Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Optimizing Xenograft Models for Breast Cancer: A Comparative Analysis of Cell-Derived and Patient-Derived Implantation Techniques in Pre-Clinical Research
Authors Khairani AF ![]() , Harmonia S, Chou Y
, Harmonia S, Chou Y ![]() , Alfarafisa NM
, Alfarafisa NM ![]() , Ramadhanti J
, Ramadhanti J ![]()
Received 7 August 2024
Accepted for publication 19 November 2024
Published 9 January 2025 Volume 2025:17 Pages 1—10
DOI https://doi.org/10.2147/BCTT.S490532
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert Clarke
Astrid Feinisa Khairani,1– 3 Shella Harmonia,2 Yoan Chou,3 Nayla Majeda Alfarafisa,1,2 Julia Ramadhanti1,2
1Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia; 2Undergraduate Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia; 3Graduate School of Master Program in Anti Aging and Aesthetic Medicine, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Astrid Feinisa Khairani, Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Jalan Ir. Soekarno KM.21, Jatinangor, Sumedang, West Java, 45363, Indonesia, Email [email protected]
Purpose: The high mortality rate of breast cancer motivates researchers to search for effective treatments. Due to their ability to simulate human conditions, xenograft models such as CDX (Cell line-Derived Xenografts) and PDX (Patient-Derived Xenografts) have gained popularity in pre-clinical research. The choice of xenograft technique is influenced by the type of tumor employed, particularly in more aggressive tumor models like TNBC with metastases. Subcutaneous or orthotopic implantation may influence tumor engraftment rates and the applicability of the models for drug testing. To optimize xenograft models and support the development of breast cancer drugs, selecting a suitable transplantation technique is essential to attaining the best results.
Methods: This scoping review used PRISMA-Scr methodology to summarize findings from eleven articles published between 2012 and 2024 on pre-clinical trials related to xenograft models for breast cancer considering PDX began traction after 2010. Using specific criteria, the review included studies from electronic platforms. The inclusion criteria ensured relevant English sources were available in full text, while the exclusion criteria eliminated certain types of articles and inadequately comprehensive studies.
Results: Subcutaneous and orthotopic implantation are critical methods for xenograft models in cancer research. Subcutaneous implantation is less invasive and more manageable but does not fully mimic the tumor’s natural environment. Orthotopic implantation accurately mimic the migration, invasion, and molecular characteristics of the original tumor, although the procedure is more complex and requires specialized techniques. The specific research objectives determine their choice, the need for accurate tumor replication, and the testing convenience.
Conclusion: Orthotopic implantation is the preferable method for developing PDX and CDX models of breast cancer because it closely mimics the tumor microenvironment and metastatic behavior, yielding clinically relevant results for drug testing. Subcutaneous implantation may result in higher engraftment rates, but it cannot accurately represent the complexity of tumors.
Keywords: breast cancer, implantation, orthotopic, subcutaneous, xenograft
Introduction
Breast cancer, which has been labeled one of the most common cancers diagnosed over the past five years, has garnered significant attention from researchers worldwide. With over 2 million women confirmed to have been affected by breast cancer, the mortality rate is alarmingly high, accounting for 684,996 deaths at a rate of 13.6 per 100,000 age-adjusted cases in 2020.1,2 Consequently, breast cancer has emerged as the leading cancer type with a notably poor life expectancy on a global scale.
Researchers have used various techniques and strategies for over forty years to construct a picture of the pre-clinical model of trial animals, primarily mice, in vitro and in vivo, intending to come as near the original as possible.3 In addition, drug efficacy and new treatment research on breast cancer still need to be sought. Therefore, the use of xenograft method in the pre-clinical model has become widely chosen by researchers. This is because pre-clinical models, xenograft especially, may simulate the conditions before human testing.4 The most popular xenograft models utilized and have significantly contributed to breast cancer research in the previous two or three decades are cell line-derived xenografts (CDX) and patient-derived xenografts (PDX). CDX models result from the implantation of cancer cell lines into immunodeficient mice.
Meanwhile, PDX models result from implanting original tumor cells or tissue into immunodeficient mice, with human cancer’s biological characteristics and microenvironments recreated.5 In general, preclinical assessment of therapeutic approaches, biomarker discovery, drug screening and treatment, and cancer research have all come to rely on PDX models. Several institutes, such as the National Cancer Institute in 2019 and the European Molecular Biology Laboratory and the Jackson Laboratory in 2023 have even amassed libraries of PDX and CDX models recently. This demonstrates that despite introducing new techniques like organoids/3D culture output, both approaches are still applicable and being improved.6
During the xenograft model procedure for CDX and PDX, both have limits. Genetic drift, poor tumour heterogeneity, and occasionally low clinical relevance due to the CDX model’s inability to replicate the natural tumour environment are all common. In addition, the PDX model uses immunocompromised mice, which limits its ability to replicate the immune system of a normal human accurately, and it has time and financial constraints.7,8 Researchers also have the option to either subcutaneously implant or inject the tumor into the skin or orthotopically into the inguinal or thoracic mammary fat pad.9 In numerous studies, significant research indicates that the choice of implantation site significantly impacts the engraftment results of breast tumors in both CDX and PDX models.10 The benefit of subcutaneous implantation is that tumor size can be readily monitored, allowing for rapid drug efficacy validation. However, there is concern that the subcutaneous microenvironment may differ from the tissue of origin for most tumor types, potentially limiting the accurate representation of human cancer complexity in PDXs.
Furthermore, the subcutaneous approach demonstrates variations in vascularization and a less suitable metastasis tendency than the tumor’s origin, which can lead to occasionally incompletely representative outcomes.11 Conversely, orthotopic implantation tends to lead to tumor metastasis in a manner consistent with corresponding human tumors, thereby creating more clinically relevant models. More substantial growth, larger tumour size, and improved re-transplantation rates were observed in orthotopically implanted PDX tumours.10
Over a decade, researchers decided to use the orthotopic technique, while others chose the subcutaneous method due to existing considerations and developed a more relevant clinical model. To boost productivity and save expenses, some researchers in fact employ alternative techniques like organoids or 3D culturing. It is nevertheless thought to be less accurate in describing actual tumors, particularly if metastasis is desired, because this method does not use the immune system or vascularization that occurs in humans. Because the CDX and PDX approaches use living organisms that can be tuned to be as close as feasible to the state of actual human tumors, the comparison between them becomes more meaningful.12 Since achieving the best results from the xenograft method may involve variations in technique despite a similar main concept and protocol, one crucial factor is how the tumor is implanted. This article presents a comparative analysis of orthotopic and subcutaneous implantation methods for CDX and PDX models in breast cancer research. By summarizing the models that employed these methods for drug testing, we aim to assist researchers in selecting the most suitable transplantation technique that optimizes the xenograft mouse model and supports future breast cancer drug development.
Methods
This study used the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Review (PRISMA-Scr) to conduct a scoping review.13 The summary of the articles’ findings will be presented in Tables 1–3. Sources of information and literature used in this study were located through electronic platforms, namely Medline Database, PubMed, and Elsevier, with keywords ((breast cancer OR breast tumor) AND (xenograft OR PDX OR CDX OR patient-derived OR cell-derived) AND (mouse model OR mice). The inclusion criteria of this study were in line with the source’s title, keywords, and abstract; sources in English, references can be read in full text, and not only containing an abstract or short summary. The time frame (2012–2024) was also selected because, after more varied implantation techniques were introduced, research on PDX began to gain traction after 2010, and studies that draw comparisons between CDX and PDX have grown in quantity and significance over the past ten years. The exclusion criteria of this study are article letter to editor type, internet-accessible material that has not been adequately published in a journal article or conference proceedings, and not mentioning the number of xenograft lines/samples used in the pre-clinical trial or engraftment rate/tumor growth rate. Ultimately, eleven articles published between 2012 and 2024, which described pre-clinical trials, were carefully evaluated.
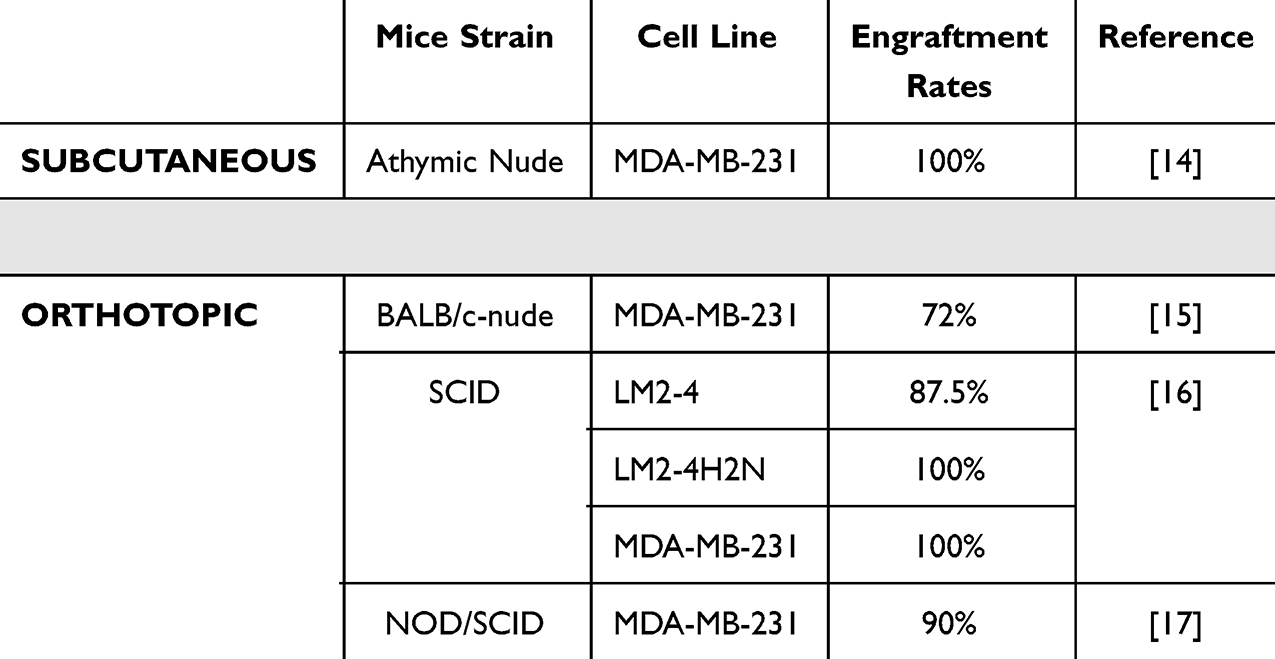 |
Table 1 Model Used in Subcutaneous and Orthotopic CDX |
 |
Table 2 Model Used in Subcutaneous and Orthotopic PDX |
 |
Table 3 Drug Testing with Subcutaneous and Orthotopic Implantation |
Results
Xenograft Transplantation Model
Cell-Derived Xenograft
CDX is one of the most basic and widely used model systems because it involves grafting human cell lines into immunosuppressed animals. These have been very helpful for assessing the genetics, biological processes, and, to some extent, the potential for metastasis of breast cancer; nevertheless, they are constrained by the reduced intra-tumor heterogeneity and the poor track record of predicting clinically successful therapy.23
Because of the rapidity and repeatability of tumor development, transplantable cell lines are appealing for therapy research. CDX models have the benefit of being easier to generate and more reproducible because they use a well-established cancer cell line that has been described and verified. Additionally, CDX models are simpler to modify in the lab, enabling scientists to investigate the impact of particular genetic changes on the behavior of cancer. The use of the CDX model depends on the study’s objectives and the unique research issue. In the CDX model, tumor heterogeneity and lineage hierarchy are vulnerable to loss. As a result, the PDX model may be preferred when researchers want to keep the human stromal components and maintain the tumor architecture related to breast cancer23,24 (Figure 1).
 |
Figure 1 Process of Tumor Implantation in cell line-derived xenografts (CDX) and patient-derived xenografts (PDX) Model. |
Patient-Derived Xenograft
Patient-derived Xenograft (PDX) animal models are created by the direct transplantation of patient-derived tumor pieces into immunocompromised mice. In brief, bits of tumors or single-cell are extracted from tumor tissues obtained through surgery or biopsy and implanted under the skin (subcutaneous transplantation), in the organ as the original tumors in the patients (orthotopic transplantation), or the renal capsule of the immunocompromised recipient mouse.24 When using PDX, tumor fragments may be implanted immediately without first being cultured following tissue collection from the patient. Instead, tumor fragments should be cut into 2–3 mm3 pieces for simpler transplanting25 (Figure 1).
The procedure is relatively simple and involves acquiring fresh surgical tissue, sectioning it into pieces no larger than three mm3, and then implanting the pieces either subcutaneously or orthotopically into the flank of an immunocompromised mouse or rat. The generation containing the patient-derived material is known as F0, and the generations after it are numbered sequentially (F1, F2, F3, etc).; at the same time, other groups have given these names instead, such as G0, G1, and so on. The period necessary for tumor “take” varies depending on tumor type, implantation site, and recipient strain. Still, in general, it is between 2 and 4 months, with failure of engraftment not being determined until at least 6 months. Pharmacological therapy may be expanded to the third generation (F3 or G3), and most organizations employ early passages for such investigations. The primary factor, however, should be how far the PDX has diverged from the patient’s tumor regarding genetics and histology.26
Implantation Site
Subcutaneous
Subcutaneous implantation entails injecting or placing tumor cells or tissue fragments into the dorsal flanks of the mouse model, precisely at the junction of the skin and muscles.9,10 The subcutaneous approach is easier to manage and less invasive, so the mouse model experiences less pain during surgery. With the minimally invasive method, surgery wounds can even heal rapidly. As a result, this method explains why, generally, in some cases, the subcutaneous method has a reasonably high success rate.9,27 Despite its advantages, there is a valid concern that the subcutaneous method may not accurately replicate the original microenvironment of the tumor when compared to the orthotopic technique.27
Subcutaneous xenograft is a more suitable method for investigating tumor development, as it facilitates easier tracking of changes, such as monitoring the volume of tumors on the skin’s surface. Additionally, due to its convenience and swift implementation, subcutaneous implantation is recommended for quickly generating multiple PDX mouse models.28 To assess tumor growth, researchers typically employ a digital caliper to measure the length and width of the tumor. Using the volume ellipsoid formula  mass estimation is quantified.29 While measuring the tumor’s height may present challenges, tracking its length and width still provides a reliable means of assessing tumor growth with greater ease.
mass estimation is quantified.29 While measuring the tumor’s height may present challenges, tracking its length and width still provides a reliable means of assessing tumor growth with greater ease.
Orthotopic
Orthotopic implantation emerges as the most optimal method for tumor transplantation, offering the flexibility to implant in the thoracic or inguinal mammary fat pads. This technique allows for the utilization of either tumor cells or tissue fragments as transplants. However, tissue fragments are particularly recommended, as they localize the tumor at the original cancer’s primary site, resulting in a higher degree of histopathological and molecular similarities to the original tumor.10 Consequently, the disease development process modeled by this method yields outcomes that closely resemble those seen in humans, making it highly valuable for medication development, especially in the context of breast cancer.9
The orthotopic method may enhance the lack of a subcutaneous method in investigating breast cancer metastasis. It can ultimately increase engraftment rates in the mouse model via migration and invasion to other organs.9 In contrast, orthotopic modeling demands a trained surgical technique for obtaining tissue fragments and developing an appropriate PDX model so that sometimes the succession rate is better in the subcutaneous method. In contrast with the subcutaneous method, a digital caliper cannot be used to measure the mass of tumors or monitor tumor growth results. Therefore, it needs the most advanced imaging technologies, such as computed tomography (CT), magnetic resonance imaging (MRI), optical imaging (OI), positron emission tomography (PET), and ultrasonography (USG), to visualize and estimate the growth of tumors.9,30
Impact of Implantation Site: Engraftment and Characteristic
The factors influencing the engraftment rate are not limited to the tumor’s implantation site. However, the implantation site is still a significant factor, as it can provide numerous considerations for researchers who wish to achieve specific objectives when developing xenograft models.30 Tumor tissue is considered engrafted if it has been successfully detected macroscopically during physical and histological analysis using a formula or technology based on the implantation technique. A high level of engraftment is necessary, but the microenvironment must be as similar as feasible to that of the original tumor.31
The models of CDX and PDX used for subcutaneous and orthotopic implantation are displayed in Tables 1 and 2. In CDX, mice implanted by subcutaneous method have high engraftment rates in total (100%).32 Conversely, the orthotopic method has reduced engraftment rates that are not statistically significant.: 72%; 87.5%; 90%.15,16,19 It also possible for orthotopic in CDX model to have 100% engraftment rates16 when using different cell lines. PDX also produced a similar output model. The subcutaneous method also yields results with higher engraftment rates, the lowest being 15%,18 while the results with a percentage of more than 50% million were successfully obtained (53%; 60%; 65%; 80%).20
In percentage terms, subcutaneous implants have a higher engraftment success rate than orthotopic implants. This is since the orthotopic method is typically more complicated and requires qualified surgical techniques to transplant specific organs, whereas the subcutaneous process has a more accessible area for implantation.20,32 The subcutaneous location also allows researchers to see and measure the exact location of tumor growth, allowing for earlier initial screening to determine successful engraftment.30 However, despite being easier to observe, the activity and volume of tumor engraftment measured subcutaneously are likely to be smaller than when measured orthotopically.33
Tumor type also influences the results of xenograft engraftment. ER(+) tumours have been observed to be less likely to engraft than TNBC. ER(+) tumours need around six times longer than TNBC tumours to reach a palpable size which indicates that aggressive tumors have a tendency to be transplanted more quickly, especially if supported by the orthotopic method.10 As additional information, the spread of triple-negative breast cancer is associated with elevated recurrence rates in visceral organs and soft tissue, nonetheless, decreased rates in bone. This can help researchers to choose the right method to see which metastases they want to study according to the research objectives.16
The subcutaneous technique has a high engraftment rate but cannot replicate the microenvironment of the original human tumor. In the first passage, implantation does not demonstrate significant variations in the microenvironment; however, in the subsequent passage, the stromal component and metastasis pattern deviate more and more from the original tumor state.34 On the other side, orthotopic tumors exhibit a more aggressive and malignant growth pattern than subcutaneous tumors. This is because the engraftment process in the orthotopic model corresponds to the original tumor’s behavior before transplantation.33 This demonstrates that every technique has benefits and drawbacks of its own. The subcutaneous technique is worth considering if researchers are looking for a quick method, need a high engraftment rate, and are interested in studying tumor types other than metastatic ones. While the orthotopic method may require more talent, it is an essential option if researchers frequently employ tumors with metastases due to its advantages, which better depict the original tumor environment.
The Relevance of Drug Testing and Clinical Situation Based on Implantation Site
The primary objective in developing xenograft models is to assess the effectiveness of breast cancer-related medications. Numerous studies have indicated that the sensitivity of therapeutic responses is comparable in these models. In Table 3, researchers have documented drug trials using both subcutaneous and orthotopic transplantation techniques. For instance, the paclitaxel trial showed similar resistance levels when administered through subcutaneous and orthotopic methods, which bears clinical relevance for patients exhibiting resistance to triple-negative therapy.20,22 In subcutaneous, Idasanutlin that response greatly in breast cancer with positive estrogen receptor, is needed in 15 µM to inhibit 50% biochemical and biological functions (IC30 = 15 µM).20 Tamoxifen has great sensitivity to the tumor model and only need 0.012 µM to inhibit half of the biological response.20 For the orthotopic method, the use of docetaxel gave <30% regression of the tumor, means that in both clinical and pre-clinical this method also give similar result.33 However, despite this similarity in therapeutic response and sensitivity, there are still notable distinctions between the two methods that researchers must carefully consider while determining the purpose of drug testing.35
The therapeutic response will be affected by the dimension of the tumor resulting from both transplantation techniques.36 In the initial phase, both methods may lead to the development of gradually spreading and metastatic tumors with comparable dimensions. However, it is observed that in the subcutaneous model, metastasis may occur in a different location than that of the primary tumor. In contrast, orthotopic tumors generally exhibit a more remarkable ability to retain their original location and behavior.37 As a result, orthotopic implantation tends to yield more relevant and accurate results compared to the subcutaneous approach.
The implantation site also affects drug concentrations in the mouse model. The orthotopic experiment of doxorubicin and cyclophosphamide revealed that orthotopic tumors contained higher doxorubicin concentrations than subcutaneous tumors. This is likely due to the subcutaneous impact of the microenvironment, where lymph node and blood vessel malformations cause the stroma to solidify and become rigid.35
The condition of the immune system, a part of the tumor’s microenvironment, is a further factor. This condition will improve the model’s ability to respond to therapy. Lymphocytes are present in the tumor stroma for both transplantation procedures. This type of situation is known to be beneficial for immunotherapy research. This demonstrates that both transplantation methods are relevant for conducting drug trials.36,37 Although this, evidence suggests that the orthotopic microenvironment is more comparable to the original tumor state, particularly regarding metastases. The orthotopic method can be used to produce even more relevant outcomes. In contrast, the subcutaneous procedure typically tends to be more effective for testing drugs derived from the primary tumor than metastases.
In comparing the subcutaneous and orthotopic techniques, it is evident that the subcutaneous approach lacks the natural tumour microenvironment of the originating organ, which ultimately influences tumour behaviour and its response to pharmacological therapies.6,10,15 This strategy also restricts researchers from further investigating tumour metastasis, as it spreads may not correspond with the spread of the original tumour.38 This frequently results in a bias in pharmacological response research. Conversely, the orthotopic method addresses the limitations of subcutaneous techniques by more accurately replicating the tumour microenvironment. Nonetheless, it necessitates proficient surgical skills to effectively transplant the tumour. Consequently, the success rate is observed to be diminished in this procedure due to the increased complexity of the transplanting.10 Biases with the measurement of tumour growth in orthotopic models must also be acknowledged, particularly as the transplant’s position within a specific organ necessitates sophisticated technology for precise assessment of tumour development.7 Furthermore, the utilisation of mouse models warrants careful consideration, as it may provide a double-edged sword; employing immunocompromised mouse models can diminish the applicability of the immunological status observed in actual humans.39
Future Considerations
Alongside the success rates of the previously mentioned studies, each also has various limitations. To enhance the quality and efficacy of xenografts, the following considerations may be explored in future studies to attain more ideal outcomes. Many studies acknowledge the presumption that the model may not closely resemble an actual microenvironment. Consequently, researchers must enhance the prediction efficacy of genomic and transcriptome indicators. Screening for responses to traditional cytotoxic and alternative-target agents can be conducted, and innovative combination strategies may be suggested, either by enhancing similarity to the microenvironment or by altering the mouse model to reflect immunocompromised conditions comparable to human circumstances.19 Furthermore, concerning tumors with metastases, non-invasive imaging can evaluate the spatiotemporal dynamics of metastasis formation, addressing significant limitations of sole endpoint studies and facilitating precise randomization of animal cohorts for treatment outcome investigation. The outlined tumor models of spontaneous metastasis and the imaging toolkit can evaluate the effectiveness of novel therapeutic regimens for metastatic breast cancer.31 Comprehensive bioinformatics and network analysis of transcriptome and proteomic data from human malignancies may uncover metastatic routes, therapeutic targets, and prospective biomarkers. Multidisciplinary research indicates that the strength and accuracy of these systems in predicting clinical outcomes are enhanced when integrated with other molecular biology and bioinformatics tools.18 There should be pertinent biological factors underlying PDX treatment resistance that can be leveraged to improve clinical treatment.20
Conclusion
In conclusion, for the development of PDX and CDX models of breast cancer, due to its wider heterogeneity, more predictive power, and greater relevance to clinical settings, the PDX approach seems to have been studied more thoroughly than CDX. Orthotopic implantation emerges as the preferred technique. This method closely replicates the tumor microenvironment and metastatic behavior, resulting in clinically relevant outcomes for drug testing. However, it requires surgical expertise and advanced imaging technologies to monitor tumor growth. On the other hand, subcutaneous implantation yields higher engraftment rates, which are suitable for research such as initial screening or testing of medications targeting primary tumors. Furthermore, this method works better in facilities with limited resources and novice technicians.
Researchers must carefully assess their research objectives and model characteristics when choosing the implantation site to optimize the use of PDX and CDX models for breast cancer research and drug development. The advantages and disadvantages of each method should thoughtfully be weighed to ensure the clinical relevance and applicability of the findings.
Funding
This work was supported by an Internal Grant (No. 1662/UN6.3.1/PT.00/2024) from Universitas Padjadjaran, West Java, Indonesia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Williams AD, Bleicher RJ, Ciocca RM. Breast cancer risk, screening, and prevalence among sexual minority women: an analysis of the national health interview survey. LGBT Health. 2020;7(2):109–118. doi:10.1089/lgbt.2019.0274
2. Global Cancer Observatory. Cancer Today. Available from: https://gco.iarc.fr/today/home.
3. Everitt JI. The future of preclinical animal models in pharmaceutical discovery and development: a need to bring in cerebro to the in vivo discussions. Toxicol Pathol. 2015;43(1):70–77. doi:10.1177/0192623314555162
4. Murayama T, Gotoh N. Patient-derived xenograft models of breast cancer and their application. Cells. 2019;8(6):621. doi:10.3390/cells8060621
5. Tsumura R, Koga Y, Hamada A, et al. Report of the use of patient-derived xenograft models in the development of anticancer drugs in Japan. Cancer Sci. 2020;111(9):3386–3394. doi:10.1111/cas.14564
6. Jin J, Yoshimura K, Sewastjanow-Silva M, et al. Challenges and prospects of patient-derived xenografts for cancer research. Cancers. 2023;15(17):4352. doi:10.3390/cancers15174352
7. Liu Y, Wu W, Cai C, et al. Patient-derived xenograft models in cancer therapy: technologies and applications. Signal Transduct Target Ther. 2023;8(1). doi:10.1038/s41392-023-01419-2
8. Souto EP, Dobrolecki LE, Villanueva H, Sikora AG, Lewis MT. In vivo modeling of human breast cancer using cell line and patient-derived xenografts. J Mammary Gland Biol Neoplasia. 2022;27(2):211–230. doi:10.1007/s10911-022-09520-y
9. Onaciu A, Munteanu R, Munteanu VC, et al. Spontaneous and induced animal models for cancer research. Diagnostics. 2020;10(9):660. doi:10.3390/diagnostics10090660
10. Okano M, Oshi M, Butash A, et al. Orthotopic implantation achieves better engraftment and faster growth than subcutaneous implantation in breast cancer patient-derived xenografts. J Mammary Gland Biol Neoplasia. 2020;25(1):27–36. doi:10.1007/s10911-020-09442-7
11. Sheng Y, Qian W, Guo S. Impact of orthotopic versus subcutaneous implantation on patient-derived xenograft transcriptomic profile. Eur J Cancer. 2022;174:S9. doi:10.1016/S0959-8049(22)00825-5
12. Bleijs M, Van De Wetering M, Clevers H, Drost J. Xenograft and organoid model systems in cancer research. EMBO J. 2019;38(15). doi:10.15252/embj.2019101654
13. Chapter 11: scoping reviews. In: JBI Manual for Evidence Synthesis; 2020. doi:10.46658/jbimes-20-12
14. Binnewies M, Roberts EW, Kersten K, et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nature Med. 2018;24(5):541–550. doi:10.1038/s41591-018-0014-x
15. Yen TH, Da LG, Chai JW, et al. Characterization of a murine xenograft model for contrast agent development in breast lesion malignancy assessment. J Biomed Sci. 2016;23(1):1–13. doi:10.1186/S12929-016-0261-4/TABLES/2
16. Lim HK, Lee H, Moon A, Kang KT, Jung J. Exploring protocol for breast cancer xenograft model using endothelial colony-forming cells. Transl Cancer Res. 2018;7(5):1228–1234. doi:10.21037/TCR.2018.09.09
17. Yen TH, Lee GD, Chai JW, et al. Characterization of a murine xenograft model for contrast agent development in breast lesion malignancy assessment. J Biomed Sci. 2016;23(1):46. doi:10.1186/s12929-016-0261-4
18. Lefley D, Howard F, Arshad F, et al. Development of clinically relevant in vivo metastasis models using human bone discs and breast cancer patient-derived xenografts. Breast Cancer Res. 2019;21(1). doi:10.1186/s13058-019-1220-2
19. Fricke IB, De Souza R, Ayub LC, et al. Spatiotemporal assessment of spontaneous metastasis formation using multimodal in vivo imaging in HER2+ and triple negative metastatic breast cancer xenograft models in mice. PLoS One. 2018;13(5):e0196892. doi:10.1371/journal.pone.0196892
20. Kanaya N, Somlo G, Wu J, et al. Characterization of patient-derived tumor xenografts (PDXs) as models for estrogen receptor positive (ER+HER2− and ER+HER2+) breast cancers. J Steroid Biochem Mol Biol. 2017;170:65–74. doi:10.1016/j.jsbmb.2016.05.001
21. Eyre R, Alférez DG, Spence K, et al. Patient-derived mammosphere and xenograft tumour initiation correlates with progression to metastasis. J Mammary Gland Biol Neoplasia. 2016;21(3–4):99–109. doi:10.1007/s10911-016-9361-8
22. Menezes ME, Shen XN, Das SK, et al. MDA-7/IL-24 functions as a tumor suppressor gene in vivo in transgenic mouse models of breast cancer. Oncotarget. 2015;6(35):36928–36942. doi:10.18632/ONCOTARGET.6047
23. Holen I, Speirs V, Morrissey B, Blyth K. In vivo models in breast cancer research: progress, challenges and future directions. DMM Dis Models Mech. 2017;10(4):359–371. doi:10.1242/dmm.028274
24. Dranoff G. Experimental mouse tumour models: what can be learnt about human cancer immunology? Nat Rev Immunol. 2012;12(1):61–66. doi:10.1038/nri3129
25. Yada E, Wada S, Yoshida S, Sasada T. Use of patient-derived xenograft mouse models in cancer research and treatment. Future Sci OA. 2018;4(3). doi:10.4155/fsoa-2017-0136
26. Jung J, Seol HS, Chang S. The generation and application of patient-derived xenograft model for cancer research. Cancer Res Treat. 2018;50(1):1–10. doi:10.4143/crt.2017.307
27. Tentler JJ, Tan AC, Weekes CD, et al. Patient-derived tumour xenografts as models for oncology drug development. Nat Rev Clin Oncol. 2012;9(6):338–350. doi:10.1038/nrclinonc.2012.61
28. Schmidt KM, Geissler EK, Lang SA. Subcutaneous murine xenograft models: a critical tool for studying human tumor growth and angiogenesis in vivo. Methods Mol Biol. 2016;1464:129–137. doi:10.1007/978-1-4939-3999-2_12
29. Singhal SS, Garg R, Mohanty A, et al. Recent advancement in breast cancer research: insights from model organisms—mouse models to zebrafish. Cancers. 2023;15(11):2961. doi:10.3390/CANCERS15112961
30. Tomayko MM, Reynolds CP. Determination of subcutaneous tumor size in athymic (nude) mice. Cancer Chemother Pharmacol. 1989;24(3):148–154. doi:10.1007/BF00300234
31. Zeng M, Ruan Z, Tang J, et al. Generation, evolution, interfering factors, applications, and challenges of patient-derived xenograft models in immunodeficient mice. Cancer Cell Int. 2023;23(1):1–23. doi:10.1186/S12935-023-02953-3
32. Beckhove P, Schütz F, Diel IJ, et al. Efficient engraftment of human primary breast cancer transplants in nonconditioned NOD/Scid mice. Int J Cancer. 2003;105(4):444–453. doi:10.1002/IJC.11125
33. Valta M, Ylä-Pelto J, Lan Y, et al. Critical evaluation of the subcutaneous engraftments of hormone naïve primary prostate cancer. Transl Androlo Urol. 2020;9(3):1120134–1121134. doi:10.21037/TAU.2020.03.38
34. Zhang Y, Zhang GL, Sun X, et al. Establishment of a murine breast tumor model by subcutaneous or orthotopic implantation. Oncol Lett. 2018;15(5):6233–6240. doi:10.3892/OL.2018.8113/DOWNLOAD
35. Zhang X, Claerhout S, Prat A, et al. A renewable tissue resource of phenotypically stable, biologically and ethnically diverse, patient-derived human breast cancer xenograft models. Cancer Res. 2013;73(15):4885–4897. doi:10.1158/0008-5472.CAN-12-4081
36. Santana-Krímskaya SE, Kawas JR, Zarate-Triviño DG, Ramos-Zayas Y, Rodríguez-Padilla C, Franco-Molina MA. Orthotopic and heterotopic triple negative breast cancer preclinical murine models: a tumor microenvironment comparative. Res Veterinary Sci. 2022;152:364–371. doi:10.1016/J.RVSC.2022.08.026
37. Arciero CA, Styblo TM. Clinically established prognostic factors in breast cancer. Breast. 2018;250–257.e3. doi:10.1016/B978-0-323-35955-9.00018-0
38. Bibby MC. Orthotopic models of cancer for preclinical drug evaluation: advantages and disadvantages. Eur J Cancer. 2004;40(6):852–857. doi:10.1016/J.EJCA.2003.11.021
39. Pedroza DA, Gao Y, Zhang XHF, Rosen JM. Leveraging preclinical models of metastatic breast cancer. Biochim Biophys Acta - Rev Cancer. 2024;1879(5):189163. doi:10.1016/j.bbcan.2024.189163
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Trastuzumab-Conjugated Nanoliposomes for Targeted Capecitabine Delivery to Suppress HER2-Positive Breast Tumor: Efficacy Analysis in NOD SCID Mice Xenografts
Das S, Satapathy BS, Rahamathulla M, Alhamhoom Y, Pattanaik S, Chawla S, Pattnaik G, Rath D, Ahmed MM, Pasha I
International Journal of Nanomedicine 2026, 21:618476
Published Date: 30 June 2026