Back to Journals » Journal of Pain Research » Volume 19
Oral Ketamine for Chronic Pain: Towards an Evidence-Based Dosing Regimen
Authors Winegarden J ![]() , Brose A
, Brose A ![]() , Storm A, Mortensen A, Carr DB
, Storm A, Mortensen A, Carr DB
Received 6 June 2025
Accepted for publication 9 January 2026
Published 7 February 2026 Volume 2026:19 545221
DOI https://doi.org/10.2147/JPR.S545221
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amitabh Gulati
Jennifer Winegarden,1 Anna Brose,2 Audra Storm,3 Alexander Mortensen,4 Daniel B Carr5
1Palliative Medicine, Mayo Clinic Health System, La Crosse, WI, USA; 2School of Psychology, Counseling and Family Therapy, Wheaton College, Wheaton, IL, USA; 3Family Medicine, Big Hollow Primary Care, OSF Healthcare, Peoria, IL, USA; 4Family Medicine Residency, Mayo Clinic Health System, La Crosse, WI, USA; 5Department of Public Health and Community Medicine, Tufts University School of Medicine, Boston, MA, USA
Correspondence: Jennifer Winegarden, Palliative Medicine, Mayo Clinic Health System, 700 West Ave. S., La Crosse, WI, 54601, USA, Email [email protected]
Purpose: Given the clinical urgency of the ongoing opioid crisis, alternative oral analgesics, like ketamine, are increasingly relevant. However, clinical trials and systematic reviews of oral ketamine for chronic cancer-related and non-cancer pain have employed a variety of dosing regimens. This key heterogeneity across studies may prove confusing to clinicians seeking to translate this literature into clinical practice. The present review sought to identify gaps in dosing regimens and adverse events reported in this literature.
Patients and Methods: A comprehensive search of MEDLINE, EMBASE, and PUBMED databases was conducted from January 1965 to July 2022 to identify studies on oral ketamine’s analgesic effects upon chronic pain. Data regarding ketamine dosage, inter-dose interval, pain relief, and adverse events were extracted. Only studies employing a range of 0.5 mg/kg BID–QID, or equivalent dosing, were included for benefit and risk analysis. Among 1556 initially identified studies, screening processes removed 17 duplicates, leaving 1539 for abstract review and 27 articles for data extraction. Due to dosing and study design inconsistencies, only 5 studies met criteria for quantitative analysis.
Results: Mean pain scores were determined to be 7.72/10 at the onset of treatment and 3.2/10 after 30– 90 days of treatment. A simple linear regression analysis demonstrated a correlation between average pain scores and treatment duration (R-square=0.76).
Conclusion: Oral ketamine benefits chronic pain, which may include allodynia and/or hyperalgesia, as deduced from various levels of evidence. Our evaluation suggests that oral ketamine has potential efficacy comparable to opioids for hyperalgesia and allodynia, and is generally well tolerated for chronic pain. Oral ketamine 0.5 mg/kg, when dosed 3 times daily for 7– 90 days, can achieve efficacy with an acceptable safety profile. This dosage regimen helps inform a need for standardized, evidence-based oral ketamine dosing for clinical care and future research when used as a component of a multimodal regimen for chronic cancer and non-cancer pain.
Keywords: oral ketamine, analgesia, standard dosing, safety
Introduction
The ongoing opioid crisis with its associated adverse effects, including tolerance and overdose, presents a major public health challenge.1 There exists a need for analgesic options that are associated with prevention of hyperalgesia and decreased opioid consumption while maintaining analgesia. Ketamine, known for its anti-nociceptive and antihyperalgesic properties primarily attributed to N-methyl-D-aspartate receptor (NMDAR) antagonism, presents a promising avenue for addressing chronic pain of various etiologies.2,3 Ketamine has been theoretically and clinically shown to reduce symptoms of central sensitization, including spinal wind-up and opioid-induced hypersensitization, and neurotoxicity.4–6 While most research has focused on intravenous administration, the longer-term effectiveness of ketamine is best explored through oral delivery owing to its clinical relevance (e.g., for home care), tolerability, ease of dosing, and cost-effectiveness.
Oral ketamine has been shown to have only 16–24% bioavailability7–9 but is effective at lower blood concentrations (40 ng/mL versus 100–160 ng/mL with IV and SQ ketamine).9–11 Accumulation of the metabolite norketamine likely enhances ketamine’s oral analgesic effectiveness. While oral ketamine’s elimination half-life is 2–3 hours,9–11 norketamine persists for <5 hours after dosing, likely contributing to a prolonged analgesic effect.2
Despite numerous publications across different levels of evidence highlighting its efficacy, a standardized clinical dosing regimen for oral ketamine administration, even as a starting dose, has yet to be attained. Variability in reports of adverse effects has further hindered its therapeutic utilization, although evidence suggests that adverse effects are largely dose-dependent and most often resolve with dose reduction.12,13
In 2010, Blonk et al attempted a quantitative analysis of oral ketamine in chronic pain but found only 22 relevant studies.14 In those publications, total daily dosing varied from 30 mg/day to 4 mg/kg/day. Without a standard dosing frequency, and with many other study variances, the quantitative analysis was unable to be completed.14 Mukhaizeemet et al published a retrospective review of oral ketamine in patients with treatment resistant chronic pain (2023). This study followed patients receiving treatment for <12 years. While this study of 73 patients showed reduced pain and few ketamine-related adverse effects, a dosing regimen could not be recommended with doses ranging from 193.84 to 1500 mg/day.2 In 2024, a large systematic review of multi-route ketamine treatment in cancer pain was completed. This analysis included 3 studies of oral ketamine; however, those oral daily doses ranged from 0.25 mg/kg/day to 400 mg/day.15 The variance in oral ketamine dosing among studies encumbers efforts to recommend a standard oral dose, while multi-route studies risk conflation of adverse events encountered in oral ketamine treatment. Therefore, we undertook this review to help determine an optimal standard ketamine dose that provided analgesic benefit, while better defining associated risks, in a difficult-to-treat patient population at greatest risk of adverse effects of opioid treatment including hyperalgesia and overdose.
When oral ketamine is administered as a standard oral dose of 0.5 mg/kg twice daily (BID) to four times daily (QID), or with a standard dose equal to such dosing, psychomimetic effects are infrequent.9,12 Furthermore, additional pain reduction appears to be related to the length of treatment for up to 3 months.
Material and Methods
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, which included identification, screening, confirmation of eligibility, and inclusion (Figure 1).16
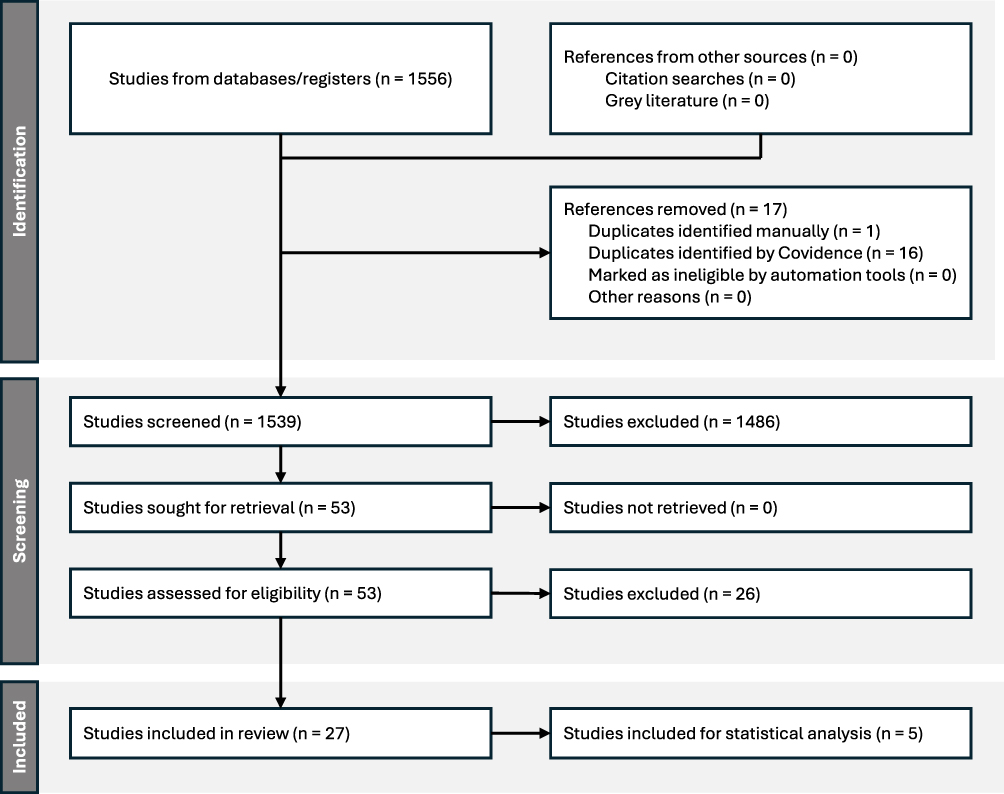 |
Figure 1 PRISMA Diagram. |
Search Strategy
A medical reference librarian devised and executed searches in the PubMed, Embase, and Web of Science databases, encompassing publications from January 1965 to June 2022 and restricted to English language. MeSH and Embase terms, such as ketamine OR esketamine, adverse effects, and pharmacologic actions, were employed. All searches were conducted on June 17, 2022. Full search strategies are detailed in Appendix 1.
The Covidence program facilitated screening of the initial 1556 articles obtained, resulting in removal of 17 duplicates and retention of 1539 articles for review. Inclusion criteria encompassed studies of all evidence levels utilizing oral ketamine for pain management in humans, with pain intensity as a measurable outcome. Exclusion criteria included non-English language, nonhuman subjects, inability to identify or quantify analgesic effects of oral ketamine, and review article status. Abstracts of all 1539 articles were independently reviewed by three reviewers, with conflicts resolved by the primary author. Subsequently, 53 articles meeting inclusion criteria were provided in the EndNote program format (see Supplementary Table 1) and underwent detailed review by the authors. Of these, 27 met criteria for further screening (see Supplementary Table 2) and the level of evidence was evaluated according to the Sackett Scale (Appendix 2). Decision for inclusion was based on adherence to pre-determined dosing and reported efficacy assessment method pre- and post-ketamine. Our accepted treatment dosing was ketamine 0.5 mg/kg orally (PO) BID-QID, or an equivalent standard dose given thrice daily, for a minimum of 7 days, and could be utilized as an adjuvant to morphine. Under these criteria, five of the articles were accepted into this evaluation. (Table 1). None of the retrieved studies evaluated ketamine as a single analgesic agent. Therefore, analysis was confined to studies administering oral ketamine as an adjunct to standard chronic pain care.
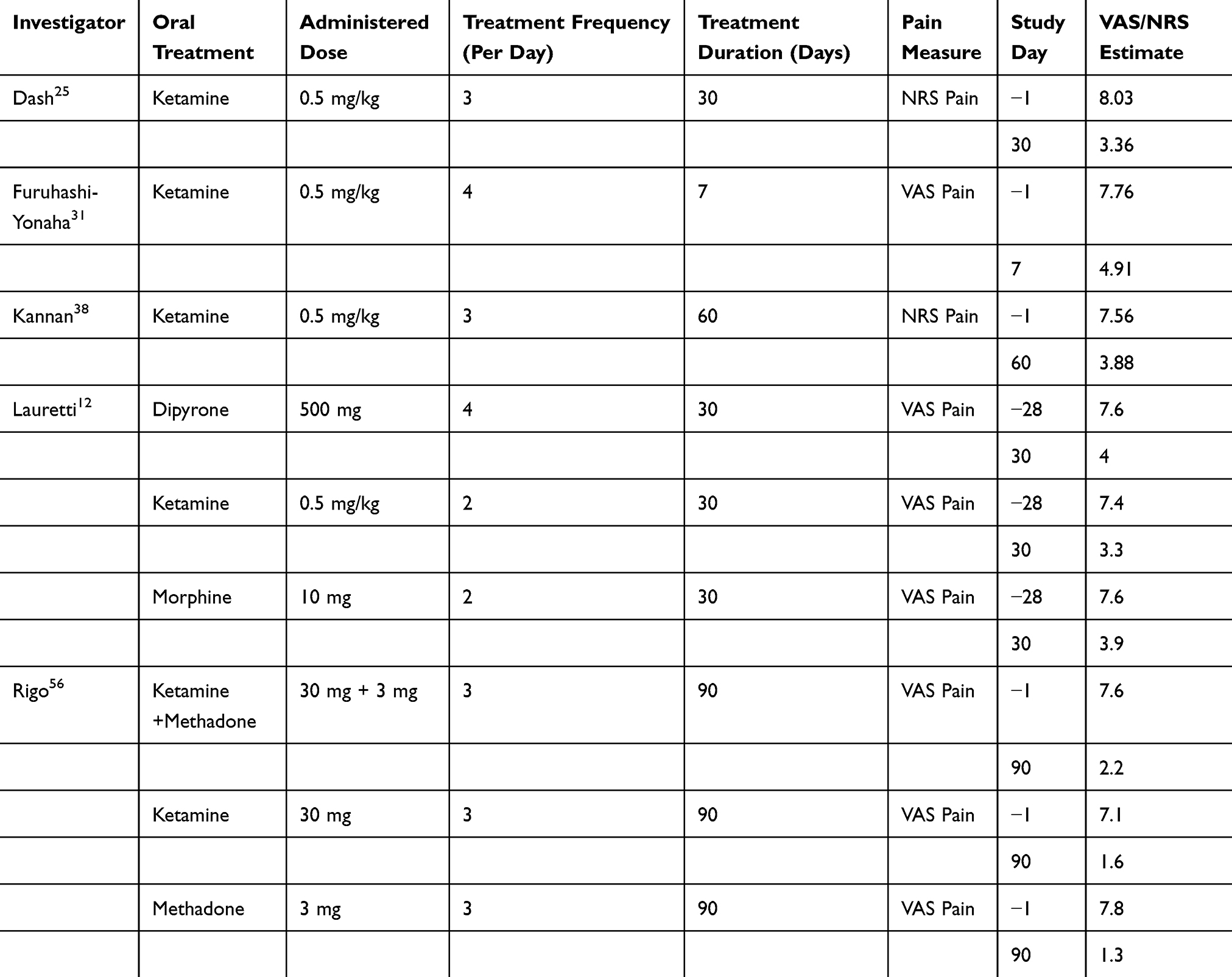 |
Table 1 VAS/NRS Pain Scores |
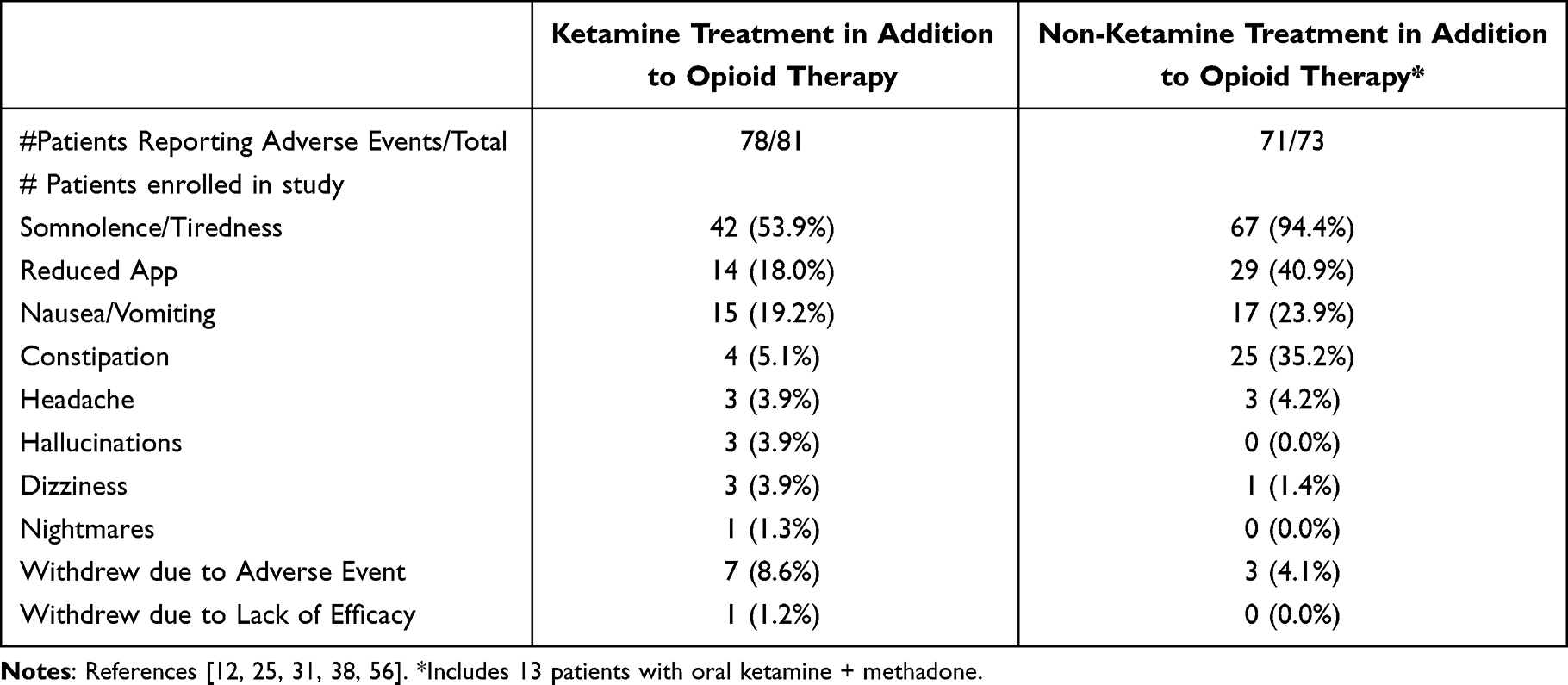 |
Table 2 Reported Adverse Effects in Ketamine vs Non-Ketamine Treatment |
Dispersion for efficacy endpoints and from safety reports were extracted from articles at all (published) times of evaluation. Similar data reported for non-ketamine treatments were also extracted. Safety data, which accompanied primary and secondary analyses, were extracted from studies and included respective analyses.
Statistical Analysis
Simple linear regression analysis was employed to assess changes in mean pain scores across treatment duration, with goodness of fit empirically evaluated with agreement of predicted and observed average scores. This included an average VAS/NRS pain score (11-point scale) as a function of duration of ketamine therapy (eg, study day; regardless of dose, duration, and dosing frequency). Results are presented in Table 1. Average VAS score was divided by 10, where warranted, to express averages across a common range. Two of these studies12,56 required the derivation of summary measures from published raw data.
Results
Primary analysis consisted of data extracted from 5 publications12,25,31,38,56 that met inclusion criteria. Four of the 5 studies reported ketamine administered at a dose, which was a function of body weight (ie, 0.5 mg/kg), while one study56 administered ketamine at a fixed 30 mg dose. Dosing frequency ranged across 2,12 3,25,38,56 and 4,31 administrations per day (Mean=2.9, SD=0.54). Duration of ketamine treatment prior to last assessment ranged across 7,31 30,25,47 6038 or 9056 days (Mean 37.2, SD=27.5). All five studies reported pre-treatment pain assessment results.
For the non-ketamine chronic pain therapies (eg, active controls) reported by Lauretti et al12 (morphine 10 mg PO q 12 hours, dipyrone 500 mg PO q 6 hours, and nitroglycerin 5 mg patch daily) and Rigo et al56 (Ketamine 30 mg + oral methadone 3 mg PO TID, oral methadone 3 mg PO TID), durations of treatment were the same as reported for ketamine.
In the Lauretti et al12 study, after 30 days treatment, average pain scores on an 11-point scale for morphine-treated patients was 3.9 (± 2.6), and the dipyrone group was 4 (± 1.6). The nitroglycerin group was 3.5 (± 1.7), and the ketamine treated group was 3.3 (± 1.6).
In the Rigo et al56 study, after 90 days of treatment, average pain score on an 11-point scale for ketamine+3 mg methadone patients was 2.2 (± 1.1), and the average for 3 mg methadone monotherapy was 1.3 (± 1.0). The ketamine treatment group had an average pain score of 1.6 (± 1.3).
In the five papers, treatment frequencies ranged from 2 to 4 per day (Mean = 2.9, SD = 0.54) with treatment durations spanning 7–90 days (Mean = 37.2, SD = 27.5). Mean pretreatment pain scores ranged from 7 to 8 (Mean=7.72, SD=0.96), with reductions observed across treatment durations. After 7 days,31 the average pain intensity score in ketamine-treated patients was 5 points. After 30 days,12,25 the average pain intensity score in ketamine-treated patients was 3 points. After 60 days,38 the average pain intensity score for ketamine-treated patients was 4 points. After 90 days,56 the average pain intensity score for ketamine-treated patients was 2 points. At the end of treatment, the mean pain intensity score was 3.2 (SD = 1.6), Figure 2.
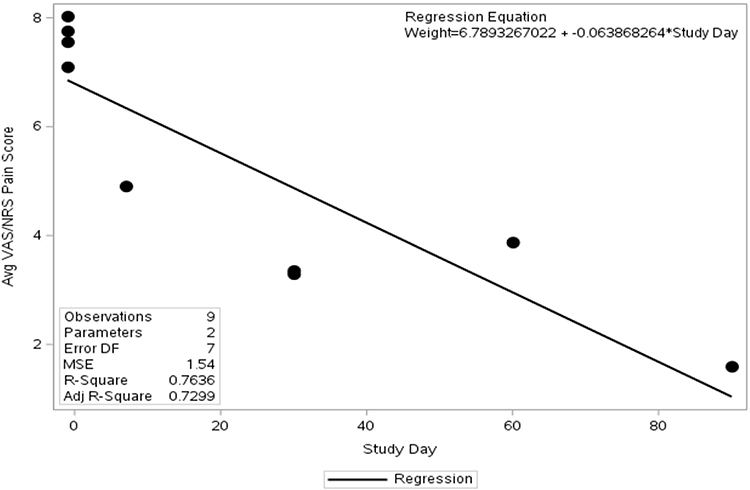 |
Figure 2 Linear Regression Analysis. |
Linear regression analysis indicated a strong relationship between average pain scores and treatment duration (R-square=0.76).
The pre-treatment average was predicted as 6.8 points, and at 7, 30, 60, and 90 days averages of 6.3, 4.9, 2.9, and 1.0 points (respectively) were predicted (R-square=0.76). With interpolation, the predicted average VAS/NRS (10-point) score at study day 15 was 5.8 points.
For patients in the ketamine arm of the studies, common adverse events included somnolence/tiredness, reduced appetite, and nausea/vomiting (reported in at least 3 of 5 studies). In 78 patients reporting adverse events, somnolence/tiredness was reported for 42 (53.9%), reduced appetite reported for 14 patients (18.0%), and nausea/vomiting was reported for 15 patients (19.2%).
Other reported symptoms in the ketamine-treated patients included constipation, which occurred in 4 patients (5.1%). Headache occurred in 3 patients (3.9%), and hallucinations also occurred in 3 patients (3.9%). Dizziness was reported in 3 patients (3.9%), and nightmares occurred in 1 patient (1.3%).
Discontinuation due to an adverse event occurred at a rate of 8.6% (7 of 81 total patients). Only 1.2% of ketamine-treated patients (1 of 81 total patients) discontinued due to lack of efficacy (Table 2).
One of the authors did not include reported adverse events for those who withdrew from the study.56 Therefore, the number of ketamine-treated patients reporting symptoms was reduced by a total of 3 from the number of participants initially enrolled in the study. Adverse events percentages were provided out of a total of 78 participants, while the number of withdrawals from studies was deducted from a total of 81.
For those patients treated with other agents (including additional oral morphine, dipyrone, topical nitroglycerin, methadone, and methadone + ketamine), common adverse events included somnolence/tiredness, reduced appetite, nausea/vomiting, and constipation. In 71 participants reporting adverse events, somnolence/tiredness was reported for 67 (94.4%), reduced appetite reported for 29 patients (40.9%), nausea/vomiting was reported for 17 (23.9%), and constipation reported for 25 patients (35.2%). Headache occurred in 3 patients (4.2%), and dizziness was reported in 1 patient (1.4%).
Discontinuation due to adverse events occurred in 3 out of 73 total patients (4.1%). There were no reports of patient discontinuations due to lack of efficacy.
Comparison of adverse events between ketamine and non-ketamine treatments for randomized control trials is included in Table 2.
One of the authors did not include reported adverse events for a total of 2 participants who withdrew from the study.56 Therefore, the percentages of adverse events was calculated out of a total of 71 patients. The number of withdrawals from studies was deducted from a total of 73 patients enrolled. One subject withdrew from an additional study due to adverse events, but was replaced so as not to affect the total number of participants.12
Discussion
Ketamine, a well-established anesthetic, has emerged as a potent analgesic at subanesthetic doses. Its unique pharmacological profile allows it to target neural plasticity and mitigate mechanisms consistent with central sensitization such as spinal wind-up and hyperalgesia.4,5 These features are critical in the management of chronic and refractory pain states, especially those involving opioid-induced hyperalgesia. The potential to “reset” the central nervous system69 underscores ketamine’s utility in pain management, particularly for individuals with complex pain syndromes. These properties present a novel approach to decrease opioid-dependence in the ongoing repercussions of the opioid crisis.1,2,15,46,47
In cancer-related pain, ketamine has garnered attention as a cornerstone adjuvant analgesic. When opioids lose efficacy, cause hyperalgesia, or when patients experience refractory breakthrough pain, ketamine has been characterized as an essential therapy. Reports highlight its capability to reduce opioid requirements, improve opioid efficacy, and enhance patient quality of life.12,15,25
Despite these advantages, adoption of ketamine for chronic pain has been limited by variability in dosing protocols and the absence of robust, standardized risk assessments. The pharmacokinetics of oral ketamine—notably lower plasma levels (40 ng/mL versus >100–160 ng/mL with IV administration)—offer a favorable safety profile, reducing the risk of psychomimetic adverse effects.10,11
At lower doses, ketamine’s primary action involves NMDA receptor antagonism. Higher doses, delivered via IV, IM, or IT routes, exhibit broader receptor interactions, including dopaminergic, monoaminergic, and opioid receptor binding, which increases the risk of side effects.70 Oral ketamine provides the additional benefit of norketamine production, a longer-acting analgesic byproduct. Due to undesirable activity of opioids in stimulating the NMDA-receptor, astrocytes, and microglia,71,72 ketamine offers an important analgesic opportunity. Additionally, it appears that the more severe or chronic the pain, and the longer a patient has been on opioid therapy, the more effective the analgesia of ketamine will be.46
While requiring oral ketamine dose of 0.5 mg/kg BID for 7 days as a minimum dosing for inclusion in our study, we accepted studies that included 0.5 mg/kg, or an equivalent standardized dose, <4 times daily for up to 90 days of treatment. Our review reveals a reduction in pain scores that can begin as early as 7 days, while improving with up to 90 days of treatment. We chose to analyze this data by plotting improvement as a function of time in linear regression, and this analysis identified a correlation between the duration of ketamine therapy and reductions in average Visual Analog Scale (VAS)/Numerical Rating Scale (NRS) scores.
Of note, 9 patients (11.5%) receiving oral ketamine during the studies remained on treatment after the study period.31,38 Data for 4 of those patients is available with their treatment lasting an additional of 9–54 months (average 30 months). Two of those patients were able to reduce their total ketamine dose by approximately 80% with no reported adverse effects or severe pain. The average final dose for those 4 patients was 66.5 mg/day.31
Commonly reported adverse effects associated with oral ketamine include somnolence, nausea, and loss of appetite, but were reported less frequently than those of alternative therapies. Importantly, the risk of constipation—a significant drawback of opioids—is markedly reduced, and reported with concomitant opioid treatment. Psychomimetic effects can be seen with oral ketamine at a dose of 0.5 mg/kg BID-QID. These may include hallucinations, headache, dizziness, and nightmares. Dose reduction is likely to treat, or reduce, these events.12,13 Patients who are considered at higher risk can be initiated on lower doses and/or treated concomitantly with low-dose benzodiazepine.31
Limitations and Research Opportunities
This paper faced significant limitations including the small number of included studies, diverse patient populations, and variability in dosing frequencies and duration of treatment. Additional confounders were within-study variability, including concomitant medications, disease process, and alternative treatments. One study included a cohort of patients receiving both oral ketamine and methadone in their alternative treatments.56
A meta-analysis was not possible given individual versus aggregate response summaries. As meta-analyses assume homogeneity across studies, our small sample size, with complex disease states and medication regimens, was problematic. However, linear regression afforded a means to assess treatment response, allowing for heterogeneity in studies and tracking of pain reduction across time. Exploratory analysis summarized improvement via multivariate approach where each study result was treated as an observation.
Active controls also included a variety of treatments, presenting neglected modifiers. This made comparative adverse effects difficult to generalize and prevented determination of ketamine’s independent effect. Again, one of the active controls included ketamine (30 mg oral ketamine + 3 mg methadone PO TID), increasing the risk for reported psychomimetic response in the active control group.
While existing evidence supports the safety and efficacy of oral ketamine, heterogeneity in study designs, dosing regimens, and patient populations limits broader conclusions, a situation frequently encountered when research involves palliative patient populations. Future research should prioritize standardized dosing protocols tailored to specific populations, including pediatric, geriatric, and cancer-related pain. Particular attention should focus on long-term efficacy and safety while controlling for variances in additional pain medication therapies.
Emerging evidence suggests that oral ketamine may offer benefit for individuals experiencing the often-intertwined burdens of chronic pain and depression. These frequently co-occurring conditions may amplify one another through shared neurobiological pathways, prolonging symptom duration and compounding functional decline. Dysregulation of serotonergic and noradrenergic systems—implicated in both nociceptive processing and affective states—provides a mechanistic rationale for ketamine’s cross-domain effects.73 Beyond its analgesic role, oral ketamine has been associated with improvements in mood, functional capacity, and overall quality of life, particularly in patients whose pain is enmeshed with emotional distress.2
A related avenue of inquiry lies in ketamine’s treatment of cancer-associated pain and depressive symptoms. As NMDA receptors have been identified not only on sensory neurons but also on immune cells and select solid tumor types, future consideration may be given to ketamine’s effect on tumor biology74 in addition to its analgesic and antidepressant effects.
Conclusion
The Initiative on Methods, Measurement and Pain Assessment in Clinical Trials (IMMPACT) consensus recommendations for the design of opioid-sparing interventions called for studies that would decrease total dosages of opioids, while providing analgesia, as a means to decrease opioid-related adverse outcomes.1 Oral ketamine is an emerging viable option in the management of chronic pain, particularly in refractory cases. With decreases in pain scores reported <41.6%,2 with superior reductions in allodynia and hyperalgesia,56 and potential efficacy comparable to opioids, ketamine offers a promising alternative for analgesia with anticipated opioid-dose reduction.
The integration of ketamine into multimodal pain management strategies, coupled with further research into optimal dosing and patient selection, positions it as a key ally in addressing the dual challenges of chronic pain and opioid reliance. As healthcare providers, we must advocate for the judicious use of ketamine, leveraging its unique pharmacological properties to improve patient outcomes and quality of life.
Acknowledgments
The authors wish to express their deep gratitude to Daniel P. Reyner, PhD, Ylisabyth S. Bradshaw, D.O., M.S. and John Mulder, M.D. (posthumously) for their contributions to the early development of this paper.
Disclosure
The authors have no funding sources, financial relationships, or conflicts of interest to disclose.
References
1. Gewandter JS, Smith SM, Dworkin RH, et al. Research approaches for evaluating opioid sparing in clinical trials of acute and chronic pain treatments: initiative on methods, measurement, and pain assessment in clinical trials recommendations. Pain. 2021;162(11):2669–10. PMID: 33863862; PMCID: PMC8497633. doi:10.1097/j.pain.0000000000002283
2. Al Mukhaizeem S, Nasa A, Waldron D, et al. Investigating the effectiveness of oral ketamine on pain, mood, and quality of life in treatment-resistant chronic pain. Front Pain Res. 2023;4:1268985. doi:10.3389/fpain.2023.1268985
3. Guimarães Pereira JE, Ferreira Gomes Pereira L, Mercante Linhares R, Darcy Alves Bersot C, Aslanidis T, Ashmawi HA. Efficacy and safety of ketamine in the treatment of neuropathic pain: a systematic review and meta-analysis of randomized controlled trials. J Pain Res. 2022;1011–1037. doi:10.2147/JPR.S358070
4. Dahan A, van Velzen M, Niesters M. Ketamine for neuropathic pain: a tiger that won’t bite? Br J Anaesth. 2020;125(3):e275–e276. doi:10.1016/j.bja.2020.05.009
5. Mion G, Villevieille T. Ketamine pharmacology: an update (pharmacodynamics and molecular aspects, recent findings). CNS Neurosci Ther. 2013;19(6):370–380. doi:10.1111/cns.12099
6. Winegarden JA, Carr DB, Bradshaw Y. Intravenous ketamine for rapid opioid-dose reduction, reversal of opioid-induced neurotoxicity, and pain control in terminal care. Pain Med. 2016;17(4):644–649. doi:10.1111/pme.12865
7. Chong C, Schug SA, Page-Sharp M, Jenkins B, Ilett KF. Development of a sublingual/oral formulation of ketamine for use in neuropathic pain. Clin Drug Invest. 2009;29(5):317–324. doi:10.2165/00044011-200929050-00004
8. Yanagihara Y, Ohtani M, Kariya S, et al. Plasma concentration profiles of ketamine and norketamine after administration of various ketamine preparations to healthy Japanese volunteers. Biopharm Drug Dispos. 2003;24(1):37–43. doi:10.1002/bdd.336
9. Zanos P, Moaddel R, Morris PJ, et al. Ketamine and ketamine metabolite pharmacology: insights into therapeutic mechanisms. Pharmacol Rev. 2018;70(3):621–660. doi:10.1124/pr.117.015198
10. Clements JA, Nimmo WS, Grant IS. Bioavailability, pharmacokinetics, and analgesic activity of ketamine in humans. J Pharm Sci. 1982;71(5):539–542. doi:10.1002/jps.2600710516
11. Grant IS, Nimmo WS, Clements JA. Pharmacokinetics and analgesic effects of IM and oral ketamine. BJA: Br J Anaesth. 1981;53(8):805–810. doi:10.1093/bja/53.8.805
12. Lauretti GR, Lima IC, Reis MP, Prado WA, Pereira NL. Oral ketamine and transdermal nitroglycerin as analgesic adjuvants to oral morphine therapy for cancer pain management. Anesthesiology. 1999;90(6):1528–1533. doi:10.1097/00000542-199906000-00005
13. Okon T. Ketamine: an introduction for the pain and palliative medicine physician. Pain Physician. 2007;10(1533–3159):493–500. doi:10.36076/ppj.2007/10/493
14. Blonk MI, Koder BG, van den Bemt PM, Huygen FJ. Use of oral ketamine in chronic pain management: a review. Eur J Pain. 2010;14(5):466–472. doi:10.1016/j.ejpain.2009.09.005
15. Jiao J, Fan J, Zhang Y, Chen L. Efficacy and safety of ketamine to treat cancer pain in adult patients: a systematic review. J Pain Symptom Manage. 2024;67(3):e185–e210. doi:10.1016/j.jpainsymman.2023.11.004
16. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
17. Amin P, Roeland E, Atayee R. Case report: efficacy and tolerability of ketamine in opioid-refractory cancer pain. J Pain Palliat Care Pharmacother. 2014;28(3):233–242. PMID: 25102039. doi:10.3109/15360288.2014.938881
18. Benítez-Rosario MA, Feria M, Salinas-Martín A, Martínez-Castillo LP, Martín-Ortega JJ. A retrospective comparison of the dose ratio between subcutaneous and oral ketamine. J Pain Symptom Manage. 2003;25(5):400–402. PMID: 12727033. doi:10.1016/s0885-3924(03)00072-1
19. Benítez-Rosario MA, Salinas-Martín A, González-Guillermo T, Feria M. A strategy for conversion from subcutaneous to oral ketamine in cancer pain patients: effect of a 1:1 ratio. J Pain Symptom Manage. 2011;41(6):1098–1105. PMID: 21398087. doi:10.1016/j.jpainsymman.2010.08.017
20. Bredlau AL, McDermott MP, Adams HR, et al. Oral ketamine for children with chronic pain: a pilot Phase 1 study. J Pediatr. 2013;163(1):194–200.e1. PMID: 23403253; PMCID: PMC3799772. doi:10.1016/j.jpeds.2012.12.077
21. Broadley KE, Kurowska A, Tookman A. Ketamine injection used orally. Palliat Med. 1996;10(3):247–250. PMID: 8817596. doi:10.1177/026921639601000309
22. Chen C, Cheng X, Lin L, Fu F. Preanesthetic nebulized ketamine vs preanesthetic oral ketamine for sedation and postoperative pain management in children for elective surgery: a retrospective analysis for effectiveness and safety. Medicine. 2021;100(6):e24605. PMID: 33578565; PMCID: PMC7886447. doi:10.1097/MD.0000000000024605
23. Chong CC, Schug SA. Efficacy and tolerability of oral compared with sublingual ketamine lozenges as rescue analgesics in adults for acute pain: the OSKet trial. Clin Drug Investig. 2021;41(9):817–823. PMID: 34368943. doi:10.1007/s40261-021-01066-x
24. Cvrcek P. Side effects of ketamine in the long-term treatment of neuropathic pain. Pain Med. 2008;9(2):253–257. PMID: 18298710. doi:10.1111/j.1526-4637.2007.00314.x
25. Dash SK, Mohanty S, Mohanty D. Effect of oral ketamine as adjuvant for treatment of neuropathic pain in cancer patients. J Evol Med Dent Sci. 2018;7(7):895–900. doi:10.14260/jemds/2018/204
26. Eide PK, Stubhaug A. Relief of glossopharyngeal neuralgia by ketamine-induced N-methyl-aspartate receptor blockade. Neurosurgery. 1997;41(2):505–508. PMID: 9257324. doi:10.1097/00006123-199708000-00043
27. Enarson MC, Hays H, Woodroffe MA. Clinical experience with oral ketamine. J Pain Symptom Manage. 1999;17(5):384–386. PMID: 10355218. doi:10.1016/s0885-3924(99)00011-1
28. Fallon MT, Wilcock A, Kelly CA, et al. Oral ketamine vs placebo in patients with cancer-related neuropathic pain: a randomized clinical trial. JAMA Oncol. 2018;4(6):870–872. doi:10.1001/jamaoncol.2018.0131
29. Fisher K, Hagen NA. Analgesic effect of oral ketamine in chronic neuropathic pain of spinal origin: a case report. J Pain Symptom Manage. 1999;18(1):61–66. PMID: 10439575. doi:10.1016/s0885-3924(99)00018-4
30. Fitzgibbon EJ, Hall P, Schroder C, Seely J, Viola R. Low dose ketamine as an analgesic adjuvant in difficult pain syndromes: a strategy for conversion from parenteral to oral ketamine. J Pain Symptom Manage. 2002;23(2):165–170. PMID: 11844639. doi:10.1016/s0885-3924(01)00393-1
31. Furuhashi-Yonaha A, Iida H, Asano T, Takeda T, Dohi S. Short- and long-term efficacy of oral ketamine in eight chronic-pain patients. Can J Anesth. 2002;49(8):886–887. doi:10.1007/BF03017431
32. Haines DR, Gaines SP. N of 1 randomised controlled trials of oral ketamine in patients with chronic pain. Pain. 1999;83(2):283–287. PMID: 10534600. doi:10.1016/s0304-3959(99)00117-7
33. Heidari SM, Saghaei M, Hashemi SJ, Parvazinia P. Effect of oral ketamine on the postoperative pain and analgesic requirement following orthopedic surgery. Acta Anaesthesiol Taiwan. 2006;44(4):211–215. PMID: 17233365.
34. Inomata S, Kakiuchi Y, Miyabe M, et al. Combined therapy with clonidine and amantadine may act in two stages of glutamate-mediated neuropathic pain caused by a needle puncture in an upper extremity. Anesth Analg. 2005;101(3):921–922. PMID: 16116017. doi:10.1213/01.ANE.0000173661.50789.25
35. Jennings CA, Bobb BT, Noreika DM, Coyne PJ. Oral ketamine for sickle cell crisis pain refractory to opioids. J Pain Palliat Care Pharmacother. 2013;27(2):150–154. PMID: 23692261. doi:10.3109/15360288.2013.788599
36. Juel J, Olesen SS, Olesen AE, et al. Study protocol for a randomised, double-blinded, placebo-controlled, clinical trial of S-ketamine for pain treatment in patients with chronic pancreatitis (RESET trial). BMJ Open. 2015;5(3):e007087. PMID: 25757947; PMCID: PMC4360788. doi:10.1136/bmjopen-2014-007087
37. Kamel AAF, Amin OAI. Analgo-sedative effects of oral or nebulized ketamine in preschoolers undergoing elective surgery: a comparative, randomized, double-blind study. Pain Physician. 2020;23(2):E195–E202. [PMID: 32214298]. doi:10.36076/ppj.2020/23/E195
38. Kannan TR, Saxena A, Bhatnagar S, Barry A. Oral ketamine as an adjuvant to oral morphine for neuropathic pain in cancer patients. J Pain Symptom Manage. 2002;23(1):60–65. doi:10.1016/S0885-3924(01)00373-6
39. Kapur N, Friedman R. Oral ketamine: a promising treatment for restless legs syndrome. Anesth Analg. 2002;94(6):1558–9, tableofcontents. PMID: 12032026. doi:10.1097/00000539-200206000-00034
40. Kaviani N, Khademi A, Ebtehaj I, Mohammadi Z. The effect of orally administered ketamine on requirement for anesthetics and postoperative pain in mandibular molar teeth with irreversible pulpitis. J Oral Sci. 2011;53(4):461–465. PMID: 22167031. doi:10.2334/josnusd.53.461
41. Kim K, Mishina M, Kokubo R, et al. Ketamine for acute neuropathic pain in patients with spinal cord injury. J Clin Neurosci. 2013;20(6):804–807. PMID: 23618680. doi:10.1016/j.jocn.2012.07.009
42. Klepstad P, Borchgrevink PC. Four years’ treatment with ketamine and a trial of dextromethorphan in a patient with severe post-herpetic neuralgia. Acta Anaesthesiologica Scandinavica. 1997;41:422–426. doi:10.1111/j.1399-6576.1997.tb04709.x
43. Kubota T, Miyata A. Successful use of ketamine for intractable burning pain of HTLV-1-associated myelopathy. J Pain Symptom Manage. 2005;30(5):397–399. PMID: 16310613. doi:10.1016/j.jpainsymman.2005.10.001
44. Kundra P, Velayudhan S, Krishnamachari S, Gupta SL. Oral ketamine and dexmedetomidine in adults’ burns wound dressing--A randomized double blind cross over study. Burns. 2013;39(6):1150–1156. PMID: 23623339. doi:10.1016/j.burns.2013.02.012
45. MacKintosh D, Brady A, Carr S. Ketamine: a real-world experience in cancer pain. J Palliat Med. 2012;15(7):733. PMID: 22780114. doi:10.1089/jpm.2012.0077
46. Marchetti F, Coutaux A, Bellanger A, Magneux C, Bourgeois P, Mion G. Efficacy and safety of oral ketamine for the relief of intractable chronic pain: a retrospective 5-year study of 51 patients. Eur J Pain. 2015;19(7):984–993. doi:10.1002/ejp.624
47. Mercadante S, Arcuri E, Ferrera P, Villari P, Mangione S. Alternative treatments of breakthrough pain in patients receiving spinal analgesics for cancer pain. J Pain Symptom Manage. 2005;30(5):485–491. doi:10.1016/j.jpainsymman.2005.04.014
48. Mikkelsen S, Jørgensen H, Larsen PS, Brennum J, Dahl JB. Effect of oral ketamine on secondary hyperalgesia, thermal and mechanical pain thresholds, and sedation in humans. Reg Anesth Pain Med. 2000;25(5):452–458. PMID: 11009229. doi:10.1053/rapm.2000.8456
49. Moazam C, Hirst J, Mesarwi P, Atayee RS. Ketamine: when delirium and desperation call for a hero. J Pain Palliat Care Pharmacother. 2019;33(3–4):120–124. PMID: 31689170. doi:10.1080/15360288.2019.1686099
50. Nikolajsen L, Hansen PO, Jensen TS. Oral ketamine therapy in the treatment of postamputation stump pain. Acta Anaesthesiol Scand. 1997;41(3):427–429. PMID: 9113191. doi:10.1111/j.1399-6576.1997.tb04710.x
51. Norambuena C, Yañez J, Flores V, Puentes P, Carrasco P, Villena R. Oral ketamine and midazolam for pediatric burn patients: a prospective, randomized, double-blind study. J Pediatr Surg. 2013;48(3):629–634. PMID: 23480923. doi:10.1016/j.jpedsurg.2012.08.018
52. Prommer E. Ketamine to control pain. J Pal Med. 2003;6(3):443–446. doi:10.1089/109662103322144808
53. Qureshi FA, Mellis PT, McFadden MA. Efficacy of oral ketamine for providing sedation and analgesia to children requiring laceration repair. Pediatr Emerg Care. 1995;11(2):93–97. PMID: 7596886. doi:10.1097/00006565-199504000-00009
54. Rayala S, Kyander M, Haridass V, et al. Low-dose oral ketamine as a procedural analgesia in pediatric cancer patients undergoing bone marrow aspirations at a resource-limited cancer hospital in India. Indian J Palliat Care. 2019;25(4):501–507. PMID: 31673202; PMCID: PMC6812415. doi:10.4103/IJPC.IJPC_110_19
55. Rayala S, Bäckdahl T, Reddy N, et al. Low-dose oral ketamine for procedural analgesia in pediatric cancer patients undergoing lumbar puncture at a resource-limited cancer hospital in India. J Palliat Med. 2019;22(11):1357–1363. PMID: 31090488. doi:10.1089/jpm.2018.0667
56. Rigo FK, Trevisan G, Godoy MC, et al. Management of neuropathic chronic pain with methadone combined with ketamine: a randomized, double blind, active-controlled clinical trial. Pain Physician. 2017;20(3):207.
57. Rothrock SG, Johnson NE. Pain management in the pediatric emergency department. Pediatr Emerg Care. 1989;5(4):298. PMID: 2602211.
58. Ryan NM, James R, Downes MA, Isbister GK. Low-dose ketamine provides poor analgesia for pain in redback spider envenoming. Br J Clin Pharmacol. 2019;85(10):2423–2427. PMID: 31269538; PMCID: PMC6783601. doi:10.1111/bcp.14052
59. Sakai T, Tomiyasu S, Ono T, Yamada H, Sumikawa K. Multiple sclerosis with severe pain and allodynia alleviated by oral ketamine. Clin J Pain. 2004;20(5):375–376. PMID: 15322448. doi:10.1097/00002508-200409000-00016
60. Saroyan JM, Tresgallo ME, Farkouh C, Morel KD, Schechter WS. The use of oral ketamine for analgesia with dressing change in an infant with epidermolysis bullosa: report of a case. Pediatr Dermatol. 2009;26(6):764–766. PMID: 20199468. doi:10.1111/j.1525-1470.2009.01036.x
61. Singh C, Pandey RK, Saksena AK, Chandra G. A comparative evaluation of analgo-sedative effects of oral dexmedetomidine and ketamine: a triple-blind, randomized study. Paediatr Anaesth. 2014;24(12):1252–1259. PMID: 25065424. doi:10.1111/pan.12493
62. Soto E, Stewart DR, Mannes AJ, et al. Oral ketamine in the palliative care setting: a review of the literature and case report of a patient with neurofibromatosis type 1 and glomus tumor-associated complex regional pain syndrome. Am J Hosp Palliat Care. 2012;29(4):308–317. PMID: 21803784; PMCID: PMC4239997. doi:10.1177/1049909111416345
63. Tobias JD, Phipps S, Smith B, Mulhern RK. Oral ketamine premedication to alleviate the distress of invasive procedures in pediatric oncology patients. Pediatrics. 1992;90(4):537–541. [PMID: 1408506]. doi:10.1542/peds.90.4.537
64. Ugur F, Gulcu N, Boyaci A. Oral ketamine for pain relief in a child with abdominal malignancy. Pain Med. 2009;10(1):120–121. PMID: 18346059. doi:10.1111/j.1526-4637.2008.00424.x
65. Urch CE, Chamberlain JH. Ketamine analgesia in vasculitic pain. Br J Rheumatol. 1998;37(6):702–703. PMID: 9667633. doi:10.1093/rheumatology/37.6.702
66. Vick PG, Lamer TJ. Treatment of central post-stroke pain with oral ketamine. Pain. 2001;92(1–2):311–3.doi. PMID: 11323153. doi:10.1016/s0304-3959(00)00488-7
67. Waldfogel JM, Nesbit S, Cohen SP, Dy SM. Successful treatment of opioid-refractory cancer pain with short-course, low-dose ketamine. J Pain Palliat Care Pharmacother. 2016;30(4):294–297. PMID: 27754734. doi:10.1080/15360288.2016.1231732
68. Yamamoto T, Watanabe M, Obuchi T, et al. Importance of pharmacological evaluation in the treatment of poststroke pain by spinal cord stimulation. Neuromodulation. 2016;19(7):744–751. PMID: 26990444. doi:10.1111/ner.12408
69. Borsook D. Ketamine and chronic pain – going the distance. Pain. 2009;145(3):271–272. doi:10.1016/j.pain.2009.05.021
70. Bell RF, Kalso EA. Ketamine for pain management. PAIN Rep. 2018;3(5):e674. doi:10.1097/pr9.0000000000000674
71. Liu X, Bae C, Liu B, et al. Development of opioid-induced hyperalgesia depends on reactive astrocytes controlled by Wnt5a signaling. Mol Psychiatry. 2023;28(2):767–779. doi:10.1038/s41380-022-01815-0
72. Pahan P, Xie JY. Microglial inflammation modulates opioid analgesic tolerance. J Neurosci Res. 2023;101(9):1383–1392. doi:10.1002/jnr.25199
73. Voute M, Lambert C, Pereira B, Pickering G. Assessment of initial depressive state and pain relief with ketamine in patients with chronic refractory pain. JAMA Network Open. 2023;6(5):e2314406. doi:10.1001/jamanetworkopen.2023.14406
74. Rodriguez Arango JA, Zec T, Khalife M. Perioperative ketamine and cancer recurrence: a comprehensive review. J Clin Med. 2024;13(7):1920. PMID: 38610685; PMCID: PMC11012833. doi:10.3390/jcm13071920
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.