Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 15
Optimizing Timing and Preparation for Allogeneic Hematopoietic Stem Cell Transplantation in Higher-Risk Myelodysplastic Syndromes
Authors Geng L, Chen E, Ji Y, Liu H, Sun Z ![]()
Received 2 April 2025
Accepted for publication 2 July 2025
Published 1 August 2025 Volume 2025:15 Pages 103—113
DOI https://doi.org/10.2147/BLCTT.S527790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Wilson Gonsalves
Liangquan Geng,1,* Erling Chen,2,* Yanping Ji,3,* Huilan Liu,1 Zimin Sun1,2,4
1Department of Hematology, The First Affiliated Hospital of University of Science and Technology of China, Hefei, People’s Republic of China; 2Institute of Hematology and Blood Diseases Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Tianjin, People’s Republic of China; 3Department of Hematology, Affiliated Hospital of Jiangsu University, Zhenjiang, People’s Republic of China; 4Blood and Cell Therapy Institute, Division of Life Sciences and Medicine, Anhui Provincial Key Laboratory of Blood Research and Applications, University of Science and Technology of China, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zimin Sun, Department of Hematology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, No. 17 Lujiang Road, Luyang District, Hefei, Anhui, 230001, People’s Republic of China, Email [email protected]
Introduction: Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is the only curative treatment for higher-risk myelodysplastic syndromes (MDS), but optimal timing and donor selection remain controversial.
Methods: We conducted a retrospective analysis of 70 higher-risk MDS patients classified by the revised International Prognostic Scoring System (IPSS-R) undergoing allo-HSCT. Patients were stratified by: 1) the interval from diagnosis to allo-HSCT (early: < 6 months vs later: ≥ 6 months); 2) pre-transplant treatment cycles (fewer: < 2 vs more: ≥ 2); 3) remission status (complete remission [CR] / partial remission [PR] vs non-remission [NR]), and 4) donor type (sibling vs unrelated cord blood [UCB]).
Results: The results showed a significantly higher 3-year overall survival (OS) in the early HSCT group (70% vs 50%, p = 0.05) with lower transplant-related mortality (TRM) (22.7% vs 46.5%, p = 0.0205). Although more pre-transplant treatment cycles were linked to a lower relapse rate (2.3% vs 15.4%, p = 0.0403), they did not significantly affect OS or TRM. Early HSCT emerged as the only significant factor influencing both OS (Hazard Ratio [HR] 2.84, p = 0.01) and TRM (HR 3.21, p = 0.01). While no significant differences were noted between sibling HSCT and unrelated cord blood transplantation (UCBT) for OS and TRM, UCBT demonstrated a lower incidence of chronic graft-versus-host disease (cGVHD) (19.0% vs 52.9%, p = 0.003).
Discussion: Our findings suggest early allo-HSCT may optimize outcomes in higher-risk MDS. In settings where sibling donors are unavailable, UCBT could serve as a potential alternative, though this observation requires validation in prospective multicenter studies to account for inherent selection biases and confounding factors.
Keywords: allogeneic hematopoietic stem cell transplantation, myelodysplastic syndromes, higher-risk
Introduction
Myelodysplastic syndromes (MDS) comprise a group of clonal disorders originating from hematopoietic stem cells, characterized by ineffective hematopoiesis that results in refractory cytopenias and an elevated risk of leukemic transformation, particularly in higher-risk patients with poor prognoses,1 although allogeneic hematopoietic stem cell transplantation (allo-HSCT) remains the only curative option.2 Several factors influence post-transplant outcomes, including pre-transplant disease characteristics such as bone marrow blasts, cytogenetic risk, the revised International Prognostic Scoring System (IPSS-R) risk stratification, and disease status, as well as patient-related factors like performance status and comorbidity index.3 Various prognostic scoring systems, such as the IPSS-R, are widely used to guide MDS management and predict survival and disease progression; however, these models do not account for transplant-specific factors.4–6 Sibling donors are generally preferred for transplantation, with alternative donor sources following a hierarchy of matched unrelated donors, haplo/mismatched unrelated donors, and unrelated cord blood (UCB); the latter being less effective overall than sibling.7 However, some pre-transplant issues in higher-risk MDS remain unresolved, including the optimal timing for transplantation, the necessity of achieving complete remission (CR) before transplant, the role of bridging therapy, and the appropriate number of treatment cycles. It is debated whether to wait for CR or proceed with allo-HSCT soon after diagnosis and to what extent blast reduction is required if CR cannot be achieved.8,9 Previous reports indicate that the 3-year overall survival (OS) for higher-risk MDS patients treated with UCB transplantation (UCBT) approaches 30%, though studies directly comparing UCBT to sibling HSCT (sib-HSCT) are rare.10 As a transplantation center processing the highest annual volume of China Marrow Donor Program (CMDP)-registered UCBT cases in China, our institution has significant experience in using UCBT for MDS patients. This article aims to retrospectively analyze the transplant outcomes of allo-HSCT in higher-risk MDS patients, with a particular focus on the significance of pre-transplant tumor burden and the necessity of multiple cycles of pre-transplant chemotherapy or hypomethylating agents (HMA) therapy to achieve remission. It also seeks to explore outcome differences between UCBT and sib-HSCT and assess whether cord blood can serve as a viable alternative donor source for transplantation.
Patients and Methods
Study Design
This retrospective study included higher-risk MDS patients who underwent their first allo-HSCT at the First Affiliated Hospital of the University of Science and Technology of China between February 2015 and December 2021. The study protocol was approved by the Institutional Review Board (Approval No. 2022-RE-070) and complied with the Declaration of Helsinki.
Diagnostic Criteria and Patient Selection
MDS diagnosis and classification followed the 2016 World Health Organization criteria.11 The study’s keywords reflect these standardized diagnostic categories and intervention modalities. Only patients classified as higher-risk (high or very high) according to the IPSS-R at diagnosis were included. Exclusion criteria included: lower-risk IPSS-R categories (very low, low, or intermediate); missing data; prior HSCT; bone marrow or peripheral blood blasts ≥ 20% at any point; or loss to follow-up. To minimize donor heterogeneity, cases of haplo-identical HSCT (n=4) were also excluded.
Transplantation Protocol
Donor selection was based on the availability of a suitable HLA-matched sibling. If unavailable or if rapid disease progression precluded finding a matched unrelated donor, a single-unit UCBT was considered. Cord blood units were matched at 4/6 to 6/6 loci using high-resolution DNA typing. Units with donor-specific antibodies positive against recipient HLA antigens were discarded. Follow-up data were collected up to March 1, 2024.
Conditioning Regimens
All patients received a myeloablative conditioning regimen without antithymocyte globulin, which included: (1) Flu + Bu + Cy ± Dec (Fludarabine [Flu], 30 mg/m² daily for 4 days; Busulfan [Bu], 0.8 mg/kg every 6 hours for 4 days; Cyclophosphamide [Cy], 60 mg/kg daily for 2 days; Decitabine [Dec], 20 mg/m² daily for 3 days); (2) Bu + Cy (same dosage as above), used only for sib-HSCT performed before 2017; (3) TBI + Ara-C + Cy (Total body irradiation [TBI], 3 Gy twice daily for 2 days; Cytarabine [Ara-C], 2 g/m² every 12 h for 4 days; Cy, 60 mg/kg daily for 2 days).
GVHD Prophylaxis
All patients received cyclosporine A (CSA) in combination with mycophenolate mofetil (MMF). 2 cases of sib-HSCT patients also received post-transplant cyclophosphamide (100 mg/kg, days +3 and +4) or methotrexate (10 mg/m², days +1, +3, and +6), respectively. From day −1 to day +30, CSA was administered intravenously at a dose of 2.5–3 mg/kg daily, and was switched to an oral regimen once the patient could tolerate it. The target trough level of CSA was maintained at 200–300 ng/mL for at least 1 month. MMF was given orally from day +1 to day +28, at a dose of 25–30 mg/kg daily, or until neutrophil recovery. The dose of MMF was tapered based on the presence of acute graft-versus-host disease (GVHD) or infection. Granulocyte colony-stimulating factor was used from day 6 until neutrophil recovery.
Outcome Measures
The primary outcomes of this study were 3-year OS, 3-year transplant-related mortality (TRM), and 3-year relapse rate. The secondary outcome was GVHD relapse-free survival (GRFS).
Definitions
OS was measured from the date of stem cell infusion to the date of death or last follow-up. TRM was defined as death without disease relapse, caused by conditioning regimen-related factors, marrow failure, infections occurring before immune recovery, or GVHD-related complications. GRFS was defined as the time from allo-HSCT to the occurrence of grade III–IV acute GVHD (aGVHD), chronic GVHD (cGVHD) requiring systemic treatment, relapse or disease progression, or death, whichever occurred first.
Statistical Analysis
Statistical analysis was conducted using SPSS version 25. Survival times were reported as medians (range). OS and GRFS were estimated using the Kaplan-Meier method, with group differences analyzed by the Log rank test. Univariate analysis was performed using logistic regression. Neutrophil and platelet engraftment rates, along with the incidence of aGVHD, TRM, and relapse, were analyzed using a competing risks model with EZR version 1.36. Cumulative incidence rates were compared using the Gray test in R software. A p-value of less than 0.05 was considered statistically significant.
Ethical Considerations
Written informed consent was obtained from all participants/legal guardians. The study was monitored by an independent data safety committee.
Results
Patient Characteristics
A total of 70 higher-risk MDS patients who underwent allo-HSCT were identified from the database. Patient demographics and disease characteristics are summarized in Table 1. The median age was 33 years (range: 2–63 years). 15 patients (21.4%) had a genetic karyotype of monosomy or complex karyotype at diagnosis. The median time from diagnosis to transplantation was 5 months (range: 1–110 months). 21 patients (30%) achieved partial remission (PR) or CR following prior chemotherapy or HMA induction, while 18 patients underwent direct transplantation without prior induction treatment. 43 patients (61.4%) were long-term transfusion-dependent before transplantation.
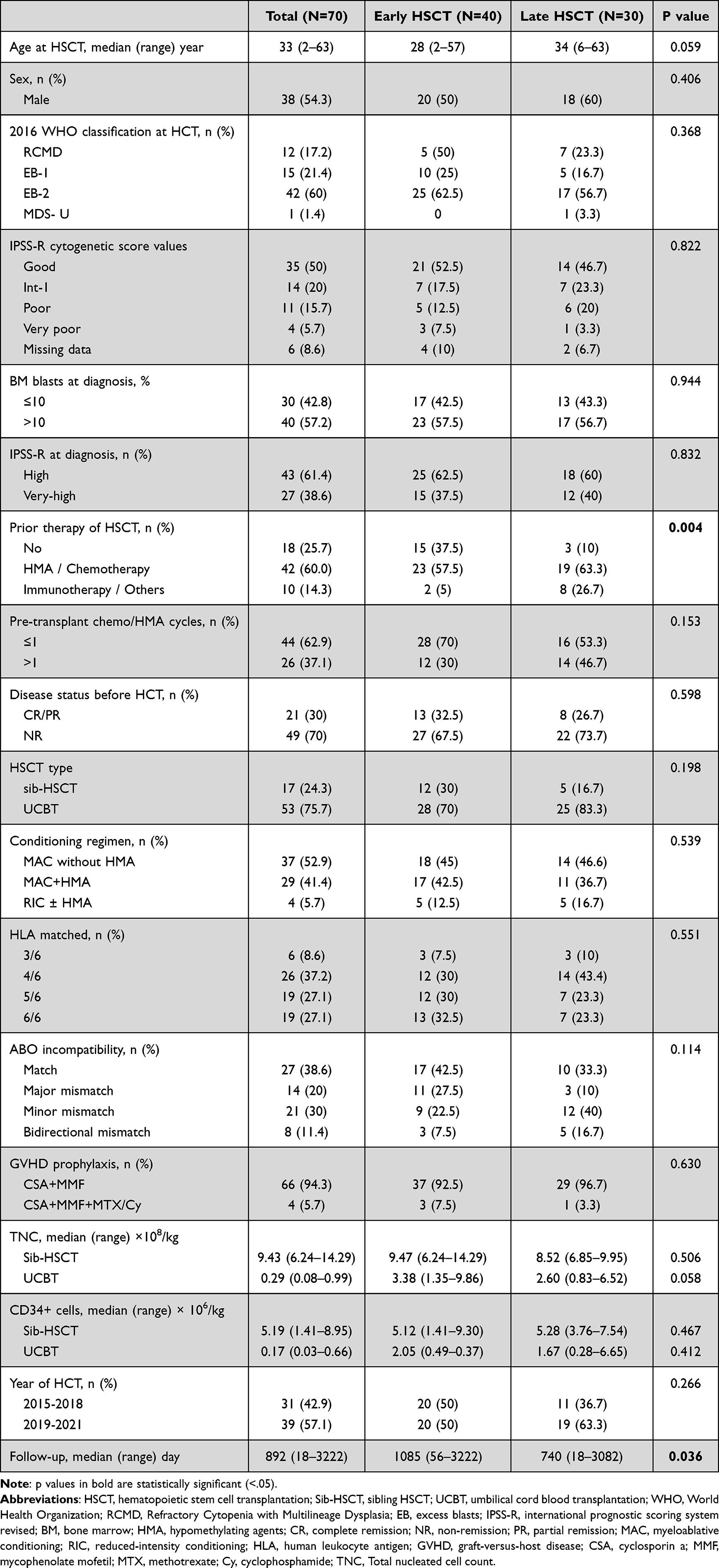 |
Table 1 Patient and Transplantation Characteristics |
Most patients were diagnosed with Refractory Anemia with Excess Blasts (RAEB)-1 or RAEB-2, had received fewer than two treatment cycles (chemotherapy or HMA), underwent HSCT within 6 months of diagnosis, received UCBT, followed a myeloablative conditioning regimen, and used combined GVHD prophylaxis with CSA and MMF. 10 patients (14.3%) received 4 or more cycles of chemotherapy/HMA before transplantation, of whom 6 (60%) achieved CR. The UCBT group had significantly lower counts of total nucleated cells and CD34+ cells infused compared to the sibling-HSCT group (p < 0.001). None of the patients received anti-thymocyte globulin during the whole period.
All patients were primarily analyzed within three subgroups: (1) based on whether HSCT was performed early after diagnosis (“early HSCT” < 6 months) or later (“later HSCT” ≥ 6 months); (2) based on the number of chemotherapy/HMA treatments prior to HSCT, categorized as “fewer treatment” (< 2 cycles) or “more treatment” (≥ 2 cycles) groups; and (3) based on pre-transplant remission status, categorized as “remission” (CR/PR) or “non-remission” (NR) groups.
Comparative analysis between the “early HSCT” and “later HSCT” subgroups demonstrated comparable baseline characteristics, with the exception of prior therapy of HSCT and follow-up duration. All other baseline clinical and laboratory parameters were well-balanced between groups (Table 1).
3-Year OS and 3-Year TRM
The 3-year OS rate was significantly higher in the “early HSCT” group compared to the “later HSCT” group (70% vs 50%, p = 0.05; Figure 1A). However, no significant difference in 3-year OS was observed between the “fewer treatment” and “more treatment” groups (57.2% vs 63.6%, p = 0.666; Figure 1D), nor between the “CR/PR” and “NR” groups (66.0% vs 59.2%, p = 0.387; Figure 1G). Similarly, the 3-year TRM rate was significantly lower in the “early HSCT” group than in the “later HSCT” group (22.7% vs 46.5%, p = 0.0205; Figure 1B). No significant differences in 3-year TRM were found between the other subgroups (34.1% vs 38.2%, p = 0.802, and 23.8% vs 36.7%, p = 0.209; Figure 1E and H, respectively). Additionally, no significant differences were observed in 3-year OS or TRM between the sibling-HSCT and UCBT groups (Figure 2A and B). Multivariate analysis identified the time from diagnosis to HSCT as the only factor significantly influencing both 3-year OS and TRM (HR 2.84 [1.22–6.63], p = 0.01, and HR 3.21 [1.29–7.94], p = 0.01; Table 2).
 |
Table 2 Multivariate Analysis of 3-year OS, 3-year TRM and 3-year Relapse |
 |
Figure 1 Three-year cumulative incidence of OS, TRM, and relapse stratified by: (A–C) Diagnosis-to-transplant interval; (D–F) Pretransplant treatment cycles; (G–I) Remission status at transplantation. |
 |
Figure 2 Outcomes stratified by HSCT type: (A) 3-year OS; (B) 3-year TRM; (C) 3-year relapse incidence; (D) 100-day grade III–IV aGVHD; (E) 3-year cGVHD; (F) 3-year GRFS. |
In multivariate analysis, parameters such as bone marrow blasts ≥10% and poor or worse cytogenetic status were not significant predictors of 3-year OS, TRM, or relapse. Likewise, variables including HSCT type, bone marrow blasts at diagnosis, number of prior chemotherapy / HMA cycles, pre-transplant remission status, cytogenetic risk, interval from diagnosis to HSCT, and HSCT year did not significantly impact 3-year OS or GRFS (Table 2).
3-Year Relapse Rate
The 3-year relapse rate was significantly higher in the “more treatment” group than the “fewer treatment” group (15.4% vs 2.3%, p = 0.0403; Figure 1F). No significant differences were observed in the other subgroup analyses (Figure 1C and I) or between the two types of HSCT (Figure 2C). In the multivariate analysis, none of the parameters showed a significant association with the 3-year relapse rate (Table 2).
Sib-HSCT vs UCBT Subgroups
In the UCBT group, 88.7% (47/53) of patients achieved neutrophil engraftment, with a median engraftment time of 17 days (range: 11–41 days), compared to 100% in the sib-HSCT group with a median of 12 days (range: 9–20 days) (p < 0.001). 69.8% (37/53) of UCBT patients achieved platelet engraftment, with a median time of 38 days (range: 14–134 days), while 100% of the sib-HSCT group with a median of 14 days (range: 11–26 days) (p < 0.001). Five patients in the UCBT group who experienced engraftment failure were rescued through second transplantation (4 haplo and 1 UCBT). Additionally, the incidence of grade III–IV aGVHD within 100 days was higher in the UCBT group compared to the sib-HSCT group, but the difference was not statistically significant (17.0% vs 0%, p = 0.717). However, the 3-year incidence of cGVHD was significantly lower in the UCBT group compared to the sibling-HSCT group and the 3-year GRFS was comparable for both subgroups (Figure 2A–F).
Causes of Death
During the follow-up period, a total of 30 patients passed away, including 7 cases (41.2%) in the sib-HSCT group and 23 cases (43.4%) in the UCBT group. The primary cause of death was infection, which accounted for 11 cases (36.7% of all deaths), multi-organ failure in 8 patients (26.6%), and relapse and GVHD, which caused 5 (16.7%) and 4 (13.3%) deaths, respectively. Early deaths occurred in 18 patients within 180 days post-transplant, with 14 cases (77.8%) resulted from infection or organ failure.
Discussion
Consistent with findings from numerous retrospective studies, our results suggest that higher-risk MDS patients should undergo allo-HSCT as early as possible after diagnosis. Attempts to achieve CR or multiple pre-transplant treatments did not confer additional benefits. In fact, patients who underwent multiple treatment cycles exhibited a higher relapse rate. Some studies indicate that reducing blasts prior to HSCT may correlate with improved prognosis. For instance, Warlick et al reported that MDS patients who achieved CR or had bone marrow blasts <5% before transplantation experienced a lower 1-year cumulative relapse rate compared to those with 5%-20% blasts (18% vs 35%, p = 0.07).12 Ryotaro et al analyzed newly diagnosed intermediate-2 or high-risk MDS patients, revealing that the HSCT group had significantly superior 3-year OS and leukemia-free survival compared to those who did not undergo HSCT (increased by 21.3%, p < 0.001, and 15.2%, p = 0.003, respectively). This survival advantage in the HSCT group was consistent across all subgroups, including age (< 65 vs ≥65 years), performance status, IPSS score, IPSS-R score, disease duration (<3 vs ≥3 months), and response to HMAs (any vs no response).13 Gregory et al conducted a prospective observational study on advanced MDS patients and found that “early HSCT” (<5 months post-diagnosis) significantly reduced mortality compared to those who did not undergo HSCT (HR 0.53, p = 0.006). In contrast, “delayed HSCT” (≥5 months post-diagnosis) did not demonstrate a significant difference in mortality (HR 1.17, p = 0.49). The OS for patients undergoing early HSCT or HSCT at CR was significantly better than for those in the non-HSCT group or those who underwent delayed HSCT without achieving CR (p = 0.01). Both early HSCT and delayed HSCT with CR were associated with a lower risk of mortality (HR 0.52, p = 0.004). Subgroup analyses indicated that patients with high-risk cytogenetics, intermediate-2 or high IPSS scores, and poor-risk MDS derived significant benefits from HSCT.14 Alzahrani et al found that patients with <5% blasts before HSCT had a relapse rate of 23%, compared to 69% for those with 5%-20% blasts and 66% for those with >20% blasts (p = 0.0004).15 Similarly, Schroeder et al compared outcomes of advanced MDS or secondary acute myeloid leukemia patients who were untreated, underwent chemotherapy (Cyclophosphamide), or HMA treatment before HSCT, finding no significant differences in 5-year OS, relapse-free survival, or relapse rates. For patients who proceeded directly to HSCT, blast levels prior to HSCT (>10% vs <10%) did not significantly impact OS or relapse-free survival.16 Overall, these findings support the notion that for higher-risk MDS patients, the advantages of early HSCT or achieving CR prior to transplantation are considerable.
In our study, the low relapse rate observed is attributed to the fact that most patients (94.3%) received myeloablative conditioning without antithymocyte globulin. This approach enhanced the graft-versus-leukemia effect following UCBT, facilitating earlier and more sustained clearance of residual tumor cells.17 Furthermore, the incidence of cGVHD was lower in the UCBT group, which is critical for improving patients’ quality of life and facilitating better reintegration into society. We conducted a retrospective analysis of immune profiles in 1945 post-transplant patients, utilizing six parameters—neutrophil, total lymphocyte, natural killer (NK), total T, CD4+ T, and B cell counts in peripheral blood—to predict early mortality (within 91–180 days after allo-HSCT). This analysis led to the development of a Composite Immune Risk Score, which demonstrated a significant correlation between higher scores and increased early mortality risk. Notably, we observed that NK, CD4+ T, and B cell counts reached significantly higher levels in the UCBT group compared to other transplant types, while CD8+ T cell counts did not show significant differences. NK cell levels in the UCBT group rapidly reconstituted during the early post-transplant period (within 30 days), potentially explaining the reduced incidence of cGVHD observed in these patients.18 Both mouse and human allo-HSCT studies have confirmed that donor NK cells can modulate GVHD by exerting cytotoxic functions against activated alloreactive T cells.19,20 Anushruti et al demonstrated that cord blood contains a high abundance of regulatory B cells (Bregs) after UCBT, with a robust recovery of Bregs observed in UCBT patients. This recovery included higher frequencies and absolute numbers of Bregs, which displayed strong inhibitory activity against allogeneic CD4+ T cells in vitro, a response not seen in cGVHD patients.21 Additionally, we found that the absolute counts and proportions of B cells and Breg cells in the UCBT group were higher than in patients receiving peripheral blood HSCT. Notably, Breg cells in the non-cGVHD group consistently exceeded those in the moderate to severe cGVHD group, suggesting that Bregs may reduce the occurrence of cGVHD.22 Together, these findings highlight a rich source of Bregs and suggest a protective role for CB-derived Bregs against the development of cGVHD in cord blood recipients. Our retrospective study demonstrated that post-transplant bone marrow recovery does not require a specific CD34+ cell threshold. We found a nearly linear correlation between log2 (CD34+/blood volume) and neutrophil recovery time.23 Additionally, in cases where HLA mismatches were ≤3/10, a CD34+ cell dosage of less than 0.83 × 105/kg was still acceptable without negatively impacting survival outcomes.24 These findings offer crucial insights for clinicians, providing greater confidence in selecting suitable cord blood units for transplantation.
However, we observed a notable incidence of early mortality, largely attributed to infections and organ failure. Many patients had transfusion dependence before transplantation, leading to significantly elevated serum ferritin levels (>1000 ng/mL) and insufficient iron chelation therapy. Iron overload has been linked to complications such as organ dysfunction, secondary infections, and transplant failure.25,26 Hence, we recommend maintaining iron chelation therapy for higher-risk MDS patients with iron overload both before and after transplantation to mitigate these risks.
Our study encompasses several critical limitations that warrant explicit discussion: (1) The retrospective analysis was conducted at a single institution, which may introduce selection bias and limit generalizability. The relatively small cohort size inherently restricts statistical power, particularly for subgroup analyses of high-risk genetic subsets. (2) Missing information on patients’ performance status (eg, ECOG score) and specific genetic mutations (eg, TP53, SF3B1, RAS mutations) hinders precise risk stratification. Additionally, incomplete data on pre-transplant blast counts and newly acquired somatic mutations may obscure their impact on transplant outcomes. (3) Inherent limitations of retrospective analysis include unmeasured confounders (eg, socioeconomic factors affecting treatment access), temporal biases (eg, evolving transplant protocols during the study period), and selection of healthier patients in the early transplant cohort. (4) The study included a small proportion of patients aged >65 years, precluding robust conclusions on UCBT efficacy in elderly high-risk MDS populations.
Based on our retrospective analysis, the observed association between earlier transplantation and improved outcomes in higher-risk MDS patients warrants further investigation in prospective studies, particularly considering potential selection biases in our cohort. The data suggest that prolonged pre-transplant treatment may not confer significant benefits, though this finding requires validation in randomized controlled trials. For carefully selected patients without HLA-matched donors, UCBT could be considered as a potential option after thorough evaluation of individual patient characteristics, including disease status, comorbidities, and treatment goals.
Ethics Statement
This study was approved by the ethical committee of the Anhui Provincial Hospital Affiliated to University of Science and Technology of China.
Acknowledgments
We thank all the patients who gave consent to disclose their medical records and answered our review calls.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; L.G., E.C and Y.J. took part in drafting, revising or critically reviewing the article; Z.S. gave final approval of the version to be published; All authors have agreed on the journal to which the article has been submitted; and Z.S. agree to be accountable for all aspects of the work.
Funding
This work was supported in part by grants from the National Natural Science Foundation of China (grant number: 81470350), the Fundamental Research Funds for the Central Universities (grant number: WK9110000001).
Disclosure
This paper is available as a preprint on Research Square at https://www.researchsquare.com/article/rs-5313687/v1. The authors report no conflicts of interest in this work.
References
1. Bernard E, Tuechler H, Greenberg PL, et al. Molecular international prognostic scoring system for myelodysplastic syndromes. NEJM Evid. 2022;1(7):EVIDoa2200008. doi:10.1056/EVIDoa2200008
2. Versluis J, Saber W, Tsai HK, et al. Allogeneic hematopoietic cell transplantation improves outcome in myelodysplastic syndrome across high-risk genetic subgroups: genetic analysis of the blood and marrow transplant clinical trials network 1102 study. J Clin Oncol. 2023;41(28):4497–4510. doi:10.1200/JCO.23.00866
3. De Witte T, Bowen D, Robin M, et al. Allogeneic hematopoietic stem cell transplantation for MDS and CMML: recommendations from an international expert panel. Blood. 2017;129(13):1753–1762. doi:10.1182/blood-2016-06-724500
4. Gagelmann N, Eikema DJ, Stelljes M, et al. Optimized EBMT transplant-specific risk score in myelodysplastic syndromes after allogeneic stem-cell transplantation. Haematologica. 2019;104(5):929–936. doi:10.3324/haematol.2018.200808
5. Shaffer BC, Ahn KW, Hu Z, et al. Scoring system prognostic of outcome in patients undergoing allogeneic hematopoietic cell transplantation for myelodysplastic syndrome. J Clin Oncol. 2016;34(16):1864–1871. doi:10.1200/JCO.2015.65.0515
6. Ciurea SO, Chilkulwar A, Saliba RM, et al. Prognostic factors influencing survival after allogeneic transplantation for AML/MDS patients with TP53 mutations. Blood. 2018;131(26):2989–2992. doi:10.1182/blood-2018-02-832360
7. Hellstrom-Lindberg ES, Kroger N. Clinical decision-making and treatment of myelodysplastic syndromes. Blood. 2023;142(26):2268–2281. doi:10.1182/blood.2023020079
8. Alessandrino EP, Porta MG, Malcovati L, et al. Optimal timing of allogeneic hematopoietic stem cell transplantation in patients with myelodysplastic syndrome. Am J Hematol. 2013;88(7):581–588. doi:10.1002/ajh.23458
9. DeFilipp Z, Ciurea SO, Cutler C, et al. Hematopoietic cell transplantation in the management of myelodysplastic syndrome: an evidence-based review from the American society for transplantation and cellular therapy committee on practice guidelines. Transpl Cell Ther. 2023;29(2):71–81. doi:10.1016/j.jtct.2022.11.014
10. Gerds AT, Woo AK, Hu ZH, et al. Outcomes after umbilical cord blood transplantation for myelodysplastic syndromes. Biol Blood Marrow Tr. 2017;23(6):971–979. doi:10.1016/j.bbmt.2017.03.014
11. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the world health organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391–2405. doi:10.1182/blood-2016-03-643544
12. Warlick ED, Cioc A, Defor T, Dolan M, Weisdorf D. Allogeneic stem cell transplantation for adults with myelodysplastic syndromes: importance of pretransplant disease burden. Biol Blood Marrow Tr. 2009;15(1):30–38. doi:10.1016/j.bbmt.2008.10.012
13. Nakamura R, Saber W, Martens MJ, et al. Biologic assignment trial of reduced-intensity hematopoietic cell transplantation based on donor availability in patients 50-75 years of age with advanced myelodysplastic syndrome. J Clin Oncol. 2021;39(30):3328–3339. doi:10.1200/JCO.20.03380
14. Pawlyn C, Cairns D, Menzies T, et al. Autologous stem cell transplantation is safe and effective for fit older myeloma patients: exploratory results from the Myeloma XI trial. Haematologica. 2022;107(1):231–242. doi:10.3324/haematol.2020.262360
15. Alzahrani M, Power M, Abou MY, et al. Improving revised international prognostic scoring system pre-allogeneic stem cell transplantation does not translate into better post-transplantation outcomes for patients with myelodysplastic syndromes: a single-center experience. Biol Blood Marrow Tr. 2018;24(6):1209–1215. doi:10.1016/j.bbmt.2018.02.007
16. Schroeder T, Wegener N, Lauseker M, et al. Comparison between upfront transplantation and different pretransplant cytoreductive treatment approaches in patients with high-risk myelodysplastic syndrome and secondary acute myelogenous leukemia. Biol Blood Marrow Tr. 2019;25(8):1550–1559. doi:10.1016/j.bbmt.2019.03.011
17. Zheng CC, Zhu XY, Tang BL, et al. Clinical separation of cGvHD and GvL and better GvHD-free/relapse-free survival (GRFS) after unrelated cord blood transplantation for AML. Bone Marrow Transpl. 2017;52(1):88–94. doi:10.1038/bmt.2016.182
18. Yu H, Liu S, Wu Z, Gao F. GNAI2 is a risk factor for gastric cancer: study of tumor microenvironment (TME) and establishment of immune risk score (IRS). Oxid Med Cell Longev. 2022;2022(1):1254367. doi:10.1155/2022/1254367
19. Hattori N, Nakamaki T. Natural killer immunotherapy for minimal residual disease eradication following allogeneic hematopoietic stem cell transplantation in acute myeloid leukemia. Int J Mol SCI. 2019;20(9):2057. doi:10.3390/ijms20092057
20. Sheng L, Mu Q, Wu X, et al. Cytotoxicity of donor natural killer cells to allo-reactive t cells are related with acute graft-vs.-host-disease following allogeneic stem cell transplantation. Front Immunol. 2020;11:1534. doi:10.3389/fimmu.2020.01534
21. Sarvaria A, Basar R, Mehta RP, et al. IL-10+ regulatory B cells are enriched in cord blood and may protect against cGVHD after cord blood transplantation. Blood. 2016;128(10):1346–1361. doi:10.1182/blood-2016-01-695122
22. Wang J, Pan TZ, Huang PP, Sun ZM, Zhu HP. Correlation between immune reconstitution and chronic graft-versus-host disease after unrelated cord blood transplantation and sibling peripheral blood stem cell transplantation. Zhonghua Xue Ye Xue Za Zhi. 2021;42(6):466–473. doi:10.3760/cma.j.issn.0253-2727.2021.06.005
23. Chen J, Gale RP, Feng Y, et al. Are haematopoietic stem cell transplants stem cell transplants, is there a threshold dose of CD34-positive cells and how many are needed for rapid posttransplant granulocyte recovery? Leukemia. 2023;37(10):1963–1968. doi:10.1038/s41375-023-01973-2
24. Sun Z, Hu Y, Ji Y, et al. Refining eligibility criteria of unit selection for myeloablative cord blood transplantation in acute leukemia: real-world experience of a referral center. EJHaem. 2023;4(2):470–475. doi:10.1002/jha2.703
25. Hoeks M, Bagguley T, van Marrewijk C, et al. Toxic iron species in lower-risk myelodysplastic syndrome patients: course of disease and effects on outcome. Leukemia. 2021;35(6):1745–1750. doi:10.1038/s41375-020-01022-2
26. Penack O, Peczynski C, van der Werf S, et al. Association of serum ferritin levels before start of conditioning with mortality after alloSCT - A prospective, non-interventional study of the EBMT transplant complications working party. Front Immunol. 2020;11:586. doi:10.3389/fimmu.2020.00586
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.