Back to Journals » Clinical Interventions in Aging » Volume 16
Orthostatic Hypotension in Elderly Patients with Essential Tremor
Authors Kaya D ![]() , Aydin AE, Isik AT
, Aydin AE, Isik AT ![]()
Received 7 December 2020
Accepted for publication 8 January 2021
Published 22 January 2021 Volume 2021:16 Pages 155—160
DOI https://doi.org/10.2147/CIA.S296190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Derya Kaya,1 Ali Ekrem Aydin,2 Ahmet Turan Isik1
1Unit for Brain Aging and Dementia, Department of Geriatric Medicine, Faculty of Medicine, Dokuz Eylül University, Izmir, Turkey; 2Department of Geriatric Medicine, Sivas State Hospital, Sivas, Turkey
Correspondence: Derya Kaya
Unit for Brain Aging and Dementia, Department of Geriatric Medicine, Faculty of Medicine, Dokuz Eylül University, Balçova, Izmir 35340, Turkey
Tel +90 232 412 43 41
Fax +90 232 412 43 39
Email [email protected]
Purpose: Essential tremor (ET) is the most common movement disorder in which dysautonomia symptoms can be present. We aimed to evaluate the presence of orthostatic hypotension (OH) and its relationship with the clinical features.
Patients and Methods: Forty-four elderly patients with ET and 118 healthy elderly controls were included. OH was assessed via the head-up tilt table test and defined, according to the change in position, as a drop of at least 20 mmHg in systolic blood pressure and/or 10 mmHg in diastolic blood pressure. Tremor severity was evaluated using the Fahn-Tolosa-Marin Tremor Rating (FTMTR) Scale. All patients underwent geriatric comprehensive assessment.
Results: There were no differences between the controls and patients with ET regarding age and gender. The mean age was 72.8± 6.1, the mean disease duration 19.1± 13.5 years and the mean FTMTR score was 30.9± 17.1 in patients with ET. The frequency of OH at the 1st minute in patients with ET was higher than in controls (31.8% vs 17.8%, p=0.046). Furthermore, the frequency of jaw tremor in patients with OH was higher than in those without OH (35.7% vs 6.7%, p=0.025). About 28.6% of ET patients with OH had orthostatic symptoms.
Conclusion: We demonstrated that ET patients, particularly those with jaw tremors, had OH and that most of them were asymptomatic. Therefore, in order to protect patients from complications related to OH, it would be appropriate to evaluate OH in the follow-up and treatment of elderly patients with ET.
Keywords: essential tremor, orthostatic hypotension, head-up tilt table test, jaw tremor, elderly
Introduction
Essential tremor (ET) is a gradual progressive movement disorder common in the elderly of 60 and above, with a prevalence of 1% to 5%. It is characterized by approximately symmetrical postural or kinetic tremors in the hands and forearms, followed by head, voice and jaw tremors in some patients.1 Neuropathological studies in ET have revealed microstructural changes in the cerebellum.2 Additionally, Lewy bodies mainly in the locus coeruleus of the brainstem were detected in some patients with ET.3 The locus coeruleus is an established structure regulating autonomic responses, resulting in modulation in blood pressure and baroreflex responses.4 Besides, recent evidence suggests that the cerebellum serves to mediate cardiovascular responses, thus contributing to the cortical autonomic network which plays a significant role in controlling cardiovascular changes occurring in response to stressors like orthostatic challenges, such as orthostatic hypotension (OH).5–7
OH, also accepted as a geriatric syndrome, can lead to several negative health outcomes in the elderly, such as increasing the risk of falls and fractures, cerebro-cardiovascular morbidity, and inability to perform activities of daily living.8,9 Therefore, screening of OH in elderly ET patients is of great importance in geriatric practices. Kim et al reported that ET cases displayed more orthostatic symptoms than controls but the frequency of OH in younger ET patients was similar to that of normal controls.10 Nonetheless, Damian et al found that with the exception of sialorrhea, there were no autonomic symptoms in ET cases.11 Thus, the issue of autonomic dysfunction in ET cases is still a topic of debate and reports addressing OH in the cases are scarce. Provided that both cardiovascular autonomic functions such as postural control of blood pressure and the source of the pathophysiology of ET appear to involve pathways through the cerebellum and locus coeruleus, certain questions arise such as “Can autonomic functions be affected in ET?” or “Can postural blood pressure changes be associated with ET in the elderly?”
Therefore, the objective of the current study was to investigate whether, in comparison to normal controls, patients with ET experience OH during postural changes in the Head-up Tilt Table (HUT) test, and to explore the clinical features of ET cases with OH.
Participants and Methods
The Study Population
ET and healthy controls were included in this cross-sectional study. All participants were patients who had been admitted to the outpatient clinic at the Department of Geriatric Medicine in Dokuz Eylul University, Faculty of Medicine, Izmir, Turkey, during the period from December 2018 to December 2019. The study was approved by the local ethics committee of the University and was conducted in accordance with the Helsinki Declaration. Written informed consent was obtained from all study participants.
All patients were clinically diagnosed with ET based on recommendations of the Consensus Statement of the Movement Disorders Society.1 Patients who had no history of movement disorders, dementia, psychiatric disorders, no family history of ET or other neurodegenerative diseases, or no evidence of vascular or other brain lesions on a standard structural CT scan in our outpatient clinic were included as a control group.
Participants who were not eligible for assessment of orthostatic blood pressure change, including severe anemia (hemoglobin<10 g/dL), critical mitral and/or aortic valve stenosis, acute or chronic renal insufficiency, decompensated cardiac and/or hepatic insufficiency, severe carotid artery stenosis and/or severe coronary artery disease (CAD), acute myocardial infarction, dehydration, and electrolyte imbalances were excluded from the study. Additionally, participants who had been receiving digoxin, thyroxine, dopaminergic medications and/or anticholinergic treatment and those with laboratory abnormalities in thyroid function, hepatic function and renal function were also excluded.
Comprehensive Geriatric Assessment (CGA)
Demographic features, physical examinations, neurological examinations, and a set of scales were obtained from the medical records. The demographic features were gender, age, family history of ET, medical and medication history, neurological history, and educational history. A family history of ET was defined as the presence of at least one first-degree relative with reported ET. The number of medications and the Charlson Comorbidity Index (CCI) were recorded. The set of scales included the Mini-Mental State Examination (MMSE) test for global cognitive evaluation,12,13 the Geriatric Depression Scale (GDS),14 the timed-up-and-go (TUG) test,15 the Tinetti Performance Oriented Mobility Assessment (POMA),16 and Basic and Instrumental Activities of Daily Living (BADL and IADL).17,18 Tremor severity was measured using the Fahn‐Tolosa‐Marin Tremor Rating (FTMTR) Scale in ET cases.19
Evaluation of Orthostatic Hypotension
The standardized tilt table was used (Gemesan® Tilt Table G-71, Istanbul, Turkey) in the HUT test. All participants were allowed to take their daily medications and warned not to smoke, drink caffeine, or drink alcoholic beverages. They were seated with a minimum of 1-hour pre- or post-lunch before the measurements were obtained. BP measurement was taken following 30 minutes of rest in a reclining position in a silent room at a controlled temperature of 20–24°C; then the patients were raised upright at 60–80° rapidly and fluently and the measurements were repeated for the same arm on the 1st, 3rd, and 5th minutes using a patient monitor (Biolight®, BIOM69, Australia) with a reusable adult arm cuff.8 During the HUT, the patients were questioned concerning OH symptoms such as dizziness, lightheadedness, blackout, nausea, etc. OH was defined as a decrease of at least 20 mmHg in systolic blood pressure and/or 10 mmHg in diastolic blood pressure upon the change in position in the HUT.20,21
Statistical Analysis
The study data were analyzed using SPSS v 22.0 (IBM Corp, U.S.A.). The descriptive statistics have been shown as mean ± standard deviation (SD) for variables with normal distribution, median (minimum to maximum) for non-normal distributions, and number of cases and percentage (%) for nominal variables. The Kolmogorov–Smirnov test was performed to test the normality of continuous variables. Differences in categorical variables between patients with ET and the controls were tested using the chi-square test, or Fisher’s exact test when the assumptions for chi-square test were unmet. All comparisons of continuous variables between the two independent groups were performed with the Mann–Whitney U-test. Binary logistic regression analysis was conducted to determine whether there was a relationship between significant variables, resulting from the comparisons between the groups, and OH. A probability of <0.05 was described as significant. In patients with ET, the correlation between the clinical parameters and the decrease in blood pressure obtained from the HUT was analyzed via the Spearman correlation coefficient. Only correlations which were statistically significant, and represented large-effect sizes, as defined by a correlation coefficient of 0.50 or higher, were presented in the results and considered for discussion.
Results
The demographic data and clinical characteristics of the controls (n=118) and patients with ET (n=44) have been summarized in Table 1. There was no difference between the groups with respect to age and gender.
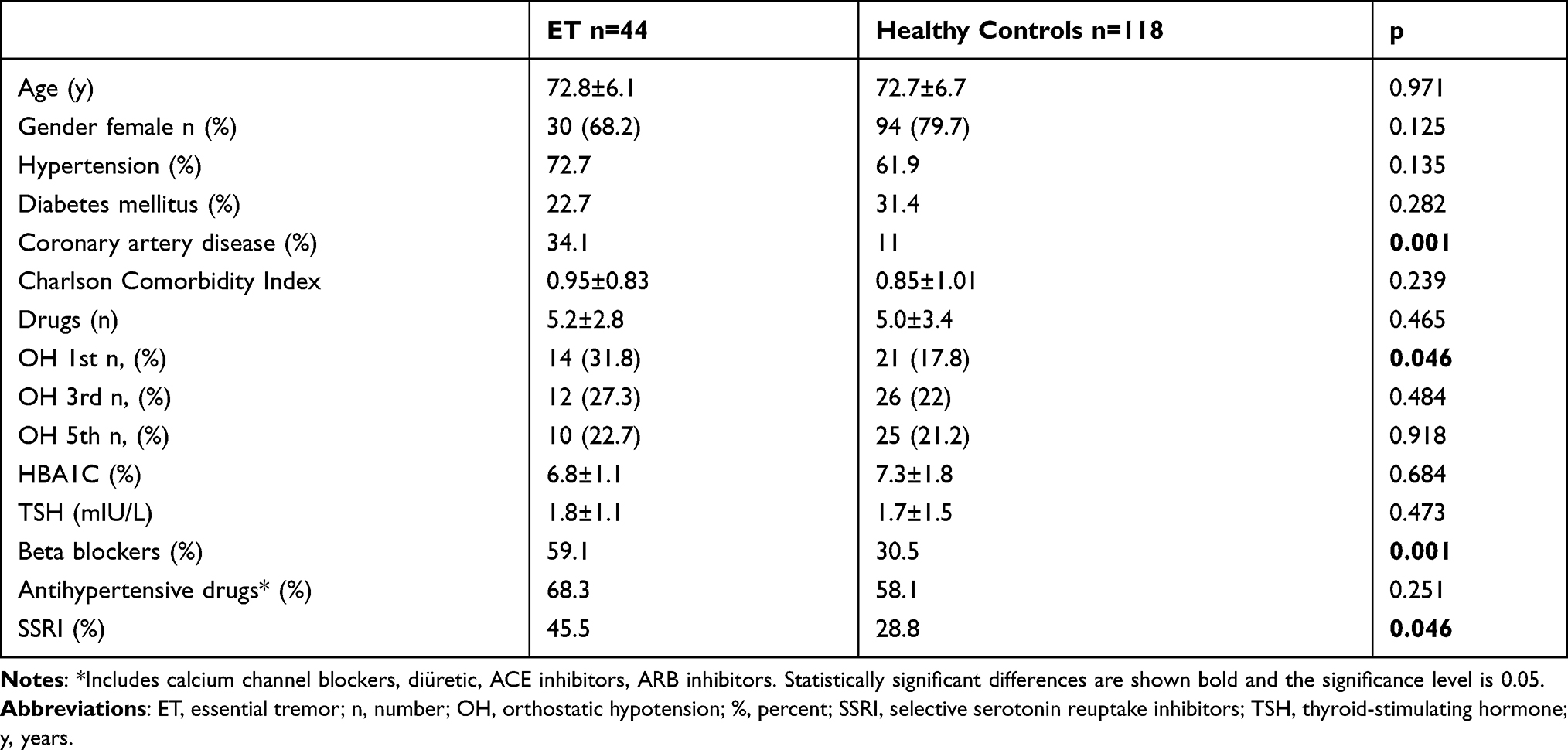 |
Table 1 Demographic and Clinical Characteristics of the Participants in the Study |
The number of subjects with OH at the 1st minute after tilting was significantly higher in patients with ET than in controls (14 of 44 vs 21 of 118 patients, p=0.046). However, the presence of OH both at the 3rd minute and the 5th minute was similar in subjects with ET and controls (p=0.484 and 0.918, respectively). CAD and the usage of beta-blockers and antidepressants were significantly more prevalent in patients with ET than in controls (p=0.001, 0.001, 0.046, respectively) (Table 1). Subsequently, binary logistic regression analysis was used to analyze whether the use of beta-blockers, antidepressants, and CAD had any relationship with OH at the 1st minute. The results indicated that the difference in OH was not related to these covariates in patients with ET (p= 0.528, 0.980 and 0.054, respectively).
The mean disease duration was 19.1±13.5 years (range: 5–55) and the mean FTMTR score was 30.9±17.1 (range: 4–63) in patients with ET. Family history was positive in 81.8% of 44 patients, voice tremors in 16 patients (36.4%), head tremors in nine patients (20.5%), and jaw tremors in seven patients (15.9%). There were no significant differences between ET patients with and without OH regarding age, gender, disease durations, and FTH scores and tremor localizations including the head and voice. However, the frequency of jaw tremors in patients with OH was higher than those without OH (35.7% vs 6.7%, p=0.025). In other words, most of the patients with jaw tremors had OH (5/7). The comparison data of ET patients with and without OH has been presented in Table 2. Only four (28.6%) out of 14 ET patients with OH complained of feeling dizzy or lightheaded while standing.
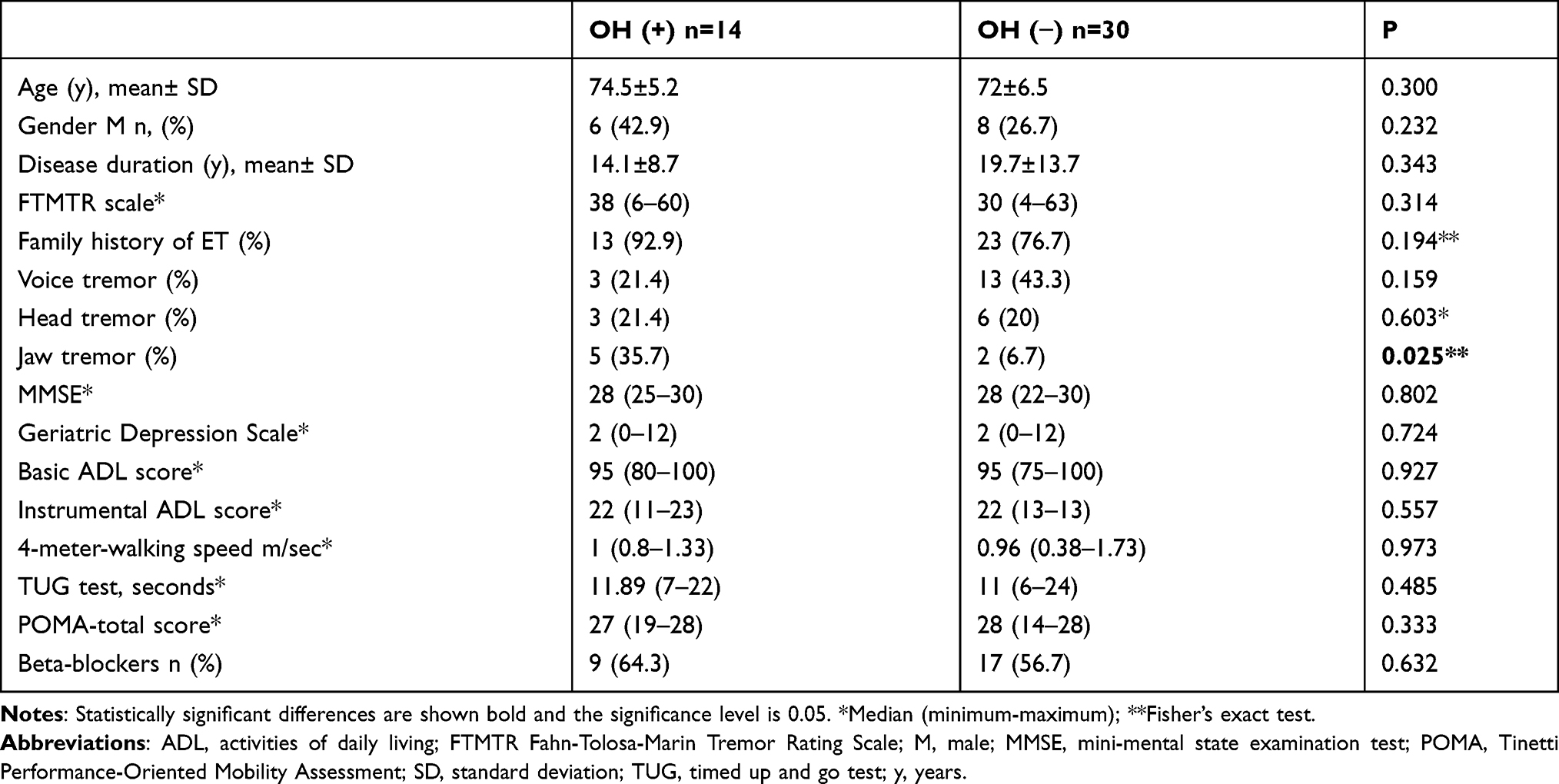 |
Table 2 The Demographic and Clinical Features of Patients with Essential Tremor |
In the ET patients with OH group, Spearman correlation analysis revealed that the decrease in systolic blood pressure (SBP) upon the change from the supine position to the upright at the 1st minute in the HUT (Δ SBP) was correlated with age (r=0.560, p= 0.038) and with MMSE scores (r=−0.690, p=0.009).
Discussion
This cross-sectional study demonstrated that the frequency of OH in elderly patients with ET was higher than healthy controls and that the majority of those with ET did not exhibit orthostatic symptoms. Moreover, most of the patients with jaw tremors had OH.
The frequency of OH has not been studied sufficiently in the literature. Kim et al10 reported it to be 12%, whereas the frequency was shown to be 32% of our study population. This discrepancy between both studies may be related to the differences such as the methodological approach and features of the patient groups. Compared to ours, the patients studied by Kim et al10 were younger with shorter disease durations. It is known that age is a risk factor for both hypertension (HT) and OH, and they often coexist due to their relation to autonomic and baroreflex dysfunctions.22 The prevalence of HT, an important cause of OH, in patients 60 years of age and above was reported as approximately 60–70%.23 Consequently, it is not surprising that the ET patients in the aforementioned study, with a lower prevalence of HT (40% of their ET patients had HT and 16% of the 25 controls), exhibited lower frequencies of OH. In addition, the discontinuation of the patient’s antihypertensive medications 7 days before evaluating postural blood pressure changes may have been the reason behind this difference observed in that study.
Interestingly, in our study, approximately 36% of ET patients with OH experienced jaw tremors, a type of midline tremor, while it was observed in only 7% of the patients without OH. Hence, it is reasonable to investigate every ET patient, in terms of OH, particularly those with midline tremors, because we demonstrated that patients with jaw tremors, who had been suffering for 10 years, displayed higher scores on the tremor severity scale, and also had tremors of the head and/or voice, and might have more OH than those without jaw tremors. Furthermore, considering that jaw tremors shared the same underlying pathophysiology of tandem gait difficulty in ET,24 it can be postulated that cerebellar dysregulation seems to be critical in the development of midline tremors. Additionally, considerable evidence suggests that control of postural blood pressure changes also involves pathways through the cerebellum of which disruption may result in deficits in adjustments during postural changes.7,25,26 Consequently, cerebellar dysregulation may become prominent in explaining the underlying pathophysiology of OH, at least, in patients with jaw tremors.
In addition to reduced GABAergic function within the locus coeruleus, and adrenergic changes following GABAergic dysfunction in ET patients,27 it can also be posited that autonomic dysfunction, such as OH, may be a result of this secondary locus coeruleus-noradrenergic deterioration in these patients. Nevertheless, these hypotheses need to be confirmed in the autopsy series of ET patients with and without OH.
Several studies indicated that both ET and OH are related to cognitive impairment.28–30 The present study demonstrated that the decrease in the systolic blood pressure within the 1st minute was correlated with lower MMSE scores. This may have been due to the fact that OH in SBP was commonly reported to be related to cerebrovascular events and vascular cognitive impairment.31–33 Nevertheless, prospective follow-up studies are needed to clarify this link between cognitive dysfunction in patients with OH and ET.
The unique aspect of this study is that, to the best of our knowledge, it is the first study of its kind to evaluate OH with HUT in elderly patients with ET. Also, all the patients underwent comprehensive geriatric assessment including clinical and neuropsychological assessment and OH was objectively evaluated using the HUT which is known to reveal satisfactory results on postural blood pressure changes. Furthermore, since patients with several comorbidities were included in the study, our results reflect real-life characteristics of older patients with ET. However, this study has a few limitations such as its retrospective design and small sample size.
Conclusion
To sum up, it appears that OH is a common accompanying condition in elderly patients with ET, particularly for those with jaw tremors, and as it is asymptomatic in most, it might be related to cognitive impairment in these patients. In addition, considering the potential complications of OH, it would be appropriate to evaluate OH in the follow-up and treatment of elderly patients with ET. In order to thoroughly evaluate the interrelationship between OH and ET in elderly patients, further longitudinal studies are needed.
Disclosure
The authors report no conflict of interest in this work.
References
1. Deuschl G, Bain P, Brin M. Consensus statement of the movement disorder society on tremor. Ad Hoc Scientific Committee. Mov Disord. 1998;13(Suppl 3):2–23. doi:10.1002/mds.870131303
2. Babij R, Lee M, Cortés E, Vonsattel JP, Faust PL, Louis ED. Purkinje cell axonal anatomy: quantifying morphometric changes in essential tremor versus control brains. Brain. 2013;136:3051–3061. doi:10.1093/brain/awt238
3. Louis ED, Faust PL, Vonsattel JP, et al. Neuropathological changes in essential tremor: 33 cases compared with 21 controls. Brain. 2007;130(Pt12):3297–3307. doi:10.1093/brain/awm266
4. Samuels ER, Szabadi E. Functional neuroanatomy of the noradrenergic locus coeruleus: its roles in the regulation of arousal and autonomic function part II: physiological and pharmacological manipulations and pathological alterations of locus coeruleus activity in humans. Curr Neuropharmacol. 2008;6(3):254–285. doi:10.2174/157015908785777193
5. Shoemaker JK, Goswami R. Forebrain neurocircuitry associated with human reflex cardiovascular control. Front Physiol. 2015;6:1–14. doi:10.3389/fphys.2015.00240
6. Baker J, Paturel JR, Kimpinski K. Cerebellar impairment during an orthostatic challenge in patients with neurogenic orthostatic hypotension. Clin Neurophysiol. 2019;130:189–195. doi:10.1016/j.clinph.2018.07.026
7. Baker J, Kimpinski K. Evidence of impaired cerebellar connectivity at rest and during autonomic maneuvers in patients with autonomic failure. Cerebellum. 2020;19(1):30–39. doi:10.1007/s12311-019-01076-8
8. Aydin AE, Soysal P, Isik AT. Which is preferable for orthostatic hypotension diagnosis in older adults: active standing test or head-up tilt table test? Clin Interv Aging. 2017;12:207–212. doi:10.2147/CIA.S129868
9. Soysal P, Veronese N, Smith L, et al. Orthostatic hypotension risk factors and health outcomes: an umbrella review of observational studies. Eur Geriatr Med. 2019;10:863–870. doi:10.1007/s41999-019-00239-4
10. Kim JS, Oh YS, Park HE, et al. Cardiovascular autonomic dysfunctions in elderly patients with essential tremor: comparison with healthy controls. Neurol Sci. 2016;37(5):711–716. doi:10.1007/s10072-015-2465-x
11. Damian A, Adler CH, Hentz JG, et al. Autonomic function, as self-reported on the SCOPA-autonomic questionnaire, is normal in essential tremor but not in Parkinson’s disease. Parkinsonism Relat Disord. 2012;18(10):1089–1093. doi:10.1016/j.parkreldis.2012.06.008
12. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–198. doi:10.1016/0022-3956(75)90026-6
13. Gungen C, Ertan T, Eker E, Yasar R, Engin F. Reliability and validity of the standardized Mini Mental State Examination in the diagnosis of mild dementia in Turkish population. Turk Psikiyatri Derg. 2002;13:273–281.
14. Durmaz B, Soysal P, Ellidokuz H, Isik AT. Validity and reliability of geriatric depression scale - 15 (Short Form) in Turkish older adults. North Clin Istanbul. 2017. doi:10.14744/nci.2017.85047
15. Podsiadlo D, Richardson S. The timed ‘Up & Go’: A test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39:142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
16. Tinetti ME. Performance-oriented assessment of mobility problems in elderly patients. J Am Geriatr Soc. 1986;34:119–126. doi:10.1111/j.1532-5415.1986.tb05480.x
17. Lawton M, Brody E. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179–186. doi:10.1093/geront/9.3_Part_1.179
18. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65.
19. Fahn S, Tolosa E, Marin C. Clinical rating scale for tremor. In: Jankovic J, Tolosa E, editors. Parkinson’s Disease and Movement Disorders. Baltimore, MD: Williams and Wilkins; 1993:271–280.
20. Parry SW, Reeve P, Lawson J, et al. The Newcastle protocols 2008: an update on head-up tilt table testing and the management of vasovagal syncope and related disorders. Heart. 2009;95(5):416–420. doi:10.1136/hrt.2007.136457
21. Shibao C, Lipsitz LA, Biaggioni I; American Society of Hypertension Writing Group. Evaluation and treatment of orthostatic hypotension. J Am Soc Hypertens. 2013;7(4):317–324. doi:10.1016/j.jash.2013.04.006
22. Biaggioni I. Orthostatic hypotension in the hypertensive patient. Am J Hypertens. 2018;31(12):1255–1259. doi:10.1093/ajh/hpy089
23. Fagard RH. Epidemiology of hypertension in the elderly. Am J Geriatr Cardiol. 2002;11(1):23–28. doi:10.1111/j.1076-7460.2002.00856.x
24. Louis ED, Rios E, Rao AK. Tandem gait performance in essential tremor: clinical correlates and association with midline tremors. Mov Disord. 2010;25(11):1633–1638. doi:10.1002/mds.23144
25. Harper RM, Gozal D, Bandler R, Spriggs D, Lee J, Alger J. Regional brain activation in humans during respiratory and blood pressure challenges. Clin Exp Pharmacol Physiol. 1998;25:483–486. doi:10.1111/j.1440-1681.1998.tb02240.x
26. Nisimaru N, Okahara K, Yanai S. Cerebellar control of the cardiovascular responses during postural changes in conscious rabbits. Neurosci Res. 1998;32:267–271. doi:10.1016/S0168-0102(98)00094-7
27. Shill HA, Adler CH, Beach TG, et al. Brain biochemistry in autopsied patients with essential tremor. Mov Disord. 2012;27(1):113–117. doi:10.1002/mds.24004
28. Bermejo-Pareja F. Essential tremor—a neurodegenerative disorder associated with cognitive defects? Nat Rev Neurol. 2011;7(5):273–282. doi:10.1038/nrneurol.2011.44
29. Bermejo-Pareja F, Louis ED, Benito-Leon J; Neurological Disorders in Central Spain (NEDICES) Study Group. Risk of incident dementia in essential tremor: a population-based study. Mov Disord. 2007;22(11):1573–1580. doi:10.1002/mds.21553
30. Freeman R, Abuzinadah AR, Gibbons C, Jones P, Miglis MG, Sinn DI. Orthostatic hypotension: JACC state-of-the-art review. J Am Coll Cardiol. 2018;72(11):1294–1309. doi:10.1016/j.jacc.2018.05.079
31. Ballard C, O’Brien J, Barber B, et al. Neurocardiovascular instability, hypotensive episodes, and MRI lesions in neurodegenerative dementia. Ann N Y Acad Sci. 2000;903:442–445. doi:10.1111/j.1749-6632.2000.tb06396.x
32. Yatsuya H, Folsom AR, Alonso A, Gottesman RF, Rose KM; ARIC Study Investigators. Postural changes in blood pressure and incidence of ischemic stroke subtypes: the ARIC study. Hypertension. 2011;57(2):167–173. doi:10.1161/HYPERTENSIONAHA.110.161844
33. Isik AT, Kocyigit SE, Kaya D, et al. The relationship between the most common subtypes of dementia and orthostatic hypotension in older adults. Dement Geriatr Cogn Disord. 2021. doi:10.1159/000512393
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.