Back to Journals » International Medical Case Reports Journal » Volume 18
Oral Opportunistic Infection Induced by Stress and Silent Type 2 Diabetes Mellitus in Young Adult Patient: A Case Report
Authors Karina D ![]() , Heldayani I, Hidayat W
, Heldayani I, Hidayat W ![]()
Received 22 July 2024
Accepted for publication 20 November 2024
Published 11 January 2025 Volume 2025:18 Pages 59—66
DOI https://doi.org/10.2147/IMCRJ.S488127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Dhini Karina,1 Iin Heldayani,1 Wahyu Hidayat2
1Oral Medicine Residency Program, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia; 2Department of Oral Medicine, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Wahyu Hidayat, Department of Oral Medicine, Faculty of Dentistry, Universitas Padjadjaran, Jalan Sekeloa Selatan I, Bandung, 40132, Indonesia, Tel +6287822404343, Email [email protected]
Introduction: Opportunistic infections (IO) are infections of microbiota (fungi, viruses, bacteria, or parasites) that generally do not cause disease but turn into pathogens when the body’s defense system is compromised. This can be triggered by various factors, one of which is due to a weakened immune system due to Diabetes Mellitus (DM), which increases the occurrence of opportunistic infections, especially in the oral cavity. Fungal (oral candidiasis) and viral (recurrent intraoral herpes) infections can occur in the oral cavity of DM patients. Recurrent intraoral herpes (RIH) is generally a recurrent herpes virus infection with one of the triggers being stress.
Objective: To determine the role of stress and silent type 2 DM and which is thought to trigger opportunistic infections in oral cavity.
Case: A 34-year-old man was referred with complaints of white patches in the mouth, sore throat a difficulty swallowing and opening the mouth. Extraoral examination, yellow-black crusts were found on the lips. Intraoral and tongue examination revealed white plaque that could be scraped off, and a mouth mirror was attached. The hard palate showed vesicles that spread to the soft palate. Laboratory tests were abnormal for blood sugar, anti-HSV-1 IgG, and presence of hyphae. Mild anxiety and moderate stress. The working diagnosis was pseudomembranous candidiasis RIH, exfoliative cheilitis, and xerostomia. Differential diagnosis was erythema multiforme.
Case Management: Pharmacologic dental management was fluconazole injection, acyclovir, NaCL 0.9%, chlorine dioxide mouthwash, and petroleum jelly. Non-pharmacologic therapy dental included oral hygiene instruction and education on oral therapy and referral to the internal medicine clinic for DM management. After two weeks of collaborative treatment between oral medicine and internal medicine, there was significant improvement.
Conclusion: Silent type 2 DM and stress can cause a decrease in the immune system, triggering opportunistic infections, namely RIH and candidiasis.
Keywords: diabetes mellitus, immunosuppression, oral opportunistic infections, stress
Introduction
Opportunistic infections are diseases caused by microbes and occur in patients with weakened immune systems, changes in the microbiota, or damage to epithelial tissue.1 Diabetes mellitus (DM) is a chronic metabolic disease characterized by hyperglycemia due to either a deficiency of insulin secretion or resistance to the action of insulin or both.2 Silent DM is DM with patients who do not realize or do not know that they have the disease. The prevalence of silent DM, according to the Centers for Disease Control and Prevention, is around seven million people and usually in young adults. The diagnosis of silent DM is made by looking at HbA1C levels. Early diagnosis is important in order to prevent high morbidity and mortality in silent or unknown DM.3 Viral and candida infections are opportunistic infections of the oral cavity in patients with diabetes mellitus that are associated with uncontrolled hyperglycemia.4–6
Herpes simplex virus (HSV) is a herpes virus whose natural reservoir is in humans.6 This virus consists of HSV-1 and HSV-2, belongs to the family Herpesviridae (herpes viruses), and has double- stranded deoxyribonucleic acid (DNA).7 HSV-1 is an alpha-herpes virus. It is the most common virus in the world, affecting more than 60% of adolescents and adults.7 In general, HSV-1 causes infections of the perioral, oropharyngeal, face, and eyes, which spread through infected saliva.7,8 Recurrent intraoral herpes (RIH) is a herpes simplex virus type 1 (HSV-1) infection that recurs or becomes reactivated.8 Triggers of HSV-1 can be exogenous or endogenous, such as stress, trauma, exposure to sunlight or ultraviolet light, fatigue, menstruation, sexual intercourse, fever, use of corticosteroids, laser treatment, nerve damage, and immunosuppression.9,10 Recurrence of HSV-1 in the oral cavity in addition to RIH can also be Herpes Associated Erythema Multiforme (HAEM). The diagnosis of HAEM is usually made clinically on the oral mucosa in the form of crusts serosanguinolenta on the lips, tend to bleed and the presence of target lesions on the skin.11,12
Oral candidiasis is an oral infection that often occurs in patients with diabetes mellitus due to overgrowth of Candida albicans and poor oral hygiene.13 The prevalence of oral candidiasis in patients with diabetes mellitus is approximately 30%, and almost 80% of this is caused by Candida albicans.14 Patients with diabetes mellitus can become infected due to immunosuppression of the immune system caused by dysregulation of the body’s defense system, both immunological and non- immunological.15,16
Immunosuppression usually occurs in people undergoing treatment with certain drugs, transplantation, or cancer therapy, but it can also be related to immune system dysfunction caused by diabetes mellitus and stress.17,18 RIH and oral candidiasis in DM have been discussed in many published case reports. Whereas this case report discusses the role of silent DM and stress in the occurrence of opportunistic oral infections, namely RIH and oral candidiasis, in young adult patients.
Case Report
A 34-year-old man of Asian ethnicity was referred to the Department of Oral Medicine (OM) from the Department of Internal Medicine. The patient complained of very dry mouth, tongue stiffness, burning making it difficult to open the mouth, and white patches on the throat that made it difficult to swallow. A few days earlier, the patient had felt nauseous, vomited, had a sore throat, and looked like he had canker sores in his mouth. To relieve his symptoms, the patient went to the clinic and was given medication. The sore throat was getting worse, so he was referred to Hasan Sadikin Hospital and diagnosed with type 2 diabetes mellitus (DM). Patients are unaware and do not know the signs or symptoms of DM. This patient has a poor lifestyle, always eating fast food, drinking sugary every day, rarely drinking water, and never exercising. In the last few months, he has been experiencing stress at work.There are no allergies to any food or medication. There was no history of alcohol use or smoking. The habit of brushing teeth three times a day was healthy, but the patient’s family never cleaned the mouth and teeth while he was in the hospital. The patient had a history of chickenpox, but he forgot when exactly he got it. The patient also has a habit of wetting his lips with his tongue when he has oral complaints. This patient’s complaint is only in the oral cavity. The diagnosis from the internal medicine department was type 2 diabetes mellitus with mild diabetic ketoacidosis, acute kidney injury, mild dehydration, and hyperemia. The diagnosis of type 2 DM was made in this patient by examining the random blood sugar (784 mg/dL) and HbA1c (13.9%) as shown in Table 1.
Extraoral examination (Figure 1) revealed exfoliation, with desquamation and erosion of the lips, multiple, not tend to bleed, but painful. Intraoral examination (Figure 1) of the labial mucosa, upper and lower gingiva, right and left buccal mucosa, and dorsum of the tongue showed multiple white plaques that could be scraped off, leaving an erythematous, painful, and the mirror stick to the buccal mucosa. The hard palate appears as vesicles filled with clear fluid, multiple, accompanied by erosion with an erythematous base, extending to the soft palate, painful with dry saliva. The dorsum of the tongue appears as depapilation with a mirror stick. There is no saliva pooling on the floor of the mouth. Additional examinations show the results of a complete blood test and others listed in Table 1, the results of the examination of fungal preparations in Table 2, and the examination of Depression Anxiety and Stress Scale-21 score (DASS-21) with results of normal depression (score 0), anxiety mild (score 4), and moderate stress (score 10) and body mass index (BMI) 38.91. The definitive diagnosis in this case based on history, clinical, and additional examination was established as RIH in the hard palate region extending to the soft palate, accompanied by pseudomembranous candidiasis on the right and left buccal mucosa, mandibular anterior gingiva, dorsal tongue, and oropharynx. There was also severe xerostomia Challacombe scale and exfoliative cheilitis of the upper and lower. The differential diagnosis for this case is Herpes Associated Erythema Multiforme (HAEM). Treatment for this patient consists of pharmacological therapy in the form of systemic and topical medication. Systemic medication with Fluconazole 150 mg injection once a day for seven days and Acyclovir 200 mg per oral five times a day (given after the IgG test results a positive value). Topical medications include 0.9% NaCl to compress the lips, clean the teeth and the tongue at least twice a day after breakfast and at night before going to bed, chlorine dioxide mouthwash to compress the oral cavity three times a day, and 100% petroleum jelly applied to the upper and lower lips after compressing. Non-pharmacological therapy includes oral hygiene instructions and education on how to compress the lips and oral cavity with NaCl 0.9% and chlorine dioxide, refer to the internal medicine clinic for DM management. The management of stress in this patient was to refer him to a professional and instruct him to take a few days off from work. The first follow-up or second visit was performed three days later, and the condition of the oral cavity has improved, the right and left lateral areas of the tongue and the ventral tongue could be evaluated as shown in Figure 2. Pseudomembranous candidiasis resolved, RIH and exfoliative cheilitis improved, severe xerostomia improved to moderate xerostomia, and keratotic lesions appeared on the right and left lateral sides of the tongue (around the radix of teeth 36 and 46), and atrophy (glossitis) occurred on the dorsum of the tongue. Acyclovir 200 mg was given five times a day for seven days. Lip compresses with NaCl and oral cavities with chlorine dioxide were discontinued. The patient rinsed with chlorine dioxide mouthwash. Acyclovir 200 mg therapy was given on day two of the initial visit for seven days, five times a day. Fluconazole injection is continued, and multivitamins are added once a day. Brush teeth and tongue with a soft- bristled toothbrush twice a day, in the morning after breakfast and the evening before bed. The result of the random blood sugar test was 475 mg/dL.
The third visit (Days +7), the condition of the patient’s oral cavity experienced significant improvement. RIH has resolved, xerostomia is still moderate, exfoliative cheilitis is still improving, and keratotic lesions at regio teeth 36 and 46 are still present. The extra and intraoral clinical picture is shown in Figure 3. The patient has not been able to remove he remaining radix 36 and 46 and remove calculus because the patient’s blood sugar was still high 275 mg/dL. The injectable fluconazole drug was stopped, the use of acyclovir 200 mg, multivitamins, and chlorine dioxide mouthwash as well as oral hygiene instructions continued, and after hospitalization, the patient was allowed to go home by the internal medicine department.
The fourth visit (Days +14) was made at the oral medicine outpatient clinic. The condition of the patient’s oral cavity had recovered optimally. The xerostomia became mild on the Challacombe scale, and the keratotic lesions on teeth 36 and 46 were still present. The dorsum of the tongue did not appear atrophic, and there was white plaque on 2/3 of the dorsum of the tongue, which could be scraped off without leaving an erythematous area. The patient was referred to the internal medicine department before scaling and extraction of radixes of teeth 36 and 46. The mouthwash was changed to 1% povidone-iodine 10 mL three times a day, acyclovir therapy was stopped, multivitamins and oral hygiene instructions were continued by brushing teeth and tongue at least twice a day after breakfast and at night before bed with a soft-bristled brush, and the patient was educated to be able to exercise. Extra and intraoral clinical features are shown in Figure 4. This case is important because the oral complaints occurred in an adult who was unaware of the symptoms of DM and under high occupational stress and differentiated from the differential diagnosis, which is herpes-associated erythema multiforme. The limitation of this case report is that the reported case is limited to only one patient. However, knowledge about the relationship between systemic diseases, triggering factors, clinical features, and appropriate supporting examinations to establish a rapid and appropriate diagnosis according to the patient’s oral complaints can be additional knowledge for dental practitioner colleagues The patient has approved and written informed consent for the case details to be published included publication of the image, and the institution has also approved for publication. This case had complied with the Declaration of Helsinki. The publication of this case report has also been approved by the institution.
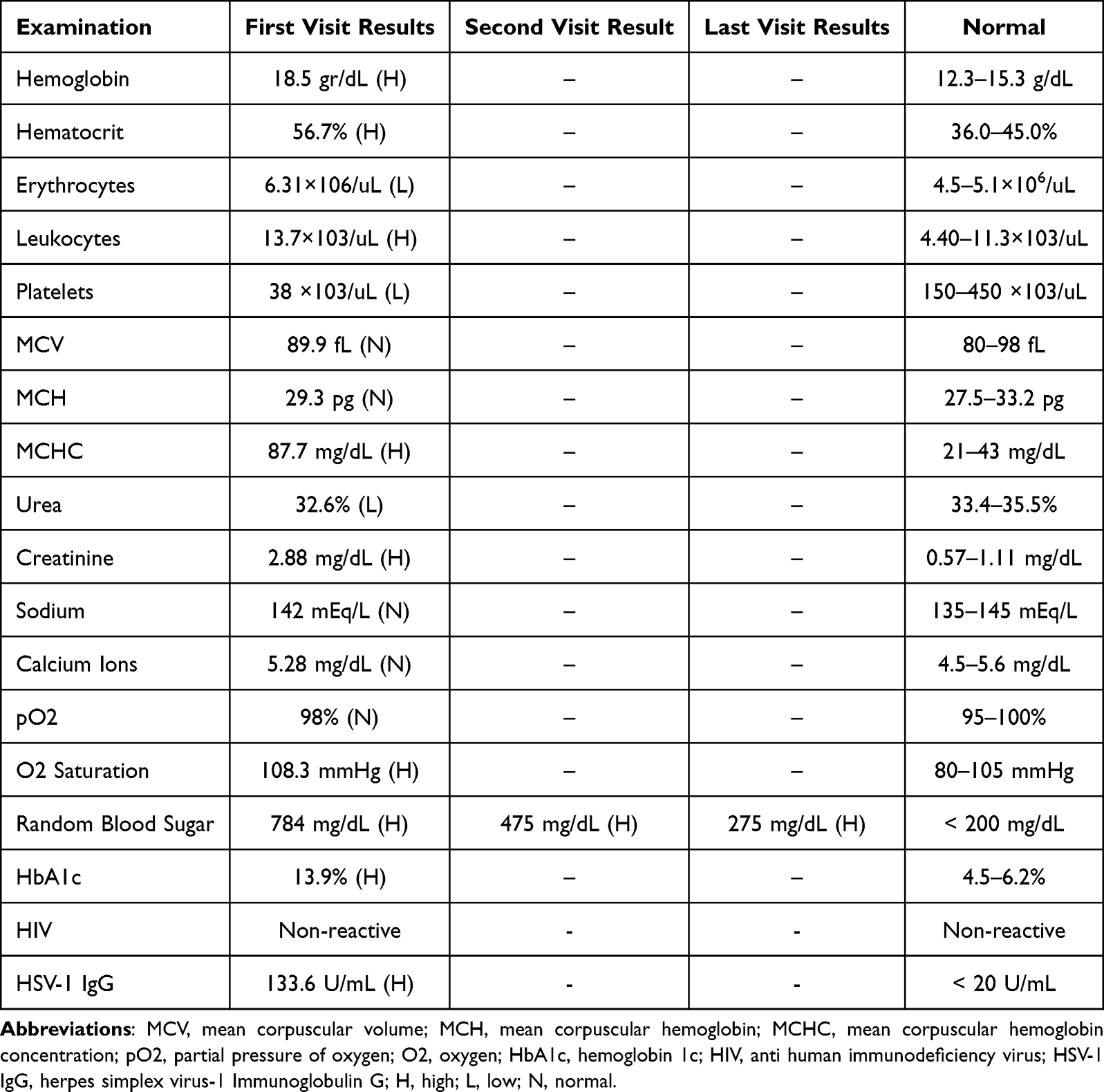 |
Table 1 Laboratory Test Results |
 |
Table 2 Test Results for Fungi |
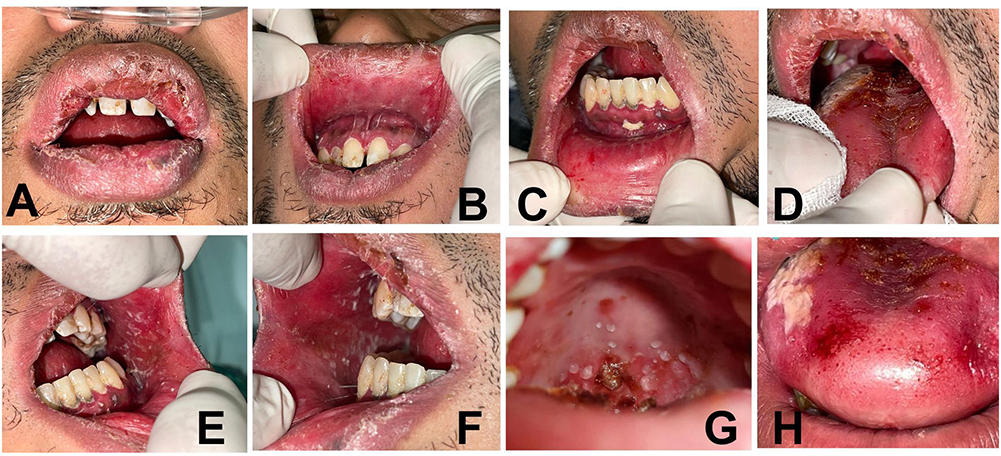 |
Figure 1 (A–H). Clinical features or intraoral examination at the first visit. |
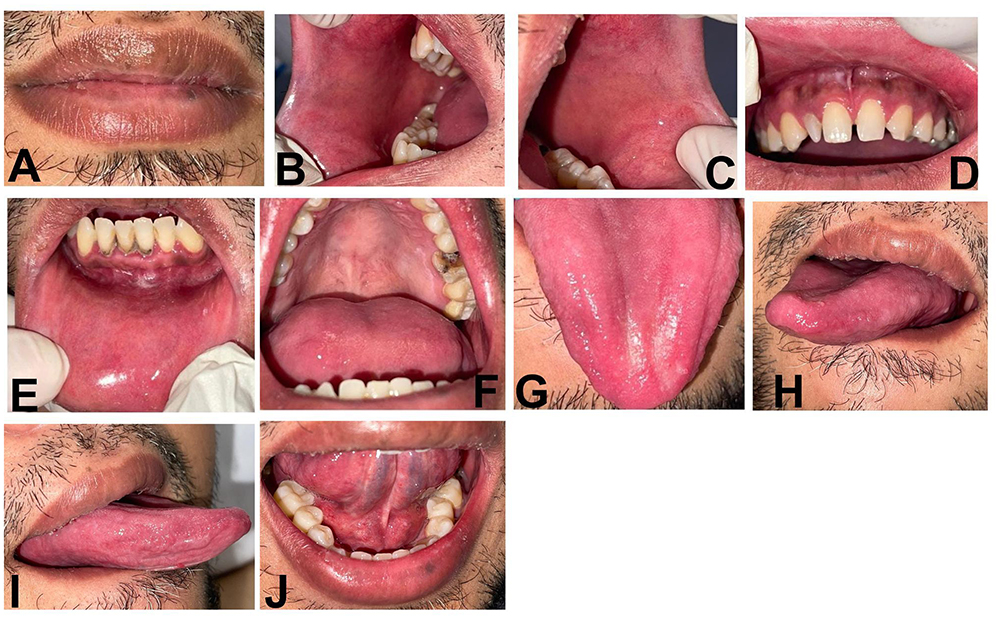 |
Figure 2 (A–J). Clinical picture of the second visit (Days+3). The condition of the oral cavity has improved, the right and left lateral areas of the tongue and the ventral tongue can now be evaluated. |
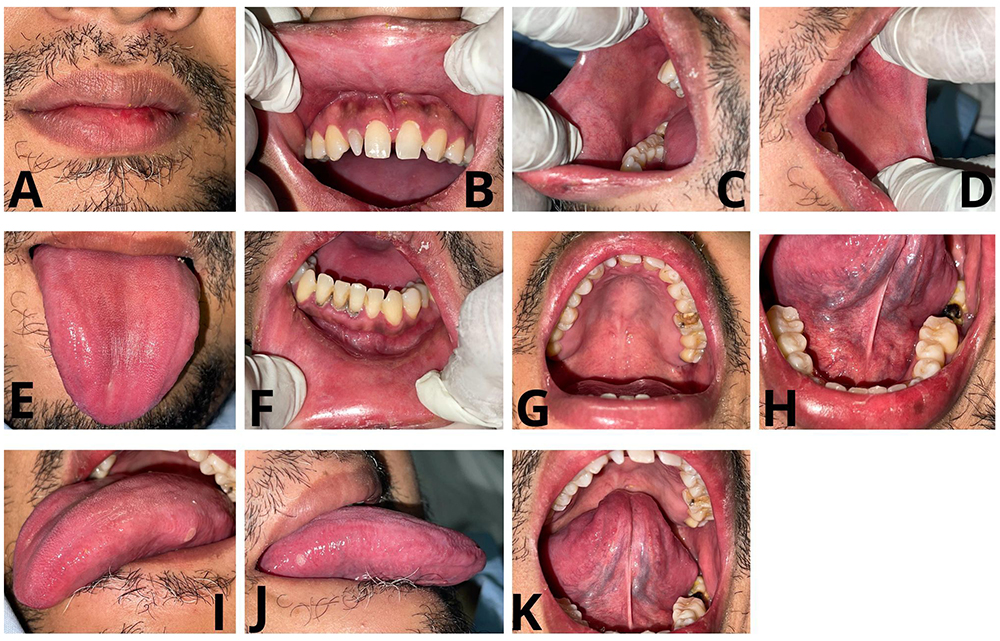 |
Figure 3 (A–K). Clinical picture of the third visit (Days+7). The condition of the patient’s oral cavity experienced significant improvement. |
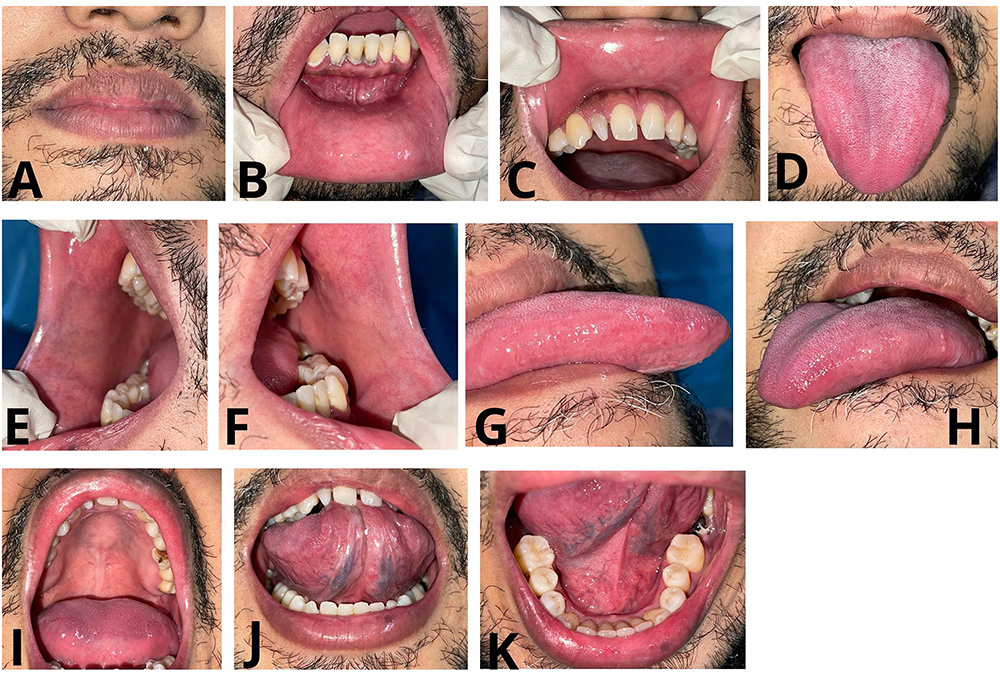 |
Figure 4 (A–K). Clinical picture of the fourth visit (Days+14). The condition of the patient’s oral cavity had recovered optimally. |
Discussion
The highlight of this case report is the suggestion that silent type 2 diabetes mellitus and stress can cause immunosuppression, which is a triggering factor for opportunistic infections, namely RIH and oral candidiasis. Silent diabetes mellitus usually occurs in adolescents or young adults with a body mass index (BMI) ≥ 30 kg/m2 due to a poor diet and can cause immunosuppression, according to Shah and Hux (2003), Muller et al, (2005), Casqueiro et al, (2012), and Calliari et al, (2019).19 Intraoral reactivation of latent HSV-1 in type 2 DM occurs in the pancreas due to the increased incidence of chronic inflammation caused by a hyperglycemic environment that increases the incidence of chronic inflammation.6,20 HSV-1 recurrence may occur because it is latent in the ganglion and spreads to sensory nerves and into tissues, especially keratinized areas. In this case, RIH was found in the hard palate that extended to the soft palate, all of which are keratinized tissues.7 HAEM, which is the differential diagnosis in this case, has a different clinical picture from RIH. The target lesion on the skin is the main difference in this case. In this case, the intra- and extra-oral clinical features showed RIH. There were no serosanguinolenta crust and tend to bleed on the lip In this case. In addition to DM, the trigger for RIH in this patient was stress. Stress-induced activation of corticosteroid levels may also cause cellular immunomodulation that indirectly suppresses the production of pro-inflammatory cytokines, chemokines and adhesion molecules. Modulation of the cellular immune system has the potential to affect viral replication. The natural killer is the body’s immune system for viral infections, which is inhibited by psychological stress.8
An increase in Candida albicans is associated with conditions of immunosuppression or disorders of the immunoregulatory system due to impaired or decreased chemotactic ability and defects in phagocytosis due to a deficiency of polymorphonuclear leukocytes.21 The antiviral therapy aims to reduce viral shedding, accelerate lesion healing, reduce the incidence of new lesions, and reduce the rate of further complications.22 Fluconazole injections are given with the aim of inhibiting the cytochrome P450 enzyme lanosterol demethylase (14α-demethylase), which is encoded by ERG11.23 Chlorine dioxide mouthwash and 0.9% NaCl physiological solution are useful for oxygenating epithelial tissue and have antiseptic, antiviral, and antifungal effects.24,25 DM that is quickly diagnosed and treated, and stress that is relieved can reduce the occurrence of opportunistic oral infections.
Conclusion
The role of silent Type 2 DM and stress causes a decrease in the immune system that uses chronic inflammatory pathways that can trigger the onset opportunistic infections, namely RIH and oral candidiasis instead of HAEM. A healthy diet, lifestyle, regular test blood sugar, and adequate rest can avoid the occurrence of opportunistic infections due to silent DM and stress in young adults.
Acknowledgments
The authors would like to thank Universitas Padjadjaran for the article processing charge (APC) funding provided for the publication of this article. Also, for patients who have given consent for the case they suffered to be appointed as a case report and published for the purposes of scientific knowledge.
Disclosure
The authors state no conflicts of interest in this work.
References
1. Sedghizadeh PP, Mahabady S, Allen CM. Opportunistic oral infections. Physiol Behav. 2017;176(3):139–148. doi:10.1016/j.cden.2016.12.007
2. Indira P, Kumar PM, Shalini S, Vaman K. Opportunistic infections among people living with HIV (PLHIV) with Diabetes Mellitus (DM) attending a tertiary care hospital in coastal city of South India. PLoS One. 2015;10(8):4–11. doi:10.1371/journal.pone.0136280
3. Carpenter DL, Gregg SR, Xu K, Buchman TG, Coopersmith CM. Prevalence and impact of unknown diabetes in the ICU. Crit Care Med. 2015;43(12):e541–e550. doi:10.1097/CCM.0000000000001353
4. Rodrigues CF, Rodrigues ME, Henriques M. Candida sp. Infections in patients with diabetes mellitus. J Clin Med. 2019;8(1):1–41. doi:10.3390/jcm8010076
5. Nurmansyah D, Stasya E, Normaidah DR, Astuti A, Astuti A. Hyperglicemia as predisposition factor of oral candidiasis on patient with diabetes mellitus. Biomedika. 2020;13(1):46–50. doi:10.31001/biomedika.v13i1.703
6. Lontchi-Yimagou E, Feutseu C, Kenmoe S, et al. Non-autoimmune diabetes mellitus and the risk of virus infections: a systematic review and meta-analysis of case-control and cohort studies. Sci Rep. 2021;11(1):1–13. doi:10.1038/s41598-021-88598-6
7. Kumar SP, Chandy ML, Shanavas M, Khan S, Suresh KV. Pathogenesis and life cycle of herpes simplex virus infection-stages of primary, latency and recurrence. J Oral Maxillofac Surg Med Pathol. 2016;28(4):350–353. doi:10.1016/j.ajoms.2016.01.006
8. Hasanah NT. Stress as trigger factor of HSV-1 reactivation causing recurrent intraoral herpes mimicking HAEM: a case report. Int Med Case Rep J. 2022;15(November):699–706. doi:10.2147/IMCRJ.S388708
9. Atyeo N, Rodriguez MD, Papp B, Toth Z. Clinical manifestations and epigenetic regulation of oral herpesvirus infections. Viruses. 2021;13(4):1–17. doi:10.3390/v13040681
10. Fatahzadeh M, Schwartz RA. Human herpes simplex virus infections: epidemiology, pathogenesis, symptomatology, diagnosis, and management. J Am Acad Dermatol. 2007;57(5):737–763. doi:10.1016/j.jaad.2007.06.027
11. Susanto H, Nurhilailah N, Ganesha R, Hendarti HT, Hadi P. Herpes-associated erythema multiforme in a postmenopausal woman. Maj Kedokt Gigi Indones. 2022;7(1):51. doi:10.22146/majkedgiind.43299
12. Dzhelyatova G, Miteva L, Dourmishev L. Herpes simplex associated erythema multiforme: a case report and review of the literature. Acta Medica Bulg. 2021;48(3):46–48. doi:10.2478/amb-2021-0036
13. Dehghan P, Mohammadi F, Javaheri MR, Nekoeian S. Identification of Candida species in the oral cavity of diabetic patients. Curr Med Mycol. 2016;2(2). doi:10.18869/acadpub.cmm.2.2.4
14. Rodríguez-Archilla A, Piedra-Rosales C. Candida species oral detection and infection in patients with diabetes mellitus: a meta-analysis. Iberoam J Med. 2021;3(2):115–121. doi:10.53986/ibjm.2021.0020
15. Jabra Rizk MA. Oral Candidiasis: an Opportunistic Infection of AIDS. J AIDS Clin Res. 2014;05(09):23–27. doi:10.4172/2155-6113.1000i101
16. Casqueiro J, Casqueiro J, Alves C. Review Article Infections in patients with diabetes mellitus: a review of pathogenesis. Indian J Endocrinol Metab. 2012;16:28–36. doi:10.4103/2230-8210.94253
17. Meidani M, Naeini AE, Rostami M, Sherkat R, Tayeri K. Immunocompromised patients: review of the most common infections happened in 446 hospitalized patients. J Res Med Sci. 2014;19(SPEC. ISSUE):2–3.
18. Tripathi P. Immunosuppression and immunomodulation [Internet] (K. Tyagi R, Sharma P, Sharma P, editors); 2023. doi:10.5772/intechopen.107362eurheartj/ehz919.
19. Sajid M, Akash H, Rehman K, Fiayyaz F, Sabir S, Khurshid M. Diabetes ‑ associated infections: development of antimicrobial resistance and possible treatment strategies. Arch Microbiol. 2020;202(5):953–965. doi:10.1007/s00203-020-01818-x
20. Sun Y, Pei W, Wu Y, Yang Y. An Association of Herpes Simplex Virus Type 1 infection with type 2 diabetes. Diabetes Care. 2005;28(2):1–2. doi:10.2337/diacare.28.2.435
21. Boza-Oreamuno YV, Mena-Lizano A. Exfoliative Cheilitis more than an aesthetic problem: case report Queilitis. ODOVTOS Int J Dent Sc. 2022;104–112. doi:10.15517/IJDS.2022.50022
22. Berkow Elizabeth L, Lockhart SR. Fluconazole resistance in Candida species: a current perspective. Infect Drug Resist. 2017;10:237–245. doi:10.2147/IDR.S118892
23. Cernik C, Gallina K, Brodell RT. The treatment of herpes simplex infections: an evidence-based review. Arch Intern Med. 2008;168(11):1137–1144. doi:10.1001/archinte.168.11.1137
24. Perwiradinata R, Radithia D, Endah A, Soebadi B. Management of xerostomia using chlorine dioxide mouthwash in post-surgical and chemotherapy breast cancer patient with aromatase inhibitor treatment (anastrazole). J Case Dent Med. 2020;2(1):16–20. doi:10.20956/jcrdm.v2i1.10725
25. Huynh NCN, Everts V, Leethanakul C, Pavasant P, Ampornaramveth RS. Rinsing with saline promotes human gingival fibroblast wound healing in vitro. PLoS One. 2016;11(7):1–13. doi:10.1371/journal.pone.015984
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Overweight and Inflammatory Indicators with Breast Cancer: A Cross-Sectional Study in Chinese Women
Zha JM, Zhang M, Wang T, Li HS, Ban QY, Liu M, Jiang XX, Guo SY, Wang J, Zhou YR, Liu YH, He WQ, Xu H
International Journal of Women's Health 2024, 16:783-795
Published Date: 6 May 2024
Therapeutic Potential of Mesenchymal Stem Cell-Derived Extracellular Vesicles in Digestive System Tumors: Modulating the Chronic Inflammatory Microenvironment
Kang H, Ding T, Lin H, Wang F, Zhu Y, Chen P, Chen H, Huang J, Wang X
International Journal of Nanomedicine 2026, 21:600593
Published Date: 18 May 2026