Back to Journals » Journal of Pain Research » Volume 11
Oral methylnaltrexone does not negatively impact analgesia in patients with opioid-induced constipation and chronic noncancer pain
Authors Webster LR ![]() , Israel RJ
, Israel RJ ![]()
Received 21 December 2017
Accepted for publication 14 June 2018
Published 13 August 2018 Volume 2018:11 Pages 1503—1510
DOI https://doi.org/10.2147/JPR.S160488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Lynn R Webster,1 Robert J Israel2
1PRA Health Sciences, Salt Lake City, UT, USA; 2Clinical and Medical Affairs, Salix Pharmaceuticals, Bridgewater, NJ, USA
Purpose: An oral formulation of methylnaltrexone has been developed for treating opioid-induced constipation (OIC). This manuscript examines the impact of oral methylnaltrexone, a peripherally acting µ-opioid receptor antagonist, on opioid analgesia.
Methods: This Phase III, randomized, double-blind, placebo-controlled trial, evaluated changes in pain intensity scores (0= no pain to 10= worst possible pain) and opioid use in adults with chronic noncancer pain. Patients taking ≥50 mg/day oral morphine equivalent dose (MED) for ≥14 days before screening with less than three rescue-free bowel movements/week received oral methylnaltrexone 150 mg/day (n=201), 300 mg/day (n=201), 450 mg/day (n=200), or placebo (n=201) once daily for 4 weeks followed by 8 weeks of oral methylnaltrexone as needed.
Results: The primary condition requiring opioid use was back pain (68.2% of 803 patients). Baseline pain intensity scores were similar among treatment groups (mean range, 6.2–6.4) and remained stable throughout the 4-week double-blind (mean range, 6.1–6.5) and 8-week as needed (mean range, 6.3–6.5) periods. Baseline mean MED was comparable between oral methylnaltrexone 150 mg (200.0 mg/day), methylnaltrexone 450 mg (218.0 mg/day), and placebo (209.7 mg/day), but was slightly higher in the oral methylnaltrexone 300-mg group (252.6 mg/day). Nonsignificant, minimal changes in mean MED were observed after 4 weeks of treatment (214.5–235.6 mg/day) and at the end of the as needed phase (202.3–234.9 mg/day). The percentage of patients who initiated new opioid medications during the 4-week, once-daily dosing period was generally similar among the oral methylnaltrexone 150-mg, 300-mg, and 450-mg groups (44.8%, 43.3%, and 35.0%, respectively), the oral methylnaltrexone combined group (41.0%), and the placebo group (39.8%). The most common newly initiated opioid medications during this once-daily period were oxycodone (oral methylnaltrexone groups combined, 14.6%; placebo, 12.4%) and morphine (oral methylnaltrexone combined, 10.1%; placebo, 7.0%).
Conclusion: Oral methylnaltrexone does not elicit opioid withdrawal or interfere with opioid analgesia.
Keywords: methylnaltrexone, constipation, opioid analgesics, chronic pain, opiate dependence, opioid-related disorders
Introduction
Opioid analgesics are among the most commonly prescribed medications for the management of chronic noncancer pain.1 Opioids provide analgesia predominantly by targeting µ-, δ-, and κ-opioid receptors within the central nervous system.2 However, opioids also stimulate peripheral µ-opioid receptors in the gastrointestinal tract, which can result in delayed gastric emptying, oral-cecal transit, and colonic transit.3,4 These adverse effects on bowel function can inhibit defecation, resulting in opioid-induced constipation (OIC). This affects between 40% and ≥95% of patients on long-term opioid therapy,5–8 is characterized by hard stools that are difficult to pass, resulting in straining, incomplete evacuation, and prolonged time to passage, often requiring manual maneuvers to facilitate defecation.9
Constipation is the most bothersome gastrointestinal side effect reported by patients on long-term opioid therapy.5,6 Unlike other opioid-related adverse events (AEs), patients do not develop tolerance to OIC over time, and symptoms are often refractory to lifestyle modifications (eg, increased fluid intake and exercise, and dietary changes).10,11 Over-the-counter laxatives and stool softeners have limited efficacy because they do not target the underlying pathophysiology of OIC (ie, delayed gastrointestinal transit, increased water absorption, and nonpropulsive motor activity due to µ-opioid receptor activation).2,12
Methylnaltrexone (Relistor®, Salix Pharmaceuticals, a division of Valeant Pharmaceuticals North America LLC, Bridgewater, NJ, USA) is a selective, peripherally acting µ-opioid receptor antagonist that inhibits opioid-induced increases in oral-cecal transit time and time to gastric emptying.13–15 A formulation of methylnaltrexone for subcutaneous injection is approved for the treatment of OIC in adults with advanced illness or pain caused by active cancer who require opioid dosage escalation for palliative care and for the treatment of OIC in adults with chronic noncancer pain, including those with chronic pain related to prior cancer or its treatment who do not require frequent opioid dosage escalation.16,17 An oral formulation of methylnaltrexone was developed to provide an alternative dosing option for patients requiring long-term management of OIC18; this formulation received US Food and Drug Administration approval in 2016 for the treatment of OIC in adults with chronic noncancer pain.16–18 The efficacy of oral methylnaltrexone for OIC was demonstrated in a pivotal Phase III trial in 803 patients with chronic noncancer pain where the percentage of patients that had an increase in mean percentage of days resulting in rescue-free bowel movements (RFBMs) within 4 hours of dosing during a 4-week once-daily (QD) dosing period was significantly greater with methylnaltrexone 300 mg (24.6%) and methylnaltrexone 450 mg (27.4%) compared with placebo (18.2%; both P≤0.01).18
It is important that drugs used to treat OIC do not disrupt the central analgesia provided by opioid analgesics.11 Therefore, analyses of secondary endpoints from the pivotal Phase III trial of oral methylnaltrexone18 were performed to examine the potential effects of oral methylnaltrexone on centrally mediated opioid analgesia in adults with chronic noncancer pain and OIC.
Methods
The present analysis of a Phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group study (ClinicalTrials.gov identifier: NCT01186770) was conducted to evaluate whether oral methylnaltrexone had any negative effects on analgesia in patients with OIC and chronic noncancer pain. The study was conducted in accordance with the ethical principles in the Declaration of Helsinki; the International Conference on Harmonization Good Clinical Practice guidelines; Code of Federal Regulations 50, 56, and 312; and all other applicable laws and regulations. The study protocol and all amendments were reviewed and approved by appropriate institutional review boards prior to study initiation (Meritus Medical Center Institutional Review Board, Hagerstown, MD; Partners Human Research Committee, Boston, MA; Quorum Review IRB, Seattle, WA; Schulman Associates IRB, Inc., Cincinnati, OH; SDHIPM IRB, San Diego, CA; University of Utah IRB, Salt Lake City, UT). All patients who participated in this trial provided written informed consent prior to enrollment in the study.
Patient population
Men and women ≥18 years of age with documented chronic noncancer pain for ≥2 months before the screening visit were eligible for study enrollment if they were in generally good health for ≥30 days before the screening visit; had a calculated creatinine clearance of ≥30 mL/min; were taking oral, transdermal, intravenous, or subcutaneous opioid analgesics for chronic noncancer pain for ≥1 month; were receiving ≥50 mg/day of an oral morphine equivalent dose (MED) of an opioid analgesic for ≥14 days; and had a history of OIC for ≥30 days before the screening visit. OIC was defined as less than three RFBMs (ie, bowel movements without laxative use within the previous 24 hours) per week on average over the last four consecutive weeks and one or more of the following: a Bristol Stool Form Scale type one or two for ≥25% of RFBMs, straining during ≥25% of RFBMs, and/or a sensation of incomplete evacuation after ≥25% of RFBMs.
Patients were excluded from the study if they had any of the following: history of chronic constipation prior to initiation of opioid therapy, mechanical bowel obstruction, or megacolon; fecal incontinence, rectal prolapse, fecal ostomy, or other clinically significant gastrointestinal disorders such as inflammatory bowel disease or clinically significant irritable bowel syndrome; rectal bleeding not associated with hemorrhoids or fissure within 60 days of providing informed consent; need for manual disimpaction or pelvic floor support techniques, including manual maneuvers, within 14 days before the screening visit; rectal outlet obstruction or fecal impaction at the screening visit; history of substance abuse within 1 year before the screening visit; any unstable hepatic, renal, pulmonary, cardiovascular, ophthalmologic, neurologic, psychiatric, or other medical condition that might have compromised the study or put the patient at greater risk during study participation; history or presence of orthostatic hypotension; or planned surgery during the study.
Men and women who were not surgically sterile or postmenopausal were required to use a medically acceptable method of birth control or to maintain sexual abstinence for the duration of the study.
Laxatives were to be discontinued at the screening visit; however, rescue laxative therapy was permitted during the study for patients who did not have a bowel movement for three consecutive days. Rescue therapy consisted of up to three oral bisacodyl tablets per day. If bisacodyl tablets failed and patients did not have a bowel movement within 24 hours, an enema or an additional dose of bisacodyl was permitted.
Study design
This Phase III, randomized, double-blind, placebo-controlled study consisted of a 14-day screening period, a 4-week period of QD treatment, an 8-week period of as-needed (PRN) treatment, and a 14-day follow-up period. Double-blind status was maintained throughout the entire 12-week treatment phase of the study.
During the screening period, patients were evaluated for objective evidence of OIC and satisfaction of other enrollment criteria. Patients that remained eligible at the baseline visit (day 1) were randomized in a 1:1:1:1 ratio using a computer-generated schedule to receive methylnaltrexone 150, 300, or 450 mg QD, or placebo. To maintain blinding, all patients took three tablets per day of study drug; ie, patients in the placebo group took three placebo tablets, and patients in each of the methylnaltrexone groups took two placebo tablets plus one methylnaltrexone 150-, 300-, or 450-mg tablet, respectively. Following the 4-week period of QD dosing, patients began the 8-week PRN period, during which they continued to receive the same treatment to which they were assigned at randomization (QD period).
Study assessments
Throughout the screening and double-blind treatment periods, patients recorded their daily oral MEDs in an electronic diary.
Pain intensity was assessed at baseline (day one predose), at day 14 and day 28 (QD period), and at days 42, 56, and 84 (PRN period) using an 11-point numerical rating scale. Patients rated their average pain over the past 24 hours from 0 (no pain) to 10 (worst possible pain).19
Opioid withdrawal was assessed by a trained clinician at baseline (day 1 predose), 1 hour postdose on day 1, at day 14 and day 28 (QD period), and at days 42, 56, and 84 (PRN period) using the objective opioid withdrawal scale (OOWS).20 The OOWS is a 13-item questionnaire designed to assess opioid withdrawal as a result of opioid abstinence in patients who are physically dependent on opioids.20 The OOWS contains an item that assesses abdominal cramping; however, abdominal cramping has been identified as an AE associated with constipation and/or induction of laxation in patients with OIC upon treatment with methylnaltrexone. As such, the abdominal cramping item was considered to be a potential confounding factor, and withdrawal analyses were performed with and without the OOWS item related to abdominal cramping. Higher OOWS scores (range, 0–13) indicate greater numbers or intensity of withdrawal symptoms.20
Other safety assessments performed in this study included assessment of the incidence of treatment-emergent AEs (TEAEs) and changes from baseline in clinical laboratory parameters and vital sign measurements. TEAEs were defined as any newly occurring or worsening AEs that were observed after the first dose of study drug.
Statistical analyses
A planned sample size of 750 patients was used to ensure that at least 700 evaluable patients (175 per treatment group) participated in the study. All analyses were performed on the safety population, which included all randomized patients who received at least one dose of study medication.
Comparisons of changes from baseline to each assessment time point in pain intensity and OOWS scores were performed for each methylnaltrexone dose vs placebo using the Wilcoxon-Mann-Whitney test.
Results
Patients
A total of 804 patients were randomized to double-blind treatment, and 803 patients received at least one dose of study medication. In all treatment groups, approximately 90% (723/803) of patients completed the 4-week QD dosing period. Reasons for early discontinuation of 10% of patients during the 4-week QD dosing period included ineligibility (n=2, <1%); protocol violation (n=12, 1%); adverse event (n=14, 2%); withdrawal requested by patient (n=28, 3%); lost to follow-up (n=11, 1%); insufficient response to treatment (n=12, 1%); and other (n=2, <1%). A total of 694 patients participated in the 8-week PRN dosing period (177, 181, and 169 in the methylnaltrexone 150-, 300-, and 450 mg/day groups, respectively, and 167 in the placebo group). The rate of early discontinuation from the PRN dosing period was 12% (63/527) among all methylnaltrexone-treated patients and 14% (24/167) in the placebo group. Reasons for early discontinuation of 13% of patients during the 8-week PRN dosing period included protocol violation (n=23, 3%); adverse event (n=11, 2%); withdrawal requested by patient (n=20, 3%); lost to follow-up (n=26, 4%); insufficient response to treatment (n=6, 1%); and other (n=1, <1%).
Demographic and baseline characteristics, including baseline pain intensity scores, were generally similar among treatment groups (Table 1). The primary pain condition requiring opioid use was back pain, reported by 68.2% (548/803) of patients. The baseline MED was slightly higher in the oral methylnaltrexone 300 mg/day group compared with other groups; this group included two patients who reported higher daily morphine doses than other patients.
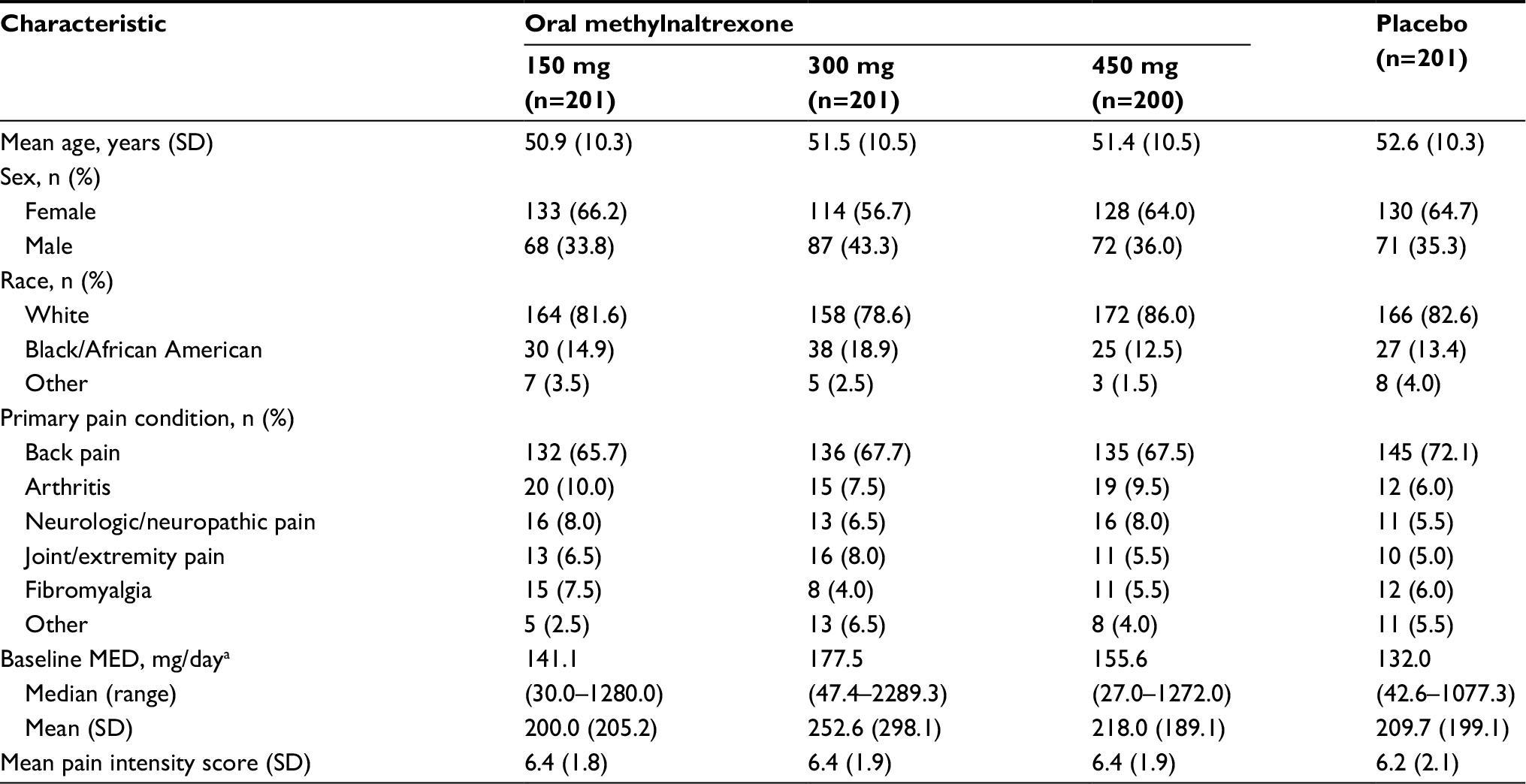 | Table 1 Patient demographic and baseline characteristics Notes: aBaseline opioid dose defined as average of daily oral MED during screening (within 30 days of first dose of study drug): calculated as (sum of total oral morphine equivalents during screening)/(number of days during screening). Abbreviation: MED, morphine equivalent dose. |
Effects of methylnaltrexone on opioid analgesia
Mean pain intensity scores remained stable throughout the 4-week QD and 8-week PRN periods. There were no significant differences between the three oral methylnaltrexone treatment groups (150, 300, and 450 mg/day) and placebo in patient reported mean pain intensity scores (Table 2).
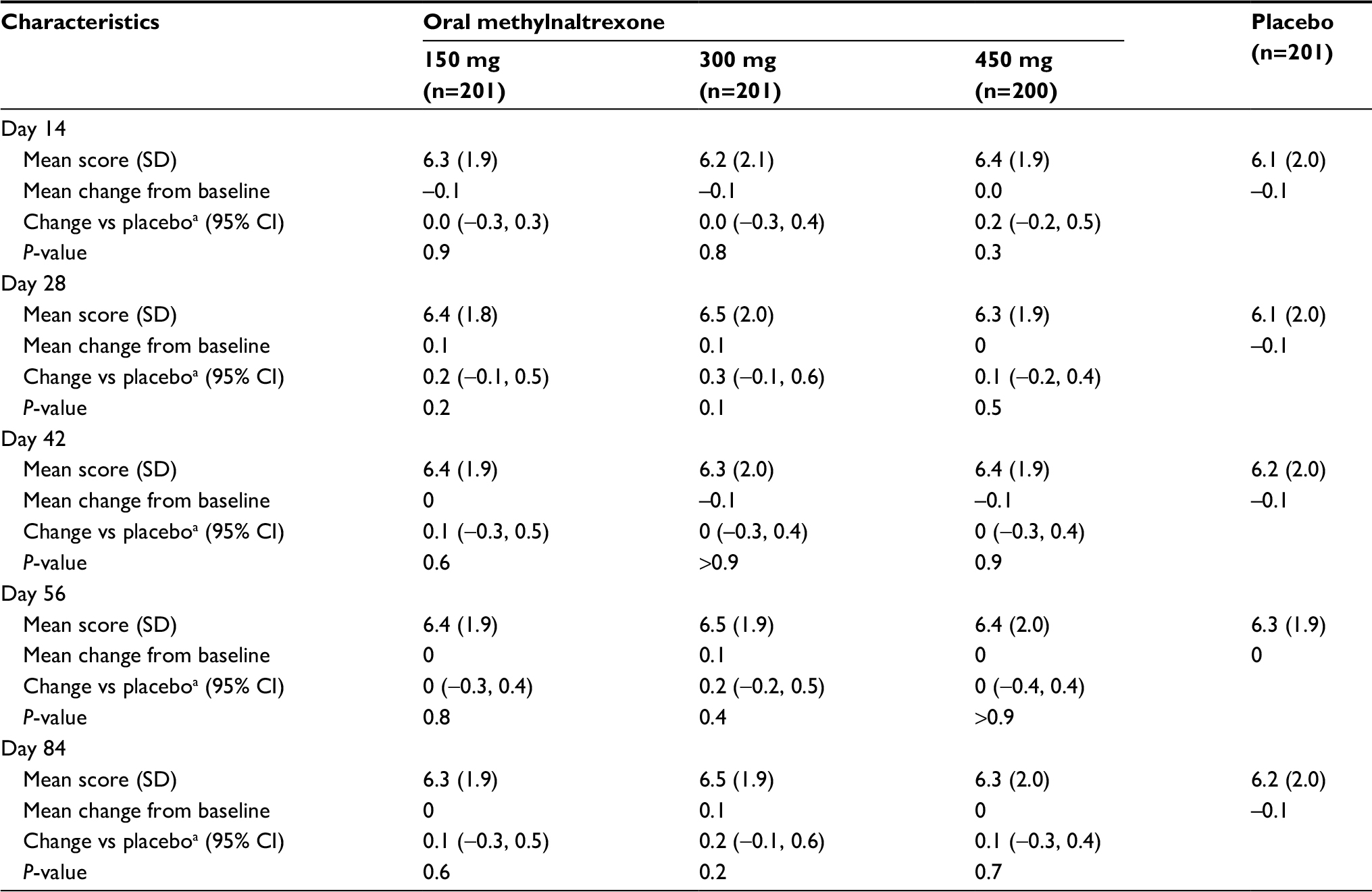 | Table 2 Changes in pain intensity during treatment with oral methylnaltrexone Notes: aValue reflects least-squares mean difference vs placebo. |
During the 4 weeks of QD dosing and 8 weeks of PRN dosing, minimal changes were observed in median MED in patients with OIC (Figure 1). Mean MED data were also consistent with minimal changes observed after 4 weeks of QD dosing (range, 214.5–235.6 mg/day) and after 8 weeks of PRN dosing (range, 202.3–234.9 mg/day).
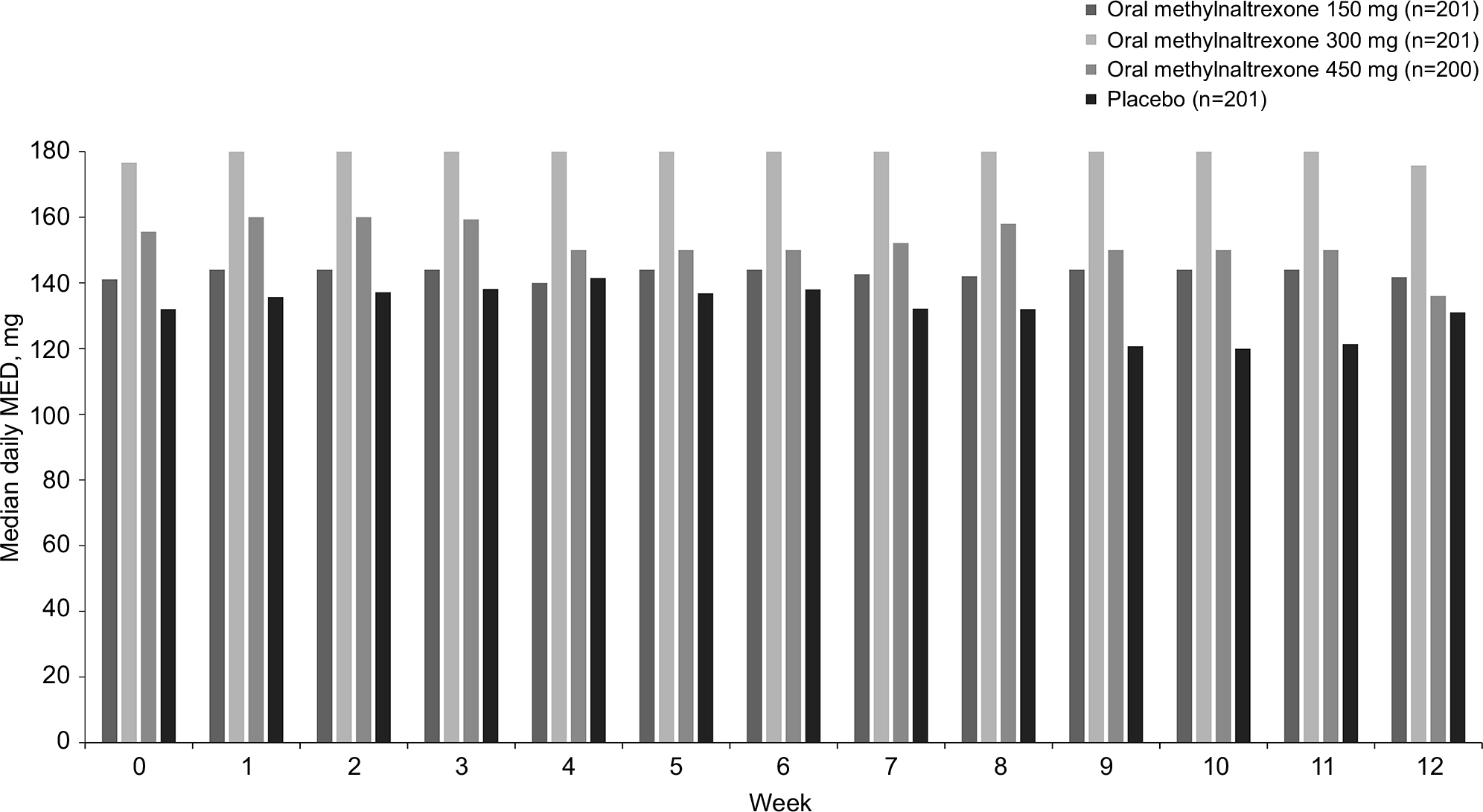 | Figure 1 Median daily morphine equivalent dose over time. Abbreviation: MED, morphine equivalent dose. |
The percentage of patients who initiated new opioid medications during the QD period was generally similar in the oral methylnaltrexone 150-, 300-, and 450 mg/day groups (44.8%, 43.3%, and 35.0%, respectively), the oral methylnaltrexone combined group (41.0%), and the placebo group (39.8%). The most common newly initiated opioid medications during the QD dosing period were oxycodone (oral methylnaltrexone groups combined, 14.6%; placebo, 12.4%) and morphine (oral methylnaltrexone combined, 10.1%; placebo, 7.0%).
Over the 12-week treatment period, there were minimal mean changes from baseline in OOWS scores both with (data not shown) and without (Figure 2) inclusion of abdominal cramping assessments. Changes from baseline in OOWS scores were comparable across the placebo and methylnaltrexone treatment groups.
 | Figure 2 Mean Objective Opioid Withdrawal Scale scorea over time. Notes: aScoring excluded items related to abdominal cramping. #P<0.05 vs placebo for change from baseline. Abbreviation: OOWS, objective opioid withdrawal scale. |
Safety
During the 12-week treatment period, the incidence of TEAEs was 59% in the combined methylnaltrexone group and 63% in the placebo group. The most commonly reported TEAEs (incidence ≥5% in any group) were abdominal pain (methylnaltrexone, 8.0%; placebo, 8.5%), nausea (methylnaltrexone, 6.8%; placebo, 9.0%), and diarrhea (methylnaltrexone, 6.0%; placebo, 3.5%). In the methylnaltrexone and placebo groups, respectively, the incidence of other common (≥2%) TEAEs that can be associated with opioid withdrawal20 was as follows: vomiting, 2.7% vs 4.5%; anxiety, 3.7% vs 1.5%; hyperhidrosis, 3.3% vs 2.0%; tremor, 2.3% vs 0.5%; rhinorrhea, 2.2% vs 1.5%; and hot flush, 1.0% vs 2.0%.
Most TEAEs were mild or moderate in intensity. There were no clinically meaningful changes in clinical laboratory parameters or vital signs with any methylnaltrexone dose compared with placebo.
Discussion
Opioid-induced constipation is a burdensome side effect of opioid analgesics used for the management of chronic noncancer pain. The discomfort and distress associated with OIC causes many patients to stop taking opioid analgesics or to reduce opioid doses.2,5,6,12,21 To reduce this cycle of gastrointestinal distress and uncontrolled pain, treatments for OIC are needed that allow patients to have consistent and reliable bowel movements without compromising analgesia or inducing symptoms of opioid withdrawal.
Findings from the current study demonstrated that both once-daily and as-needed treatment with oral methylnaltrexone provided clinically significant, dose-related improvements in OIC18 without compromising analgesia. The present analyses showed that median daily MED and pain intensity scores were stable throughout the 12-week treatment period, without observation of any clinically meaningful signs or symptoms of opioid withdrawal.
Results from the current study evaluating oral methylnaltrexone are consistent with previous studies of intravenous and subcutaneous methylnaltrexone that showed a lack of effects on analgesia and central withdrawal in patients receiving opioid analgesics.15,22–25 In a study with a design similar to the current study, subcutaneous methylnaltrexone 12 mg was shown to have minimal effects on median MED, pain intensity scores, and opioid withdrawal when administered either once daily or as needed for symptoms of OIC.23
Methylnaltrexone acts on peripheral opioid receptors in the gastrointestinal tract. Importantly, the chemical properties of methylnaltrexone limit its ability to act on central opioid receptors that regulate pain sensations. Methylnaltrexone’s parent compound, naltrexone, exhibits systemic antagonism; however, N-methylation of naltrexone produces a polar, positively charged species with low lipid solubility that has restricted ability to cross the blood–brain barrier.24 The observations from the current study that methylnaltrexone has minimal effects on required opioid analgesic dose and pain intensity scores support that methylnaltrexone has peripheral, rather than central, effects.
Opioid withdrawal can present as a complex range of central and peripheral symptoms, including anxiety, irritability, restlessness, hot and cold flashes, tremors, hyperhidrosis, bone or muscle aches, and gastrointestinal upset (eg, nausea, vomiting, and abdominal cramping).20 Throughout this study, the presence of opioid withdrawal symptoms was very low, based on OOWS results showing that out of 13 possible points, mean scores were ≤0.4 at all assessment time points and were similar in the methylnaltrexone and placebo groups. Additionally, rates of TEAEs associated with opioid withdrawal (eg, nausea/vomiting, anxiety, tremor, rhinorrhea, and hyperhidrosis) were low and similar across groups. TEAEs of abdominal pain/discomfort were common in this study, and abdominal cramping is a characteristic feature of opioid withdrawal. However, in the current study, abdominal cramping may have been a result of either OIC or the propulsive effects of methylnaltrexone to alleviate constipation. Therefore, abdominal cramping was considered to be a potential confounder when interpreting whether abdominal AEs were related to opioid withdrawal. Findings from the OOWS were similar regardless of whether the item related to abdominal cramping was included in the analysis.
Primary efficacy results from this pivotal Phase III trial demonstrated that a significantly (P≤0.002) greater percentage of patients treated with 300 mg/day and 450 mg/day of methylnaltrexone had an increase in mean percentage of dosing days resulting in an RFBM within 4 hours of dosing during weeks 1 through 4 of the trial compared with patients treated with placebo.18 In addition, the percentage of responders and the change from baseline in mean number of weekly RFBMs was significantly (P≤0.03) greater in the 300 mg/day and 450 mg/day treatment groups compared with the placebo treatment group.18 The percentage of responders was significantly greater in the methylnaltrexone 450 mg group compared with the placebo group throughout the 12-week study, demonstrating the durability of response, even throughout the PRN 8-week dosing period.18
Conclusion
In conclusion, results of this study show no demonstrable effects of up to 450 mg once-daily oral methylnaltrexone on centrally mediated opioid analgesia in patients with chronic noncancer pain and OIC. These data further support that methylnaltrexone can be considered as an option for the treatment of OIC, without clinically significant concerns about compromising pain management strategies in patients with chronic noncancer pain.
Acknowledgments
The study was funded by Salix Pharmaceuticals, Bridgewater, NJ, USA. Progenics Pharmaceuticals, Inc., New York, NY, USA, had a role in the study design, implementation of the study, and data collection. Salix had a role in the data collection, data analysis, and the decision to publish. Technical editorial assistance was provided, under the direction of the authors, by Lisa Feder, PhD, of Echelon Brand Communications, Parsippany, NJ, USA. Funding for this assistance was provided by Salix Pharmaceuticals.
The data were previously presented in poster format at the American Pain Society 35th Annual Scientific Meeting, May 11–14, 2016, in Austin, TX, USA, with the abstract published in the Journal of Pain, Volume 17, Issue 4, Supplement page S94. The poster was also presented as an encore at the 2016 PAINWeek National Conference, September 6–10, 2016, in Las Vegas, NV; the 15th Annual ASRA Pain Medicine Meeting, November 17–19, 2016, in San Diego, CA; PGA70: Postgraduate Assembly in Anesthesiology, December 9–13, 2016, in New York, NY; and the International Conference on Opioids, June 11–13, 2017, in Boston, MA, USA.
Disclosure
Dr Israel is an employee of Salix (Valeant) Pharmaceuticals. Dr Webster has served as a board member for Charleston Labs, Daiichi Sankyo, Depomed, Egalet, Inspirion, Insys, Kaléo, Orexo, Pfizer, Proove Biosciences, Scilex, Signature Therapeutics, TEVA, Trevena; has consulted for Acura Pharmaceuticals, Alcobra, AstraZeneca, AcelRX, Egalet, Elysium, Indivior, Insys, Kaléo, KemPharm, Mallinckrodt, Marathon, Merck, Neura, Pain Therapeutics, Pfizer, Proove Biosciences, Shionogi, Vector Pharma, Zogenix; and is employed by PRA Health Sciences. The authors report no other conflicts of interest in this work.
References
Nelson AD, Camilleri M. Chronic opioid induced constipation in patients with nonmalignant pain: challenges and opportunities. Therap Adv Gastroenterol. 2015;8(4):206–220. | ||
Pappagallo M. Incidence, prevalence, and management of opioid bowel dysfunction. Am J Surg. 2001;182(5A Suppl):11S–18S. | ||
Kaufman PN, Krevsky B, Malmud LS, et al. Role of opiate receptors in the regulation of colonic transit. Gastroenterology. 1988;94(6):1351–1356. | ||
De Luca A, Coupar IM. Insights into opioid action in the intestinal tract. Pharmacol Ther. 1996;69(2):103–115. | ||
Bell TJ, Panchal SJ, Miaskowski C, Bolge SC, Milanova T, Williamson R. The prevalence, severity, and impact of opioid-induced bowel dysfunction: results of a US and European Patient Survey (PROBE 1). Pain Med. 2009;10(1):35–42. | ||
Cook SF, Lanza L, Zhou X, et al. Gastrointestinal side effects in chronic opioid users: results from a population-based survey. Aliment Pharmacol Ther. 2008;27(12):1224–1232. | ||
Kalso E, Edwards JE, Moore RA, McQuay HJ. Opioids in chronic non-cancer pain: systematic review of efficacy and safety. Pain. 2004;112(3):372–380. | ||
Benyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician. 2008;11(2 Suppl):S105–S120. | ||
Dorn S, Lembo A, Cremonini F. Opioid-induced bowel dysfunction: epidemiology, pathophysiology, diagnosis, and initial therapeutic approach. Am J Gastroenterol Suppl. 2014;2(1):31–37. | ||
McNicol E, Horowicz-Mehler N, Fisk RA, et al. Management of opioid side effects in cancer-related and chronic noncancer pain: a systematic review. J Pain. 2003;4(5):231–256. | ||
Pergolizzi Jr JV, Raffa RB, Pappagallo M, et al. Peripherally acting μ-opioid receptor antagonists as treatment options for constipation in noncancer pain patients on chronic opioid therapy. Patient Prefer Adherence. 2017;11:107–119. | ||
Coyne KS, LoCasale RJ, Datto CJ, Sexton CC, Yeomans K, Tack J. Opioid-induced constipation in patients with chronic noncancer pain in the USA, Canada, Germany, and the UK: descriptive analysis of baseline patient-reported outcomes and retrospective chart review. Clinicoecon Outcomes Res. 2014;6:269–281. | ||
Murphy DB, Sutton JA, Prescott LF, Murphy MB. Opioid-induced delay in gastric emptying: a peripheral mechanism in humans. Anesthesiology. 1997;87(4):765–770. | ||
Siemens W, Becker G. Methylnaltrexone for opioid-induced constipation: review and meta-analyses for objective plus subjective efficacy and safety outcomes. Ther Clin Risk Manag. 2016;12:401–412. | ||
Slatkin N, Thomas J, Lipman AG, et al. Methylnaltrexone for treatment of opioid-induced constipation in advanced illness patients. J Support Oncol. 2009;7(1):39–46. | ||
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. Relistor. 2016. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/. Accessed July 21, 2016. | ||
Relistor [package insert]. Bridgewater, NJ: Salix Pharmaceuticals; 2017. | ||
Rauck R, Slatkin NE, Stambler N, Harper JR, Israel RJ. Randomized, double-blind trial of oral methylnaltrexone for the treatment of opioid-induced constipation in patients with chronic noncancer pain. Pain Prac. 2017;17(6):820–828. | ||
Farrar JT, Young Jr JP, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. | ||
Handelsman L, Cochrane KJ, Aronson MJ, Ness R, Rubinstein KJ, Kanof PD. Two new rating scales for opiate withdrawal. Am J Drug Alcohol Abuse. 1987;13(3):293–308. | ||
Noble M, Tregear SJ, Treadwell JR, Schoelles K. Long-term opioid therapy for chronic noncancer pain: a systematic review and meta-analysis of efficacy and safety. J Pain Symptom Manage. 2008;35(2):214–228. | ||
Yuan CS, Foss JF, O’Connor M, Toledano A, Roizen MF, Moss J. Methylnaltrexone prevents morphine-induced delay in oral-cecal transit time without affecting analgesia: a double-blind randomized placebo-controlled trial. Clin Pharmacol Ther. 1996;59(4):469–475. | ||
Webster LR, Brenner DM, Barrett AC, Paterson C, Bortey E, Forbes WP. Analysis of opioid-mediated analgesia in Phase III studies of methylnaltrexone for opioid-induced constipation in patients with chronic noncancer pain. J Pain Res. 2015;8:771–780. | ||
Thomas J, Karver S, Cooney GA, et al. Methylnaltrexone for opioid-induced constipation in advanced illness. N Engl J Med. 2008; 358(22):2332–2343. | ||
Chamberlain BH, Cross K, Winston JL, et al. Methylnaltrexone treatment of opioid-induced constipation in patients with advanced illness. J Pain Symptom Manage. 2009;38(5):683–690. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.