Back to Journals » Drug Design, Development and Therapy » Volume 19
Optimizing Venlafaxine Therapy in Pregnancy: A Maternal–Fetal PBPK Modeling Approach
Authors Choi SY, Yang E, Shin KH ![]()
Received 15 July 2025
Accepted for publication 11 November 2025
Published 22 November 2025 Volume 2025:19 Pages 10367—10382
DOI https://doi.org/10.2147/DDDT.S553888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Seo-Yeon Choi,1 Eunsol Yang,2 Kwang-Hee Shin1,3
1College of Pharmacy, Research Institute of Pharmaceutical Sciences, Kyungpook National University, Daegu, Republic of Korea; 2Department of Bioengineering and Therapeutic Sciences, University of California, San Francisco, CA, USA; 3Infectious Disease Healthcare, Kyungpook National University, Daegu, Republic of Korea
Correspondence: Kwang-Hee Shin, College of Pharmacy, Research Institute of Pharmaceutical Sciences, Kyungpook National University, 80 Daehak-ro, Buk-gu, Daegu, 41566, Republic of Korea, Tel +82 53 950 8582, Fax +82 53 950 8557, Email [email protected]
Background: Pregnancy-induced physiological changes can substantially alter venlafaxine pharmacokinetics. Despite the clinical relevance of both venlafaxine and its active metabolite, O-desmethylvenlafaxine (ODV), no physiologically-based pharmacokinetic (PBPK) models have been developed that simultaneously describe their disposition during pregnancy. In this study a PBPK model was developed to predict maternal and fetal exposure to venlafaxine and ODV and to optimize dosing regimens.
Methods: PBPK models for venlafaxine and ODV in non-pregnant women, pregnant women, and the fetal–placental unit were developed using the Simcyp® simulator. Model performance was evaluated using visual predictive checks, assessing whether observed data were contained within the predicted 95% confidence intervals, and by comparing predicted versus observed ratios for maximum plasma concentration (Cmax) and area under the concentration–time curve (AUC) using a prespecified range (0.7– 1.3).
Results: In non-pregnant women, observed venlafaxine and ODV concentrations fell within the 95% confidence intervals of model predictions, with Cmax and AUC prediction ratios between 0.7 and 1.3. Most observed data in pregnant women also fell within the 95% confidence intervals. Venlafaxine and ODV concentrations decreased as pregnancy progressed for doses ranging from 37.5 to 225 mg. Cord-to-maternal concentration ratios were approximately 1.02 at 37.5– 150 mg and 1.01 at 225 mg. Predicted venlafaxine and ODV concentrations remained within the therapeutic range (100– 400 ng/mL) at 150 mg during the first and second trimesters, whereas 225 mg was necessary in the third trimester. At a 375 mg dose, the umbilical cord Cmax for venlafaxine reached 195.26 ng/mL, a level approaching thresholds of fetal toxicity. These findings should be interpreted with caution, given the limited sample size in pregnant women (n= 7 for plasma and n=9 for cord blood).
Conclusion: A venlafaxine dose of 150 mg/day is recommended during pregnancy, balancing efficacy with the risk of toxicity in both mother and fetus.
Keywords: venlafaxine, O-desmethylvenlafaxine, pregnancy, PBPK modeling
Introduction
Perinatal depression is a prevalent complication of pregnancy, affecting approximately 20% of pregnant women.1 Despite this high prevalence, only about 40% of women with perinatal depression receive any treatment, and merely 8.6% receive adequate therapy.2 Concerns regarding adverse effects of antidepressants likely contribute to these low treatment rates.3 Untreated antenatal depression is a recognized risk factor for postpartum depression. Depression during pregnancy is associated with increased risks of preterm birth, low birth weight, and, in severe cases, maternal suicide.2,4,5 Notably, discontinuation of antidepressant therapy during pregnancy has been shown to markedly increase the risk of maternal depression relapse, particularly in the first trimester.6 Thus, perinatal depression poses substantial risks to both mother and fetus, highlighting the need for effective treatment during pregnancy.
Venlafaxine is among the most frequently prescribed non-SSRI antidepressants during pregnancy, following selective serotonin reuptake inhibitors (SSRIs), which are generally considered safer for use in pregnant women.7 As a serotonin-norepinephrine reuptake inhibitor, venlafaxine is commonly prescribed for depression, generalized anxiety disorder, and panic disorder. It is used by approximately 1.2% of women of reproductive age and 0.3% of pregnant women annually.8 Among women aged 15–45 years, venlafaxine accounts for 11.2% of all redeemed antidepressant prescriptions, ranking fourth after fluoxetine, citalopram, and escitalopram.7
Venlafaxine exhibits approximately 92% absorption, but its bioavailability is about 45% due to first-pass metabolism. The drug is primarily metabolized by cytochrome P450 2D6 (CYP2D6) to its active metabolite, O-desmethylvenlafaxine (ODV), with minor contributions from CYP2C9 and CYP2C19.9 Venlafaxine and ODV possess similar pharmacological activity.10 Their plasma protein binding rates are approximately 27% and 30%, respectively.11 Approximately 87% of a venlafaxine dose is eliminated in urine within 48 hours; the half-lives of venlafaxine and ODV are about 5 hours and 11 hours, respectively.11 Venlafaxine therapy is typically initiated at 37.5 mg/day to enhance tolerability, with a therapeutic range of 75 to 225 mg/day.11
Pregnancy-induced physiological changes can substantially alter venlafaxine pharmacokinetics. These include changes in gastric emptying, pH, and transit time, which influence bioavailability.12 Increased total body water and decreased plasma protein concentrations affect drug distribution and protein binding.13 Metabolic activity is also altered: CYP2D6 activity increases approximately threefold, while CYP1A2 activity decreases by more than 60% compared to pre-pregnancy.14 Renal blood flow and glomerular filtration rate (GFR) are also elevated during pregnancy.13 Consistent with these physiological changes, the elimination half-life of venlafaxine has been reported to decrease from approximately 8.7 hours in the first trimester to 7.3 hours in the second trimester and 3.2 hours in the third trimester, compared with 6.5 hours in the postpartum period.15 These adaptations impact venlafaxine and ODV concentrations. Two studies have shown that venlafaxine concentrations decline from 98.9% to 87% of postpartum values between the first and third trimesters,16,17 while the ODV/venlafaxine metabolic ratio rises from 76.9% to 196.7%.16
Optimizing venlafaxine dosing in clinical practice remains challenging, particularly during pregnancy. According to the consensus guideline, venlafaxine therapeutic drug monitoring (TDM) is classified as level 2, indicating that TDM is recommended for dose titration or in specific clinical situations rather than as a routine measure.18 A recent study showed that only 39% of patients achieved the therapeutic range (100–400 ng/mL) for venlafaxine active moiety.19 In female patients, the median plasma concentration of the active moiety exceeded this range, emphasizing the difficulty of maintaining therapeutic concentrations and the importance of TDM for guiding dose adjustment.19 This variability is in part attributable to CYP2D6 genetic polymorphisms. The Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline reports that CYP2D6 genetic polymorphisms influence venlafaxine metabolism, which may affect dosing, efficacy, and tolerability.20 Specifically, poor and ultrarapid metabolizers may experience therapeutic failure or adverse effects, necessitating consideration of alternative therapy.20 These clinical challenges, combined with pregnancy-induced physiological changes, further complicate dose adjustment in pregnant women.
Safety concerns have been raised regarding venlafaxine use in late pregnancy. In addition to pharmacokinetic changes, regulatory guidance highlights potential risks. According to the FDA label, third-trimester use of venlafaxine has been associated with neonatal withdrawal symptoms and adverse fetal outcomes such as respiratory distress, feeding difficulties, and excessive irritability.11 Case reports also describe neonatal seizures and respiratory distress following third-trimester exposure.21 These effects are attributed to serotonergic toxicity or drug discontinuation syndrome, and close neonatal monitoring is recommended.
Physiologically based pharmacokinetic (PBPK) modeling is widely used to predict drug concentrations in humans and supports dosing regimen design in special populations, including pregnant women and fetuses.22 For model evaluation, prediction ratios of maximum plasma concentration (Cmax) and area under the curve (AUC) were selected as validation criteria to ensure model reliability.23–25 Existing PBPK models for venlafaxine and ODV have incorporated CYP2D6 genotypes and drug interactions; however, no predictive model has been developed specifically for pregnancy.25 One prior study simulated venlafaxine plasma concentrations during pregnancy using PBPK modeling; however, ODV was not included.24 To date, no PBPK modeling study has simultaneously incorporated both venlafaxine and ODV to predict maternal and fetal exposure.
Therefore, an integrated venlafaxine–ODV PBPK model was developed to capture the sequential metabolism between the parent drug and its active metabolite, enabling simultaneous prediction of the exposure of both compounds in pregnant women and supporting optimal dosing regimens for this population.
Materials and Methods
Software and Workflow
The PBPK models for venlafaxine and ODV in non-pregnant women, pregnant women, and the fetoplacental unit were developed using Simcyp® version 21 (Certara, Princeton, NJ, USA). The modeling workflow is illustrated in Figure 1. Initially, a model for non-pregnant women was constructed by integrating physiological parameters, drug physicochemical properties, ADME characteristics, and clinical study design, using available clinical data. This model was validated against published data. Subsequently, pregnancy-induced physiological changes were incorporated to establish a predictive model for pregnant women, which was also validated. Finally, a fetal–placental model was added, relevant fetal pharmacokinetic parameters were applied, and final model validation was conducted.
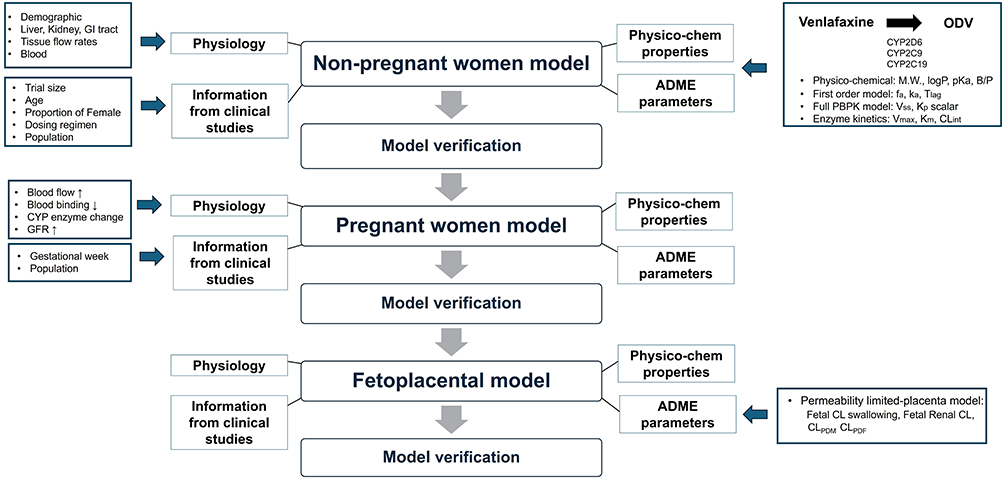 |
Figure 1 Workflow for developing a PBPK model of venlafaxine and ODV during pregnancy. Arrows indicate the direction of the workflow direction or the metabolic conversion of venlafaxine to ODV. Arrows adjacent to physiological parameters denote an increase or decrease. Abbreviations: ODV, O-desmethylvenlafaxine; LogP, logarithm of octanol/water partition coefficient; pKa, negative logarithm of acid dissociation constant; B/P, blood-to-plasma ratio; fup, fraction unbound in plasma; fa, fraction absorbed; ka, absorption rate constant; Kp scalar, tissue-to-plasma partition coefficient; Vmax, maximum reaction rate; Km, substrate concentration at which the reaction rate is half-maximal; GFR, glomerular filtration rate; CLint, intrinsic clearance; CLPDM, maternal-placental barrier clearance; CLPDF, placenta-fetal barrier clearance. |
Development of Non-Pregnant Model
The PBPK model for non-pregnant women was developed using the Simcyp® simulator, which includes compartments for organs such as the liver, kidney, skin, gastrointestinal tract, brain, lung, blood, and other tissues.26 The fraction absorbed (fa), permeability assay value and enzyme parameters for venlafaxine were obtained from the literature (Table 1).24,27,28 Lag time (Tlag), absorption rate constant (ka), and renal clearance (CLR) were optimized using the Simcyp® parameter estimation module, because predictions based on literature values showed discrepancies with observed plasma concentration–time data in healthy participants.29 Parameter estimation was performed using a weighted least squares objective function with the Nelder–Mead minimization method, and the optimization procedure was repeated 100 times to obtain the parameter values. The tissue-to-plasma partition coefficient scalar was sourced from published data and used to predict steady-state volume of distribution via the Rodgers and Rowland method (method 2) (Table 1). Additional systemic clearance was optimized by fitting the predicted plasma concentration–time curve to observed data, as no reliable literature value was available (Table 1).29
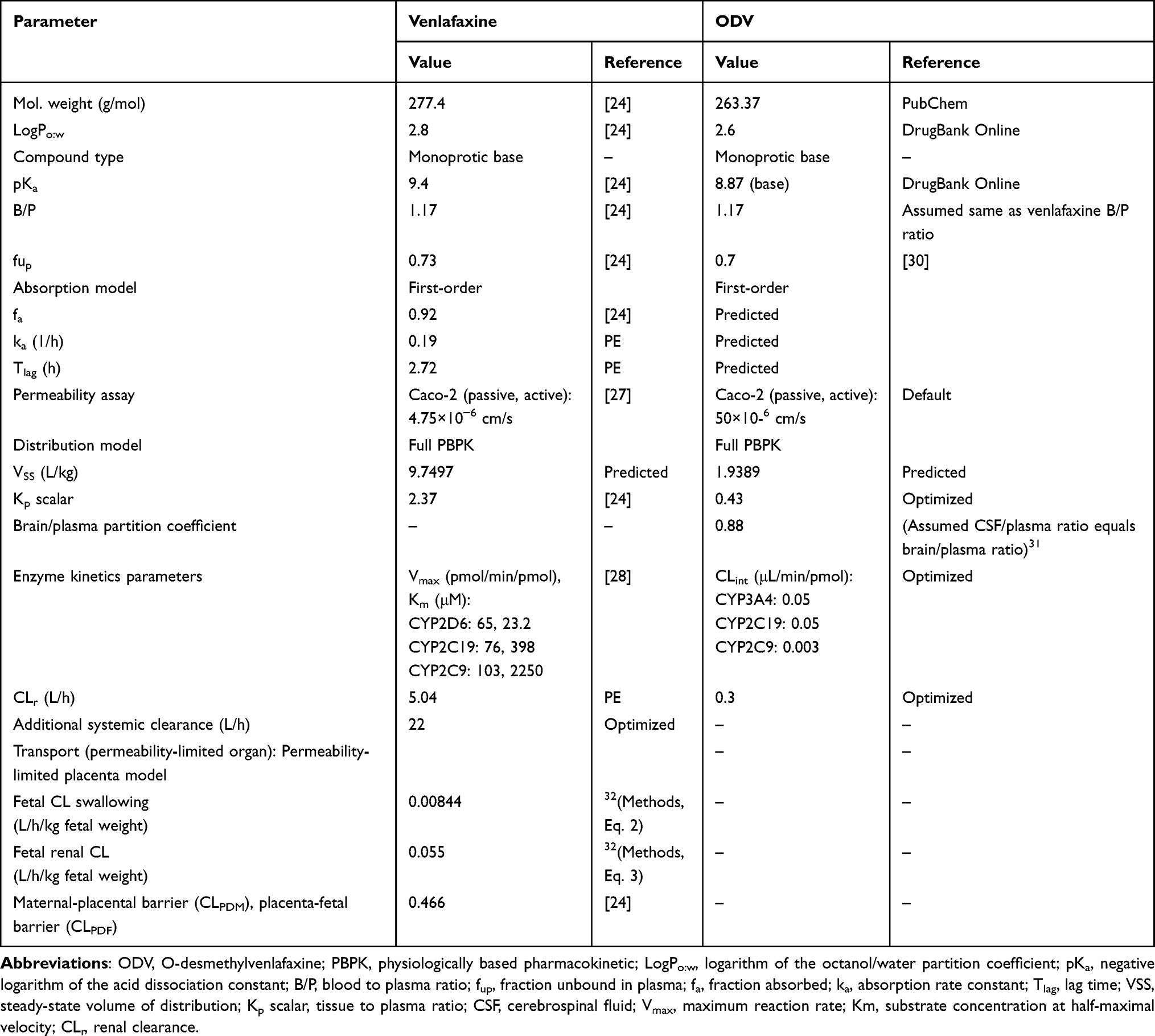 |
Table 1 Input Parameters for the Venlafaxine and ODV PBPK Model |
The fraction unbound in plasma (fup) for ODV was obtained from the literature (Table 1).30 The tissue-to-plasma partition coefficient scalar was adjusted to improve agreement between predicted plasma concentration–time curve and observed data (Table 1).29 The brain-to-plasma distribution coefficient was estimated by assuming equivalence between the cerebrospinal fluid (CSF)–to–plasma ratio and the brain-to-plasma ratio (Table 1), as ODV concentrations in CSF have been reported to be similar to those in the cerebellum.31,33 The steady-state volume of distribution was calculated using the Rodgers and Rowland method based on the tissue-to-plasma partition coefficient scalar. Intrinsic clearance of ODV mediated by CYP3A4, CYP2C19, and CYP2C9 could not be reliably obtained from the literature. Reported values for renal clearance showed discrepancies between predicted plasma concentration–time profiles and observed data.29 Consequently, elimination parameters were selected to achieve consistency with observed plasma concentration–time profiles.29 The robustness of the applied parameters for venlafaxine and ODV was further ensured through evaluation with independent datasets.34
Participants were healthy individuals aged 18–45 years, with a female proportion ranging from 0 to 0.5.29,34 Although original studies enrolled healthy individuals, simulations were performed in non-pregnant women at gestational week 0, with the female proportion set to 1.0 (Table S1). The number of participants ranged from 12 to 22, and each trial was replicated 10 times (Table S1). Dosing regimens included single doses of two 75 mg venlafaxine tablets, a single 75 or 150 mg dose, or repeated 75 mg dosing over 4 days (Table S1).
Development of Pregnant Model
Trimester-specific physiological parameters were integrated into the PBPK model using a gestational age-dependent equation in Simcyp®. These parameters included changes in plasma volume, hepatic CYP enzyme activity, renal function, and blood flow. Each parameter was continuously adjusted across gestational weeks using Equation 1 (Eq. 1), enabling trimester-specific scaling without discrete compartmentalization.35

GW0 denotes the baseline value at week 0 of gestation. B1, B2, B3, and B4 are coefficients that describe changes in these physiological parameters as functions of gestational week (GW), with each coefficient corresponding to a different power of GW. GW represents gestational week, serving as the independent variable to model physiological changes throughout pregnancy. In addition, CYP2D6 genetic variability was represented at the population level by applying the default phenotype frequencies implemented in the Simcyp® pregnancy population model (extensive metabolizer [EM]: 56.8%, poor metabolizer [PM]: 8.2%, intermediate metabolizer [IM]: 32.5%, ultrarapid metabolizer [UM]: 2.5%). These default frequencies are broadly consistent with global allele frequency distributions (PM 5–24%, IM 2–45%, EM/NM 47–80%, UM 2–12%).36
Participants were pregnant women aged 26–34 years, with one to three participants per dose group.16 Because of the limited sample size, default Simcyp® population values were used, which may limit the statistical power and generalizability of the validation. Dosing regimens included 37.5 mg, 75 mg, 150 mg, and 225 mg of venlafaxine administered once daily for 7 days (Table S2). This duration was selected based on FDA-approved prescribing information, which indicates that venlafaxine reaches steady state within 3 days. All dosing regimens reflected observed doses reported in clinical studies and selected according to the specific dosage strengths listed in the FDA-approved labeling. Although other doses are within the approved range, only the standard strengths explicitly referenced in the prescribing information (ie, 37.5 mg, 75 mg, 150 mg, and 225 mg) were included (Table S2).
Plasma trough concentrations were measured for each trimester. Trimester-specific PBPK models were developed according to the timing of drug administration. For participants with dose adjustments across trimesters, each regimen was modeled based on the actual administered dose.
Development of Fetoplacental Model
A fetoplacental model was incorporated into the pregnancy model, integrating fetal-specific pharmacokinetic parameters. This model simulates drug transfer from the placenta to fetal circulation, enabling assessment of fetal drug exposure throughout pregnancy. Fetal clearance via swallowing (L/h/kg fetal weight) was calculated using Eq. 2, based on the average amniotic fluid volume ingested by a full-term fetus (750 mL) and the average fetal weight (3.7 kg).32,37,38 Fetal renal clearance (L/h/kg fetal weight) was determined using Eq. 3, incorporating adult renal clearance (5.04 L/h), fetal and adult GFR values, and fetal weight.32,38–40 Maternal-placental and placenta-fetal barrier clearances were obtained from published sources.24


Participants were pregnant women aged 28–40 years, and the trial size was set to the Simcyp® default of 10×10 because of limited sample availability, which may limit the statistical power and generalizability of the validation (Table S3).41 Dosing regimens included 37.5 mg, 75 mg, 112.5 mg, 150 mg, and 225 mg of venlafaxine once daily for 7 days. Gestational age ranged from 37 to 39 weeks (Table S3).
For simulations evaluating fetal exposure, trial size and maternal age were set to Simcyp® defaults, and gestational week was fixed at 40 weeks (Table S4).
Evaluation of the PBPK Model
In two previously published PBPK studies on venlafaxine, prediction ratios for pharmacokinetic parameters were assessed using the commonly applied twofold range.24,25 In this study, a 30% deviation from unity (0.7–1.3) was applied for prediction ratios for key pharmacokinetic parameters, including Cmax and AUC, providing a more stringent and precise evaluation of model performance.23 The prediction ratio was calculated using Eq. 4. The predictive performance of the model was also evaluated by determining whether the observed mean plasma concentration–time profiles fell within the predicted 95% confidence intervals.

Sensitivity Analysis
Local sensitivity analysis assessed the impact of CYP2D6-related parameters on AUC and Cmax using the third-trimester pregnancy model. Global sensitivity analysis, performed using the Morris method, quantified the influence of 18 physicochemical and drug-specific parameters in the non-pregnant and pregnant models, and 22 parameters in the fetoplacental prediction model, on AUC and Cmax predictions. High absolute mean (µ*) values facilitated parameter ranking; larger µ* indicated greater influence on model outputs.42
Results
Development and Verification of the Prediction Model for Venlafaxine and ODV in Non-Pregnant Women
Observed data generally fell within the 95% confidence intervals of the predicted curves for both venlafaxine and ODV in non-pregnant women (Figure S1). Prediction ratios for Cmax and AUC for venlafaxine and ODV ranged from 0.92–1.27 and 0.81–1.19, respectively, within the acceptable range of 0.7–1.3 (Table S5).
Development and Verification of the Prediction Model for Venlafaxine and ODV in Pregnant Women
Most observed data were within the 95% confidence intervals of the predicted venlafaxine curves (Figures 2 and 3); however, some observed values fell outside these intervals (Figure 3f–h). As with venlafaxine, most observed ODV data were within the 95% confidence intervals of the predicted curves (Figures S2 and S3), although some values were outside these intervals (Figure S3f–S3h). As pregnancy progressed from non-pregnancy through the third trimester, venlafaxine Cmax and AUC decreased by 39.7% and 38.5%, respectively, across all dose (37.5 mg, 75 mg, 150 mg, and 225 mg) levels. Similarly, ODV Cmax and AUC decreased by 31.6% and 40.3%, respectively (Table 2).
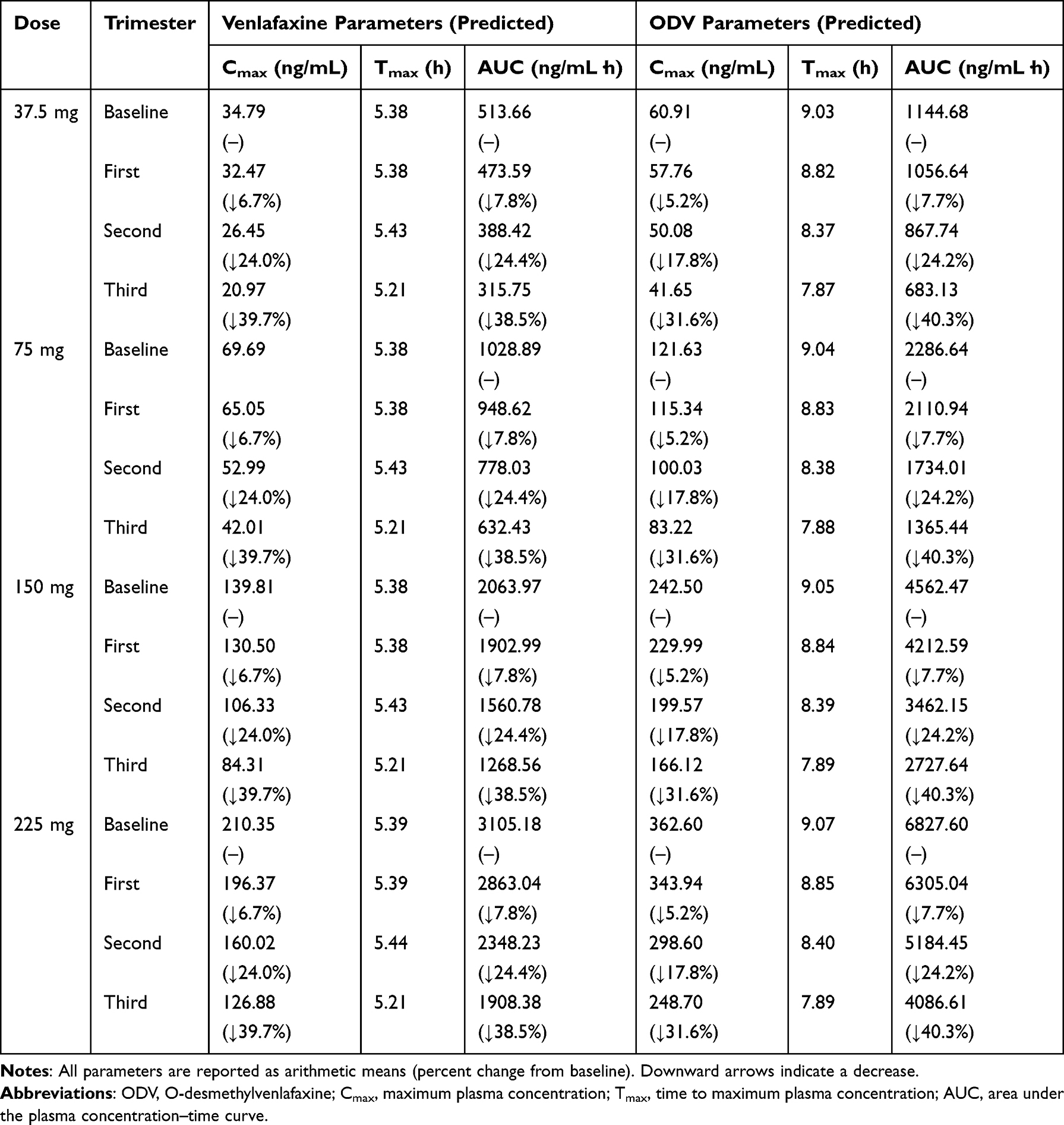 |
Table 2 Predicted Pharmacokinetic Parameters of Venlafaxine and ODV in Non-Pregnant and Pregnant Women Across Pregnancy Trimesters After Multiple Oral Doses |
 |
Figure 2 Predicted plasma concentration–time profiles of venlafaxine following once-daily administration in (a–d) non-pregnant and pregnant women receiving 37.5 mg and (e–h) 75 mg doses. Subfigures (a and e) represent non-pregnant women; (b and f), first trimester; (c and g), second trimester; and (d and h), third trimester. The blue line represents the mean predicted plasma concentrations, and the gray dotted lines denote the 5th and 95th percentiles of predicted concentrations. Circles indicate observed plasma concentrations. |
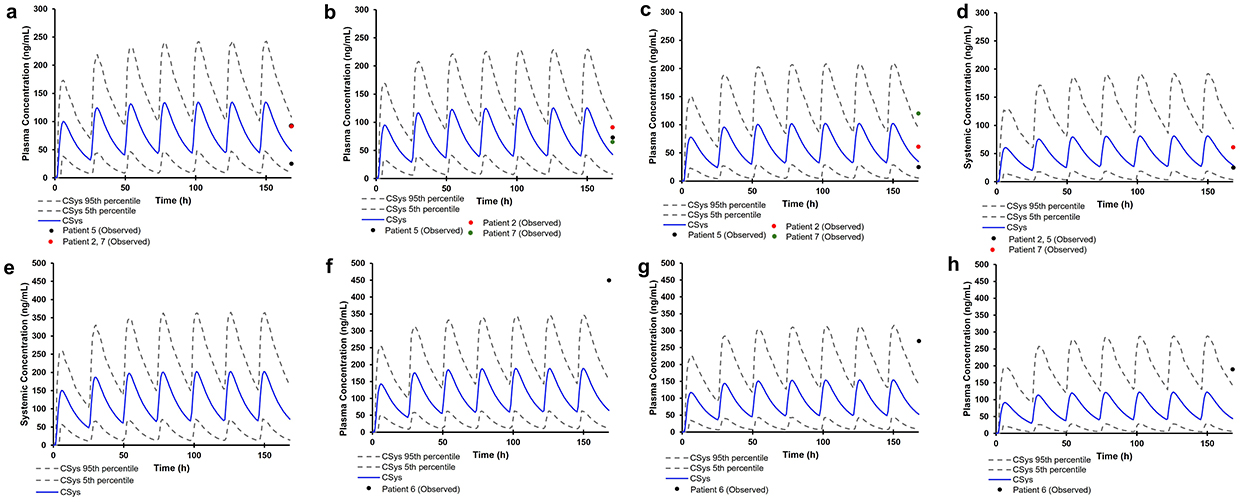 |
Figure 3 Predicted plasma concentration–time profiles of venlafaxine following once-daily administration in (a–d) non-pregnant and pregnant women receiving 150 mg, and (e–h) those receiving 225 mg. Subfigures (a and e) represent non-pregnant women; (b and f) the first trimester; (c and g) the second trimester; and (d and h) the third trimester. The blue line represents the mean predicted plasma concentrations, and the gray dotted lines denote the 5th and 95th percentiles of predicted concentrations. Circles indicate observed plasma concentrations. |
Development and Verification of the Prediction Model for Venlafaxine in the Fetoplacental Unit
Most observed data fell within the 95% confidence intervals of the predictions (Figure 4). Predicted pharmacokinetic parameters of venlafaxine in umbilical cord blood following oral administration of 37.5 mg, 75 mg, 112.5 mg, 150 mg, and 225 mg are presented in Table 3. The predicted cord-to-maternal concentration ratios for venlafaxine were 1.02 at doses of 37.5–150 mg and 1.01 at the 225 mg dose (Table 3).
 |
Table 3 Predicted Venlafaxine Pharmacokinetic Parameters in Term Pregnancy After Repeated Oral Venlafaxine Administration |
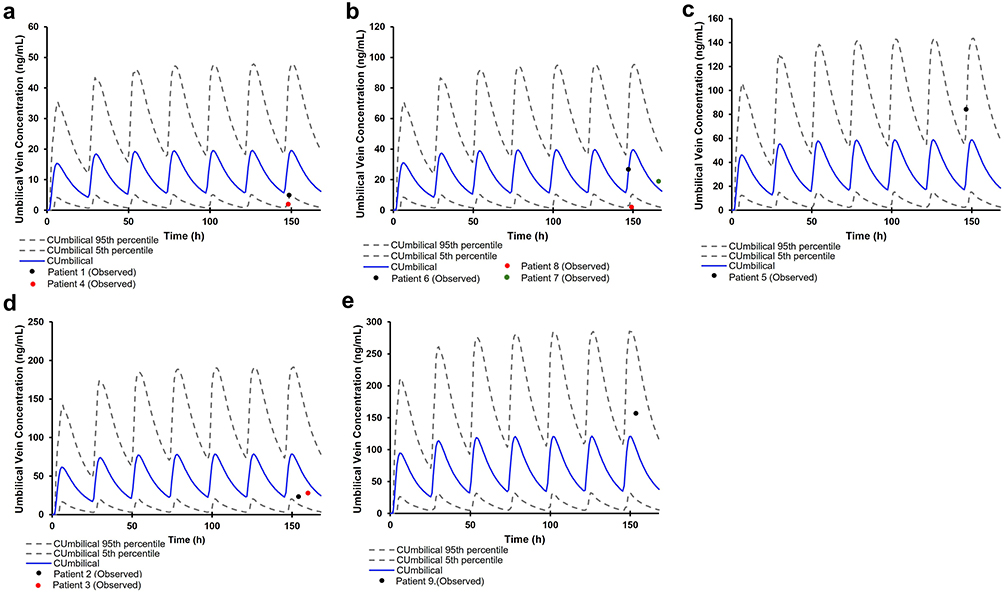 |
Figure 4 Predicted umbilical vein concentration–time profiles of venlafaxine at term pregnancy following (a) 37.5 mg, (b) 75 mg, (c) 112.5 mg, (d) 150 mg, and (e) 225 mg once daily. The blue line represents the mean predicted umbilical vein concentrations, while the gray dotted lines denote the 5th and 95th percentiles of predicted concentrations. Circles indicate observed umbilical vein concentrations. |
Global Sensitivity Analysis of Prediction Model for Venlafaxine in Pregnant Women and Fetoplacental Unit
In both non-pregnant and pregnant models, parameters with the greatest impact on AUC were LogP, pKa, CLR, and Additional CL, while LogP, pKa, B/P, and ka were most influential for Cmax. Across trimesters, most parameters’ µ* values decreased, altering the relative ranking for AUC. However, key parameters influencing Cmax remained consistent throughout all trimesters (Figure S4). In the fetoplacental prediction model, parameters most affecting AUC were LogP, Additional CL, fa, and B/P, while those impacting Cmax were LogP, ka, B/P, and fa (Figure S5). LogP and B/P consistently exhibited high influence across all models, whereas the contributions of clearance-related parameters (CLR, additional CL) varied depending on pregnancy stage and pharmacokinetic parameter.
Dose Optimization of Venlafaxine in the Predicted Model for Pregnant Women
The therapeutic range for combined venlafaxine and ODV concentrations is reported as 100–400 ng/mL.18 In this study, venlafaxine and ODV concentrations were summed to assess whether predicted concentrations were within the therapeutic range.
In the predictive model for pregnant women, venlafaxine + ODV exposure at 37.5 mg and 75 mg/day did not reach the therapeutic range in any trimester (Figure 5 and Table S6).
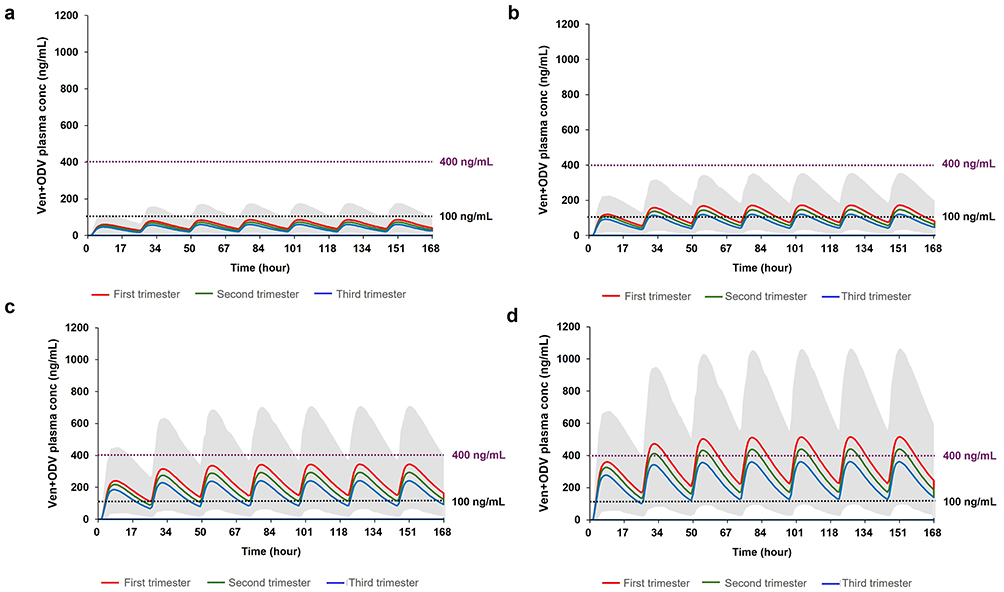 |
Figure 5 Dose optimization of venlafaxine throughout gestation following (a) 37.5 mg, (b) 75 mg, (c) 150 mg, and (d) 225 mg administered once daily. Red lines indicate predicted plasma concentrations during the first trimester, green lines during the second trimester, and blue lines during the third trimester. The shaded gray area represents the 5th and 95th percentiles of predicted Ven + ODV concentrations across trimesters. Dotted horizontal lines denote the therapeutic range (Ven + ODV: 100–400 ng/mL). Abbreviations: Ven, venlafaxine; ODV, O-desmethylvenlafaxine. |
At 150 mg/day, Cmin and Cmax were within the therapeutic range in the first and second trimesters, while Cmin remained marginally below range in the third trimester (Figure 5). At 225 mg/day, both Cmin and Cmax of venlafaxine + ODV were within the therapeutic range in the third trimester (Table S6).
Prediction of Fetal Toxic Exposure to Venlafaxine in the Prediction Model for the Fetoplacental Unit
In vivo studies have shown that the maximum recommended dose of venlafaxine (375 mg) may cause adverse fetal effects.43,44 After administration of 375 mg venlafaxine, the predicted Cmax in umbilical cord blood was 195.26 ng/mL, with a Tmax of 5.43 hours and an AUC of 2805.17 ng·h/mL (Figure S6).
Discussion
In this study, we used the pharmacokinetic parameters of venlafaxine and ODV to develop and validate a predictive model for non-pregnant women, which we subsequently adapted for pregnant women. The prediction ratios for venlafaxine and ODV Cmax and AUC ranged from 0.92–1.27 (95% confidence interval: 0.87–1.33) and 0.81–1.19 (0.77–1.25), respectively, meeting the predefined evaluation criteria (Table S5).
Inter-individual physiological variability, including genetic polymorphisms and other factors, can affect plasma concentrations of venlafaxine and ODV. We constructed a prediction model based on non-pregnant women to estimate venlafaxine and ODV concentrations during pregnancy. Most observed data fell within the 95% confidence intervals of the predictions for venlafaxine doses of 37.5 mg, 75 mg, 150 mg, and 225 mg (Figures 2, 3, S2 and S3). However, some data points (patients 3, 6, and 7) were outside these intervals, likely due to inter-individual variability and genetic factors. P-glycoprotein (P-gp), encoded by the ABCB1 gene, is an efflux transporter and a known substrate for venlafaxine, influencing its bioavailability and brain distribution.9 In vivo studies have shown that knockout of P-gp increases brain concentrations of venlafaxine and ODV by two- to fourfold compared with wild-type mice.9 Additionally, a clinical study found that co-administration of venlafaxine with indinavir, which induces P-gp, resulted in a 28% reduction in AUC and a 36% decrease in Cmax.45 Furthermore, a study using PBPK modeling demonstrated that CYP2D6 genetic polymorphisms and co-administration of CYP2D6 inhibitors, such as clarithromycin or paroxetine, can alter venlafaxine pharmacokinetics.25 Plasma concentrations of venlafaxine are elevated in patients with reduced CYP2D6 activity, indicating that individual metabolic capacity should be considered for dose optimization.25
During pregnancy, physiological changes can reduce the therapeutic efficacy of venlafaxine. In this study, as pregnancy progressed, Cmax and AUC values decreased for all venlafaxine doses tested (Table 2). Previous research similarly reported that venlafaxine plasma concentrations during pregnancy declined from 98.9% to 87.0% of postpartum levels.16 This reduction may be attributable to increased metabolic enzyme activity during pregnancy. The simulated abundance of CYP2D6, the primary enzyme responsible for venlafaxine metabolism, increased by 62.59% in the third trimester compared to baseline (Table S7). In addition, local sensitivity analysis showed that increasing the Vmax of CYP2D6 reduced both Cmax and AUC of venlafaxine, while a higher Km value led to increased drug exposure (Figure S7). Moreover, CYP2D6 activity has been reported to increase approximately threefold during pregnancy,14,46 which may contribute to the observed reductions in Cmax and AUC.
Our results indicate that fetal circulation can be exposed to venlafaxine at concentrations similar to those in maternal plasma. Using a fetoplacental prediction model, we found that the predicted cord-to-maternal concentration ratios of venlafaxine were 1.02 at doses from 37.5 mg to 150 mg and 1.01 at 225 mg (Figure 4 and Table 3), closely matching previously reported ratios of approximately 1.05.41 Venlafaxine’s high lipid solubility (logP 2.8) and low ionization (pKa 9.4) facilitate placental transfer.47
Our PBPK model predicts that dose adjustments may be necessary to maintain therapeutic exposure throughout pregnancy. Both venlafaxine and ODV contribute to pharmacological activity, making it essential to consider their combined effects when adjusting doses.48 Notably, active moiety concentrations below 100 ng/mL have been associated with insufficient therapeutic response, as venlafaxine acts primarily as an SSRI at these levels rather than as a serotonin-norepinephrine reuptake inhibitor.18
A dose of 150 mg/day is predicted to be optimal during pregnancy. Combined venlafaxine and ODV exposure at the target dose of 75 mg/day did not reach the therapeutic range in all trimesters, indicating the need for dose adjustment during pregnancy (Figure 5 and Table S6). A 150 mg/day dose achieved the therapeutic range during the first and second trimesters, but the Cmin remained slightly below the therapeutic range in the third trimester (Figure 5). At 225 mg/day, both the Cmin and Cmax of the combined venlafaxine and ODV were within the therapeutic range in the third trimester, suggesting that additional dose escalation may offer further benefit (Table S6). In the third trimester, a daily dose of 225 mg may provide marginally higher exposure compared to 150 mg/day; however, the difference appears minimal. Furthermore, previous research assessing dose optimization based on CYP2D6 phenotypes also recommended increasing doses as pregnancy progresses.24 Both studies underscore the need to adjust venlafaxine dosing during pregnancy.
These findings suggest a practical framework for venlafaxine dose adjustment during pregnancy. A dose of 150 mg/day appears appropriate for patients in the first and second trimesters of pregnancy, whereas escalation to 225 mg/day may be considered in the third trimester if therapeutic concentrations are not achieved. This escalation remains within the FDA-approved therapeutic range (75–225 mg/day); however, safety considerations must be weighed.11 Although 225 mg/day is within the FDA-labeled maximum dose for major depressive disorder and anxiety disorders, third-trimester use has been associated with maternal complications, including preeclampsia and postpartum hemorrhage as well as neonatal adaptation syndrome.11 Therapeutic plasma concentrations of 100–400 ng/mL represent the internationally recommended reference range for venlafaxine and ODV; however, their relationship with perinatal depression outcomes is not fully established, and this range should be interpreted with caution.18
It is essential to avoid doses that may pose fetal risk. Administration of venlafaxine at the maximum recommended dose (375 mg) resulted in predicted umbilical cord concentrations of 195.26 ng/mL (Figure S6). In vivo studies have shown that doses equivalent to this human exposure level can increase fetal oxidative stress and apoptotic signaling, promoting neurodegeneration and potential cognitive and emotional deficits in adulthood.43,44 Therefore, a predicted umbilical cord concentration of 195.26 ng/mL may represent a threshold for adverse fetal effects.
This study has some limitations. The number of pregnant participants with venlafaxine plasma level measurements was small. Furthermore, most umbilical cord concentration data were collected only at delivery, which limited the statistical power and hindered model validation across different gestational stages. This limitation is common among PBPK pregnancy models, which are frequently validated using small clinical datasets (1–10 participants).49–51 These challenges underscore the inherent difficulties associated with validating PBPK models in the pregnant population. Consequently, these results should be considered exploratory. Further prospective multi-center studies are required to confirm these findings and establish their clinical applicability. Following this validation, the proposed dosing recommendations could be considered for clinical implementation. Despite these limitations, we successfully predicted the concentration–time profiles of venlafaxine and ODV during pregnancy and provided insights into fetal exposure. These model-based predictions can expand the understanding of drug disposition in this population and provide a framework for trimester-specific dosing optimization that considers both venlafaxine and ODV, which has not been addressed in previous studies.
Conclusion
We successfully developed and validated a maternal-fetal PBPK model for venlafaxine and ODV, enabling informed dose optimization during pregnancy, despite the limited observational sample size. A venlafaxine dose of 150 mg once daily is recommended during pregnancy, considering therapeutic range and the potential fetal toxicity associated with higher doses such as 375 mg/day. These findings enhance our understanding of venlafaxine pharmacokinetics during pregnancy and support the development of safer and more effective treatment strategies for this population; however, these recommendations require further validation before clinical application.
Abbreviations
ODV, O-desmethylvenlafaxine; Cmax, maximum plasma concentration; SSRI, serotonin reuptake inhibitor; CYP2D6, cytochrome P450 2D6; GFR, glomerular filtration rate; PBPK, physiologically based pharmacokinetic; ka, absorption rate constant; CLR, renal clearance; GW, gestational week; AUC, area under the curve; Tlag, lag time; EM, extensive metabolizer; PM, poor metabolizer; IM, intermediate metabolizer; UM, ultrarapid metabolizer; µ*absolute mean.
Data Sharing Statement
The data supporting this study are available from the corresponding author (Dr. Kwang-Hee Shin) upon reasonable request.
Ethics Approval and Informed Consent
All clinical data included in this analysis were obtained from previously published studies and contained no information that could identify individual participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. RS-2023-00251397) and by the BK21 FOUR (Fostering Outstanding Universities for Research) program through the National Research Foundation of Korea (NRF) under the Ministry of Education (No. 2120240615414, Healthcare Convergence Educational Group for Infectious Disease Management).
Disclosure
No conflicts of interest are associated with this research.
References
1. Leung BM, Kaplan BJ. Perinatal depression: prevalence, risks, and the nutrition link—a review of the literature. J Am Diet Assoc. 2009;109(9):1566–1575. doi:10.1016/j.jada.2009.06.368
2. Cox EQ, Sowa NA, Meltzer-Brody SE, Gaynes BN. The perinatal depression treatment cascade: baby steps toward improving outcomes. J Clini Psych. 2016;77(9):20901. doi:10.4088/JCP.15r10174
3. Petersen I, Gilbert RE, Evans SJ, Man S-L, Nazareth I. Pregnancy as a major determinant for discontinuation of antidepressants: an analysis of data from The Health Improvement Network. J Clini Psych. 2011;72(7):15209. doi:10.4088/JCP.10m06090blu
4. Vigod SN, Wilson CA, Howard LM. Depression in pregnancy. BMJ. 2016;352. doi:10.1136/bmj.i1547
5. Talge NM, Neal C, Glover V, et al. Antenatal maternal stress and long‐term effects on child neurodevelopment: how and why? J Child Psychol Psychiatry. 2007;48(3‐4):245–261. doi:10.1111/j.1469-7610.2006.01714.x
6. Cohen LS, Nonacs R, Bailey J, et al. Relapse of depression during pregnancy following antidepressant discontinuation: a preliminary prospective study. Arch Women’s Mental Health. 2004;7(4):217–221. doi:10.1007/s00737-004-0059-3
7. Wemakor A, Casson K, Dolk H. Prevalence and sociodemographic patterns of antidepressant use among women of reproductive age: a prescription database study. J Affective Disorders. 2014;167:299–305. doi:10.1016/j.jad.2014.06.015
8. Summers AD, Anderson KN, Ailes EC, et al. Venlafaxine prescription claims among insured women of reproductive age and pregnant women, 2011–2016. Birth Defects Res. 2021;113(14):1052–1056. doi:10.1002/bdr2.1897
9. Magalhães P, Alves G, Llerena A, Falcão A. Venlafaxine pharmacokinetics focused on drug metabolism and potential biomarkers. Drug Metab Drug Interact. 2014;29(3):129–141. doi:10.1515/dmdi-2013-0053
10. Haufroid V, Hantson P. CYP2D6 genetic polymorphisms and their relevance for poisoning due to amfetamines, opioid analgesics and antidepressants. Clin Toxicol. 2015;53(6):501–510. doi:10.3109/15563650.2015.1049355
11. U.S. Food and Drug Administration. Label for EFFEXOR XR® (venlafaxine Extended-Release) Capsules. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/020699s118lbl.pdf.
12. Levy D, Williams O, Magides A, Reilly C. Gastric emptying is delayed at 8–12 weeks’ gestation. Br J Anaesth. 1994;73(2):237–238. doi:10.1093/bja/73.2.237
13. Mattison DR, Blann E, Malek A. Physiological alterations during pregnancy: impact on toxicokinetics. Fundam Appl Toxicol. 1991;16(2):215–218. doi:10.1016/0272-0590(91)90103-B
14. Abduljalil K, Furness P, Johnson TN, Rostami-Hodjegan A, Soltani H. Anatomical, physiological and metabolic changes with gestational age during normal pregnancy: a database for parameters required in physiologically based pharmacokinetic modelling. Clin Pharmacokinet. 2012;51:365–396. doi:10.2165/11597440-000000000-00000
15. Yue M, Kus L, Katta S, et al. Pharmacokinetics of Antidepressants in pregnancy. J Clin Pharmacol. 2023;63:S137–S158. doi:10.1002/jcph.2282
16. Ter Horst P, Larmené‐Beld K, Bosman J, Van Der Veen E, Wieringa A, Smit J. Concentrations of venlafaxine and its main metabolite O‐desmethylvenlafaxine during pregnancy. J Clin Pharm Therapeutics. 2014;39(5):541–544. doi:10.1111/jcpt.12188
17. Westin AA, Brekke M, Molden E, Skogvoll E, Spigset O. Selective serotonin reuptake inhibitors and venlafaxine in pregnancy: changes in drug disposition. PLoS One. 2017;12(7):e0181082. doi:10.1371/journal.pone.0181082
18. Hiemke C, Bergemann N, Clement H, et al. Consensus guidelines for therapeutic drug monitoring in neuropsychopharmacology: update 2017. Pharmacopsychiatry. 2018;51(01/02):9–62. doi:10.1055/s-0043-116492
19. Krivosova M, Grendár M, Kertys M, et al. Therapeutic drug monitoring of venlafaxine and impact of age, gender, BMI, and diagnosis. Eur Pharmaceut J. 2020;67(1):33–37.
20. Bousman CA, Stevenson JM, Ramsey LB, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A genotypes and serotonin reuptake inhibitor antidepressants. Clin Pharmacol Ther. 2023;114(1):51–68. doi:10.1002/cpt.2903
21. Bellantuono C, Vargas M, Mandarelli G, Nardi B, Martini MG. The safety of serotonin–noradrenaline reuptake inhibitors (SNRIs) in pregnancy and breastfeeding: a comprehensive review. Hum Psychopharmacol Clin Exp. 2015;30(3):143–151. doi:10.1002/hup.2473
22. Abbiati RA, Manca D. A modeling tool for the personalization of pharmacokinetic predictions. Comput Chem Eng. 2016;91:28–37. doi:10.1016/j.compchemeng.2016.03.008
23. Jeong H-C, Kim M-G, Wei Z, et al. Integration of a physiologically based pharmacokinetic and pharmacodynamic model for tegoprazan and its metabolite: application for predicting food effect and intragastric pH alterations. Pharmaceutics. 2022;14(6):1298. doi:10.3390/pharmaceutics14061298
24. Alenezi M, Badhan RK. Precision dosing of venlafaxine during pregnancy: a pharmacokinetics modelling approach. J Pharm Pharmacol. 2024;76(2):122–137. doi:10.1093/jpp/rgad106
25. Cho C-K, Kang P, Jang C-G, et al. PBPK modeling to predict the pharmacokinetics of venlafaxine and its active metabolite in different CYP2D6 genotypes and drug–drug interactions with clarithromycin and paroxetine. Arch Pharmacal Res. 2024;47:1–24.
26. Khalidi H, Onasanwo A, Islam B, et al. SimRFlow: an R-based workflow for automated high-throughput PBPK simulation with the Simcyp® simulator. Front Pharmacol. 2022;13:929200. doi:10.3389/fphar.2022.929200
27. Oganesian A, Shilling AD, Young-Sciame R, et al. Desvenlafaxine and venlafaxine exert minimal in vitro inhibition of human cytochrome P450 and P-glycoprotein activities. Psychopharmacol Bull. 2009;42(2):47–63. doi:10.64719/pb.4308
28. Pansari A, Faisal M, Jamei M, Abduljalil K. Prediction of basic drug exposure in milk using a lactation model algorithm integrated within a physiologically based pharmacokinetic model. Biopharm Drug Dispos. 2022;43(5):201–212. doi:10.1002/bdd.2334
29. Troy SM, Dilea C, Martin PT, Rosen AS, Fruncillo RJ, Chiang ST. Bioavailability of once-daily venlafaxine extended release compared with the immediate-release formulation in healthy adult volunteers. Curr Ther Res. 1997;58(8):492–503. doi:10.1016/S0011-393X(97)80041-0
30. Lin H-P, Sun D, Zhang X, Wen H. Physiologically based pharmacokinetic modeling for substitutability analysis of venlafaxine hydrochloride extended-release formulations using different release mechanisms: osmotic pump versus openable matrix. J Pharmaceut Sci. 2016;105(10):3088–3096. doi:10.1016/j.xphs.2016.06.015
31. Murrell MD, Cruz DA, Javors MA, Thompson PM. Distribution of venlafaxine, O‐desmethylvenlafaxine, and O‐desmethylvenlafaxine to venlafaxine ratio in postmortem human brain tissue. J Forensic Sci. 2014;59(3):683–689. doi:10.1111/1556-4029.12393
32. Werdan Romão MA, Pinto L, Cavalli RC, et al. Mechanistic framework to predict maternal‐placental‐fetal pharmacokinetics of Nifedipine employing physiologically based pharmacokinetic modeling approach. J Clin Pharmacol. 2024;64(5):568–577. doi:10.1002/jcph.2404
33. Paulzen M, Groppe S, Tauber SC, Veselinovic T, Hiemke C, Gründer G. Venlafaxine and O-desmethylvenlafaxine concentrations in plasma and cerebrospinal fluid. J Clini Psych. 2014;76(1):22165.
34. Troy SM, Dilea C, Martin PT, Leister CA, Fruncillo RJ, Chiang ST. Pharmacokinetics of once-daily venlafaxine extended release in healthy volunteers. Curr Ther Res. 1997;58(8):504–514. doi:10.1016/S0011-393X(97)80042-2
35. Jogiraju VK, Avvari S, Gollen R, Taft DR. Application of physiologically based pharmacokinetic modeling to predict drug disposition in pregnant populations. Biopharm Drug Dispos. 2017;38(7):426–438. doi:10.1002/bdd.2081
36. Gaedigk A, Sangkuhl K, Whirl-Carrillo M, Klein T, Leeder JS. Prediction of CYP2D6 phenotype from genotype across world populations. Genet Med. 2017;19(1):69–76. doi:10.1038/gim.2016.80
37. Blackburn ST. Maternal, Fetal, & Neonatal Physiology: A Clinical Perspective. Elsevier Health Sciences. 2007.
38. Johnsen SL, Rasmussen S, Wilsgaard T, Sollien R, Kiserud T. Longitudinal reference ranges for estimated fetal weight. Acta obstetricia et gynecologica Scandinavica. 2006;85(3):286–297. doi:10.1080/00016340600569133
39. Ezuruike U, Blenkinsop A, Pansari A, Abduljalil K. Quantification of fetal renal function using fetal urine production rate and its reflection on the amniotic and fetal creatinine levels during pregnancy. Front Pediatrics. 2022;10:841495. doi:10.3389/fped.2022.841495
40. Rhodin MM, Anderson BJ, Peters AM, et al. Human renal function maturation: a quantitative description using weight and postmenstrual age. Pediatr Nephrol. 2009;24:67–76. doi:10.1007/s00467-008-0997-5
41. Paulzen M, Schoretsanitis G, Gründer G, Franz C, Stingl JC, Augustin M. Pregnancy exposure to venlafaxine—therapeutic drug monitoring in maternal blood, amniotic fluid and umbilical cord blood and obstetrical outcomes. J Affective Disorders. 2020;266:578–584. doi:10.1016/j.jad.2020.02.010
42. Liu D, Li L, Rostami-Hodjegan A, Bois FY, Jamei M. Considerations and caveats when applying global sensitivity analysis methods to physiologically based pharmacokinetic models. AAPS J. 2020;22:1–13. doi:10.1208/s12248-020-00480-x
43. Singh K, Sharma P, Singh M. Prenatal Venlafaxine Exposure–Induced Neurocytoarchitectural and Neuroapoptotic Degeneration in Striatum and Hippocampus of Developing Fetal Brain, Manifesting Long-term Neurocognitive Impairments in Rat Offspring. Neurotox Res. 2022;40(5):1174–1190. doi:10.1007/s12640-022-00541-3
44. Singh M, Singh K, Shukla S, Dikshit M. Assessment of in-utero venlafaxine induced, ROS-mediated, apoptotic neurodegeneration in fetal neocortex and neurobehavioral sequelae in rat offspring. Int J Dev Neurosci. 2015;40:60–69. doi:10.1016/j.ijdevneu.2014.10.007
45. Magalhães P, Alves G, LLerena A, Falcão A. Clinical drug-drug interactions: focus on venlafaxine. Drug Metabol Personalized Ther. 2015;30(1):3–17. doi:10.1515/dmdi-2014-0011
46. Jeong H. Altered drug metabolism during pregnancy: hormonal regulation of drug-metabolizing enzymes. Expert Opin Drug Metab Toxicol. 2010;6(6):689–699. doi:10.1517/17425251003677755
47. Loebstein R, Lalkin A, Koren G. Pharmacokinetic changes during pregnancy and their clinical relevance. Clin Pharmacokinet. 1997;33:328–343. doi:10.2165/00003088-199733050-00002
48. Garland M. Pharmacology of drug transfer across the placenta. Obstetrics Gynecol Clin North Am. 1998;25(1):21–42. doi:10.1016/S0889-8545(05)70356-9
49. Gaohua L, Abduljalil K, Jamei M, Johnson TN, Rostami‐Hodjegan A. A pregnancy physiologically based pharmacokinetic (p‐PBPK) model for disposition of drugs metabolized by CYP1A2, CYP2D6 and CYP3A4. Br J Clin Pharmacol. 2012;74(5):873–885. doi:10.1111/j.1365-2125.2012.04363.x
50. Le Merdy M, Szeto KX, Perrier J, Bolger MB, Lukacova V. PBPK modeling approach to predict the behavior of drugs cleared by metabolism in pregnant subjects and fetuses. Pharmaceutics. 2024;16(1):96. doi:10.3390/pharmaceutics16010096
51. Szeto KX, Le Merdy M, Dupont B, Bolger MB, Lukacova V. PBPK modeling approach to predict the behavior of drugs cleared by kidney in pregnant subjects and fetus. AAPS J. 2021;23(4):89. doi:10.1208/s12248-021-00603-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.