Back to Journals » Cancer Management and Research » Volume 14
Oral Squamous Cell Carcinoma Metastasizing to the Heart: A Case Report from Taiwan
Authors Hsu JY ![]() , Lin HY, Yang YP
, Lin HY, Yang YP ![]()
Received 18 April 2022
Accepted for publication 6 October 2022
Published 21 October 2022 Volume 2022:14 Pages 3063—3070
DOI https://doi.org/10.2147/CMAR.S364150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmet Emre Eşkazan
Jhe-Yuan Hsu,1 Hsuan-Yu Lin,2 Yuan-Po Yang3– 5
1Division of General Practice, Department of Medical Education, Changhua Christian Hospital, Changhua, Taiwan; 2Division of Hematology/Oncology, Changhua Christian Hospital, Changhua, Taiwan; 3Department of Cardiology, Changhua Christian Hospital, Changhua, Taiwan; 4Ph.D Program in Tissue Engineering and Regenerative Medicine, National Chung Hsing University and National Health Research Institutes, Taichung, Taiwan; 5Institute of Biomedical Engineering and Nanomedicine, National Health Research Institutes, Miaoli, Taiwan
Correspondence: Yuan-Po Yang, Department of Cardiology, Changhua Christian Hospital, No. 135, St. Nan-xiao, Chang-Hua City, 500209, Taiwan, Tel +886-917-153-130, Fax +886 04-7232942, Email [email protected]
Background: The most common sites for metastasis from head and neck cancers are the lungs, bones, and liver. We present a rare case of squamous cell carcinoma of the buccal mucosa that metastasized to the right ventricle, pericardium, and bilateral lungs.
Methods: A 61-year-old man with oral squamous cell carcinoma (cT4aN2cM0) exhibited mass-like echogenicity adhering to the right ventricular free wall that was accidentally discovered after concurrent chemoradiotherapy. A biopsy of the mass confirmed the oral origin of the metastasis.
Results: The patient received palliative care and died 1 month after being diagnosed with cardiac involvement.
Conclusion: Cardiac involvement is often not assessed because of its low prevalence. Cardiac metastasis should be considered in patients with malignancies presenting with nonspecific cardiac symptoms.
Keywords: heart, metastasis, squamous cell carcinoma, head and neck cancer, biopsy
Introduction
According to statistics from the World Health Organization, cancer was the second leading cause of death in 2018, accounting for one in six deaths worldwide. Head and neck cancers account for 3% and 4% of the malignancies in the United States and Europe, respectively.1,2 The most common sites for metastasis from head and neck cancer are the lungs, bones, and liver.3 However, in this case report, we present a rare case in which squamous cell carcinoma of the buccal mucosa metastasized to the right ventricle, pericardium, and bilateral lungs.
Case Presentation
A 61-year-old man with no personal history or family history of malignancy, but with a long history of smoking presented with mouth pain and an ulcerative mass over the left lower gingiva. He was diagnosed with squamous cell carcinoma in October 2019 following an incisional biopsy of the left lower ridge. Computed tomography (CT) of the deep neck and whole-body positron emission tomography (PET) revealed an extensive soft tissue mass lesion in the left buccomasseteric region, measuring 81×24 mm, with retromolar trigone and skin invasion and destruction of the cortex of the left side of the mandible. Metastatic lymphadenopathy was observed in the left level II neck up to 21 mm, left submandibular region, right anterior submandibular region, and submental region. According to the eighth edition of the staging manual of the American Joint Committee on Cancer, the clinical stage was T4aN2cM0 (stage IVA). The patient began treatment with neoadjuvant chemotherapy on November 19, 2019. However, CT performed on February 11, 2020, demonstrated a left buccal cancer measuring 75×22 mm. Metastatic lymphadenopathy was observed at the bilateral level Ia/Ib and left level II, and the size of right level I lymph nodes had increased. A new lymph node metastasis was discovered in the left parotid gland. Therefore, concurrent chemoradiotherapy (CCRT), including cetuximab, docetaxel, cisplatin, and radiotherapy, was initiated on March 13, 2020, at a dose of 7000 cGy/35 fractions. On May 13, 2020, CT performed for post-CCRT evaluation revealed obvious resolution of the previously noted left buccal cancer, with only a residual ulcerated lesion in the left lower gingiva with necrosis of the left side of the mandibular body. Consequently, the patient was referred to the Otorhinolaryngology Department for possible surgical intervention.
However, echocardiography performed on July 31, 2020, which was recommended owing to chest pain, revealed a 4.97×2.72 cm mass-like echogenicity adhering to the right ventricular free wall (Figure 1). Furthermore, chest CT performed on August 6, 2020, demonstrated a new lesion in the right ventricle near the pulmonary valve, and metastasis in the pericardium was ruled out (Figure 2). Mild pericardial effusion was observed. The patient was admitted to the Oncology Service for further survey and treatment. Subsequent whole-body PET performed on August 14, 2020 revealed metastases in the right submandibular and mediastinal lymph nodes, bilateral lungs, heart, and pericardium (Figure 3). On August 19, 2020, cardiac magnetic resonance imaging revealed a lobulated and infiltrative enhancing soft tissue mass (measuring approximately 4.5 cm), mainly located in the anterior wall of the right ventricle, with heterogeneous contrast enhancement and an increase in pericardial effusion (Figure 4). The patient complained of intermittent chest tightness. Electrocardiography (ECG) showed atrial fibrillation with a rapid ventricular response and new-onset ST-segment changes. Since the laboratory data showed no elevation of cardiac enzymes, the symptoms were attributed to the right ventricular mass. After discussing with a cardiologist, the patient, and his family, a biopsy of the right ventricular mass was performed on August 21, 2020. We set the 6-French sheath over right internal jugular vein and directed the guiding catheter to face the right ventricular septum. Then, we used the bioptome, which is a catheter with jaws in its tip, for cardiac muscle biopsy through the multi-purpose 6-French and 45 cm guiding catheter. We got 4 pieces of specimens and used contrast medium to check the heart rupture or not after the biopsy. The formal pathological report showed rare, atypical oval to polygonal tumor cells with hyperchromatic nuclei in fibrotic stroma. Some reactive mesothelial cells were also present. Immunohistochemically, the tumor cells were cytokeratin 5/6(+), calretinin(–), p63(+), and thyroid transcription factor-1(–). Therefore, metastatic squamous cell carcinoma was suspected. Surgical intervention for pericardial effusion was not feasible owing to the high risk of anesthesia complications and airway difficulty. We also consulted a radiologist regarding the possibility of radiotherapy for the right ventricular tumor. However, owing to its high risk and uncertainty, radiotherapy was not feasible. On August 31, 2020, the patient was transferred to the hospice ward after being informed of his condition and having a thorough discussion. On September 2, 2020, approximately 1 month after discovering the cardiac metastasis, the patient experienced a cardiac arrest with no spontaneous breathing.
 |
Figure 1 Echocardiogram performed on July 31, 2020 showing a 4.97×2.72 cm mass-like echogenicity on the right ventricular free wall. Abbreviations: Ao, aorta; LV, left ventricle; RA, right atrium; RV, right ventricle. |
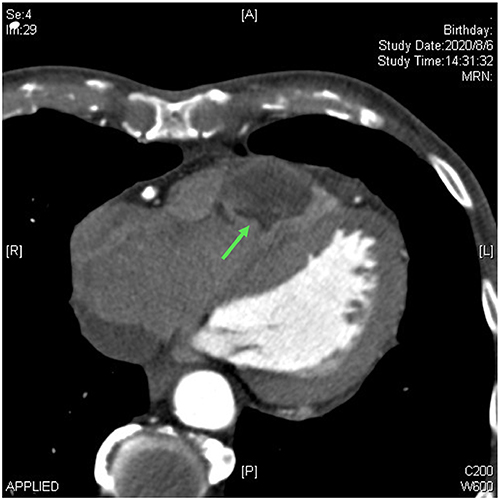 |
Figure 2 Chest computed tomography performed on August 6, 2020, showing a new lesion in the right ventricle near the pulmonary valve. |
 |
Figure 3 PET scan image of the heart on August 14, 2020, revealing increased FDG uptakes in the right submandibular and mediastinal lymph nodes, bilateral lungs, heart, and pericardium which impress metastases. |
 |
Figure 4 Cardiac magnetic resonance imaging on August 19, 2020, revealing a lobulated and infiltrative enhancing soft tissue mass, mainly located in the anterior wall of the right ventricle. |
Oral informed consent was obtained from the patient examined in this study.
Discussion
Detection of primary cardiac tumors is rare. A study that examined 22 large autopsy series showed that the prevalence of primary cardiac tumors was approximately 0.02%.4 Therefore, we can logically infer that cardiac malignancies are typically metastatic. According to Duband et al, common primary sites of cardiac metastasis include lung cancer, breast cancer, melanoma, and leukemia.5 Conversely, the lung, bone, and liver are the most frequent distant metastatic sites of head and neck cancer.3 In our case, the primary tumor was oral squamous cell carcinoma, which rarely metastasizes to the heart.
The mechanisms underlying cardiac metastases are unclear. However, Gould6 identified the following five hypotheses for mechanisms of metastasis: direct extension, hematogenous spread via the coronary arteries, retrograde dissemination through lymphatic channels, pulmonary venous invasion with endocardial implantation, and tumor thrombus. The protection of the myocardium is mainly attributed to the following three factors: tumor seeding by the rapid flow of blood, minimal lymphatic connections, and some other vague metabolic features.6
Only 10 cases of antemortem diagnosis of cardiac metastasis of head and neck cancer have been reported in the literature. This may be because clinical manifestations of cardiac metastases are not obvious. There are no significant or specific symptoms or signs in the initial stage unless the cardiac metastasis progresses to a severe degree or extends to systemic disease. After our collection and comparison of the data from previous literature and our case,7–14 we found some similarities and differences (Table 1). The mean age of the 11 patients was approximately 55 years, and the sex distribution was almost equal. No metastases were found when these patients were newly diagnosed with head and neck squamous cell carcinoma. There is a trend that the original tumor sites tend to be in the oral cavity rather than the throat. Treatment of the primary site included surgery, chemotherapy, and radiotherapy. Apart from the heart, metastases were located in the lungs, bones, and thyroid. Symptoms and signs were variable, including chest pain, shortness of breath, palpitations, and pericardial effusion. In addition, some cardiac metastases could be detected by physical examination, such as cardiac murmur, edema, and decreased breathing sounds. Most of these patients had abnormal ECG findings, ST-segment elevation or depression, atrial fibrillation with a rapid ventricular response, right bundle branch block, and Q-wave. However, owing to these nonspecific findings, imaging studies, especially echocardiography, have been used to detect cardiac metastasis.
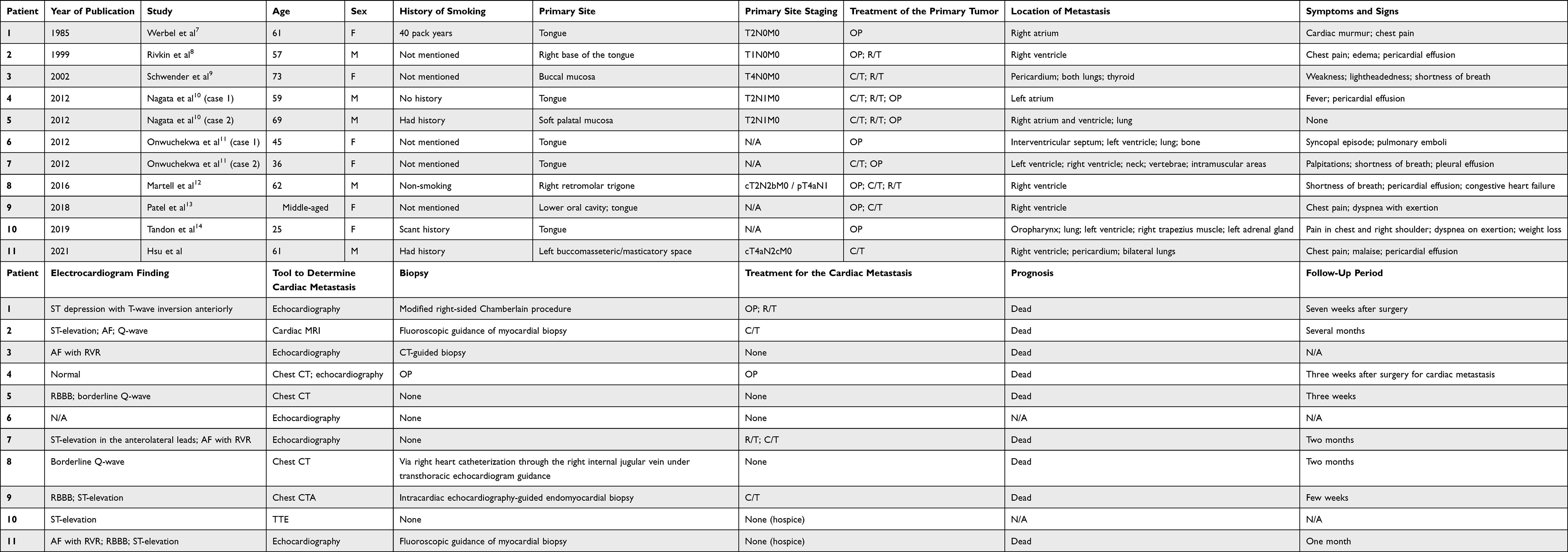 |
Table 1 Previous Cases of Metastasis to the Heart from Head and Neck Cancers That Were Diagnosed Before Death |
An increasing number of safer facilities and methods for obtaining cardiac tumor tissues by biopsy have been developed in recent years. Fluoroscopic guidance is a commonly used method for myocardial biopsy. Other methods, such as CT-guided biopsy and intracardiac echocardiography-guided endomyocardial biopsy, have also been performed in previous cases.9,13 The safety of each method relies not only on operator competence but also on patient conditions, such as the location of the tumor, renal function, and comorbidities.
Since there is no generally acknowledged therapy for cardiac tumors, it is uncertain whether the cytology of cardiac tumors influences the treatment. The role of surgery, choice of chemotherapy regimen, and dosage of radiotherapy also remain unclear. One case of surgical removal of the cardiac tumor has been reported, but it is controversial whether surgery prolongs the life span.10 In addition, compared to quality of life with palliative treatment, quality of life after the operation has not been adequately assessed. Owing to the lack of guidelines for therapy, the prognosis of cardiac metastases is poor and warrants further research. Hence, in patients with malignancies, the medical staff must always consider the possibility of cardiac metastasis. Furthermore, the benefits and risks of any type of therapy should be carefully evaluated.
Conclusion
The most common origins of cardiac metastasis are lung cancer, breast cancer, melanoma, and leukemia.5 Nevertheless, in our case, the primary tumor was an oral squamous cell carcinoma. Clinical manifestations included chest pain and pericardial effusion with echocardiographic abnormalities. A ventricular tumor was incidentally detected on preoperative assessment. After reviewing the literature, we deduced some prodromes and common objective findings. Echocardiography is the most commonly used tool for discovering a mass in the heart. The choice of biopsy method depends on the experience of the operator, patient’s condition, and accessibility of the facility. The treatment of cardiac metastases includes resection, chemotherapy, and radiation therapy. However, more data are needed to predict patient outcomes and prognoses.10,15 Although the possibility of a cardiac metastasis is relatively low, it should be suspected in patients with a history of squamous cell carcinoma of the head and neck who present with cardiovascular symptoms and signs or any abnormal findings in laboratory data or images.
Abbreviations
CT, computed tomography; PET, positron emission tomography; CCRT, concurrent chemoradiotherapy; ECG, electrocardiography.
Ethics Approval and Informed Consent
The collection of data, analysis and publication were conducted in accordance with the declaration of Helsinki. Consent to participate was obtained prior to the commencement of the study from the brother of the deceased patient.
Consent for Publication
Consent for publication was obtained from the deceased patient’s family, and no institutional approval was required to publish the case details.
Acknowledgments
We thank the colleagues in Changhua Christian Hospital make all-out effort to take care of the patient. Besides, the patient and his families agree to publish their experience to raise the awareness of heart tumor which is metastasized from oral squamous cell carcinoma.
Funding
This study did not receive any external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
2. Gatta G, Botta L, Sánchez MJ, et al. Prognoses and improvement for head and neck cancers diagnosed in Europe in early 2000s: the EUROCARE-5 population-based study. Eur J Cancer. 2015;51(15):2130–2143. doi:10.1016/j.ejca.2015.07.043
3. Probert JC, Thompson RW, Bagshaw MA. Patterns of spread of distant metastases in head and neck cancer. Cancer. 1974;33(1):127–133. doi:10.1002/1097-0142(197401)33:1<127::AID-CNCR2820330119>3.0.CO;2-L
4. Reynen K. Frequency of primary tumors of the heart. Am J Cardiol. 1996;77(1):107. doi:10.1016/S0002-9149(97)89149-7
5. Duband S, Paysant F, Scolan V, Forest F, Péoc’h M. Sudden death due to myocardial metastasis of lingual squamous cell carcinoma. Cardiovasc Pathol. 2011;20(4):242–243. doi:10.1016/j.carpath.2010.07.002
6. Gould SE. Pathology of the Heart and Blood Vessels.
7. Werbel GB, Skom JH, Mehlman D, Michaelis LL. Metastatic squamous cell carcinoma to the heart. Unusual cause of angina decubitus and cardiac murmur. Chest. 1985;88(3):468–469. doi:10.1378/chest.88.3.468
8. Rivkin A, Meara JG, Li KK, Potter C, Wenokur R. Squamous cell metastasis from the tongue to the myocardium presenting as pericardial effusion. Otolaryngol Head Neck Surg. 1999;120(4):593–595. doi:10.1053/hn.1999.v120.a84489
9. Schwender FT, Wollner I, Kunju LP, Nakhleh RE, Chan KM. Squamous cell carcinoma of the buccal mucosa with metastases to the pericardial cavity, lung and thyroid. Oral Oncol. 2002;38(1):114–116. doi:10.1016/S1368-8375(01)00021-5
10. Nagata S, Ota K, Nagata M, Shinohara M. Cardiac metastasis of head and neck squamous cell carcinoma. Int J Oral Maxillofac Surg. 2012;41(12):1458–1462. doi:10.1016/j.ijom.2012.07.017
11. Onwuchekwa J, Banchs J. Early cardiac metastasis from squamous cell carcinoma of the tongue in 2 patients. Tex Heart Inst J. 2012;39(4):565–567.
12. Martell K, Simpson R, Skarsgard D. Solitary myocardial metastasis from locoregionally controlled squamous cell carcinoma of the oral cavity. Cureus. 2016;8(6):e650. doi:10.7759/cureus.650
13. Patel H, Francke M, Stahura H, El-Hajjar M, Schulman-Marcus J. Solitary cardiac metastasis from primary oral squamous cell carcinoma presenting as ST-elevation MI. BMJ Case Rep. 2018;2018:bcr2018224732. doi:10.1136/bcr-2018-224732
14. Tandon V, Kethireddy N, Balakumaran K, Kim AS. Metastatic squamous cell carcinoma to the heart: an unusual cause of ST elevation-a case report. Eur Heart J Case Rep. 2019;3(2):ytz029. doi:10.1093/ehjcr/ytz029
15. Zemann W, Feichtinger M, Kowatsch E, Schanbacher M, Kärcher H. Cardiac metastasis after squamous cell carcinoma of the oral cavity: case report. Br J Oral Maxillofac Surg. 2007;45(5):425–426. doi:10.1016/j.bjoms.2005.12.017
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.