Back to Journals » Clinical Interventions in Aging » Volume 17
Osteogenic Circulating Endothelial Progenitor Cells are Associated with Vascular Aging of the Large Arteries in Rheumatoid Arthritis
Authors Chan YH, Ngai MC ![]() , Chen Y, Wu MZ, Yu YJ, Zhen Z, Lai K, Chung HY, Lau CS, Tse HF, Yiu KH
, Chen Y, Wu MZ, Yu YJ, Zhen Z, Lai K, Chung HY, Lau CS, Tse HF, Yiu KH
Received 12 September 2021
Accepted for publication 18 January 2022
Published 17 March 2022 Volume 2022:17 Pages 287—294
DOI https://doi.org/10.2147/CIA.S337118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Yap-Hang Chan,1,2 Michael Cheong Ngai,3 Yan Chen,1,2 Mei-Zhen Wu,2 Yu-Juan Yu,2 Zhe Zhen,2 Kevin Lai,2 Ho-Yin Chung,4 Chak-Sing Lau,4 Hung-Fat Tse,1,2 Kai-Hang Yiu1,2
1Cardiology Division, Department of Medicine, The University of Hong Kong-Shenzhen Hospital, Shenzhen, People’s Republic of China; 2Cardiology Division, Department of Medicine, Queen Mary Hospital, University of Hong Kong, Hong Kong, Special Administrative Regions, People’s Republic of China; 3Division of Hematology, Department of Medicine, Queen Mary Hospital, University of Hong Kong, Hong Kong, Special Administrative Regions, People’s Republic of China; 4Division of Rheumatology, Department of Medicine, Queen Mary Hospital, University of Hong Kong, Hong Kong, Special Administrative Regions, People’s Republic of China
Correspondence: Kai-Hang Yiu, Cardiology Division, Department of Medicine, The University of Hong Kong-Shenzhen Hospital, 1 Haiyuan 1st Road, Futian District, Shenzhen, 518053, Guangdong, People’s Republic of China, Tel +852 22553633, Fax +852 28186304, Email [email protected]
Background and Aim: Rheumatoid arthritis is associated with both abnormal bone metabolism and accelerated vascular aging but a mechanistic link was lacking. This study aims to investigate the role of osteocalcin (OCN)-expressing circulating endothelial progenitor cells (EPCs) in vascular aging, as determined by arterial calcifications in rheumatoid arthritis.
Methods: We performed flow cytometry studies in 145 consecutive patients with rheumatoid arthritis to determine osteogenic circulating levels of OCN-positive (OCN+) CD34+KDR+ and OCN+CD34+ versus conventional early EPC CD34+CD133+KDR+. Total calcium load of the thoracic aorta (ascending plus descending) and the carotid arteries were assessed by non-contrast computed tomography (CT) and contrast CT angiography.
Results: Osteogenic EPCs OCN+CD34+KDR+ (P = 0.002) and OCN+CD34+ (P = 0.001), together with clinical parameters of age, history of hypertension, systolic blood pressure, serum levels of triglycerides, HbA1c and creatinine, use of leflunomide and brachial-ankle pulse-wave velocity (all P < 0.05), were associated with the clustered presence of aortic and carotid calcification. Multivariable analyses revealed that circulating OCN+CD34+KDR+ (B = 14.4 [95% CI 4.0 to 24.8], P = 0.007) and OCN+CD34+ (B = 9.6 [95% CI 4.9 to 14.3], P < 0.001) remained independently associated with increased aortic calcium load. OCN+CD34+ EPC (B = 0.8 [95% CI 0.1 to 1.5], P = 0.023), but not OCN+CD34+KDR+ EPC (B = 1.2 [95% CI − 0.2 to 2.6], P = 0.09), was further independently associated with carotid calcium load. In comparison, conventional early EPC CD34+CD133+KDR+ had no significant association with aortic or carotid calcium load (P = 0.46 and 0.88, respectively).
Conclusion: Circulating level of osteogenic EPC is associated with increased vascular aging in terms of calcification of the large arteries in patients with rheumatoid arthritis. The findings may suggest a role of the bone-vascular axis underlying vascular aging in rheumatic diseases. Further research is needed to characterize the mechanistic links and basis of these observations.
Keywords: osteocalcin, endothelial progenitor cells, vascular aging, rheumatoid arthritis
Introduction
Mechanisms underlying vascular degeneration and aging remained incompletely understood. While circulating endothelial progenitor cells (EPC) were believed to generally play a protective role in ameliorating vascular insults by homing to sites of vascular injury and promoting re-endothelialization,1 recent studies revealed that sub-progenies of EPC that express the osteoblastic marker, namely osteocalcin (OCN), could have detrimental effects in promoting cardiovascular calcification and aging.2–4
OCN-expressing, or osteogenic EPCs, have the potential to promulgate vascular calcification and were found to be associated with coronary endothelial dysfunction, higher risk of coronary artery disease and unstable angina, as well as aortic valve degenerative calcification.5,6 Whether the pro-calcific effects of osteogenic EPC exert similar influences in different parts of the vasculature, such as the aorta and carotid arteries, remained unknown.
For instance, subjects with rheumatic diseases such as rheumatoid arthritis (RA) have escalated risk of dysfunctional bone remodeling including bone erosion, osteopenia, and osteoporosis, and are also at higher risk of atherosclerotic cardiovascular (CV) diseases. The pathophysiology underlying this association remained obscure. The osteogenic EPCs, a cellular signaling pathway mediated along the bone-vascular axis, may provide a potentially novel explanatory mechanism.
Based on these rationales, we sought to investigate in this study the role of OCN-expressing circulating EPCs in vascular aging, as gauged by the severity and dissemination of systemic arterial calcifications, in patients with RA.
Methods
Study Sample
This translational clinical study comprised 145 patients diagnosed with RA according to the American College of Rheumatology clinical criteria,7 recruited consecutively from internal medicine specialty clinics during the study period March 2015 to November 2016.8 Demographic and clinical characteristics were retrieved from clinical records and ascertained. Relevant data was collected from the Clinical Management System (CMS), a territory-wide digitalized clinical data network of all Hong Kong public hospitals. Fasting blood was sampled for biochemistry studies included serum low-density lipoprotein (LDL)-cholesterol, triglycerides, high-density lipoprotein (HDL)-cholesterol, HbA1c and creatinine. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were measured. Written informed consent was obtained from all patients. This investigation was approved by the Ethics Committee (Institutional Review Board, University of Hong Kong/ Hong Kong Hospital Authority, Hong Kong West Cluster) and was coherent with principles in the Declaration of Helsinki.
Flow Cytometry
Absolute numbers of peripherally circulating EPCs and osteocalcin (OCN) expression were studied using fluorescence-activated cell analysis. Osteogenic progenies including OCN-positive (OCN+) CD34+KDR+ and OCN+CD34+ circulating EPCs were determined (unit, x103/mL peripheral blood), with their represented percentages of total peripheral blood mononuclear cells (PBMC) calculated. Prior studies suggested that CD34+CD133+KDR+ cells could represent EPCs in the earlier stage of differentiation,5 and they were found correlated with markers of bone turnover.9 Thus conventional early circulating EPC was defined as CD34+CD133+KDR+ in this study. Whole blood samples were aliquoted into 4 portions and preserved under −70 °C prior to analysis. Each 100 μL of blood sample was incubated with a fluorescein isothiocyanate (FITC)-conjugated antibody targeting respectively at CD34 and CD133 (Beckman Coulter, Fullerton, CA, USA). Human OCN phycoerythrin-conjugated antibody (R&D Systems) was employed to identify OCN+ cells. Differential gating was performed with FITC-labelled anti-human CD45 antibody. FITC-labelled IgG1a (Beckman Coulter) and phycoerythrin-labelled IgG2b (Becton Dickinson, Franklin Lakes, NJ, USA) were used as isotypic controls. Analysis included counting of 1,000,000 events assisted with an automated fluorescence-activated cell counter (Elite, Beckman Coulter). The absolute cell counts of all measured components per 1,000,000 events in the lymphocyte gate were thus derived.
Total Thoracic Aortic and Carotid Calcium Load
Computed Tomography (CT) assessment of the thoracic aorta and carotid arteries were performed for all subjects using a 64-slice multi-detector CT (MDCT) (Lightspeed, VCT, GE Healthcare, USA), as prior described.10 Imaging was performed when patients rested in their supine position and were instructed to hold breaths for 30s during image acquisition with prospective electrocardiogram gating (rotation time = 0.35 s, slice thickness = 2.5 mm; 120 kV; 250 mA; trigger delay = 70% R-R interval). Total calcium load of the targeted arterial regions were assessed using the software “smart score” (GE Healthcare) with threshold set for pixels >130 Hounsfield units and expressed in Agatston units. Total carotid calcium was defined as aggregated calcium load detected in the common carotid arteries, internal carotid arteries, and carotid bulbs. Total thoracic aortic calcium load included regions of the ascending plus descending thoracic aorta. Images so obtained were studied offline at post-processing workstation (Advantage windows 4.02, GE Healthcare, USA). Acquired images with dyssynchronous electrocardiographic triggering or significant motion artifacts were excluded. Two independent investigators who were blinded to clinical conditions of subjects separately studied all images. Prior inter-observer and intra-observer variability correlation coefficients of similar calcium score analyses from our group were 0.92 and 0.91, respectively.
Assessment of Arterial Stiffness
Non-invasive assessment of arterial stiffness was performed using VP-2000 System (Colin Corp., USA) to derive estimates of brachial-ankle pulse wave velocity (PWV) The methodology was prior described in details with demonstrably good reproducibility.11,12
Statistical Analysis
Relations of clinical and flow cytometry parameters with vascular aging, ie aortic/ carotid artery calcium load, were examined by Student’s t-test/ Analysis of Variance (ANOVA) and Chi-Square test, as appropriate. Strengths of linear associations were represented by the Pearson’s correlation coefficient. Univariable linear regression was used to examine the unadjusted associations between variable of interest and aortic/ carotid artery calcium load. A multivariable linear regression model was used to estimate the standardized coefficients (expressed as B with 95% confidence intervals) each of the osteogenic (OCN+CD34+KDR+ and OCN+CD34+ EPCs) and conventional early (CD34+CD133+KDR+) EPC lineages for prediction of aortic/ carotid calcium load, in which each potentially confounding variable with P-value ≤0.10 derived from univariable analysis were entered. Considered potential confounders including age, gender, history of smoking, systolic and diastolic blood pressure, resting heart rate, fasting levels of LDL-/HDL-cholesterol, triglycerides, HbA1c, creatinine, use of statins and disease-modifying anti-rheumatic agents and duration of RA. All analyses were performed using SPSS Statistics (Version 21). P-value <0.05 was considered statistically significant.
Results
Vascular Aging in Terms of Arterial Calcification
Clinical characteristics of the subjects are shown in Table 1. Conventional CV risk factors including hypertension, diabetes mellitus and hyperlipidemia had prevalence of 42%, 6.2%, and 47% respectively. Five patients (3.4%) had history of coronary artery disease. Stratified into 3 groups, the clustered presence of aortic and/ or carotid calcium load above the respective sample median values, was associated with conventional CV risk factors including age (P<0.001), history of hypertension (P<0.001), systolic blood pressure (P<0.001), serum levels of triglycerides (P=0.001), HbA1c (P=0.003) and creatinine (P<0.001), and use of leflunomide (P=0.045). A positive association of aortic/carotid calcium load with brachial-ankle pulse-wave velocity (P<0.001) lent support to the internal validity of vascular functional estimates. It was shown that osteogenic EPCs OCN+CD34+KDR+ (P=0.002) and OCN+CD34+ (P=0.001) were both positively associated with the clustered presence of aortic and/ or carotid calcium load (Figure 1). Of note, inflammatory markers (including serum CRP and ESR) and RA disease duration had no significant association with the dissemination of arterial calcification (all P>0.05).
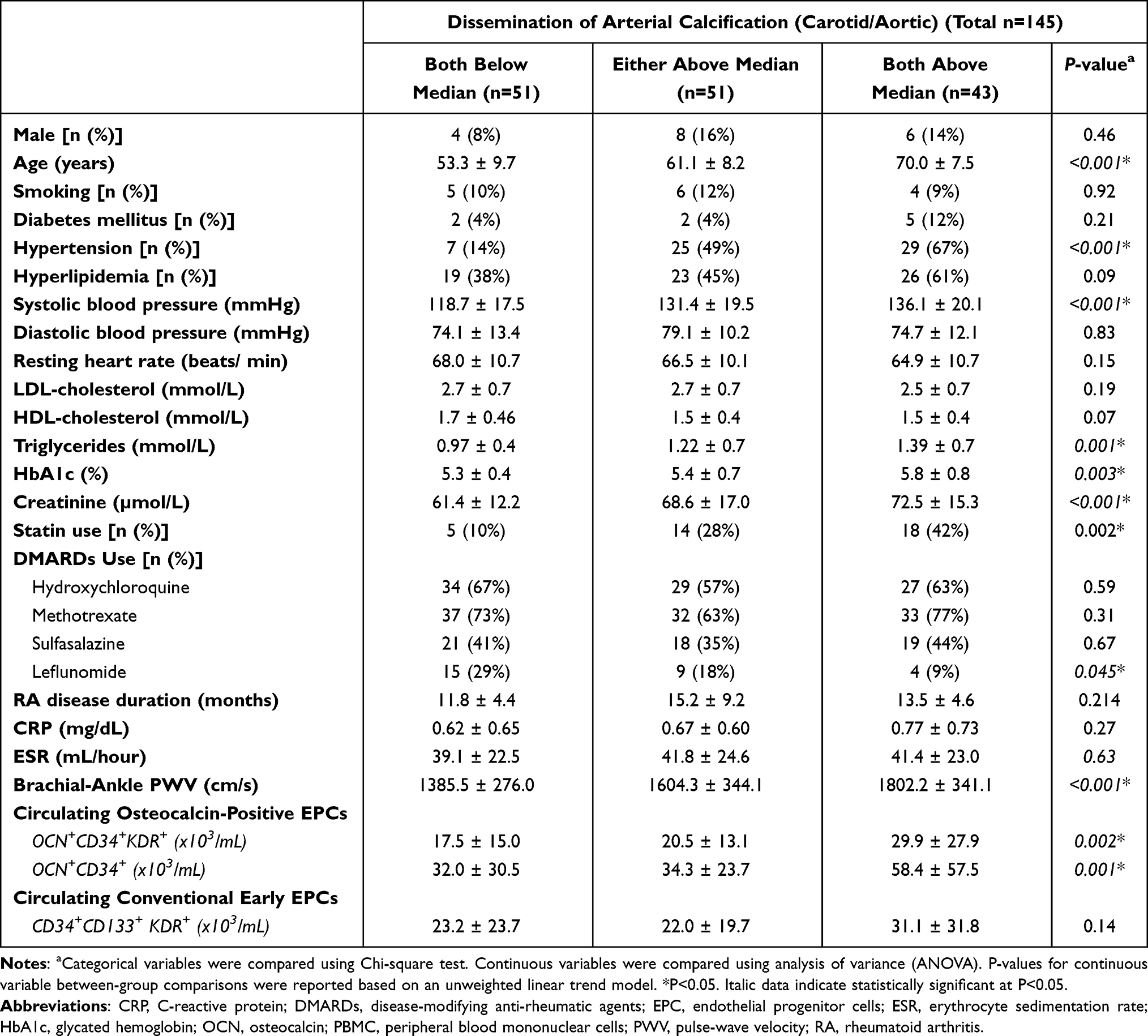 |
Table 1 Flow Cytometry and Clinical Characteristics of Subjects Stratified by Arterial Calcification Phenotype |
 |
Figure 1 Osteogenic OCN+ CD34+KDR+/OCN+CD34+ circulating EPCs and phenotype profile of vascular aging (*P<0.05). |
Osteogenic EPCs and Calcific Aging of the Thoracic Aorta
As further interrogated in Table 2, both osteogenic EPCs OCN+CD34+KDR+ (B=33.0 [95% CI 18.0 to 48.0], P<0.001) and OCN+CD34+ (B=18.4 [95% CI 11.2 to 25.7], P<0.001) were univariate predictors of aortic calcium load. In contrast, conventional early EPC CD34+CD133+ KDR+ was not associated with aortic calcium load (B=4.7 [95% CI −7.8 to 17.1], P=0.46). Multivariable analyses revealed that age, systolic blood pressure, HbA1c, and circulating levels of OCN+CD34+KDR+ (B=14.4 [95% CI 4.0 to 24.8], P=0.007) and OCN+CD34+ (B=9.6 [95% CI 4.9 to 14.3], P<0.001) remained to be independent predictors for increased aortic calcium load.
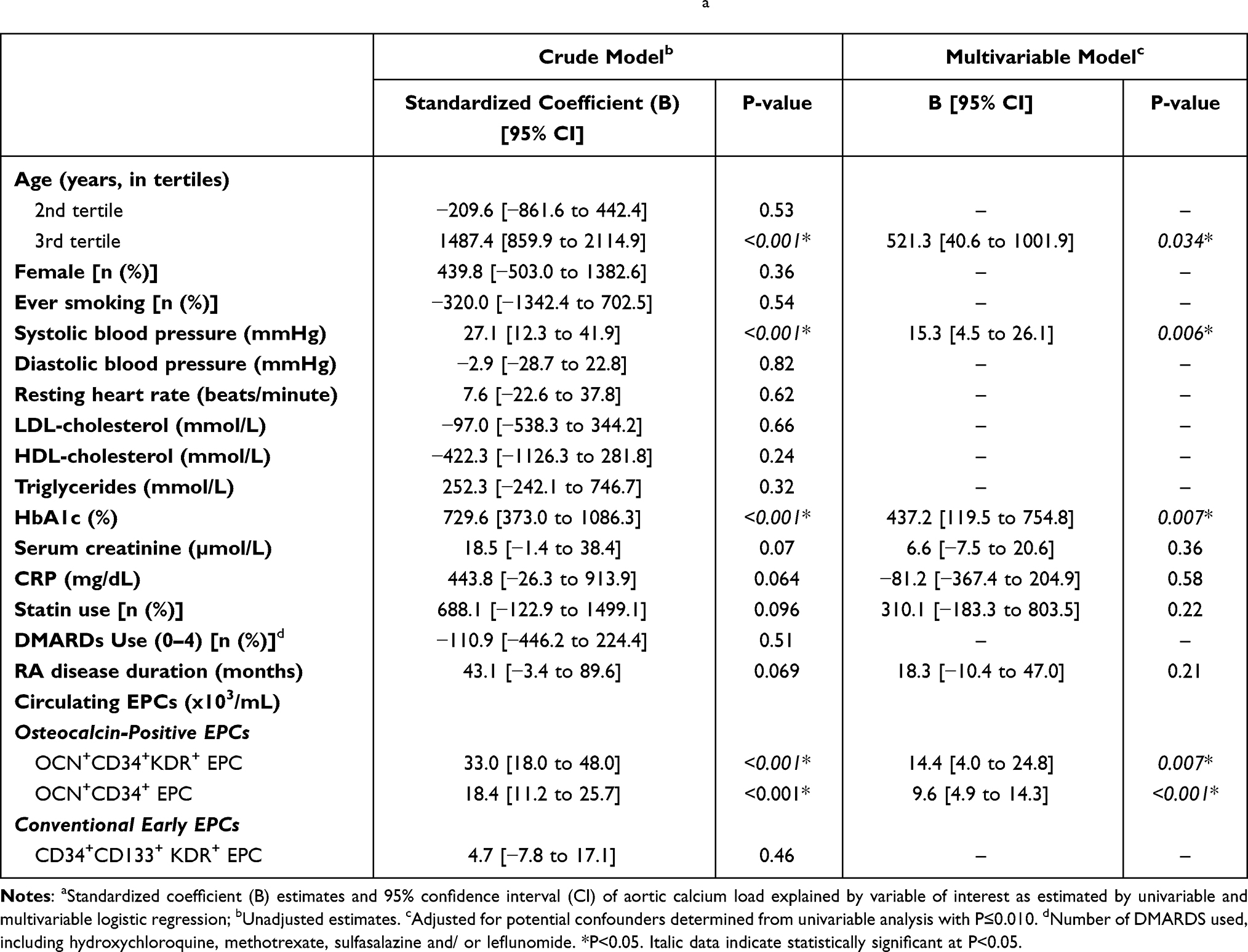 |
Table 2 Clinical and Flow Cytometry Predictors for Aortic Calcium Loada |
Osteogenic EPCs and Calcific Aging of the Carotid Arteries
Table 3 shows that osteogenic EPCs OCN+CD34+KDR+ (B=1.69 [95% CI 0.37 to 3.01], P=0.012) and OCN+CD34+ EPC (B=1.0 [95% CI 0.39 to 1.67], P=0.002) were both associated with increased carotid artery calcium load. Adjusted for potential confounders in the multivariable model, only HbA1c (P=0.018), use of statins (P=0.027), and osteogenic EPC OCN+CD34+ (B=0.8 [95% CI 0.1 to 1.5], P=0.023) but not OCN+CD34+KDR+ EPC (B=1.2 [95% CI −0.2 to 2.6], P=0.09), were independently predictors for carotid calcium load. In contrast, conventional early EPC CD34+CD133+KDR+ had no significant association with carotid calcium load (P=0.88). The positive association of statin use with carotid calcium load likely reflected the increased atherosclerosis status in subjects who by clinical indications required the use of statin (such as hyperlipidemia or established CV diseases).
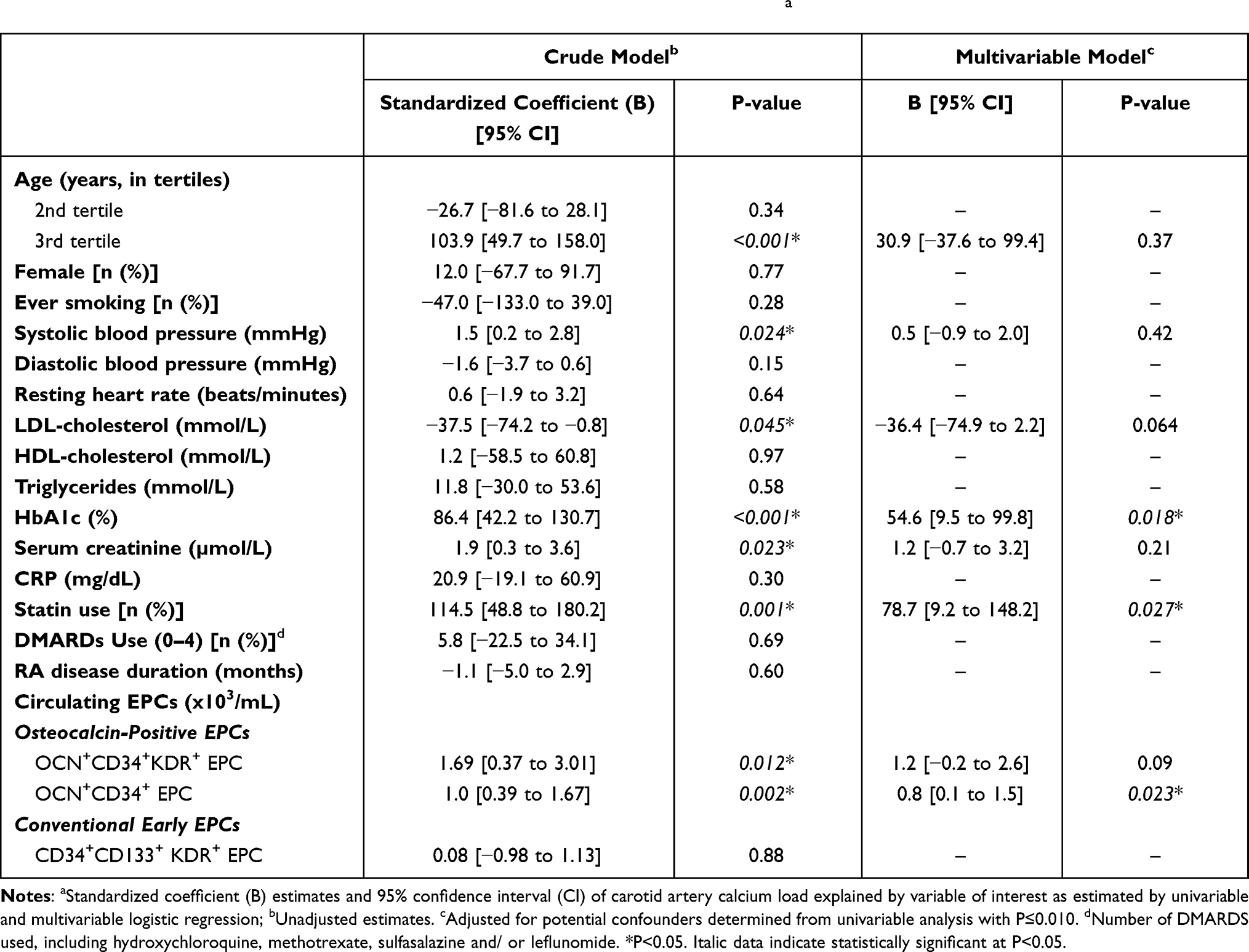 |
Table 3 Clinical and Flow Cytometry Predictors for Carotid Artery Calcium Loada |
Discussion
While the osteogenic EPCs were recently found to promulgate coronary and valvular calcifications, their role in aging of the large arteries was unknown. In this study, we established that osteogenic EPCs that expressed the osteoblastic marker OCN were independently linked to the severity of large arterial calcifications, and further associated with dissemination of vascular aging (in terms of calcium load spanning across the thoracic aorta and carotid artery regions). Importantly, RA is known to be associated with both accelerated vascular aging and abnormal bone metabolism, but the mechanism was poorly understood. Our findings suggest that the bone-vascular axis may provide a unified mechanistic link between these two clinical observations. Prior studies showed that inflammatory stress exerted upon the vasculature predisposed patients with rheumatic diseases to atherosclerosis, which translated into a higher risk of clinical CV events. Incorporating the insights from our study, promulgated systemic arterial calcifications in RA may be a result of abnormal recapitulation of osteoblastic influence on the systemic arterial system.3
Dysfunctional bone remodeling and the immune system have inextricable links in patients with rheumatic diseases. One major regulatory mechanism was the differential expression of osteoprotegerin versus receptor activator of nuclear factor-kappa-B (NF-κB) (RANK) in the competitive binding for ligand of receptor activator of nuclear factor-kappa-B (RANK-L).13–15 A recent study revealed that patients with severe calcific aortic stenosis had elevated circulating OCN+CD34+KDR+ EPC compared to control subjects, with strikingly demonstrated co-localization of OCN and NF-κB in tissues of both calcified stenotic and normal valves under immunofluorescence studies.5 Furthermore, tissue analyses in the same study revealed that osteogenic progenitor cells were found abundantly in the endothelial and deep layers of valvular tissues only in subjects with severe calcific aortic stenosis. Several other clinical studies respectively showed that osteogenic EPCs were associated with cardio-metabolic derangements,16 could undergo retention in the coronary circulation and have an important role in coronary endothelial dysfunction,6 and predisposed patients to higher risk of coronary artery disease3 and clinically manifest unstable angina.4 Our study findings thus enrich and are largely consistent with the literature. Taken together, the pro-calcific effects of osteogenic EPCs and highly active biomineralization orchestrated by the osteogenic morphogens17 on the vasculature appear to be ubiquitous, encompassing the major large arteries including the aorta, carotid arteries, the coronary arteries, as well as the heart valves.
It is noteworthy that in our study, serum inflammatory markers including ESR and CRP were not related to thoracic aorta or carotid calcium load. Neither were these biomarkers associated with the circulating level of osteogenic EPCs. This observation was not surprising, as our patient sample had a mean duration of clinically diagnosed RA for 14 years, and the majority of them had received longstanding and effective anti-rheumatic treatment, resulting in clinically and/ or serologically quiescent disease. Such disease quiescence would have rendered the current snapshot measurement of inflammatory markers non-representative of the preceding cumulated inflammatory stress that their vasculature had prior endured. The post-treatment measurement of inflammatory exposure was acknowledged as the major limitation of our study. Furthermore, the lack of valvular calcification assessment, and that of vitamin K measurement, were other limitations of our study. Despite a relatively small sample size, our study was adequately powered to detect significant associations between osteogenic EPCs and calcium load surrogates. While limited by the cross-sectional design, and that unmeasured/ residual confounding cannot be completely excluded, we adopted meticulous multivariable models to minimize the effect of confounding by adjusting for clinically and/ or pathophysiologically-relevant parameters in our analyses to derive unbiased estimates as far as possible. Future studies should include large, preferably population-based cohorts that include prospective or comprehensive retrospective gauging of cumulative inflammatory load prior to vascular assessments. Moreover, further research is needed to characterize the mechanistic links and basis of these observations.
Conclusions
Circulating level of osteogenic EPC is associated with increased vascular aging, in terms of aortic and carotid calcification in patients with RA. The findings may suggest a role of the bone-vascular axis underlying vascular aging in rheumatic diseases. Further research is needed to characterize the mechanistic links and basis of these observations.
Abbreviations
CAD, coronary artery disease; CI, Confidence Interval; CRP, C-reactive protein; DMARDs, disease-modifying anti-rheumatic agents; EPC, endothelial progenitor cells; ESR, erythrocyte sedimentation rate; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; KDR, kinase insert domain receptor; LDL, low-density lipoprotein; NF-κB, nuclear factor kappa-B; OCN, osteocalcin; PBMC, peripheral blood mononuclear cells; PWV, pulse wave velocity; RA, rheumatoid arthritis; RANK, receptor activator of nuclear factor kappa-B; RANKL, receptor activator of nuclear factor kappa-B ligand.
Acknowledgments
The abstract of this paper was presented at the European Society of Cardiology Congress, Paris, in 2019, as an oral presentation with interim findings. The relevant abstract was published in European Heart Journal, Volume 40, Issue Supplement 1, October 2019, ehz745.0012 (https://doi.org/10.1093/eurheartj/ehz745.0012).
Funding
This study was supported by Sanming Project of Medicine in Shenzhen, China (No. SZSM201911020), HKU-SZH Fund for Shenzhen Key Medical Discipline (No. SZXK2020081), and General Research Fund, Research Grants Council of Hong Kong. Y.H.C. is supported by Li Shu Fan Medical Fellowship for Internal Medicine 2021/22, The University of Hong Kong.
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Shantsila E, Watson T, Lip GY. Endothelial progenitor cells in cardiovascular disorders. J Am Coll Cardiol. 2007;49(7):741–752. doi:10.1016/j.jacc.2006.09.050
2. Chan YH, Ngai MC, Chen Y, et al. Osteogenic circulating endothelial progenitor cells are linked to electrocardiographic conduction abnormalities in rheumatic patients. Ann Noninvasive Electrocardiol. 2019;24(5):e12651. doi:10.1111/anec.12651
3. Gossl M, Modder UI, Atkinson EJ, Lerman A, Khosla S. Osteocalcin expression by circulating endothelial progenitor cells in patients with coronary atherosclerosis. J Am Coll Cardiol. 2008;52(16):1314–1325. doi:10.1016/j.jacc.2008.07.019
4. Flammer AJ, Gossl M, Widmer RJ, et al. Osteocalcin positive CD133+/CD34-/KDR+ progenitor cells as an independent marker for unstable atherosclerosis. Eur Heart J. 2012;33(23):2963–2969. doi:10.1093/eurheartj/ehs234
5. Gossl M, Khosla S, Zhang X, et al. Role of circulating osteogenic progenitor cells in calcific aortic stenosis. J Am Coll Cardiol. 2012;60(19):1945–1953. doi:10.1016/j.jacc.2012.07.042
6. Gossl M, Modder UI, Gulati R, et al. Coronary endothelial dysfunction in humans is associated with coronary retention of osteogenic endothelial progenitor cells. Eur Heart J. 2010;31(23):2909–2914. doi:10.1093/eurheartj/ehq373
7. Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31(3):315–324. doi:10.1002/art.1780310302
8. Chan YH, Ngai MC, Chen Y, et al. Cumulative rheumatic inflammation modulates the bone-vascular axis and risk of coronary calcification. J Am Heart Assoc. 2019;8(11):e011540. doi:10.1161/JAHA.118.011540
9. Peris P, Atkinson EJ, Gossl M, et al. Effects of bisphosphonate treatment on circulating osteogenic endothelial progenitor cells in postmenopausal women. Mayo Clin Proc. 2013;88(1):46–55. doi:10.1016/j.mayocp.2012.08.019
10. Wang S, Yiu KH, Mok MY, et al. Prevalence and extent of calcification over aorta, coronary and carotid arteries in patients with rheumatoid arthritis. J Intern Med. 2009;266(5):445–452. doi:10.1111/j.1365-2796.2009.02123.x
11. Chan YH, Siu CW, Yiu KH, et al. Abnormal vascular function in PR-interval prolongation. Clin Cardiol. 2011;34(10):628–632. doi:10.1002/clc.20958
12. Chan YH, Siu CW, Yiu KH, et al. Adverse systemic arterial function in patients with selenium deficiency. J Nutr Health Aging. 2012;16(1):85–88. doi:10.1007/s12603-011-0086-5
13. Tanaka Y, Ohira T. Mechanisms and therapeutic targets for bone damage in rheumatoid arthritis, in particular the RANK-RANKL system. Curr Opin Pharmacol. 2018;40:110–119. doi:10.1016/j.coph.2018.03.006
14. Poubelle PE, Chakravarti A, Fernandes MJ, Doiron K, Marceau AA. Differential expression of RANK, RANK-L, and osteoprotegerin by synovial fluid neutrophils from patients with rheumatoid arthritis and by healthy human blood neutrophils. Arthritis Res Ther. 2007;9(2):R25. doi:10.1186/ar2137
15. Boyce BF, Xing L. Biology of RANK, RANKL, and osteoprotegerin. Arthritis Res Ther. 2007;9(Suppl 1):S1. doi:10.1186/ar2165
16. Flammer AJ, Gossl M, Li J, et al. Patients with an HbA1c in the prediabetic and diabetic range have higher numbers of circulating cells with osteogenic and endothelial progenitor cell markers. J Clin Endocrinol Metab. 2012;97(12):4761–4768. doi:10.1210/jc.2012-2642
17. Bostrom KI, Rajamannan NM, Towler DA. The regulation of valvular and vascular sclerosis by osteogenic morphogens. Circ Res. 2011;109(5):564–577. doi:10.1161/CIRCRESAHA.110.234278
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.