight out of the total 27 (29.6%) eyes required hypotensive medication. There were 3 (11.1%) eyes with IOP of <6 mmHg.
Visual Acuity
The mean post-operative Snellen BCVA was 0.73 ± 0.24. Twenty-seven (61.4%) eyes had BCVA within 2 lines of pre-operative visual acuity. Thirteen (29.5%) eyes had a loss in BCVA. Out of which 6 (46.2%) eyes had ≥3 lines loss, 3 (50%) of them had advanced glaucomatous optic neuropathy (GON). Mean number of Snellen lines loss was 0.26 ± 0.16. Ten (22.7%) had an improvement in BCVA, of which 4 (40%) had ≥3 lines improvement. None of the patients lost perception of light vision.
Complications
Intra-operative and postoperative complications are shown in Table 3. One (2.3%) eye required revision for early hypotony (within 3 months). Five (11.4%) had late-onset hypotony between 7 months and the final follow-up that required surgical bleb revision. Four (9.1%) had an IOP ≤5 mmHg at the final follow-up. Two of these 4 eyes lost ≥4 lines in Snellen BCVA, both of which had a pre-existing advanced GON. Three (6.8%) eyes had hyphema on the first post-operative day that resolved within 1 month. No intraoperative hyphema was encountered. Three (6.8%) eyes had bleb leaks, 2 of them occurred within 1 month after surgery and both were sutured. The last one had late-onset (60 months) leak from ischemic/avascular bleb that required bleb revision surgery.
 |
Table 3 Complications: Intraoperative & Post-Operative |
Interventions
Post-operative interventions administered from surgery to the final follow-up are shown in Table 4. Bleb needling with MMC injection was done in 22 (50%) eyes. Out of which, 16 (72.7%) eyes received it within the first 6 months. Three vitrectomies were performed (1 for aqueous misdirection, 1 for epiretinal membrane and the last 1 for cataract surgery complication – posterior capsule rupture).
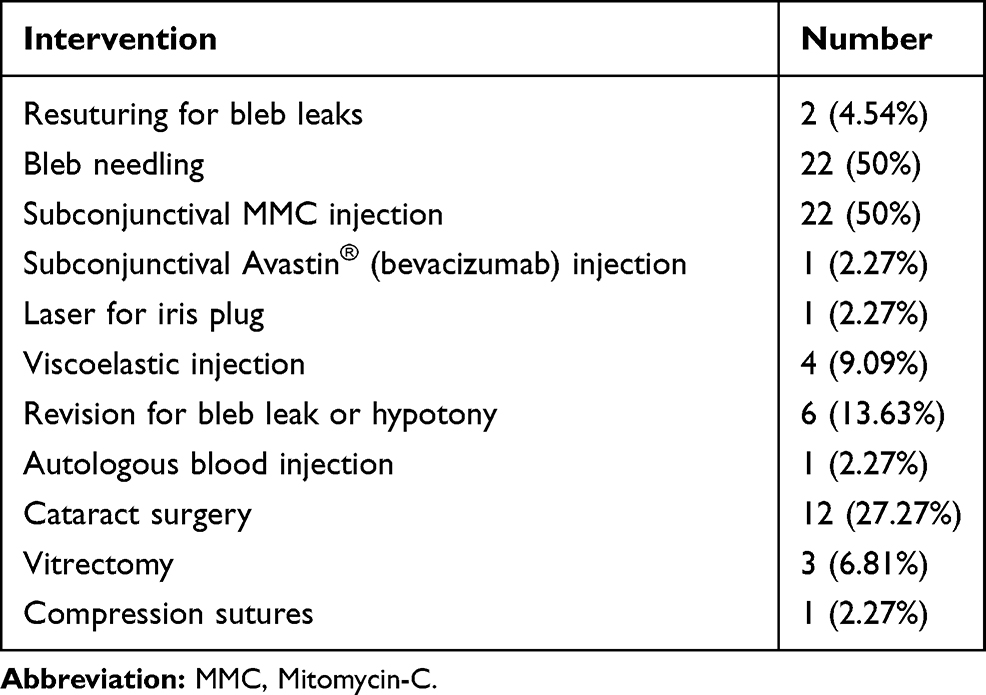 |
Table 4 Post-Operative Interventions |
Discussion
This study shows that combined mDST is an effective surgical option to reduce IOP in the management of glaucoma. The combined surgery was performed in patients with different types of glaucoma including primary open-angle glaucoma, pseudoexfoliation glaucoma, angle-closure glaucoma, traumatic and aphakic glaucoma with a follow-up of a minimum 24 months. As alluded to earlier, trabeculectomy is the most effective surgical procedure for reducing IOP in patients with open-angle glaucoma. However, it was associated with a higher incidence of complications when compared with NPDS.10,12–14 Combining these two surgical procedures appears to provide a comparable result to trabeculectomy in terms of IOP reduction but with a relatively fewer rate of flat or shallow anterior chamber when paralleled retrospectively to published results.
The goal for any glaucoma therapy is the prevention of further glaucomatous optic nerve damage and visual field loss with preservation of visual function. At present, the lowering of IOP remains the only means to achieve this goal. Hence, the most useful measure of the effect of glaucoma surgery is a reduction in IOP. In the present study, the mean postoperative IOP at the final follow-up visits was 11.5 ± 4.7 mmHg, which is comparable to other studies having 13.3 ± 6.8 mmHg15 and 11.4 ± 6.0 mmHg16 after trabeculectomy. The surgical success in terms of IOP reduction achieved in our study was 50% for criterion 1; 43.2% for criterion 2; 36.4% for criterion 3 (complete success) and 70.5% for criterion 1; 56.8% for criterion 2; 47.7% for criterion 3 (qualified success). On comparing our results to trabeculectomy, a more reasonable candidate would be the Tube Versus Trabeculectomy (TVT)15 study, which had a similar diagnosis profile and criteria for surgical success. In the trabeculectomy arm of TVT, 40% had complete success and 26% had qualified success in 3 years follow-up compared to 50% of complete success and 70.45% of qualified success at the final follow-up in the present study. In studies comparing NPDS to trabeculectomy, the reported complete success rate varied from 40% to 79% in NPDS versus 45% to 92.6% in trabeculectomy and the qualified success rate varied from 76.5% to 95% in NPDS versus 88.9% to 95% in trabeculectomy.12–14,17–19 It is difficult to compare different studies and surgical techniques with dissimilar success criteria and diagnosis profile. However, one must remember that all the patients in other studies reported had common features of open-angle glaucoma, underwent primary surgery (no previous glaucoma surgery) and varied follow-up periods ranging from 12 months to 48 months. On the other hand, our study had a mixed diagnosis of glaucoma with a follow-up of minimum 24 months. Besides, we had 8 (18.2%) eyes with previously failed glaucoma surgeries after undergoing deep sclerectomy and Ex-PRESS® glaucoma filtration device (Alcon®). Moreover, the success criteria used in the other studies were different from the current study having more rigorous criteria incorporating both IOP value and percentage reduction. These factors might explain the differences in results seen between our current report and the reports mentioned above.
Two previous studies20,21 of combined deep sclerectomy and trabeculectomy have reported a complete success rate of 83.3% to 92.2%. However, it should be noted that all their patients underwent primary glaucoma surgery, had a smaller sample (12 and 31 eyes respectively) of solely open-angle glaucoma, and had dissimilar surgical technique and success criteria with one21 of the studies having only 8 (25.8%) eyes by the 12-month follow-up and 13 (41.9%) eyes requiring post-operative medications. Furthermore, the follow-up period was shorter having a mean duration of 8.3 to 12 months. It must be pointed out that mean duration of 12 months follow-up is comparatively shorter when it is known for success rate to decline with time after filtering surgery.22–24 Higher rates of shallow anterior chamber were reported in 13%20,21 compared with 4.5% in our current study. Similarly, 13%20,21 of choroidal detachment was seen compared to nil in our study.
The number of post-operative medications in other studies mentioned earlier ranged from 0.30 ± 0.40 to 1.0 ± 1.0 in NPDS and 0.27 ± 0.5 to 1.2 ± 1.1 in trabeculectomy. In our study, it was 0.54 ± 0.95 which is comparable and lesser than some of the studies mentioned above.
Although NPDS studies did not report any occurrence of flat or shallow anterior chamber, trabeculectomy had a high rate varying from 7.7% to 33.3%.12–15,17 The incidence was much lower (4.5%) in our study. A possible explanation for this lower figure could be due to the use of several intra-scleral space-occupying materials along with the application of multiple interrupted sutures to the scleral flap that provided suitable resistance to the aqueous flow. Furthermore, we did not encounter any eye with choroidal detachment (0%) when compared to previous reports of 0% to 5% in NPDS12,14 and 3% to 30% in trabeculectomy.14,15 Bleb leak was seen in 6.81% in our study, which is comparable to other studies reporting 2.6 to 12% in NPDS13,18 and 7 to 12% in trabeculectomy.12,18
Hyphema was seen in 6.81% in our study compared with 2 to 15% in NPDS12,14 and 7.7 to 41% in trabeculectomy.13,18 This lower rate could be possibly related to surgical technique and location of anterior chamber entry and iridectomy.
Hypotonic maculopathy was seen in 4.5% and aqueous misdirection was seen in 1 eye in our study, which is comparable to 4% and 1 eye respectively in TVT15 study (trabeculectomy arm). The rate of hypotony was 13.6%, which is slightly higher than NPDS (10%)14 but lower than trabeculectomy (2.6 to 27.8%).13,17
There were frequent post-operative interventions in the current study where 50% had bleb needling done when there were signs of bleb failure as evidenced by increased bleb vascularity with progressive IOP elevation or bleb encapsulation. Overall 13.6% underwent revision for bleb leak or hypotony. These figures possibly reflect our aggressive and proactive post-operative management in the pursuit of achieving target IOP for each patient.
Fortunately, none of the eyes in our study experienced serious sight-threatening complications such as endophthalmitis compared with 3% (trabeculectomy group) in TVT study15 during the post-operative follow-up ranging from 24–77 months.
The current report has limitations inherent in a retrospective study with a potential loss to follow-up, smaller sample size, non-controlled use of intrascleral space maintainer and that the data relied on past clinical notes. However, it gives us an insight into the ground realities of what could be achieved in our clinical practice with this technique. Moreover, this mDST can be useful to those surgeons who are learning to perform NPDS and transitioning from trabeculectomy to NPDS. Should inadvertent perforation of TDM occur during their NPDS procedure, the surgeon would be able to simply convert the NPDS to mDST.
Conclusions
Combined mDST is a viable and effective procedure in the surgical reduction of IOP with associated complications commonly seen in glaucoma filtering surgery. The use of intra-scleral space maintainer may help provide resistance and modulate aqueous flow that could lower the risk of flat or shallow anterior chamber during the early postoperative period. Further prospective controlled randomized study comparing trabeculectomy with mDST may be worthwhile to determine its true place in terms of its effectiveness and safety in the armamentarium of glaucoma surgical procedures.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cairns JE. Trabeculectomy. Preliminary report of a new method. Am J Ophthalmol. 1968;66:673–679. doi:10.1016/0002-9394(68)91288-9
2. Ramulu PY, Corcoran KJ, Corcoran SL, Robin AL. Utilization of various glaucoma surgeries and procedures in Medi-care beneficiaries from 1995 to 2004. Ophthalmology. 2007;114:2265–2270. doi:10.1016/j.ophtha.2007.02.005
3. Chen CW, Huang HT, Bair JS, Lee CC. Trabeculectomy with simultaneous topical application of mitomycin-C in refractory glaucoma. J Ocul Pharmacol. 1990;6:175–182. doi:10.1089/jop.1990.6.175
4. Rothman RF, Liebmann JM, Ritch R. Low-dose 5-fluorouracil trabeculectomy as initial surgery in uncomplicated glaucoma: long-term follow-up. Ophthalmology. 2000;107:1184–1190. doi:10.1016/S0161-6420(00)00085-3
5. DeBry PW, Perkins TW, Heatley G, et al. Incidence of late- onset bleb-related complications following trabeculectomy with mitomycin. Arch Ophthalmol. 2002;120:297–300. doi:10.1001/archopht.120.3.297
6. Fyodorov SN. Non-penetrating deep sclerectomy in open angle glaucoma [in Russian]. Eye Microsurg. 1989;1:52–55.
7. Kozlov VI, Bagrov SN, Anisimova SY, et al. Deep sclerectomy with collagen [in Russian]. Eye Microsurg. 1990;3:44–46.
8. Chiou AGY, Mermoud A, Underdahl JP, Schnyder CC. An ultrasound biomicroscopic study of eyes after deep sclerectomy with collagen implant. Ophthalmology. 1998;105:746–750. doi:10.1016/S0161-6420(98)94033-7
9. Kazakova D, Roters S, Schnyder CC, et al. Ultrasound biomicroscopy images: long-term results after deep sclerectomy with collagen implant. Graefe’s Arch Clin Exp Ophthalmol. 2002;240:918–923. doi:10.1007/s00417-002-0567-7
10. Rulli E, Biagioli E, Riva I, et al. Efficacy and safety of trabeculectomy vs nonpenetrating surgical procedures: a systematic review and meta-analysis. JAMA Ophthalmol. 2013;131:1573–1582. doi:10.1001/jamaophthalmol.2013.5059
11. Heuer DK, Barton K, Grehn F, et al. Consensus on definitions of success. In: Shaarawy TM, Sherwood MB, Grehn F, editors. World Glaucoma Association Guidelines on Design and Reporting of Glaucoma Surgical Trials. Amsterdam, The Netherlands: Kugler; 2009:15–24.
12. Mermoud A, Schnyder CC, Sickenberg M, et al. Comparison deep sclerectomy with collagen implant and trabeculectomy in open-angle glaucoma. J Cataract Refract Surg. 1999;25:323–331. doi:10.1016/S0886-3350(99)80079-0
13. El Sayyad F, Helal M, El-Kholify H, et al. Nonpenetrating deep sclerectomy vs trabeculectomy in bilateral primary open-angle glaucoma. Ophthalmology. 2000;107:1671–1674. doi:10.1016/S0161-6420(00)00263-3
14. Ambresin A, Shaarawy T, Mermoud A. Deep sclerectomy with collagen implant in one eye compared with trabeculectomy in the other eye of the same patient. J Glaucoma. 2002;214–220. doi:10.1097/00061198-200206000-00009
15. Gedde SJ, Schiffman JC, Feuer WJ, Tube Versus Trabeculectomy Study Group, et al. Three-year follow-up of the Tube Versus Trabeculectomy Study. Am J Ophthalmol. 148;2009:670–684. doi:10.1016/j.ajo.2009.06.018
16. Law SK, Shih K, Tran DH, et al. Long-term outcomes of repeat vs initial trabeculectomy in open-angle glaucoma. Am J Ophthalmol. 2009;148:685–695. doi:10.1016/j.ajo.2009.05.032
17. Cillino S, Di Pace F, Casuccio A, et al. Deep sclerectomy vs punch trabeculectomy with or without phacoemulsification: a randomized clinical trial. J Glaucoma. 2004;13:500–506. doi:10.1097/01.ijg.0000137869.18156.81
18. Chiselita D. Non-penetrating deep sclerectomy vs trabeculectomy in primary open-angle glaucoma surgery. Eye. 2001;197–201. doi:10.1038/eye.2001.60
19. Russo V, Scott IU, Stella A, et al. Nonpenetrating deep sclerectomy with reticulated hyaluronic acid implant vs punch trabeculectomy: a prospective clinical trial. Eur J Ophthalmol. 2008;18:751–757. doi:10.1177/112067210801800515
20. Kayikcioglu OR, Emre S, Kaya Z. Trabeculectomy combined with deep sclerectomy and scleral flap suture tension adjustment under an anterior chamber maintainer: a new modification of trabeculectomy. Int Ophthalmol. 2010;30:271–277. doi:10.1007/s10792-009-9326-7
21. Chihara E, Okazaki K, Takahashi H, et al. Modified deep sclerectomy (D-lectomy MMC) for primary open-angle glaucoma: preliminary results. J Glaucoma. 2009;18:132–139. doi:10.1097/IJG.0b013e3181752cc8
22. Gedde SJ, Schiffman JC, Feuer WJ, Tube vs Trabeculectomy Study Group, et al. Treatment outcomes in the tube vs trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153:789–803. doi:10.1016/j.ajo.2011.10.026
23. The Fluorouracil Filtering Surgery Group. Five-year follow-up of the fluorouracil filtering surgery study. Am J Ophthalmol. 1996;121:349–366. doi:10.1016/S0002-9394(14)70431-3
24. The Advanced Glaucoma Intervention Study (AGIS): 11. Risk factors for failure of trabeculectomy and argon laser trabeculoplasty. Am J Ophthalmol. 2002;134:481–498. doi:10.1016/S0002-9394(02)01658-6
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.