Back to Journals » Advances in Medical Education and Practice » Volume 16
Organ-System-Based Curriculum in Medical Education: A Scoping Review
Authors Xia L ![]() , Jiang B, Zhang J, Yang K, Zhang Q, Zhu PY
, Jiang B, Zhang J, Yang K, Zhang Q, Zhu PY
Received 18 June 2025
Accepted for publication 27 August 2025
Published 13 September 2025 Volume 2025:16 Pages 1675—1681
DOI https://doi.org/10.2147/AMEP.S548097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Long Xia,1 Binglei Jiang,2 Jie Zhang,3 Kun Yang,3 Qiang Zhang,1 Ping-Yu Zhu1
1Department of Urology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China; 2Department of Ultrasound, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China; 3Department of Nephrology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China
Correspondence: Ping-Yu Zhu, Email [email protected]
Background: The Organ-System-Based Curriculum (OSC) has emerged as a transformative approach to medical education, gradually replacing traditional subject-based teaching. However, the existing literature on OSC has not been comprehensively evaluated.
Methods: Following the Joanna Briggs Institute (JBI) guidelines for scoping reviews, we systematically searched five databases—Medline (PubMed), Embase, ERIC, CINAHL, and Web of Science—for studies published in English between 2010 and 2024. We aimed to answer three key questions regarding OSC implementation strategies, effectiveness in medical education, and challenges in promotion. Two reviewers independently screened articles and extracted data based on predefined inclusion and exclusion criteria, with a third reviewer resolving disagreements.
Results: From an initial 1206 records, six studies met the inclusion criteria. Thematic analysis revealed: (1) Interdisciplinary team-based teaching with variable integration of basic sciences and clinical medicine, exemplified by improved student satisfaction and exam performance in integrated modules; (2) Effectiveness of academic interventions, including tutoring and problem-based learning, which enhanced clinical reasoning and examination outcomes; (3) Challenges, such as insufficient curriculum integration, limited student engagement in clinical practice, and difficulties integrating surgical education, highlighting areas needing improvement.
Conclusion: This scoping review synthesizes current evidence on OSC, demonstrating its potential to enhance multidimensional competencies in healthcare professionals. Addressing identified design and implementation challenges will be crucial to optimizing OSC’s impact and wider adoption.
Keywords: organ-system-based curriculum, medical education, undergraduate education
Background
Medical education, as the core component of training clinical physicians, has undergone continuous evolution over the past century. Traditional medical education follows a discipline-based model, emphasizing the separation of basic sciences and clinical medicine.1
For instance, subjects such as anatomy and physiology are taught independently from clinical disciplines like internal medicine and surgery, with instruction delivered in distinct, sequential stages. While this model offers advantages such as a clear structure and systematic content delivery, its lack of sufficient interdisciplinary integration often leads students to struggle with synthesizing knowledge across disciplines in clinical practice.2 This has resulted in challenges such as knowledge fragmentation and inadequate development of clinical reasoning skills. With the rapid growth of medical knowledge and increasing complexity in clinical practice, the traditional discipline-based model faces difficulties meeting modern demands for integrative competencies.3 In response, the Organ-System-Based Curriculum (OSC) has emerged as a pivotal reform in global medical education. OSC structures learning around organ systems or physiological functions, integrating foundational disciplines such as anatomy, physiology, pathology, and pharmacology horizontally, while closely linking them to clinical cases.4 This approach aims to cultivate an interdisciplinary knowledge network and enhance clinical reasoning skills among medical students.
Studies have shown that OSC improves examination performance,1 and fosters a holistic understanding of the structure-function-disease triad, increasing students’ confidence in addressing complex clinical scenarios.5 Additionally, OSC can shorten the transition period from basic sciences to clinical practice amid the prolonged training of clinical physicians.6 Technological advances have further reshaped OSC delivery; for example, online Case-Based Learning (CBL) via virtual platforms such as Zoom and patient simulations has expanded accessibility, particularly during the COVID-19 pandemic.7 Although meta-analyses suggest online CBL achieves comparable knowledge transmission to traditional methods, challenges remain regarding student self-discipline, technological infrastructure, and interactive engagement.8 Cultural contexts significantly influence OSC design. In Sweden, reforms integrating internships into curricula align with EU standards, whereas US medical schools emphasize early clinical immersion by shortening preclinical phases.9 Contrastingly, some Asian countries like Japan retain traditional discipline-based models due to longstanding educational conventions.10
Despite the increasing adoption of OSC and its demonstrated short-term benefits—such as improved exam performance and student satisfaction—high-quality evidence regarding its long-term effects remains limited, particularly in relation to clinical competence during residency and adaptability across diverse cultural contexts.11 This research gap restricts the ability of educators and policymakers to make fully informed decisions on curriculum development. Moreover, the successful implementation of OSC is contingent upon the engagement of key stakeholders: students, whose adaptation to new learning modalities is required; faculty, for whom adequate training and support are essential to ensure effective delivery of integrated content; and institutional leaders, who bear responsibility for resource allocation and curricular oversight. The absence of a unified framework for technology-driven curriculum innovations, combined with disparities in faculty development and resource distribution, has the potential to further exacerbate educational inequities.12 Addressing these challenges is essential for optimizing the effectiveness and sustainability of OSC.
In light of these gaps, a scoping review was conducted to systematically map the existing literature on OSC, identify knowledge gaps, and explore directions for future research. The review is intended to provide a foundational framework for curriculum design, address the needs of key stakeholders, including students and faculty, and ultimately enhance medical education on a global scale.
Methods
This study was conducted in accordance with the scoping review guidelines established by the Joanna Briggs Institute (JBI).13 To provide a comprehensive understanding of the application and impact of OSC in medical education, a scoping review of literature published between 2010 and 2024 in English and Chinese was undertaken. The review addressed three principal questions: (1) What implementation strategies and design features of OSC are currently employed across various countries and regions? (2) How effective are these curricula in enhancing medical students’ academic performance and clinical competencies? (3) What common challenges arise in the promotion of these curricula, and what potential improvements can be identified?
An initial search was performed in the Medline (PubMed) and PsycINFO (EBSCOhost) databases to identify relevant citations within the specified period. A search strategy was subsequently developed based on the retrieved citations and tailored to the study objectives. A comprehensive search was then carried out across Medline (PubMed), Embase (Embase.com), ERIC (EBSCOhost), CINAHL (EBSCOhost), and Web of Science (Science and Social Sciences Citation Index).
All retrieved records were imported into EndNote for management. Abstracts were independently screened by two reviewers to assess relevance, and any disagreements were resolved by a third reviewer. Full texts of selected articles were subsequently reviewed by two reviewers, with a third reviewer adjudicating discrepancies. Studies were excluded if they met any of the following criteria: (1) the publication was an abstract, thesis, or letter to the editor; (2) OSC was not described; (3) specific implementation strategies or measurable outcomes of OSC were not reported; or (4) the study was conducted outside the domain of clinical medical education, such as in nursing or pharmacy. Data extraction was performed independently by two reviewers using a standardized form, ensuring consistency and accuracy across studies.
Results
Our initial database search identified 1,206 articles. After removing duplicates, 1,179 unique records remained. Following title and abstract screening, we excluded 1,093 articles, and 86 were left for full-text review. After a thorough evaluation, we ultimately identified six articles that met our inclusion criteria.14–19 Figure 1 illustrates our screening process, and Table 1 summarizes the characteristics of various organ-system-based curricula.
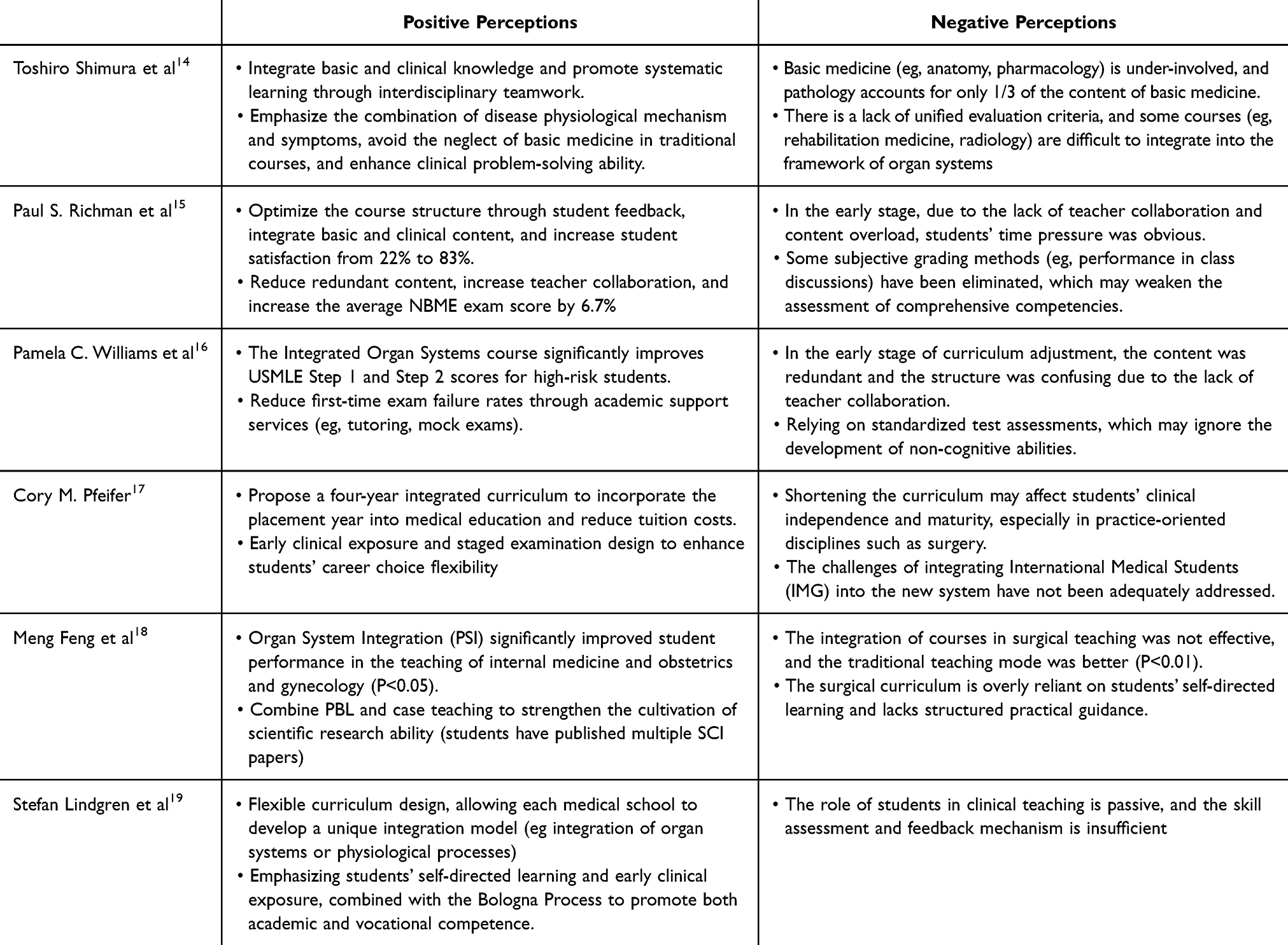 |
Table 1 Positive and Negative Perceptions of Various Organ-System-Based Curricula |
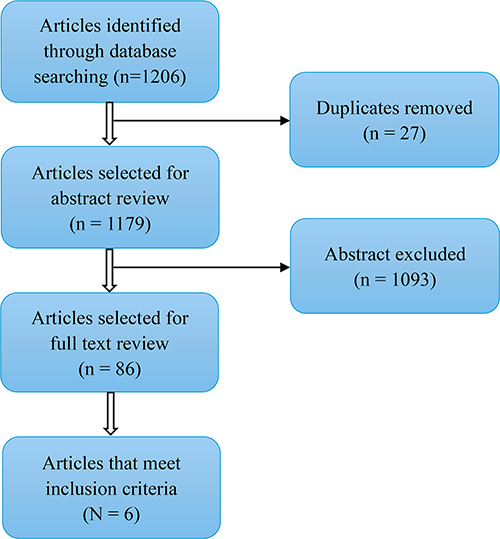 |
Figure 1 Study search strategy flowchart. |
Interdisciplinary Team-Based Teaching
A study from Japan indicates that integrated curricula, such as neurology modules, are delivered by multidisciplinary teams comprising neurosurgery, neurology, and pathology specialists. However, the integration of basic sciences, such as anatomy and pharmacology, remains insufficient, accounting for only 14% of the curriculum. In private medical schools, the integration of clinical medicine (91%) is significantly higher than that of basic sciences (9%).14 At Stony Brook University in the United States, the integration of cardiovascular, pulmonary, and renal (CPR) system courses allowed physiology and pathology to be taught concurrently. This reform led to an increase in student satisfaction from 22% to 83%, along with a 6.7% improvement in NBME examination scores.15
Effectiveness of Academic Interventions
At Meharry Medical College in the United States, academic support programs—including tutoring and simulated exams—were implemented for high-risk students. As a result, their USMLE Step 1 scores increased from 73.7 to 85, approaching the national average of 93. Additionally, Step 2 scores improved from 83.7 to 88.7. The integration of structured academic support within the curriculum led to a higher first-time exam pass rate and a reduction in student attrition.16
Studies from Japan, China, and the United States have incorporated Problem-Based Learning (PBL) and case-based discussions into integrated curricula. At Xi’an Jiaotong University, a “role-playing–classroom debate–faculty Q&A” model was introduced, significantly enhancing students’ clinical reasoning skills. Moreover, the number of SCI-indexed publications authored by students increased notably, with six papers published in journals with an impact factor greater than 5.14,17,18
Challenges and Unsolved Problems
According to the survey of Japanese teachers, 58% believe that the curriculum is not well integrated, and 66% call for greater participation in basic medicine. The Swedish assessment pointed out that students are mostly “bystanders” in clinical practice, and there is a lack of active role design.14,19
Difficulty in surgical integration: The surgical curriculum of Xi’an Jiaotong University in China relies on self-directed learning and hands-on ability training, and the integration effect is not good, suggesting that the teaching methods need to be improved.18
Discussion
The OSC approach was developed in the mid-20th century, with its primary objective being the dismantling of traditional disciplinary boundaries and the integration of theoretical knowledge with clinical practice. As medical technology advanced, higher demands were placed on teaching methodologies. The traditional discipline-centered model was increasingly recognized as limited, characterized by fragmented knowledge and insufficient integrative application skills.20 In response, the adoption of organ-centered learning was promoted, facilitating more comprehensive acquisition and practical application of medical knowledge among students.
The greatest advantage of the OSC approach in clinical medical education lies in its ability to facilitate knowledge integration and practical application. In traditional discipline-oriented teaching, various medical fields are often taught in isolation. As a result, students studying pathology, pharmacology, or anatomy frequently struggle to connect knowledge across disciplines.21
OSC dismantles these barriers by fusing content across multiple subjects, enabling students to better grasp the complexity of the human body. For instance, when studying a specific organ system—such as the heart—students do not only learn about its anatomy and physiology, but also engage with relevant pathology, therapeutic interventions, and the biochemical foundations of cardiovascular pharmacology. This interdisciplinary linkage enhances students’ intuitive understanding of the holistic and practical nature of medical knowledge.22,23 Moreover, OSC promotes teaching innovation by fostering collaboration among multidisciplinary teaching teams. Through team-teaching strategies, students benefit from the expertise of multiple specialists in a single session, gaining a more comprehensive perspective. Research has shown that this model not only increases student engagement and motivation but also improves knowledge retention and application in clinical practice.24
Despite its many advantages, the implementation of OSC presents significant challenges for both educators and institutions. One of the primary obstacles is faculty development. OSC requires instructors to possess a broad, interdisciplinary knowledge base, yet many educators are accustomed to teaching within the confines of a single discipline. This makes the shift to integrated teaching not only conceptually difficult but also logistically challenging.25 Secondly, structural challenges in curriculum design arise. Successfully integrating diverse subject matter to support OSC demands meticulous planning and coordination. This includes organizing teaching content for each organ system, allocating instructional time appropriately, and aligning the integrated curriculum with existing national or institutional standards.26 Furthermore, the logical sequencing of topics across disciplines must be handled with care to avoid redundancies or content gaps. Coherence in delivery is crucial to ensure that students can form meaningful connections across subjects. Another critical area is assessment reform. Traditional exams may fall short in evaluating students’ ability to synthesize and apply knowledge. As a result, there is a growing need for diversified assessment tools that better reflect the integrated nature of learning in OSC. Methods such as Problem-Based Learning (PBL) assessments, skills-based evaluations, and clinical reasoning simulations are recommended to comprehensively measure both conceptual understanding and practical competency.24 These challenges underscore the need for flexibility and adaptability among educators and policymakers to meet the evolving demands of modern medical education.
To facilitate further reform in OSC, optimization of pedagogical resources is proposed as a foundational strategy, given their critical role in augmenting educational outcomes. In traditional medical education, the predominant reliance on compartmentalized textbooks and monolithic instructional media has constrained learners’ interdisciplinary comprehension. Contemporary educational paradigms now recognize resource diversification as an educational imperative, wherein strategic integration of multimedia modalities demonstrably enhances students’ multidimensional understanding of organ systems.27 Furthermore, interactive engagement and practical application have been identified as essential components of this pedagogical framework. Systematic enhancement of peer-to-peer and student-instructor collaboration mechanisms enables learners to construct meaningful cognitive linkages across complex medical domains.28
Notably, the strategic incorporation of information technology has redefined modern medical education. Within OSC, technological integration not only augments learning accessibility but also catalyzes innovative pedagogical strategies. For instance, massive open online course (MOOC) platforms facilitate ubiquitous knowledge acquisition, with empirical studies validating the efficacy of video-based learning modules and real-time interactive assessments in reinforcing clinical competencies.29
This investigation has several inherent limitations that warrant consideration. Primarily, the paucity of dedicated literature comprehensively delineating OSC frameworks necessitates that findings should be interpreted with caution, particularly regarding potential discrepancies in cross-study replicability. Furthermore, considerable heterogeneity in strategic implementation across national contexts manifested through divergent curricular designs and assessment methodologies may constrain the generalizability of observed educational outcomes, as institutional priorities and cultural determinants differentially influence programmatic objectives.
Conclusion
Our research shows that OSC significantly improves test results, student satisfaction, and clinical reasoning skills. However, the continued underrepresentation of basic sciences, limited integration of surgical courses, and insufficient active participation of learners suggest that true multidisciplinary integration has not yet been achieved. Future reforms should prioritize strengthening the connection between basic and clinical, optimizing surgical teaching strategies, and promoting active participation to ensure the sustainable improvement of the quality of medical education.
Data Sharing Statement
The datasets used and analyzed during the study are available from the corresponding author on reasonable request.
Consent for Publication
All authors agree to the publication of this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Sichuan Provincial First-Class Undergraduate Course, “Structure, Function, and Diseases of the Urological and Male Reproductive System” (Grant No. YLKC02211). These grants provided financial support and assisted with this study’s implementation.
Disclosure
The authors declare no competing interests in this work.
References
1. Burgess A, Matar E, Roberts C, et al. Scaffolding medical student knowledge and skills: team-based learning (TBL) and case-based learning (CBL). BMC Medical Education. 2021;21(1):238. doi:10.1186/s12909-021-02638-3
2. Harden RM, Sowden S, Dunn WR. Educational strategies in curriculum development: the SPICES model. Medical Education. 1984;18(4):284–297. doi:10.1111/j.1365-2923.1984.tb01024.x
3. Thistlethwaite JE, Davies D, Ekeocha S, et al. The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME Guide No. 23. Medical Teacher. 2012;34(6):e421–44. doi:10.3109/0142159X.2012.680939
4. Cen XY, Hua Y, Niu S, Yu T. Application of case-based learning in medical student education: a meta-analysis. European Review for Medical and Pharmacological Sciences. 2021;25(8):3173–3181. doi:10.26355/eurrev_202104_25726
5. Kulasegaram K, Mylopoulos M, Tonin P, et al. The alignment imperative in curriculum renewal. Medical Teacher. 2018;40(5):443–448. doi:10.1080/0142159X.2018.1435858
6. Donkin R, Yule H, Fyfe T. Online case-based learning in medical education: a scoping review. BMC Medical Education. 2023;23(1):564. doi:10.1186/s12909-023-04520-w
7. Duan Y, Li Z, Wang X, Gao Z, Zhang H. Application of online case-based learning in the teaching of clinical anesthesia for residents during the COVID-19 epidemic. BMC Medical Education. 2021;21(1):609. doi:10.1186/s12909-021-03047-2
8. Thibaut D, Schroeder KT. A case-based learning approach to online biochemistry labs during COVID-19. Biochemistry and molecular biology education: a bimonthly publication of the International Union of Biochemistry and Molecular Biology. Biochemistry and Molecular Biology Education: a Bimonthly Publication of the International Union of Biochemistry and Molecular Biology. 2020;48(5):484–485. doi:10.1002/bmb.21408
9. Campbell N, Wozniak H, Philip RL, Damarell RA. Peer-supported faculty development and workplace teaching: an integrative review. Medical Education. 2019;53(10):978–988. doi:10.1111/medu.13896
10. Lomis K, Amiel JM, Ryan MS, et al. Implementing an Entrustable Professional Activities Framework in Undergraduate Medical Education: early Lessons From the AAMC Core Entrustable Professional Activities for Entering Residency Pilot. Academic Medicine: Journal of the Association of American Medical Colleges. 2017;92(6):765–770. doi:10.1097/ACM.0000000000001543
11. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–1958. doi:10.1016/S0140-6736(10)61854-5
12. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology. 2018;18(1):143. doi:10.1186/s12874-018-0611-x
13. Peters MD, Godfrey C, McInerney P, Munn Z, Tricco AC. Khalil HJJmfes. Scoping Reviews. 2020;10:
14. Shimura T, Aramaki T, Shimizu K, Miyashita T, Adachi K, Teramoto A. Implementation of integrated medical curriculum in Japanese medical schools. Journal of Nippon Medical School = Nippon Ika Daigaku Zasshi. 2004;71(1):11–16. doi:10.1272/jnms.71.11
15. Richman PS, Olvet DM, Ahmad S, Chandran L. Use of student feedback to drive quality improvement (QI) in a preclinical U.S. medical school course. Medical Education Online. 2019;24(1):1583968. doi:10.1080/10872981.2019.1583968
16. Williams PC, Epps AC, McCammon S. The strategic impact of a changing curriculum and learning environment on medical students’ academic performance. Journal of the National Medical Association. 2011;103(9–10):802–810. doi:10.1016/S0027-9684(15)30433-8
17. Pfeifer CM. A progressive three-phase innovation to medical education in the United States. Medical Education Online. 2018;23(1):1427988. doi:10.1080/10872981.2018.1427988
18. Fang C, Li M, Liu L et al. A phased analysis of the teaching effect of the eight-year organ-system integration clinical course. Medicine and Philosophy. 2024;45(7):70–75.
19. Lindgren S, Brännström T, Hanse E, et al. Medical education in Sweden. Medical Teacher. 2011;33(10):798–803. doi:10.3109/0142159X.2011.570816
20. Adkoli B, SJTP P. Systems approach in medical education: the thesis, antithesis, and synthesis. Tropical Parasitology. 2019;9(1):3–6. doi:10.4103/tp.TP_7_19
21. Obi CO, Onosogbe M, Ehimen AG, et al. Comparison of the integrated organ/systems-based curriculum with the traditional subjects-based medical curriculum: short communication. Annals of Medicine and Surgery. 2022;73:103116. doi:10.1016/j.amsu.2021.103116
22. Attardi SM, Venuti JMJTFJ. Medical Student Learning Experiences in Organ System Course Sessions using a Histology and Embryology Team‐taught Integrated Format. FASEB J. 2018;32:241.
23. Lee CT, Wang JYJASE. Interactive audio human organ model combined with team‐based learning improves the motivation and performance of nursing students in learning anatomy and physiology. Anatomical Sci Educ. 2024;17(2):307–318. doi:10.1002/ase.2350
24. Lundmark PE. The Great Organ System Debates. Adv Physiol Educ. 2023;2023:1.
25. Shehnaz SI, Sreedharan JJM. Students’ perceptions of educational environment in a medical school experiencing curricular transition in United Arab Emirates. Medical Teacher. 2011;33(1):e37–e42. doi:10.3109/0142159X.2011.530312
26. Brands MW, Schumacher LJA. Active learning strategies to teach renal-cardiovascular integration with high student-to-teacher ratios. Advances in Physiology Education. 2009;33(4):282–285. doi:10.1152/advan.00055.2009
27. Vázquez R, Riesco JM, Juanes JA, Blanco E, Rubio M, Carretero JJEJo A. Educational strategies applied to the teaching of anatomy. The evolution of resources. Eur J Anatomy. 2007;11:31.
28. Hsieh MH, Shih F-J, Sheu S-J, Wang -S-S, F-JJM S. Using an informatics education strategy to resolve the dilemma of teaching transplantation in medical institutions: multidisciplinary medical team perspectives. Medicine. 2018;97(43):e12809. doi:10.1097/MD.0000000000012809
29. Hsieh MH, Shih F-J, Wang -S-S, F-JJT S. Using Informatic Education Strategy to Break Through the Dilemma of Teaching Transplantation in Medical Institutions–Compare medical and administrative informatic team perspectives. Transplantation. 2018;102:S819.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.