Back to Journals » Journal of Asthma and Allergy » Volume 16
Oral Corticosteroid Reduction Between Biologics Initiated and Non-Initiated Patients with Severe Asthma
Authors Tanaka A, Takahashi M, Fukui A, Arita Y, Fujiwara M ![]() , Makita N, Tashiro N
, Makita N, Tashiro N
Received 16 March 2023
Accepted for publication 20 July 2023
Published 14 August 2023 Volume 2023:16 Pages 839—849
DOI https://doi.org/10.2147/JAA.S411404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Luis Garcia-Marcos
Akihiko Tanaka,1 Mai Takahashi,2 Ayako Fukui,3 Yoshifumi Arita,3 Masakazu Fujiwara,3 Naoyuki Makita,3 Naoki Tashiro3
1Division of Respiratory Medicine and Allergology, Department of Medicine, School of Medicine, Showa University, Tokyo, Japan; 2Medical, AstraZeneca K.K., Tokyo, Japan; 3Medical, AstraZeneca K.K., Osaka, Japan
Correspondence: Akihiko Tanaka, Division of Respiratory Medicine and Allergology, Department of Medicine, School of Medicine, Showa University, 1-5-8 Hatanodai Shinagawa-ku, Tokyo, 142-8666, Japan, Tel +81 3-3784-8000, Fax +81 3-3784-8517, Email [email protected]
Purpose: The oral corticosteroid (OCS)-sparing effect of several biologics (BIOs) has been shown in clinical trials. To date, no study has evaluated differences in OCS dose reduction between BIO-initiated and BIO-non-initiated patients in real-world clinical practice. We compared dose reductions in maintenance OCS between BIO-initiated and BIO-non-initiated severe asthma patients in a real-world setting.
Patients and Methods: This retrospective cohort study used the data from the Diagnosis Procedure Combination database of Medical Data Vision in Japan. Severe asthma patients with continuous use of OCS were selected from December 2015 to February 2020. The primary endpoint was the proportion reduction in daily maintenance OCS dose from Week 0 to Week 24. Analyses were performed using inverse probability treatment weighting.
Results: In total, 2927 patients were included (BIO-initiated: 239 patients, BIO-non-initiated: 2688 patients). Adjusted median (quartile [Q] 1–Q3) proportion reduction in daily maintenance OCS dose at Week 24 from the index date was 25.0% (0.0– 100.0%) and 0.0% (0.0– 83.3%) in the BIO-initiated and BIO-non-initiated groups, respectively (Hodges–Lehmann estimate [95% confidence interval], 0.0000% [0.0000– 0.3365%]). Respective proportions of patients in the BIO-initiated and BIO-non-initiated groups achieving dose reductions from the index date in the daily maintenance OCS dose at Week 24 were > 0% reduction, 56.6% and 44.1% (odds ratio [OR] 1.6554); ≥ 25% reduction, 50.5% and 40.6% (OR 1.4888); ≥ 50% reduction, 42.8% and 33.7% (OR 1.4714); and 100% reduction, 26.2% and 24.4% (OR 1.1005).
Conclusion: Among severe asthma patients, the daily dose of maintenance OCS was reduced with BIO treatment. Although a higher percentage of patients in the BIO-initiated group had an OCS reduction of ≤ 75% than the BIO-non-initiated group, we found no clear difference in OCS reduction. Our findings will be justified by further research that incorporates a longer observation period and variables excluded from this study.
Trial Registration: ClinicalTrials.gov (NCT05136547).
Keywords: severe asthma, asthma exacerbation, oral corticosteroid, biologics, retrospective cohort study
Plain Language Summary
Patients with severe uncontrolled asthma receive maintenance therapy with oral corticosteroids to control their symptoms and prevent exacerbations. However, long-term use of oral corticosteroids causes many side effects. Biologics are drugs used to treat severe asthma that have been found to improve lung function, reduce asthma exacerbations, and reduce the amount of oral corticosteroids needed. However, to date, no studies have investigated the differences in oral corticosteroid dose reduction between severe asthma patients treated and not treated with biologics in real-world clinical practice.
This study investigated the reduction in oral corticosteroid use after 24 weeks in severe asthma patients who were either initiated or not initiated with biologics by using data from a health insurance claim database. The daily dose of maintenance oral corticosteroid was reduced with the use of biologics. However, no clear difference was observed in the oral corticosteroid dose reduction between patients initiated and not initiated with biologics. Several study limitations may have contributed to our study results, and therefore, further research is warranted to validate our findings.
Introduction
Symptoms of asthma are generally controlled with inhaled corticosteroids (ICS) and long-acting β2-agonists (LABA).1,2 Approximately 5–10% of asthma patients in the general population have severe asthma,3 which is defined as asthma for which high-dose ICS therapy and an additional controller medication are necessary to achieve control or asthma that remains uncontrolled despite this treatment.4 In Japan, a recent study estimated that the prevalence of severe asthma was 7.8%.5
Currently, patients with severe uncontrolled asthma receive maintenance therapy with oral corticosteroids (OCS) to control symptoms and prevent the recurrence of exacerbations. However, the risk of adverse drug reactions such as diabetes mellitus, osteoporosis, and psychiatric disorders increases with prolonged OCS administration; therefore, reducing the dose is considered an important treatment modality in patients with severe asthma.1,2 Additionally, prolonged OCS administration is no longer the preferred option in the latest Global Initiative for Asthma guidelines.4
In recent years, several biologics (BIOs), including anti-immunoglobulin E antibodies (omalizumab), anti-interleukin (IL)-5 antibodies (mepolizumab), anti-IL-5 receptor α antibodies (benralizumab), and anti-IL-4 receptor α antibodies (dupilumab), have been licensed for the treatment of severe asthma. The benefits of these BIOs are dependent on phenotypic testing and correct BIO selection;4 nevertheless, BIOs have been reported to have an OCS-sparing effect, as well as lowering the frequency of exacerbations and improving quality of life in placebo-controlled clinical trials.2,6–8 However, unlike clinical trials with strict OCS dose reduction criteria stipulated in their protocols, OCS dose reduction in real-world clinical practice is at the physician’s clinical discretion and is based on subjective measures of a patient’s symptoms and exacerbation status. Other factors such as current OCS dose, pulmonary function, and the physician’s experience with OCS sparing may also play a role.
We hypothesized that the maintenance OCS dose at 24 weeks would be lower in BIO-initiated patients than in BIO-non-initiated patients in real-world clinical practice in Japan. The objective of this study was to compare the dose reduction in maintenance OCS at Week 24 between BIO-initiated and BIO-non-initiated severe asthma patients in a real-world setting.
Materials and Methods
Study Design
This was a retrospective cohort study of patients diagnosed with severe asthma conducted using data from 22 December 2015 to 29 February 2020. De-identified data were extracted from the Diagnosis Procedure Combination (DPC) database (Supplementary Figure 1). The data source was the Medical Data Vision (MDV) database, which collects claims and DPC data and has a coverage of approximately 22% of 1727 DPC hospitals in Japan. DPC hospitals are large medical institutions that provide comprehensive medical services to patients in Japan. The MDV database includes data on the treatments prescribed in hospitals, regardless of insurance coverage, and BIOs administered at medical facilities in Japan.
This study aimed to determine the OCS-sparing effect of BIOs for OCS prescribed during the observation period. Based on real-world clinical practice, maintenance therapy was reached when the number of OCS prescription days was ≥8 days to distinguish from short-term OCS use.
Patients in the BIO-initiated group and the BIO-non-initiated group were defined as follows: the BIO-initiated group included patients with a record of one or more BIO prescriptions between 7 June 2016 and 14 September 2019 and the BIO-non-initiated group included patients without a record of a BIO prescription, which were omalizumab, mepolizumab, benralizumab and dupilumab during the entire study period. The index date of the BIO-initiated group was defined as the date when the BIO treatment was prescribed for the first time after 7 June 2016, when mepolizumab was launched in Japan. The index date of the BIO-non-initiated group was defined as the date when maintenance OCS was prescribed after 7 June 2016. If multiple dates were identified for a patient, the index date was selected randomly to avoid biased selection of the index date in terms of OCS prescription duration. In addition, OCS prescription duration was included as a covariate in propensity score estimation to minimize the impact of bias.
This study was conducted as per the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects. The data for this study were extracted from a commercially available de-identified database. According to the ethical guidelines above, informed consent is not required for de-identified data. This study was registered at ClinicalTrials.gov under the identifier number NCT05136547.
Patients
The groups included patients with severe asthma who satisfied the inclusion criteria. The inclusion criteria were as follows: Patients ≥16 years old at the start of observation who were prescribed a high-dose ICS or ICS/LABA during the baseline period of 24 weeks before the index date and with a diagnosis of asthma (International Statistical Classification of Diseases and Related Health Problems [ICD]-10: J45 [asthma] or J46 [status asthmaticus]); a record of at least one hospital visit during the baseline period, at least two hospital visits during the observation period, and at least one hospital visit after the observation period; and a total maintenance OCS prescription duration ≥12 weeks during the baseline period (including the observation start date).
Patients with autoimmune diseases as per the following ICD-10 codes were excluded from this study as these diseases may require OCS for treatment: M05 (rheumatoid arthritis with rheumatoid factor), M06 (other rheumatoid arthritis), M30 (polyarteritis nodosa and related conditions), L93 (lupus erythematosus), M32 (systemic lupus erythematosus), K50 (Crohn disease [regional enteritis]), K51 (ulcerative colitis), K52 (other noninfective gastroenteritis and colitis), and N04 (nephrotic syndrome with minor glomerular abnormality).
Study Endpoints
The primary endpoint was the proportion reduction in the daily maintenance OCS dose from Week 0 to Week 24 in the full analysis set (FAS). The secondary endpoint was the proportions of patients in the FAS who achieved a >0%, ≥25%, ≥50%, or 100% reduction in their daily maintenance OCS dose from Week 0 to Week 24. Exploratory endpoints included: proportion reductions in the daily maintenance OCS dose from Week 0 to Week 24 in different patient subgroups; proportions of patients who achieved a >0%, ≥25%, ≥50%, or 100% reduction in the daily maintenance OCS dose from Week 0 to Week 24 in different patient subgroups; reductions in the daily maintenance OCS dose from Week 0 to Weeks 8 and 16 in the FAS; and reductions in the daily maintenance OCS dose at Week 24 for benralizumab- or mepolizumab-initiated and BIO-non-initiated groups.
Statistical Analysis
Regarding the sample size calculation and rationale, 188 BIO-initiated severe asthma patients and approximately 3500 BIO-non-initiated severe asthma patients were identified in this database through a feasibility assessment. If the mean difference between the groups and a common standard deviation (SD) for proportion reduction of OCS dose were 30% and 50%, respectively, based on benralizumab and dupilumab OCS-sparing studies,2,6,7 the expected sample size based on the feasibility assessment provides a power >90%, with a two-sided significance level of 0.05.
The inverse probability treatment weighting (IPTW) method using propensity scores was used to minimize bias. The following covariates were included in the propensity score estimation: index date, age, sex, cumulative maintenance OCS prescription days, OCS dose, short-acting β2-agonist prescription, asthma exacerbation with OCS, asthma exacerbation with hospitalization, allergic rhinitis, chronic rhinosinusitis, and atopic dermatitis.
The analytical study population was the FAS, defined as all individuals who met the inclusion/exclusion criteria in the MDV database during the study period.
For the primary endpoint analysis, the proportion reduction of OCS dose from Week 0 to Week 24 was evaluated using a functional response model-based causal Wilcoxon rank-sum test9 with IPTW weights. Median differences between groups were estimated using the Hodges–Lehmann estimator, weighted by IPTW, and a two-sided confidence interval (CI). A sensitivity analysis was based on a stratified Wilcoxon rank-sum test, stratified by covariates included in the propensity score model.
In Phase 1, a propensity score estimation was performed. Spearman correlations were calculated for all pairs of covariates. If covariates were highly correlated (eg, Spearman correlation >0.7), then exclusion or merging of covariates were considered. The propensity scores for initiating BIOs were estimated based on two versions of logistic models: the continuous version, which included continuous covariates as is, and the categorical version, which included continuous covariates categorized. Once propensity scores were estimated, the mean (SD) and the minimum and maximum weight of the IPTW were calculated. If there were no extreme values, it was assumed that the positivity was satisfied, and there were no clear misspecifications of the propensity score model. If the condition was not satisfied, propensity score estimation might have been repeated using a different set of covariates. After estimating the propensity score, balance diagnostics were performed along with the standardized difference between groups in the original sample. Similarly, a descriptive summary of covariates was calculated in the weighted sample for both continuous and categorical versions (based on the weight of IPTW estimated). If the absolute mean standardized difference was ≤0.10, it was considered sufficiently balanced.
If all of the following conditions were met in either continuous or categorical versions of the model, then Phase 2 analysis was conducted as planned using the IPTW approach: (a) no extreme weights and (b) standardized differences in the weighted sample are ≤0.10 for all covariates included in the propensity score model. If both models satisfied these conditions and there was no clear advantage in standardized differences, then the continuous version of the model was used for the Phase 2 analysis. If the maximum standardized difference was lower in one model version, then the version with the lower maximum standardized difference was used in the Phase 2 analyses. If some of these conditions were not satisfied for any models considered, then the propensity score estimation was repeated with a different set of covariates. In this case, no statistical tests were conducted in the Phase 2 analysis. The software used for statistical analysis was SAS® Viya® V.03.05 (SAS Institute Inc., Cary, NC, USA).
Results
Patient Disposition
Of the 3,081,923 patients diagnosed with asthma (ICD-10 code: J45 or J46) during the study period recorded in the MDV database, 3,077,778 did not meet the inclusion criteria, and 1218 had a prespecified autoimmune disease. Thus, 2927 patients were included in the FAS. The BIO-initiated group included 239 patients, and the BIO-non-initiated group included 2688 patients (Figure 1). Supplementary Table 1 shows that the total enrolled population was adequately powered for evaluating the primary outcome.
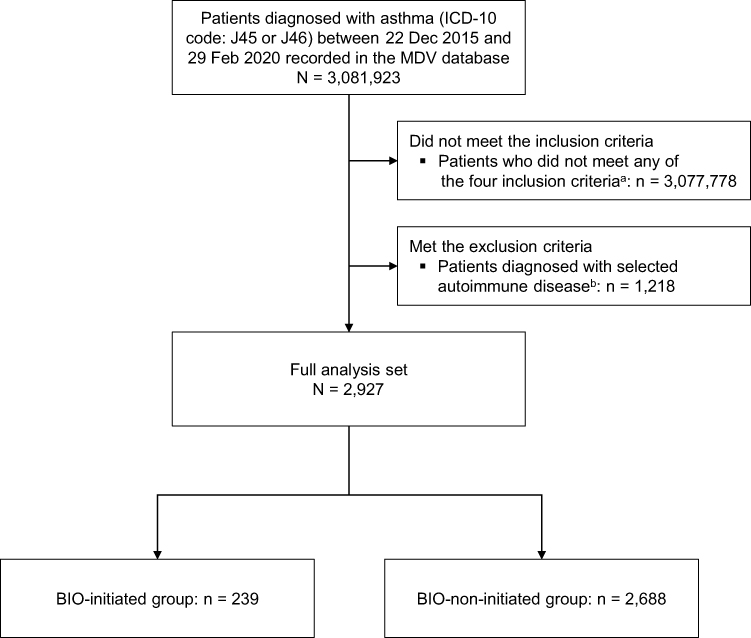 |
Figure 1 Patient disposition. aThe four inclusion criteria were prescription of high-dose inhaled corticosteroids or inhaled corticosteroids/long-acting β2-agonists during the baseline period of 24 weeks before the index date; a record of ≥1 hospital visit during the baseline period, ≥2 hospital visits during the observation period, and ≥1 hospital visit after the observation period; and a total maintenance oral corticosteroid prescription duration ≥12 weeks during the baseline period (including the observation start date); and age ≥16 years at the start of the observation period. bPatients with the following selected autoimmune diseases were excluded: rheumatoid arthritis with rheumatoid factor (ICD-10 code: M05), other rheumatoid arthritis (M06), polyarteritis nodosa and related conditions (M30), lupus erythematosus (L93), systemic lupus erythematosus (M32), Crohn disease (regional enteritis) (K50), ulcerative colitis (K51), other noninfective gastroenteritis and colitis (K52), and nephrotic syndrome with minor glomerular abnormality (N04). Abbreviations: BIO, biologics; ICD, International Statistical Classification of Diseases and Related Health Problems; MDV, Medical Data Vision. |
Patient Characteristics
The mean ± SD ages of patients in the BIO-initiated and BIO-non-initiated groups were 63.9 ± 14.04 and 67.8 ± 14.36 years, of which 61.1% and 51.9% were female, respectively. In the BIO-initiated and BIO-non-initiated groups, respectively, the most common upper or lower airway-related comorbidities during the baseline period were chronic obstructive pulmonary disease (58.6% and 52.2%), allergic rhinitis (57.7% and 44.0%), respiratory infection (29.3% and 27.7%), pneumonia (26.4% and 25.8%), and chronic paranasal sinusitis (24.7% and 12.8%). The most common steroid-related comorbidities during the baseline period were osteoporosis (62.8% and 50.4%), diabetes mellitus (41.0% and 42.7%), and psychiatric disorders (18.8% and 18.5%). Asthma exacerbation-related events included hospitalization due to asthma exacerbation during the baseline period (26.8% and 31.6%), intravenous steroid use (46.9% and 29.0%), and OCS burst (63.2% and 40.7%) (Table 1). The mean ± SD maintenance OCS dose during the baseline period (adjusted by weight of IPTW) was 7.02 ± 5.574 and 6.87 ± 5.964 mg/day in the BIO-initiated and BIO-non-initiated groups, respectively.
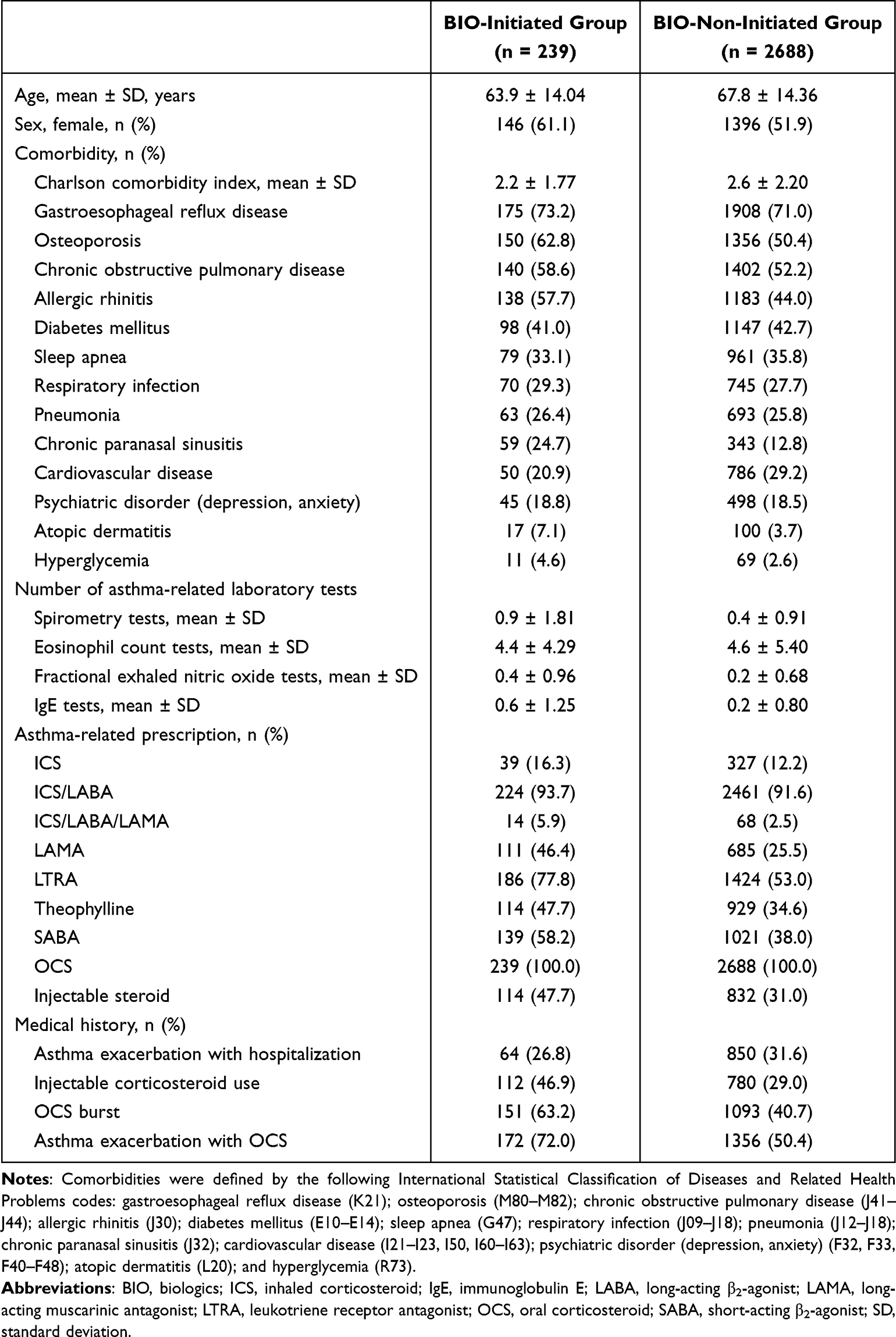 |
Table 1 Background Characteristics of Patients |
Analysis of Propensity Score Estimation
In the first step, which involved propensity score estimating, analyses were made to match the patient background characteristics of the two groups. Spearman correlation coefficients between covariates were calculated. The highest correlation coefficient reported was 0.35 (Supplementary Table 2). The logistic regression analysis for the propensity score model was valid, given that the C-statistic was >0.70 (Supplementary Table 3). When estimating the propensity score, no bias towards any patient characteristic was observed (Supplementary Figure 2).
Balance diagnostics after propensity score estimation investigated whether the adjusted patient characteristics were consistent between the two groups. The results of the weighting of patient characteristics in the two groups are shown in Supplementary Figure 3.
Because the mean standardized differences of some covariates exceeded 0.10 (Supplementary Table 4), and the number of covariates showing a difference >0.10 was smaller in the continuous version, it was decided that a Phase 2 analysis should be conducted to investigate the OCS-sparing effect using the continuous version of the model. The IPTW-adjusted mean standardized difference was 0.15 for asthma exacerbations with hospitalization but <0.1 for other covariates. Therefore, no statistical tests were conducted based on prespecified criteria.
Study Endpoints
Proportion Reduction in the Daily OCS Maintenance Dose from Week 0 to Week 24
Table 2 shows the reduction in the daily maintenance OCS dose at Week 24. The adjusted median (quartile [Q] 1–Q3) proportion reduction in the daily maintenance OCS dose at Week 24 from the index date was 25.0% (0.0–100.0%) in the BIO-initiated group and 0.0% (0.0–83.3%) in the BIO-non-initiated group. The adjusted mean proportion reductions were 22.7% and 20.3% in the BIO-initiated and BIO-non-initiated groups, respectively. The Hodges–Lehmann estimate (95% CI) of the proportion reduction of the daily maintenance OCS dose at Week 24 from the index date in the BIO-initiated group compared with the BIO-non-initiated group after IPTW adjustment was 0.0000% (0.0000%, 0.3365%).
 |
Table 2 Reduction in Daily Maintenance OCS Dose at Week 24 |
Proportions of Patients Who Achieved the Daily Maintenance OCS Dose Reduction from Week 0 to Week 24
Table 3 shows the proportions of patients who achieved a >0%, ≥25%, ≥50%, and 100% reduction in their daily maintenance OCS dose at Week 24. The proportions of patients in the BIO-initiated and BIO-non-initiated groups who achieved dose reductions in the daily maintenance OCS dose at Week 24 from the index date were: >0% reduction in 56.6% and 44.1% (odds ratio [OR] 1.66 [95% CI 1.49, 1.84]), ≥25% reduction in 50.5% and 40.6% (OR 1.49 [95% CI 1.34, 1.65]), ≥50% reduction in 42.8% and 33.7% (OR 1.47 [95% CI 1.32, 1.64]), and 100% reduction in 26.2% and 24.4% (OR 1.10 [95% CI 0.98, 1.24]), respectively.
 |
Table 3 Proportion of Patients Who Achieved a >0%, ≥25%, ≥50%, and 100% Reduction in Their Daily Oral Corticosteroid Maintenance Dose at Week 24 |
Subgroup Analysis of OCS Reduction Stratified by Asthma Exacerbation, the Daily Maintenance OCS Dose, and Type of BIO
When stratified by asthma exacerbation at baseline, OCS reduction tended to be higher in the BIO-initiated group than in the BIO-non-initiated group in patients without exacerbation versus patients with exacerbation (Supplementary Table 5). This trend was not seen in patients without exacerbation (Supplementary Table 5).
As in the full population, the Hodges–Lehmann estimate of the proportion reduction in the daily maintenance OCS dose in the BIO-initiated and BIO-non-initiated groups in patients with a baseline maintenance OCS dose at Week 24 of ≤5 mg/day, >5 mg/day, or ≤10 mg/day was 0.0000%, while that in patients with a baseline maintenance OCS dose of >10 mg/day was 9.3964% (95% CI 0.0000%, 28.0000%) (Supplementary Table 6). The proportions of patients who achieved dose reduction in the daily maintenance OCS dose tended to be higher in the BIO-initiated group than in the BIO-non-initiated group in patients with a dose of >5 mg/day versus patients with a dose of ≤5 mg/day and in the group of patients with a dose of >10 mg/day versus patients with a dose of ≤10 mg/day (Supplementary Table 6). The median (interquartile range [IQR]) proportion reductions in the daily maintenance OCS dose at Week 24 from the index date were 33.3% (0.0%, 85.7%) in the benralizumab/mepolizumab group and 0.0% (0.0%, 90.8%) in the BIO-non-initiated group; the Hodges–Lehmann estimate was 0.0000% (Supplementary Table 7).
Proportion Reduction in the Daily OCS Maintenance Dose from Week 0 to Week 8 and Week 16
The median reduction in maintenance OCS dose from Week 0 to Week 8 from the index date was 0.0% in both groups. The mean ± SD percentages of reduction in maintenance OCS dose in the BIO-initiated and BIO-non-initiated groups were 9.7% ± 105.26% and 17.2% ± 62.97%, respectively, with a median difference of 0.0%. At Week 16, the proportion reduction in the daily maintenance OCS dose tended to be higher in the BIO-initiated group. The median (IQR) proportion reduction was 22.2% (0.0%, 75.0%) in the BIO-initiated group and 0.0% (0.0%, 60.0%) in the BIO-non-initiated group. The Hodges–Lehmann estimate (95% CI) was 0.0225% (0.0000%, 1.1845%) (Supplementary Table 8).
Proportion of Patients with Asthma Exacerbation
The proportions of patients who experienced asthma exacerbation during the 24 weeks from the index date were 53.1% (n = 127) in the BIO-initiated group and 41.2% (n = 1108) in the BIO-non-initiated group. The proportions of patients with asthma exacerbation requiring OCS at baseline were 72.0% (n = 172) in the BIO-initiated group and 57.2% (n = 1537) in the BIO-non-initiated group (Supplementary Table 9).
Discussion
This retrospective cohort study of patients with severe asthma extracted from the DPC database explored whether the maintenance OCS dose would be lower in BIO-initiated patients than in BIO-non-initiated patients in real-world clinical practice in Japan. To the best of our knowledge, no reports in the literature thus far have evaluated OCS dose reduction between patients who have been initiated with BIO treatment and those who have not in real-world clinical practice. Our results show that the OCS dose was reduced by 25.0% after BIO administration. However, the Hodges–Lehmann estimate of the proportion reduction of the daily maintenance OCS dose at Week 24 from the index date in the BIO-initiated group compared with the BIO-non-initiated group after IPTW adjustment was 0.0000%. There was a complete reduction of the OCS dose in 26.2% of the BIO-initiated patients.
It was considered that the sample extracted is representative of a patient population with severe asthma who is receiving maintenance OCS based on the following: the proportion of female patients in the present study (52.79%) was consistent with that in the previous cohort studies of severe asthma patients in Japan (50.6–69.3%), including two studies using the MDV database and the Japanese Medical Data Center Claims database.5,10–12 Regarding respiratory-related comorbidities, many patients in the present study had comorbidities related to the upper and lower respiratory tract, including chronic obstructive pulmonary disease (52.7%), allergic rhinitis (45.1%), pneumonia (25.8%), and chronic paranasal sinusitis (13.7%). These comorbidities were generally consistent with common comorbidities reported in the previous cohort studies using health insurance claim databases.5,12 The high proportion of patients with comorbid chronic obstructive pulmonary disease in this study may reflect both the higher age of patients who visit DPC hospitals in Japan and the broad definition used (including patients with simple chronic bronchitis, unspecified chronic bronchitis, emphysema, and other chronic obstructive pulmonary disease). For the inclusion criteria of maintenance OCS treatment in this study, several patients had comorbidities that can be related to steroid use, including osteoporosis (51.5%), diabetes mellitus (42.5%), psychiatric disorder (depression, anxiety) (18.6%), which is consistent with the findings from previous cohort studies.10–12 In addition, several patients also experienced asthma-related exacerbation events during the baseline period, including OCS burst (42.5%), hospitalization (31.2%), and injectable corticosteroid use (30.5%). Taken together, it can be considered that the patient population in this study was representative of the severe asthma patient population on maintenance OCS treatment.
In this study, the reduction in maintenance OCS doses among BIO-initiated patients tended to be higher in patients without exacerbation during the baseline period. In the BIO-non-initiated group, the proportion of patients who achieved a dose reduction was higher among those with exacerbation than those without during the baseline period. The reduction in maintenance OCS doses also tended to be higher in patients with a baseline dose of >5 mg/day in the BIO-initiated group. In patients with a baseline maintenance OCS dose of >10 mg/day, the median difference in the proportion reduction in maintenance OCS dose was 9.4%, which differed from the 0.0% in the whole population. The proportion reduction in OCS dose tended to be greater in those with a larger baseline OCS dose in the BIO-initiated group. In terms of the proportion of patients who achieved a dose reduction, this tended to be higher in the BIO-initiated group than in the BIO-non-initiated group in patients with an OCS dose >10 mg/day during the baseline period. This study found that higher OCS doses during the baseline period had a greater effect in reducing the OCS dose with BIO, which may have contributed to the reduction of OCS dose with BIO among patients with more severe disease.
At Week 8, no reduction was observed in OCS dose relative to baseline. It is thought that the effect of the BIO was still being ascertained at 8 weeks, and it was too early to see an OCS dose reduction. At Week 16, a difference in the estimated OCS dose reduction between the BIO-initiated group and the BIO-non-initiated group was observed, but the difference was not marked. The same was true for the proportion reduction in dose at Week 24.
At baseline, the proportions of patients who experienced an asthma exacerbation were 72.0% and 57.2% in the BIO-initiated and BIO-non-initiated groups, respectively. During the 24 weeks from the index date, the proportion of patients who experienced an asthma exacerbation was 53.1% in the BIO-initiated group, which is higher than in the BIO-non-initiated group (41.2%). It is likely that the proportion of patients with exacerbations was higher in the BIO-initiated than the BIO-non-initiated group at Week 24 because the proportion of patients with exacerbation at baseline was higher in the BIO-initiated than the BIO-non-initiated group. A similar tendency was also observed for other covariates. In clinical practice, BIOs are likely to be selected for patients with more severe disease. Although this study did not identify whether patients were receiving treatment from specialists, the BIO-initiated group had a higher percentage of patients who had undergone fractional exhaled nitric oxide testing than the BIO-non-initiated group (25.5% vs 10.6%), which suggests that more patients in the BIO-initiated group had received specialist care.
A systematic review of the efficacy and safety of treatment with BIOs concluded that benralizumab, dupilumab, and mepolizumab clearly reduced the daily dose of OCS with a high level of certainty13 based on three randomized studies evaluating the OCS-sparing effect of these BIOs2,6,7 compared with placebo. It has previously been reported that the median reduction in OCS dose with benralizumab at Week 24 in real-world clinical practice in the UK was >50%.14 The maintenance OCS dose with mepolizumab in a Japanese Medical Data Center Claims Database study was decreased from 26% in the 3 months prior to the index date to 16% at the 12-month follow-up,15 indicating that BIOs do contribute to OCS dose reductions.16 Furthermore, mepolizumab led to OCS use reduction among real-world OCS users with severe asthma in the USA (14.7% reduction in the proportion of patients with ≥1 OCS claim from baseline to 12-month follow-up).17 An analysis of the KEIFU study reported that the mean OCS dose was the same 1 year before and after the index date in the BIO-non-initiated group.18
This study has several potential limitations. It should be noted that the study was not randomized. Likely confounding factors were adjusted by using IPTW, but other confounding factors, such as eosinophil counts and fractional exhaled nitric oxide levels, were not included in the database and could not be assessed. The DPC data were collected from hospitals that provide acute care, so further investigation of the study result generalizability is necessary. There was no traceability across medical institutions, and multiple institutions could prescribe OCS, so the prescribed dose of OCS could have been underestimated. It is possible that in some cases, OCSs were administered for diseases other than asthma. There is also a possibility of misclassification due to data definitions within the study. In the case of the definition of OCS prescriptions, in particular, OCS could be used as maintenance therapy (taken continuously) or as needed during asthma exacerbations. However, the database does not contain information that allows us to ascertain the intent behind a prescription. In this study, formal verification of OCS prescriptions was not performed.
The reason for not identifying differences between the BIO-initiated and BIO-non-initiated groups may be that it was difficult to compare these groups due to study limitations. These may include: the 24-week observation period, which may have been too short to assess the effects; non-inclusion of data for variables that may have caused bias as confounding factors (eg, eosinophil counts, lung function, asthma symptoms, non-anti-inflammatory drugs such as long-acting muscarinic antagonists and leukotriene receptor antagonists, as well as other unknown confounders) in the database; and differences in diagnosis distribution due to the lack of randomization. Furthermore, over half of the patients in both groups had comorbid chronic obstructive pulmonary disease, which may have contributed to the results observed. Other possible reasons were that perhaps the OCS dose was not reduced in BIO-initiated patients despite symptoms improving, which may be because clinicians were wary of a patient’s exacerbation history as well as fears associated with OCS withdrawal symptoms, such as steroid-induced adrenal insufficiency. Similarly, physicians might have decided not to initiate BIO because of patient status, such as few symptoms and exacerbation history. As such, the physician may have determined that it was possible to reduce the OCS dose even if the patient did not initiate BIO treatment.
Conclusion
This retrospective database study found that the daily dose of maintenance OCS was reduced with BIO treatment among severe asthma patients. However, no clear difference was observed in OCS dose reduction between the BIO-initiated and BIO-non-initiated groups. The result is partly explained by the finding that the percentage of patients achieving a 100% reduction was similar between the BIO-initiated and BIO-non-initiated groups even though a higher percentage of patients achieved a reduction of ≤75% in the BIO-initiated group compared with the BIO-non-initiated group. Further research with a longer observation period and assessment of variables excluded from consideration in the current study is required.
Abbreviations
BIO, biologics; CI, confidence interval; DPC, Diagnosis Procedure Combination; FAS, full analysis set; ICD, International Statistical Classification of Diseases and Related Health Problems; ICS, inhaled corticosteroid; IL, interleukin; IPTW, inverse probability treatment weighting; IQR, interquartile range; LABA, long-acting β2-agonist; LTRA, leukotriene receptor antagonist; MDV, Medical Data Vision; OCS, oral corticosteroid; OR, odds ratio; Q, quartile; SABA, short-acting β2-agonist; SD, standard deviation.
Data Sharing Statement
Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.
Ethics Approval and Informed Consent
This study was conducted per the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects. The protocol was reviewed and approved (Approval No. 210229) by the Non-Profit Organization MINS Institutional Review Board (Tokyo, Japan). The data for this study were extracted from a commercially available de-identified claims database. According to the Ethical Guidelines above, informed consent is not required for de-identified data.
Acknowledgments
The authors wish to thank Keyra Martinez Dunn, MD of Edanz, Japan, for providing medical writing support, funded by AstraZeneca K.K.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by AstraZeneca K.K., Osaka, Japan. AstraZeneca K.K. participated in the study design, analysis, and interpretation of data, writing the report, and deciding to submit the article for publication. Statistical analyses were entrusted to EPS, an external vendor appointed and funded by AstraZeneca K.K.
Disclosure
Akihiko Tanaka received support for this article from AstraZeneca K.K. and has received payments or honoraria from AstraZeneca K.K., GSK K.K., Sanofi K.K., Kyorin Pharmaceutical Co., Ltd., and Novartis Pharma K.K. Mai Takahashi, Naoyuki Makita, and Naoki Tashiro are employees of and own stock in AstraZeneca K.K. Ayako Fukui, Yoshifumi Arita, and Masakazu Fujiwara are employees of AstraZeneca K.K. The authors report no other conflicts of interest in this work.
References
1. Japanese Society of Allergology Asthma Guideline Committee. Guideline for Prevention and Management of Asthma 2021. Tokyo: Kyowa Kikaku; 2021.
2. Nair P, Wenzel S, Rabe K, et al. Oral glucocorticoid-sparing effect of benralizumab in severe asthma. N Engl J Med. 2017;376(25):2448–2458. doi:10.1056/NEJMoa1703501
3. Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–373. doi:10.1183/09031936.00202013
4. GINA Global initiative for asthma. Global strategy for asthma management and prevention; 2023. Available from: https://ginasthma.org/wp-content/uploads/2023/05/GINA-2023-Full-Report-2023-WMS.pdf.
5. Nagase H, Adachi M, Matsunaga K, et al. Prevalence, disease burden, and treatment reality of patients with severe, uncontrolled asthma in Japan. Allergol Int. 2020;69(1):53–60. doi:10.1016/j.alit.2019.06.003
6. Bel EH, Wenzel SE, Thompson PJ, et al. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. 2014;371(13):1189–1197. doi:10.1056/NEJMoa1403291
7. Rabe K, Nair P, Brusselle G, et al. Efficacy and safety of dupilumab in glucocorticoid-dependent severe asthma. N Engl J Med. 2018;378(26):2475–2485. doi:10.1056/NEJMoa1804093
8. Canonica GW, Rottoli P, Bucca C, et al. Improvement of patient-reported outcomes in severe allergic asthma by omalizumab treatment: the real life observational PROXIMA study. World Allergy Organ J. 2018;11(1):33. doi:10.1186/s40413-018-0214-3
9. Wu P, Han Y, Chen T, Tu XM. Causal inference for Mann-Whitney-Wilcoxon rank sum and other nonparametric statistics. Stat Med. 2014;33(8):1261–1271. doi:10.1002/sim.6026
10. Kimura H, Makita H, Taniguchi N, et al. Determination of the cutoff values of Th2 markers for the prediction of future exacerbation in severe asthma: an analysis from the Hokkaido Severe Asthma Cohort Study. Allergol Int. 2021;70(1):68–73. doi:10.1016/j.alit.2020.09.001
11. Tanosaki T, Kabata H, Matsusaka M, et al. Clinical characteristics of patients with not well-controlled severe asthma in Japan: analysis of the Keio Severe Asthma Research Program in Japanese population (KEIO-SARP) registry. Allergol Int. 2021;70(1):61–67. doi:10.1016/j.alit.2020.06.002
12. To Y, Taguchi Y, Shimazaki T, et al. Real-world treatment and health care resource use among severe asthma patients in Japan. Respir Investig. 2021;59(4):464–477. doi:10.1016/j.resinv.2021.02.010
13. Agache I, Beltran J, Akdis C, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines - recommendations on the use of biologicals in severe asthma. Allergy. 2020;75(5):1023–1042. doi:10.1111/all.14221
14. Kavanagh JE, Hearn AP, Dhariwal J, et al. Real-world effectiveness of benralizumab in severe eosinophilic asthma. Chest. 2021;159(2):496–506. doi:10.1016/j.chest.2020.08.2083
15. Nagase H, Tamaoki J, Suzuki T, et al. Effectiveness of mepolizumab in severe asthma in Japan: a real-world study using claims data. Clin Transl Allergy. 2021;11(8):e12063. doi:10.1002/clt2.12063
16. Kimura Y, Suzukawa M, Inoue N, Imai S, Akazawa M, Matsui H. Real-world benefits of biologics for asthma: exacerbation events and systemic corticosteroid use. World Allergy Organ J. 2021;14(11):100600. doi:10.1016/j.waojou.2021.100600
17. Silver J, Bogart M, Packnett E, Wu J, McMorrow D, Hahn B. Real-world reductions in oral corticosteroid use in the USA following mepolizumab therapy for severe asthma. J Asthma Allergy. 2020;13:689–699. doi:10.2147/JAA.S275944
18. Matsunaga K, Adachi M, Nagase H, Okoba T, Hayashi N, Tohda Y. Association of low-dosage systemic corticosteroid use with disease burden in asthma. NPJ Prim Care Respir Med. 2020;30(1):35. doi:10.1038/s41533-020-00192-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characterization of Patients in the International Severe Asthma Registry with High Steroid Exposure Who Did or Did Not Initiate Biologic Therapy
Chen W, Sadatsafavi M, Tran TN, Murray RB, Wong CBN, Ali N, Ariti C, Garcia Gil E, Newell A, Alacqua M, Al-Ahmad M, Altraja A, Al-Lehebi R, Bhutani M, Bjermer L, Bjerrum AS, Bourdin A, Bulathsinhala L, von Bülow A, Busby J, Canonica GW, Carter V, Christoff GC, Cosio BG, Costello RW, FitzGerald JM, Fonseca JA, Yoo KH, Heaney LG, Heffler E, Hew M, Hilberg O, Hoyte F, Iwanaga T, Jackson DJ, Jones RC, Koh MS, Kuna P, Larenas-Linnemann D, Lehmann S, Lehtimäki LA, Lyu J, Mahboub B, Maspero J, Menzies-Gow AN, Sirena C, Papadopoulos N, Papaioannou AI, Pérez de Llano L, Perng DW, Peters M, Pfeffer PE, Porsbjerg CM, Popov TA, Rhee CK, Salvi S, Taillé C, Taube C, Torres-Duque CA, Ulrik CS, Ra SW, Wang E, Wechsler ME, Price DB
Journal of Asthma and Allergy 2022, 15:1491-1510
Published Date: 21 October 2022
The Effect of Biologic Therapy in Severe Asthmatics and ER Admissions During COVID-19: A Retrospective Study
Cleland D, Arias C, Alismail A, Daher N, Leeper L, Casillas P, Tan LD
Journal of Asthma and Allergy 2023, 16:833-837
Published Date: 10 August 2023
Adult Severe Asthma Registries: A Global and Growing Inventory
Cushen B, Koh MS, Tran TN, Martin N, Murray R, Uthaman T, Goh CYY, Vella R, Eleangovan N, Bulathsinhala L, Maspero JF, Peters MJ, Schleich F, Pitrez P, Christoff G, Sadatsafavi M, Torres-Duque CA, Porsbjerg C, Altraja A, Lehtimäki L, Bourdin A, Taube C, Papadopoulos NG, Zsuzsanna C, Björnsdóttir U, Salvi S, Heffler E, Iwanaga T, al-Ahmad M, Larenas-Linnemann D, van Boven JF, Aarli BB, Kuna P, Loureiro CC, Al-lehebi R, Lee JH, Marina N, Bjermer L, Sheu CC, Mahboub B, Busby J, Menzies-Gow A, Wang E, Price DB
Pragmatic and Observational Research 2023, 14:127-147
Published Date: 20 October 2023
Multiple Biologics for Multiple T2 Diseases: A Pharmacoepidemiological Algorithm for Sorting Out Patients by Indication
Charriot J, Descamps V, Jankowski R, Maravic M, Bourdin A
Journal of Asthma and Allergy 2023, 16:1287-1295
Published Date: 29 November 2023
Real-World Biologic Use Patterns in Severe Asthma, 2015–2021: The CLEAR Study
Tran TN, Chen S, Emmanuel B, Altraja A, Bourdin A, Sheu CC, Tsai MJ, Hoyte FC, Quinton A, Cook B, Bulathsinhala L, Henley W, Goh CYY, Liu Y, Ariti C, Carter V, Price DB
Pragmatic and Observational Research 2025, 16:51-66
Published Date: 18 March 2025