Back to Archived Journals » Integrated Blood Pressure Control » Volume 14
Orthostatic Hypotension in Male Hypertensive Patients: A Cross-Sectional Study at the University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia
Authors Getu AA ![]() , Abuhay DA
, Abuhay DA ![]() , Goshu BT
, Goshu BT ![]()
Received 28 July 2021
Accepted for publication 23 September 2021
Published 5 October 2021 Volume 2021:14 Pages 133—139
DOI https://doi.org/10.2147/IBPC.S331467
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Ayechew Adera Getu,1 Deribew Abebaw Abuhay,2 Bahiru Tenaw Goshu3
1Department of Physiology, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara, Ethiopia; 2Department of Physiology, College of Medicine and Health Sciences, Debre Tabor University, Debre Tabor, Amhara, Ethiopia; 3Department of Human Anatomy, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara, Ethiopia
Correspondence: Ayechew Adera Getu Tel +251-91-086-6216
Email [email protected]
Background: Orthostatic hypotension (OH) is defined as a fall in systolic blood pressure (SBP) ≥ 20 mmHg or diastolic BP (DBP) ≥ 10 mmHg within 3 minutes of standing. OH incidence is increased with hypertension, and management of these patients may pose challenges, as treatment of one can worsen the other.
Objective: This study aimed to determine the prevalence of OH and its associated factors among male hypertensive patients at the University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia.
Methods: A hospital-based cross-sectional design was employed. Seated BP was measured twice and the average of the two taken. After BP had been stabilized for 5 minutes, SBP within 3 minutes of standing was measured twice and the minimum of the two taken. A drop of ≥ 20 mmHg in SBP within 3 minutes of standing was taken as OH. All male hypertensive patients who were able to attain a standing position were included. Sociodemographic, anthropometric, and clinical status of the patients were taken using structured interviewer-administered questionnaires. Data were entered and analyzed using SPSS 21. Both bivariate and multivariate logistic regression analysis were done. P≤ 0.05 was considered statistically significant.
Results: The median age of study participants was 57 (25– 96) years. The prevalence of OH was 17.6%. Uncontrolled hypertension (adjusted OR 2.08, 95% CI 1.125– 3.872) and duration of hypertension ≥ 5 years (adjusted OR 2.04, 95% CI 1.069– 3.895) were significantly associated with OH in hypertensive patients.
Conclusion: The prevalence of OH among male hypertensive patients was high. Hypertensive patients whose BP was uncontrolled and having had hypertension ≥ 5 years were risk factors of OH.
Keywords: orthostatic hypotension, hypertension, prevalence, Ethiopia
Background
Abnormal BP responses to assuming standing posture may predict adverse health outcomes. Though the definition of orthostatic hypotension (OH) is inconsistent, it is generally defined as a fall in systolic blood pressure (SBP) ≥20 mmHg or diastolic BP (DBP) ≥10 mmHg within 3 minutes of standing.1 Under healthy physiological conditions, attaining an upright posture from sitting or lying down does not significantly change BP. This is because a drop in BP due to blood pooling downward and reducing venous return and cardiac output induces reflex vasoconstriction and myocardial contractility, critical for maintaining BP to vital tissue.2 OH is common particularly in the elderly, which increases the risk of morbidity, mortality, and falls.3 Aging coupled with such comorbidities as hypertension, diabetes mellitus, and Parkinson’s disease and associated polypharmacy results in higher prevalence of OH in the elderly population.4–6
Studies on the incidence of OH and its complications have been concentrated on elderly populations.7,8 Management of hypertension coexisteing with OH might be a challenge for physicians, as treatment of hypertension can worsen the degree of OH.3,9
A key risk factor of cardiovascular, neuronal, and renal diseases, hypertension is defined as SBP ≥140 mmHg or DBP ≥90 mmHg.10,11 It is often a silent medical condition and is a major cause of premature death affecting about 1.13 billion people worldwide, with a majority of cases living in low- and middle-income countries.12
OH is mainly due to the redistribution of substantial blood volume (300–1,000 mL) pooling in the lower extremities and splanchnic veins as a result of gravity, due to assuming a standing position from a sitting or supine position1,9 This causes a transient reduction in venous return, a stroke volume and cardiac output, and finally BP level.13 Due to the substantial decrease in cerebral blood flow, patients with OH often experience such symptoms as lightheadedness, dizziness, blurred vision, cognitive blunting, tiredness, headache, and neck ache.14
Under healthy conditions, as a consequence of reduction in BP, baroreceptors located in the carotid sinus and aortic arch are activated, resulting in stimulation of the sympathetic nervous system and diminished activity of the parasympathetic system, which increases heart rate, myocardial contractility, and vascular tone.15 However, studies have suggested that patients with chronic hypertension may be at risk of developing OH because of altered sensitivity of both baroreceptors and adrenergic receptors, especially when assuming an upright posture.7,16 Inadequate sympathetic response and desensitization of baroreceptor reflex as consequences of prolonged hypertension might contribute to BP reduction following standing up.
Though causes vary, OH commonly occurs in patients with inadequate autonomic nervous system (ANS) adjustment and can be due to drugs, depletion of intravascular volume, and neurogenic problems.15 In essence, OH is usually classified according to its etiopathogenesis into neurogenic and non-neurogenic forms. Neurogenic OH is determined by structural lesions of autonomic pathways due to disorders affecting central or peripheral autonomic structures, including Parkinson’s disease, diabetes mellitus and chronic kidney disease.1
The presence of OH is associated with increased mortality and morbidity.14 The reason for this is multifold, but includes the consequences of repeated falls, resulting in fractures, head injury, and their complications.17 OH is said to be highly prevalent in older people, and as age increases, the incidence of OH also increases.9,14
OH incidence increases exponentially after age 65 years, and its importance is likely to increase as our population ages.18 OH is not only a cause of disability and impaired quality of life but also associated with a 2.6-fold increase in the risk of falls in the elderly.19
Epidemiological studies have reported associations of OH with coronary artery disease, stroke, and heart failure.20,21 The presence of OH doubles the risk of developing chronic kidney disease,22 and as an independent risk factor, it is comparable to having coronary artery disease, smoking, or hypertriglyceridemia.18
Several studies have speculated that OH is strongly associated with hypertension. Depending on age and coexisteing medical conditions and medications, OH prevalence among hypertensive patients is 13.4%–32.1%.23 Longitudinal epidemiological studies have identified OH as an independent risk factor of cardiovascular morbidity, including hypertension and all-cause mortality.24,25 OH is aggravated in elderly patients with multiple comorbidities and taking numerous medications.8,26 Diabetes is present in about 40% of patients, as would be expected, given that this is the most common cause of peripheral and autonomic neuropathy. However, the most common comorbidity among patients with OH is hypertension.8 In healthy elderly, the incidence of OH is about 2%, and this increases to 5% in elderly with controlled hypertension, but to 19% in those with uncontrolled hypertension.27,28 Furthermore, elderly with uncontrolled hypertension and OH are at more than double the risk of falls.28
In a retrospective cohort of hypertensive patients in Italy, Di Stefano et al found that the prevalence of OH was of 10.4% and increased in those aged 60 years.29 This retrospective evidence showed that the presence of diabetes mellitus and chronic kidney diseases was significantly associated with OH and that coexistence of hypertension with OH complicated the management of either condition, as the treatment of one can worsen the other.
The prevalence of OH among hypertensive patients in Ethiopia has not been established. The present study thus aimed to assess the prevalence of OH among male hypertensive patients and identify risk factors related to OH in these patients coming for routine BP checkups at the University of Gondar Comprehensive Specialized Hospital chronic diseases followup clinic.
Methods
Study Design, Setting, and Patients
This hospital-based cross-sectional study focused on male hypertensive patients selected by systematic random sampling coming for routine followup during April 10 to June 30, 2021 at the University Gondar of Comprehensive Specialized Hospital, Gondar, Ethiopia. The sample size required for this study was determined using a single population–proportion formula with assumptions of OH proportion of 0.5, since no previous study had been conducted, 95% CI, and 5% marginal error, yielding a sample size of 384. With a 5% nonresponse rate assumed, the total sample was 403. All male hypertensive patients who were unable to attain a standing position with/without support were excluded.
Data-Collection Tools and Procedures
A total of 318 patients agreed to participate, and BP was measured and recorded in the sitting position after 5 minutes’ rest and 3 minutes’ standing in a thermoneutral and comfortable environment. Sociodemographic parameters, behavioral characteristics, use of medications, and history of OH symptoms were collected by structured interviewer-administered questionnaires.
For each patient and for the first visit only variables SBP, DBP, age (stratified into two groups: <40 years and ≥40 years), degree of hypertension (controlled <140/90, uncontrolled ≥140/90), and antihypertensive medications, considered both individually and in combination, were recorded. BP was measured by manual sphygmomanometery with an appropriate cuff size. After 5 minutes’ sitting, BP was measured twice 1 minute apart until stabilization, then at 3 minutes after standing twice. The average of the last two SBP values measured in the sitting position and the lowest of the two measurements during standing were taken and analyzed. A drop ≥20 mmHg in SBP within 3 minutes of standing from sitting was taken as OH.
Data Analysis
Data were analyzed with SPSS 21 after being checked for completeness. Bivariate and multivariate binary logistic regression analyses were conducted to identify factors associated with OH. Variables with P≤0.25 on bivariate logistic regression were further analyzed using multivariate logistic regression. Strength of associations is expressed in ORs and 95% CIs. P≤0.05 was taken to be statistically significant. Descriptive statistics using tables and texts are used to present the findings.
Ethics
Ethics clearance was obtained from the ethics review committee of the School of Medicine, University of Gondar (433/2021), and was conducted in accordance with the Declaration of Helsinki. Each participant was informed about the purpose of the study, the importance of their participation, and the right to withdraw from at any time and informed written consent was obtained prior to data collection. Privacy and confidentiality of information given by each respondent was kept properly.
Results
Sociodemographic and Behavioral Characteristics
Table 1 shows the sociodemographic and behavioral characteristics of study participants. The median age of hypertensive male patients on follow-up was 57 (25–96) years, 59 (18.6%) had had no form of education and were not able to read or write, and 81 (25.5%) had had a formal education at Ethiopian higher-education institutions. A significant proportion were overweight (36.2%), and more than half (53.8%) practiced some form of physical activity on a daily basis.
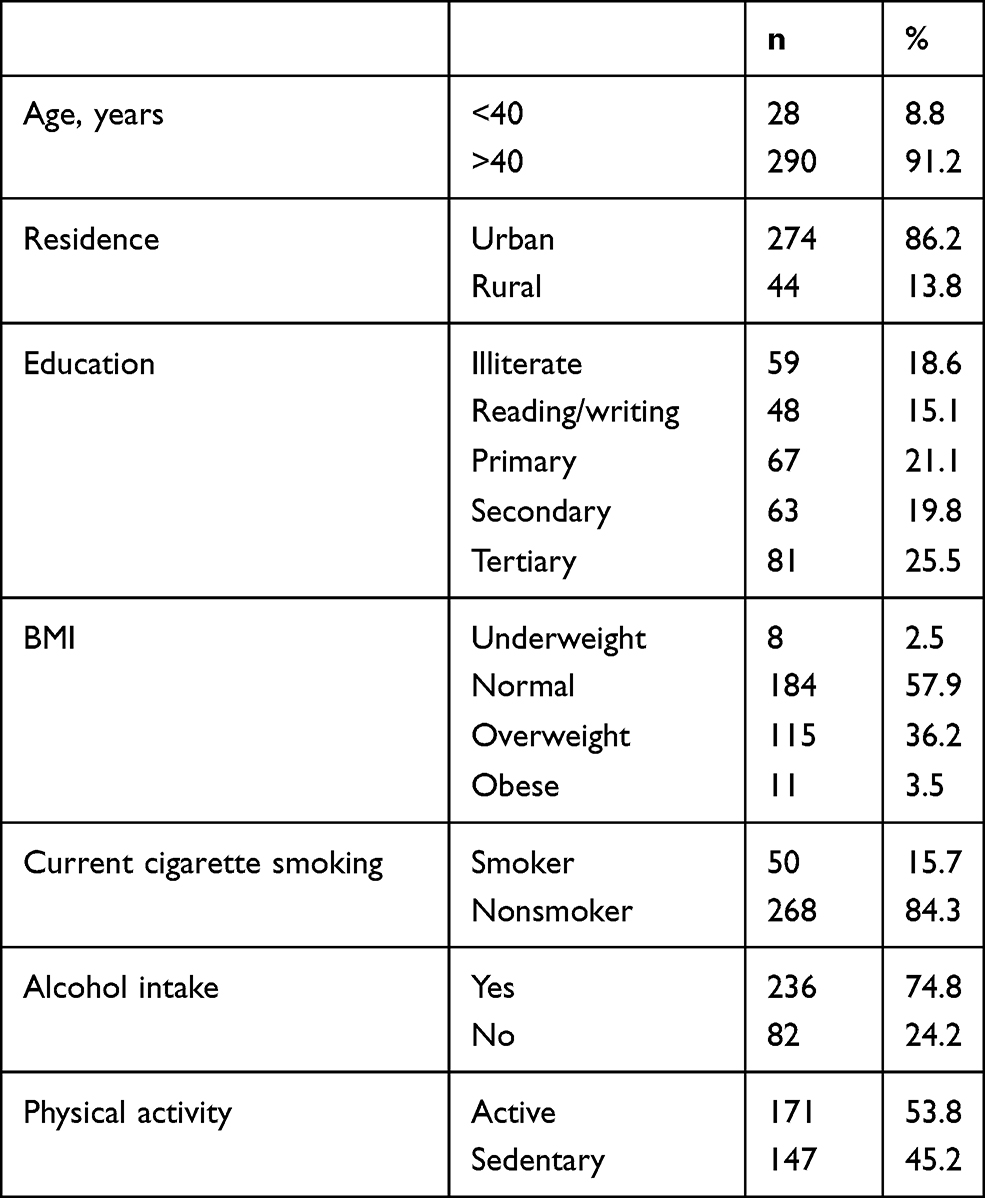 |
Table 1 Sociodemographic and behavioral characteristics of patients (n=318) |
Clinical Characteristics
Table 2 shows the patients’ clinical characteristics. Grade and duration of hypertension, antihypertensive drugs (considered both individually and in combination), any form of comorbidity, and BP in standing position after 3 minutes were recorded. About 54% of patients had their BP controlled (<140/90 mmHg), nearly 47% had a history of hypertension ≥5 years, and a majority (93.1%) were taking one or more antihypertensive medications. Diuretics were the most widely prescribed drug type (25.7%). More than half were taking more than one antihypertensive medication (polytherapy), about 40% had one or more coexisting diseases, with diabetes mellitus (23.3%) the commonest, followed by cardiovascular diseases (10.1%).
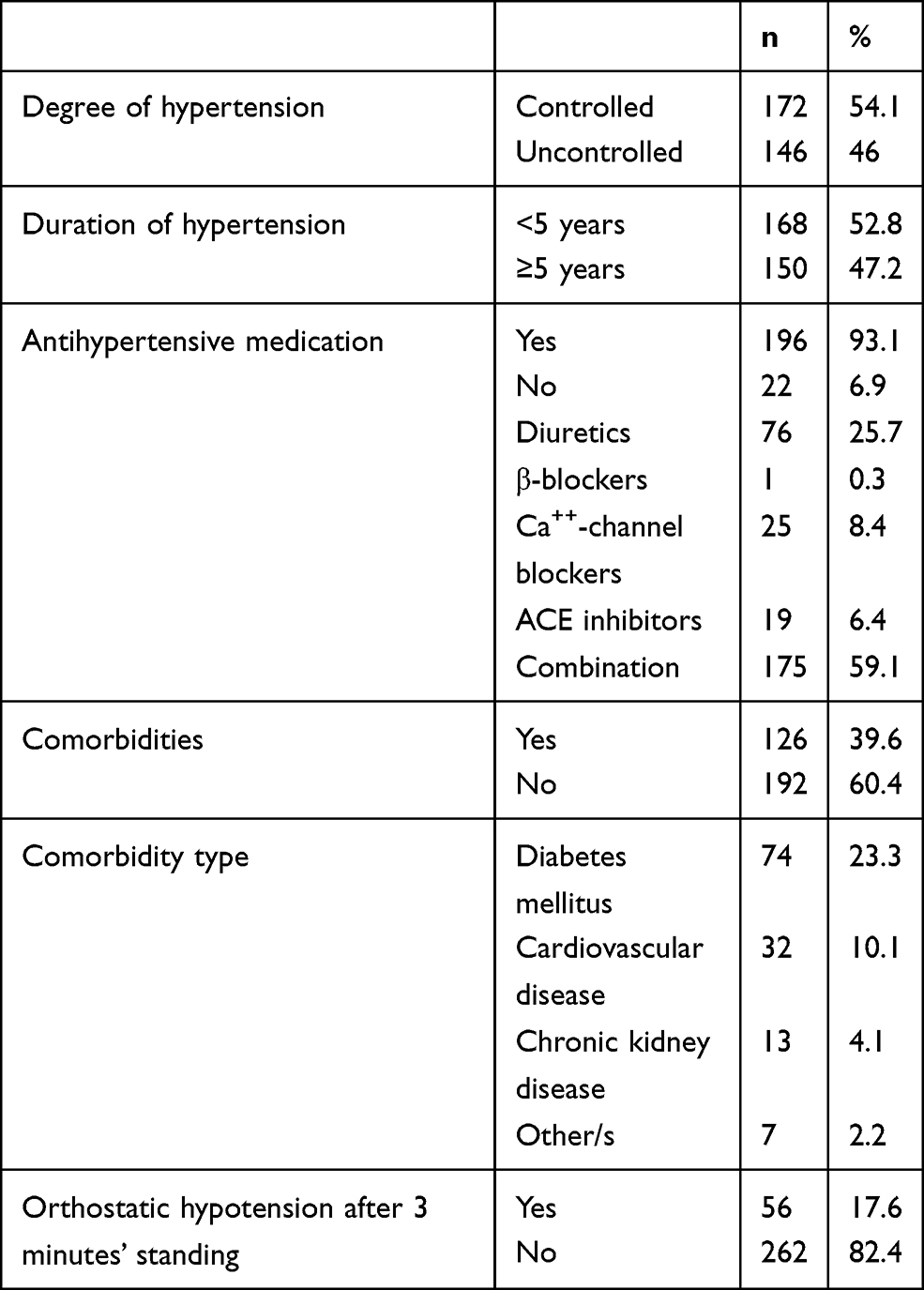 |
Table 2 Clinical characteristics of patients (n=318) |
Prevalence of Orthostatic Hypotension
OH prevalence among male hypertensive patients after 3 minutes of standing was 17.6%. Almost all (96.4%) those with OH were aged ≥40 years. Patients with uncontrolled BP (≥140/90) were significantly more likely (41%) to have OH than those with controlled BP. About 66% that had had hypertension ≥5 years showed hypotensive responses when standing.
Factors Associated with Orthostatic Hypotension
Table 3 shows bivariate and multivariate logistic analyses of factors associated with OH. Age, residence, alcohol intake, exercise habits, seated BP, and duration of hypertension were associated with OH on bivariate logistic regression analysis. Variables with P≤0.25 were further analyzed with multivariate logistic regression, and level of BP in a seated position (AOR 2.08, 95% CI 1.125–3.872) and duration of hypertension ≥5 years (AOR 2.04 95% CI 1.069–3.895) were significantly associated with OH.
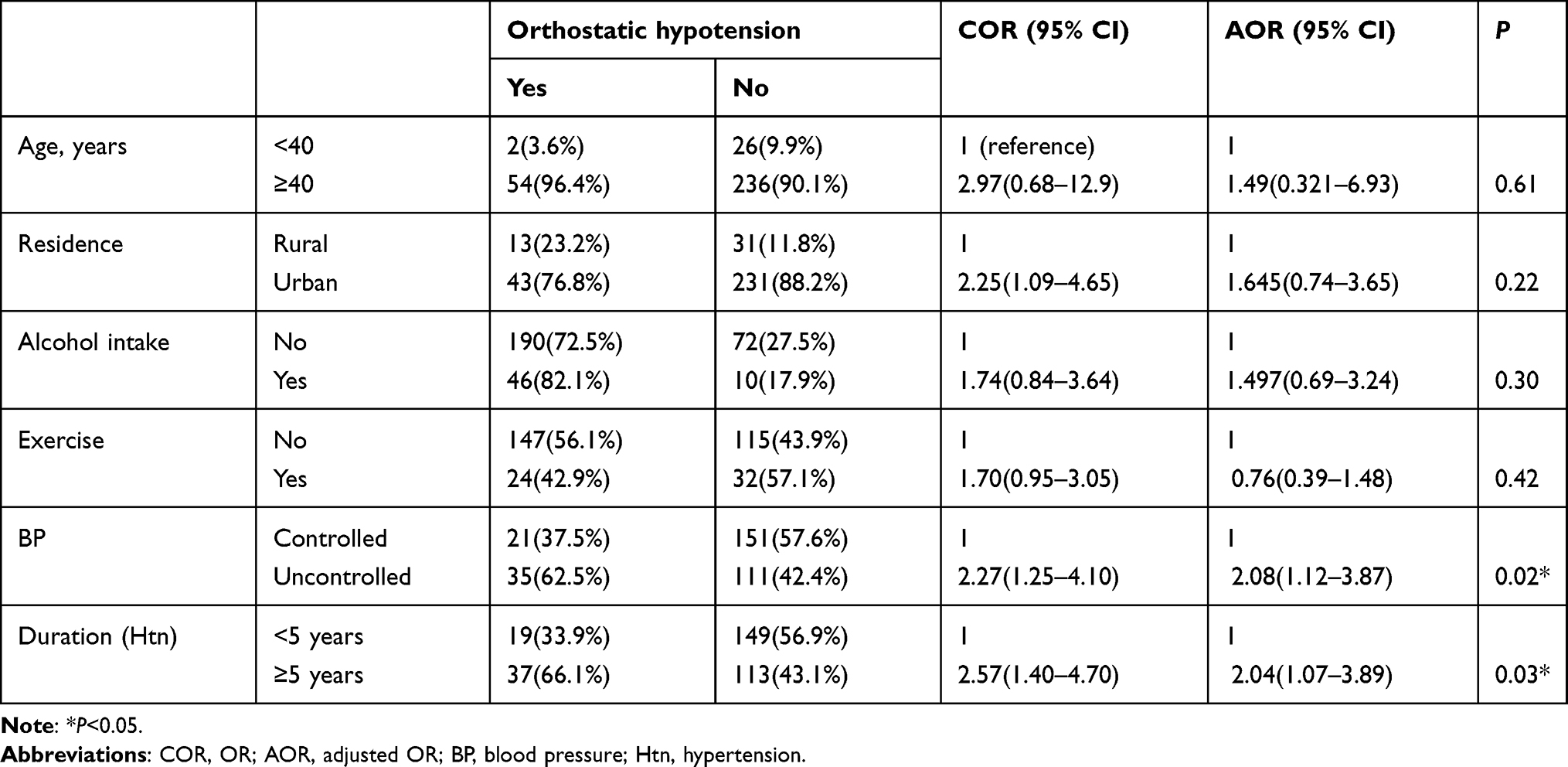 |
Table 3 Bivariate and multivariate logistic regression analyses of factors associated with OH (n=318) |
Discussion
The aim of this study was to determine the prevalence of OH among male hypertensive patients on follow-up at the University of Gondar Comprehensive Specialized Hospital. We collected data on all age-groups with a history of hypertension. In this study, we investigated the prevalence of OH using only manometric criteria (SBP changes only). OH was defined as SBP decrease of at least 20 mmHg within 3 minutes of standing from sitting.
The overall prevalence of OH was 17.6%. This is comparable to a systematic meta-analysis study showing prevalence of OH with hypertension of 20%.17 In a 2007 US study, the commonest comorbidity among patients with OH was hypertension, which is present in approximately 70% of patients.8 In a retrospective cohort of hypertensive patients in Italy, Di Stefano et al found that OH prevalence was 10.4% and increased in those aged 60 years and above.29 In a UK study, the prevalence of OH among women was 28% and increased in hypertension and age.27 That study concluded that uncontrolled hypertension, use of three or more antihypertensives, and multiple comorbidities were predictors of OH in older women.
Uncontrolled hypertension and duration of hypertension were independent factors associated with OH. However, this study failed to associate age, obesity, antihypertensive medications, or comorbidity other than hypertension with OH, contrary to other studies.5,17,27
Aging is an important factor in OH and its associated symptoms.14,30 The prevalence of OH varies greatly depending on the population studied, and there were conflicting results regarding aging and incidence of OH, challenging the generally accepted consensus of aging coupled with an increase in prevalence of chronic diseases increases the occurrence of OH.6 Nevertheless, OH is said to be highly prevalent in older people. It occurs in about 6% of healthy elderly, 18%–54% of nursing-home residents, and up to 60% in hospitalized elderly.9 In a systematic review and meta-analysis (n=24,967), the pooled prevalence of OH in community-dwelling older people was 22.2%.30 In this study, 54 (16.9%) patients with OH ere aged >40 years, though we failed to find a statistically significant association between age and OH. This might have been because of the age distribution and categorization of our study participants (we included all hypertensive patients, irrespective of age, which was 25–90 years).
Cross-sectional and longitudinal epidemiological studies have identified OH as an independent risk factor of cardiovascular morbidity, including hypertension and all-cause mortality.24,25 In the current study, seated BP level (AOR 2.08, 95% CI 1.13–3.87) was significantly associated with OH (P=0.02). The odds of having OH among patients whose BP was uncontrolled was higher than those with controlled BP. In support of this finding, the incidence of OH in healthy elderly with other studies was about 2%, but increased to 5% with controlled hypertension and 19% in those with uncontrolled hypertension.27,28 Furthermore, elderly with uncontrolled hypertension and OH have more than double the risk of falls.28
Another important finding of this study was the association between duration of hypertension and OH. Hypertension for ≥5 years showed a significant association with OH (AOR 2.04, 95% CI 1.07–3.89). Studies have suggested that patients with chronic hypertension may be at risk of developing OH because of altered sensitivity of both baroreceptors and adrenergic receptors, especially when assuming an upright posture.7,16 Inadequate sympathetic response and desensitization of the baroreceptor reflex as a consequence of prolonged hypertension might contribute to BP reduction following standing.
OH is very common with coexistent diseases. A retrospective study in Italy showed that the presence of diabetes mellitus and chronic kidney diseases was significantly associated with OH.29 However, in the current study there was no significant association between coexisting disease (eg, diabetes mellitus) and OH. This might have been due to the small number of hypertensive patients with other comorbidities and the duration of these comorbidities not being known.
Limitations
This study has its limitations. First, it examined only male hypertensive patients, making generalization to female patients difficult. Second, we analyzed outcomes using only manometric criteria (we did not assess the presence of orthostatic symptoms). Finally, the study design was cross-sectional, making it difficult to ascertain a cause-and-effect relationship between OH and other variables.
Conclusion
The prevalence of OH among male hypertensive patients on follow-up at the University of Gondar Comprehensive Specialized Hospital was high. Uncontrolled hypertension and duration of hypertension ≥5 years were factors associated with increased prevalence of OH. Though we did not assess the presence of orthostatic symptoms, careful control of BP is warranted to minimize the likelihood of developing OH and its complications. Further research is recommended to clarify the degree of symptomatic OH among hypertensive patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bradley JG, Davis KA. Orthostatic hypotension. Am Fam Physician. 2003;68(12):2393–2398.
2. Matalon SV, Farhi LE. Cardiopulmonary readjustments in passive tilt. J Appl Physiol. 1979;47(3):503–507.
3. Ricci F, De Caterina R, Fedorowski A. Orthostatic hypotension: epidemiology, prognosis, and treatment. J Am Coll Cardiol. 2015;66(7):848–860. doi:10.1016/j.jacc.2015.06.1084
4. Shen S, He T, Chu J, He J, Chen X. Uncontrolled hypertension and orthostatic hypotension in relation to standing balance in elderly hypertensive patients. Clin Interv Aging. 2015;28(10):897–906. doi:10.2147/CIA.S81283
5. Wu JS, Wu NH, Lu FH, Chang CJ. Factors associated with orthostatic hypotension in the Chinese population in Taiwan. Am J Hypertens. 1996;9(10 Pt 1):999–1005. doi:10.1016/0895-7061(96)00151-3
6. Senard JM, Raï S, Lapeyre-Mestre M, et al. Prevalence of orthostatic hypotension in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 1997;63(5):584–589. doi:10.1136/jnnp.63.5.584
7. Kanjwal K, George A, Figueredo VM, Grubb BP. Orthostatic hypotension: definition, diagnosis and management. J Cardiovasc Med. 2015;16:75–81. Lippincott Williams and Wilkins.
8. Shibao C, Grijalva CG, Raj SR, Biaggioni I, Griffin MR. Orthostatic hypotension-related hospitalizations in the United States. Am J Med. 2007;120(11):975–980. doi:10.1016/j.amjmed.2007.05.009
9. Biaggioni I. Orthostatic hypotension in the hypertensive patient. Am J Hypertens. 2018;31(12):1255–1259. doi:10.1093/ajh/hpy089
10. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42(6):1206–1252. doi:10.1161/01.HYP.0000107251.49515.c2
11. Kokubo Y, Iwashima Y. Higher blood pressure as a risk factor for diseases other than stroke and ischemic heart disease. Hypertension. 2015;66(2):254–259. doi:10.1161/HYPERTENSIONAHA.115.03480
12. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–237. doi:10.1038/s41581-019-0244-2
13. Kanjwal K, George A, Figueredo VM, Grubb BP. Orthostatic hypotension: definition, diagnosis and management. J Cardiovasc Med. 2015;16(2):75–81. Lippincott Williams and Wilkins.
14. Low PA, Tomalia VA. Orthostatic hypotension: mechanisms, causes, management. J Clin Neurol. 2015;11(3):220–226. doi:10.3988/jcn.2015.11.3.220
15. Brignole M, Moya A, De Lange FJ, et al. Practical Instructions for the 2018 ESC guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39(21):e43–80. doi:10.1093/eurheartj/ehy071
16. Lamarre-Cliche M. Orthostatic hypotension and supine hypertension in the patient with autonomic failure. Can J Gen Inter Med. 2015;9:3.
17. McDonagh STJ, Mejzner N, Clark CE. Prevalence of postural hypotension in primary, community and institutional care: a systematic review and meta-analysis. BMC Fam Pract. 2021;22:1. doi:10.1186/s12875-020-01313-8
18. Shibao C, Biaggioni I. Orthostatic hypotension and cardiovascular risk. Hypertension. 2010;56:1042–1044. doi:10.1161/HYPERTENSIONAHA.110.162768
19. Ooi WL, Hossain M, Lipsitz LA. The association between orthostatic hypotension and recurrent falls in nursing home residents. Am J Med. 2000;108(2):106–111. doi:10.1016/S0002-9343(99)00425-8
20. Rose KM, Tyroler HA, Nardo CJ, et al. Orthostatic hypotension and the incidence of coronary heart disease: the Atherosclerosis Risk in Communities study. Am J Hypertens. 2000;13(6 Pt 1):571–578. doi:10.1016/S0895-7061(99)00257-5
21. Koski K, Laippala P. Orthostatic hypotension and the risk of myocardial infarction in the home-dwelling elderly. J Intern Med. 2004;255:486–493. doi:10.1111/j.1365-2796.2004.01313.x
22. Franceschini N, Rose KM, Astor BC, Couper D, Vupputuri S. Orthostatic hypotension and incident chronic kidney disease: the atherosclerosis risk in communities study. Hypertension. 2010;56(6):1054–1059. doi:10.1161/HYPERTENSIONAHA.110.156380
23. Benvenuto LJ, Krakoff LR. Morbidity and mortality of orthostatic hypotension: implications for management of cardiovascular disease. Am J Hypertens. 2011;24(2):135–144. doi:10.1038/ajh.2010.146
24. Masaki KH, Schatz IJ, Burchfiel CM, et al. Orthostatic hypotension predicts mortality in elderly men: the Honolulu Heart Program. Circulation. 1998;98(21):2290–2295. doi:10.1161/01.CIR.98.21.2290
25. Xin W, Lin Z, Mi S. Orthostatic hypotension and mortality risk: a meta-analysis of cohort studies. Heart. 2014;100(5):406–413. doi:10.1136/heartjnl-2013-304121
26. Rivasi G, Rafanelli M, Mossello E, Brignole M, Ungar A. Drug-related orthostatic hypotension: beyond anti-hypertensive medications. Drugs Aging. 2020;37(10):725–738. doi:10.1007/s40266-020-00796-5
27. Kamaruzzaman S, Watt H, Carson C, Ebrahim S. The association between orthostatic hypotension and medication use in the British Women’s Heart and Health Study. Age Ageing. 2009;39(1):51–56. doi:10.1093/ageing/afp192
28. Gangavati A, Hajjar I, Quach L, et al. Hypertension, orthostatic hypotension, and the risk of falls in a community-dwelling elderly population: the maintenance of balance, independent living, intellect, and zest in the elderly of Boston study. J Am Geriatr Soc. 2011;59(3):383–389. doi:10.1111/j.1532-5415.2011.03317.x
29. Di Stefano C, Milazzo V, Totaro S, Sobrero G, Ravera A, Milan SM, Maule S, Veglio F. Orthostatic hypotension in a cohort of hypertensive patients referring to a hypertension clinic. J Hum Hypertens. 2015;29:599–603. doi:10.1038/jhh.2014.130
30. Saedon NIZ, Tan MP, Frith J. The prevalence of orthostatic hypotension: a systematic review and meta-analysis. J Gerontol Ser A Biol Sci Med Sci. 2020;75:117–122. Oxford University Press. doi:10.1093/gerona/gly188
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.