Back to Journals » Journal of Pain Research » Volume 19
Optimizing Postoperative Analgesia After Perianal Abscess Surgery Using Ultrasound-Guided Pudendal Nerve Block Combined with Wrist-Ankle Acupuncture: A Randomized Controlled Trial
Authors Zhang C, Yang J ![]() , Feng L, Zhao X, Tang P
, Feng L, Zhao X, Tang P
Received 12 January 2026
Accepted for publication 6 March 2026
Published 25 March 2026 Volume 2026:19 592180
DOI https://doi.org/10.2147/JPR.S592180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Cui Zhang,1,2,* Junyi Yang,1,2,* Linhua Feng,1,2 Xizhong Zhao,1,2 Ping Tang1,2
1Department of Anorectal Surgery, Institute of Traditional Chinese Medicine, Sichuan Academy of Chinese Medicine, Chengdu, People’s Republic of China; 2Department of Anorectal Surgery, The Sichuan Second Hospital of Traditional Chinese Medicine, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Cui Zhang, Email [email protected]
Objective: To investigate the efficacy and safety of ultrasound-guided pudendal nerve block (PNB) combined with wrist-ankle acupuncture for postoperative pain management following perianal abscess surgery.
Methods: This prospective randomized controlled trial enrolled 120 patients undergoing perianal abscess surgery between January 2023 and June 2024. Patients were randomly assigned to three groups (n = 40 per group): a PNB group, a wrist–ankle acupuncture group, and a combined group (PNB plus wrist–ankle acupuncture). Visual analogue scale (VAS) pain scores at multiple postoperative time points, duration of analgesia, rescue analgesia rate, serum inflammatory markers, sleep quality, patient satisfaction, and adverse events were compared among the three groups.
Results: VAS scores at 6, 12, 24, 48, and 72 hours postoperatively were significantly lower in the combined group than in the PNB group and the wrist-ankle acupuncture group (all P < 0.01). The duration of analgesia was significantly longer in the combined group (P < 0.001), while the rescue analgesia rate was significantly lower (15.0%, P < 0.05). At 48 and 72 hours postoperatively, serum levels of C-reactive protein, interleukin-6, and tumor necrosis factor-α were significantly lower in the combined group than in either single-intervention group (all P < 0.05). In addition, postoperative sleep quality scores and patient satisfaction were significantly improved in the combined group (P < 0.05). No significant differences in the incidence of adverse events were observed among the three groups (P > 0.05).
Conclusion: Ultrasound-guided pudendal nerve block combined with wrist-ankle acupuncture provides more sustained and effective postoperative analgesia after perianal abscess surgery, attenuates inflammatory responses, improves sleep quality, and demonstrates a favorable safety profile. This combined approach may represent a promising multimodal analgesic strategy integrating conventional regional anesthesia and complementary therapy.
Trial Registration: International Traditional Medicine Clinical Trial Registry (ITMCTR). Registration No. ChiCTR-2500111901.
Clinical Trial Number: ChiCTR-2500111901.
Keywords: postoperative analgesia, pudendal nerve block, wrist-ankle acupuncture, ultrasound guidance, perianal abscess
A Letter to the Editor has been published for this article.
Introduction
Background and Rationale
Perianal abscess is a common acute suppurative infectious condition encountered in colorectal surgery, for which surgical intervention remains the primary and most effective treatment.1 Owing to the dense innervation of the perianal region, postoperative pain following perianal abscess surgery is often severe and difficult to manage.2 Inadequately controlled postoperative pain not only causes substantial physical discomfort but is also associated with sleep disturbances, reduced appetite, anxiety, depressive symptoms, and delayed mobilization. These consequences may increase the risk of postoperative complications, prolong hospital stay, and impose an additional economic burden on patients.3
A variety of analgesic strategies are currently employed in clinical practice, including nonsteroidal anti-inflammatory drugs (NSAIDs), opioid analgesics, and local infiltration anesthesia. Although NSAIDs provide moderate analgesic effects, their use is frequently limited by gastrointestinal adverse reactions, such as nausea, vomiting, abdominal pain, and diarrhea, and long-term administration may increase the risk of gastrointestinal ulceration and bleeding.4 Opioids remain effective for severe pain but are associated with well-recognized adverse effects, including respiratory depression, nausea, constipation, and the potential for dependence, which restrict their routine use.5 Local infiltration anesthesia is relatively simple to perform; however, its analgesic duration is often insufficient to meet prolonged postoperative pain control requirements. These limitations highlight the need for safer and more effective multimodal analgesic approaches for postoperative pain management after perianal surgery.6
Ultrasound-Guided Pudendal Nerve Block and Wrist-Ankle Acupuncture
Ultrasound-guided pudendal nerve block (PNB) has emerged as a targeted regional anesthesia technique capable of selectively interrupting nociceptive transmission from the perianal region.7 Compared with conventional analgesic methods, ultrasound-guided PNB allows precise localization of the pudendal nerve, resulting in improved analgesic efficacy, reduced opioid consumption, and enhanced patient satisfaction. Previous studies have demonstrated that PNB significantly lowers postoperative pain scores and delays the onset of postoperative pain following anorectal procedures.8 Nevertheless, when used alone, its analgesic duration and ability to modulate systemic inflammatory responses may be limited.
Wrist-ankle acupuncture is a minimally invasive acupuncture technique involving shallow subcutaneous stimulation of specific wrist and ankle regions. It has been increasingly applied in postoperative pain management owing to its simplicity, favorable safety profile, and minimal adverse effects.9 Clinical studies have shown that wrist-ankle acupuncture can effectively relieve postoperative pain and reduce the need for analgesic medications. The proposed mechanisms underlying its analgesic effects include modulation of neuroendocrine pathways and promotion of endogenous analgesic substances, such as endorphins and enkephalins. More broadly, acupuncture’s ability to regulate the autonomic nervous system and hypothalamic-pituitary-adrenal (HPA) axis has been demonstrated in conditions of chronic stress, such as burnout, suggesting a shared mechanism in promoting physiological homeostasis.10
Given their distinct yet potentially complementary mechanisms of action, combining ultrasound-guided PNB with wrist-ankle acupuncture may provide synergistic benefits by integrating targeted regional anesthesia with systemic pain modulation.
Current Evidence and Research Gap
In recent years, increasing attention has been directed toward the application of ultrasound-guided PNB in postoperative analgesia. International studies have reported that PNB significantly reduces postoperative pain intensity and analgesic requirements following anorectal surgery.7,8 Similar findings have been reported in domestic studies, which demonstrated that patients receiving ultrasound-guided PNB experienced lower pain scores, delayed onset of postoperative pain, reduced opioid consumption, and improved satisfaction compared with those receiving local infiltration anesthesia. Despite these advantages, the analgesic effect of PNB alone may not be sufficiently sustained, and its impact on postoperative recovery remains limited.
Substantial evidence also supports the effectiveness of wrist-ankle acupuncture in postoperative pain control.11–13 Systematic reviews and clinical studies have shown that wrist-ankle acupuncture alleviates postoperative pain and decreases analgesic drug consumption across various surgical procedures, with a low incidence of adverse events.9 However, studies specifically evaluating wrist-ankle acupuncture for postoperative pain after perianal abscess surgery are scarce, and most available evidence focuses on its use as a single intervention.
At present, clinical research investigating the combined use of ultrasound-guided PNB and wrist-ankle acupuncture for postoperative analgesia is limited, and evidence in the context of perianal abscess surgery is lacking. Whether this combined approach can provide superior analgesic efficacy and improve postoperative recovery outcomes remains unclear.
Objectives and Novelty of the Study
The present study aimed to evaluate the efficacy and safety of ultrasound-guided pudendal nerve block combined with wrist-ankle acupuncture for postoperative analgesia after perianal abscess surgery through a prospective randomized controlled trial. Specifically, we compared pain intensity at multiple postoperative time points, duration of analgesia, rescue analgesia requirements, inflammatory marker levels, sleep quality, and adverse events among patients receiving combined therapy and those receiving either intervention alone.
The novelty of this study lies in two aspects. First, to our knowledge, this is the first randomized controlled trial to investigate the combined application of ultrasound-guided PNB and wrist-ankle acupuncture for postoperative pain management in patients undergoing perianal abscess surgery. Second, by systematically evaluating both subjective pain outcomes and objective inflammatory markers, this study provides comprehensive evidence supporting a multimodal analgesic strategy that integrates conventional regional anesthesia with complementary therapy, thereby offering a clinically applicable approach to optimizing postoperative pain control.
Materials and Methods
Study Design and Participants
This prospective randomized controlled trial was conducted at our institution between January 2024 and December 2024. A total of 120 patients scheduled for perianal abscess surgery were enrolled according to predefined eligibility criteria. Prior to enrollment, all participants were fully informed about the study objectives, procedures, potential risks, and benefits, and written informed consent was obtained from each participant. Using a random number table, patients were randomly allocated in a 1:1:1 ratio to one of three groups: the pudendal nerve block (PNB) group, the wrist-ankle acupuncture group, and the combined group (PNB plus wrist-ankle acupuncture), with 40 patients in each group.
Baseline characteristics, including sex, age, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status, and abscess type, were comparable among the three groups, with no statistically significant differences observed (all P > 0.05; Table 1).
 |
Table 1 Comparison of Baseline Characteristics Among the Three Groups (n = 40) |
Inclusion and Exclusion Criteria
Inclusion Criteria
- Patients were eligible for inclusion if they met the following criteria: (1) Aged 18–65 years;
- Scheduled for surgical treatment of perianal abscess;
- Diagnosis confirmed by preoperative pelvic magnetic resonance imaging (MRI) in accordance with the Chinese Expert Consensus on the Clinical Diagnosis and Treatment of Perianal Abscess;
- ASA physical status class I–III;
- No previous history of pelvic or gluteal surgery or pudendal nerve block; and
- Provision of written informed consent by the patient and family members.
This study was approved by the Medical Ethics Committee of the Second Hospital of Traditional Chinese Medicine of Sichuan Province and registered with the Chinese Clinical Trial Registry (ChiCTR-2500111901).
Exclusion Criteria
Exclusion criteria were as follows:
- Allergy or intolerance to local anesthetics (ropivacaine);
- Coagulation disorders or infection at the puncture site;
- Pelvic MRI findings suggestive of supralevator or pelvirectal abscess;
- Concomitant anorectal diseases, such as anal fissure, anal fistula, or enteritis;
- Long-term use of analgesics or presence of chronic pain disorders;
- Severe cardiovascular, cerebrovascular, hepatic, renal, or immune system diseases; and
- Inability to cooperate with postoperative pain assessment or presence of cognitive impairment.
Anesthesia, Surgery, and Analgesic Interventions
Anesthesia and Surgical Procedure
All patients underwent surgery under combined spinal-epidural anesthesia. Surgical procedures were performed by the same team of senior colorectal surgeons following standardized operative protocols. Surgical duration and extent of tissue trauma were controlled as consistently as possible to minimize confounding effects related to surgical variability and to ensure that postoperative outcomes primarily reflected the analgesic interventions.
Analgesic Interventions
Pudendal Nerve Block Group
In the PNB group, bilateral ultrasound-guided pudendal nerve block was performed at the end of surgery. Patients were placed in the prone jackknife position. A color Doppler ultrasound system (Affiniti 30; Philips Medical Systems, Suzhou, China) equipped with a 2–5 MHz linear probe was used. The probe was initially positioned at the midpoint of the line connecting the greater trochanter and the posterior superior iliac spine to identify the hyperechoic iliac bone line. The probe was then moved parallel to the sacrum toward the lesser sciatic notch. When the hyperechoic line was interrupted, the probe was translated from the greater sciatic notch toward the ischial spine and then to the lesser sciatic notch. The sacrospinous and sacrotuberous ligaments were identified as a hyperechoic interligamentous plane. The probe was further adjusted to visualize the proximal portion of the pudendal canal (Alcock’s canal), where the pudendal nerve or pudendal vessels could be identified. The anatomical landmarks and ultrasound localization of the pudendal nerve are illustrated in Figure 1A and B.
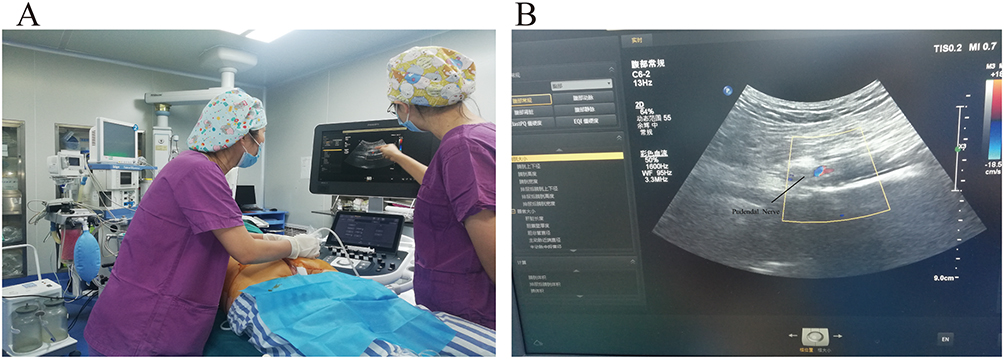 |
Figure 1 Ultrasound-Guided Pudendal Nerve Block: Localization and Nerve Block Anesthesia. (A) Schematic Diagram of Ultrasound-Guided Pudendal Nerve Block. (B) Ultrasound-guided pudendal nerve localization. |
After negative aspiration, 10 mL of 0.3% ropivacaine (10 mL:100 mg; batch No. H20183152; Ruiyang Pharmaceutical Co., Ltd., China) was slowly injected under ultrasound guidance, and adequate spread of the local anesthetic around the target area was confirmed. The same procedure was performed contralaterally.
Wrist-Ankle Acupuncture Group
In the wrist-ankle acupuncture group, treatment was initiated 6 hours postoperatively. Bilateral lower area 6 (primary points) and lower area 1 (auxiliary points) were selected. After skin disinfection, disposable sterile intradermal needles (Qingling Co., Ltd., Japan; registration No. 20162271259) were inserted subcutaneously with a shallow oblique technique to a depth of approximately 1.4 cun, with the needle direction oriented proximally. The anatomical location and needling process of wrist-ankle acupuncture are shown in Figure 2A–F.
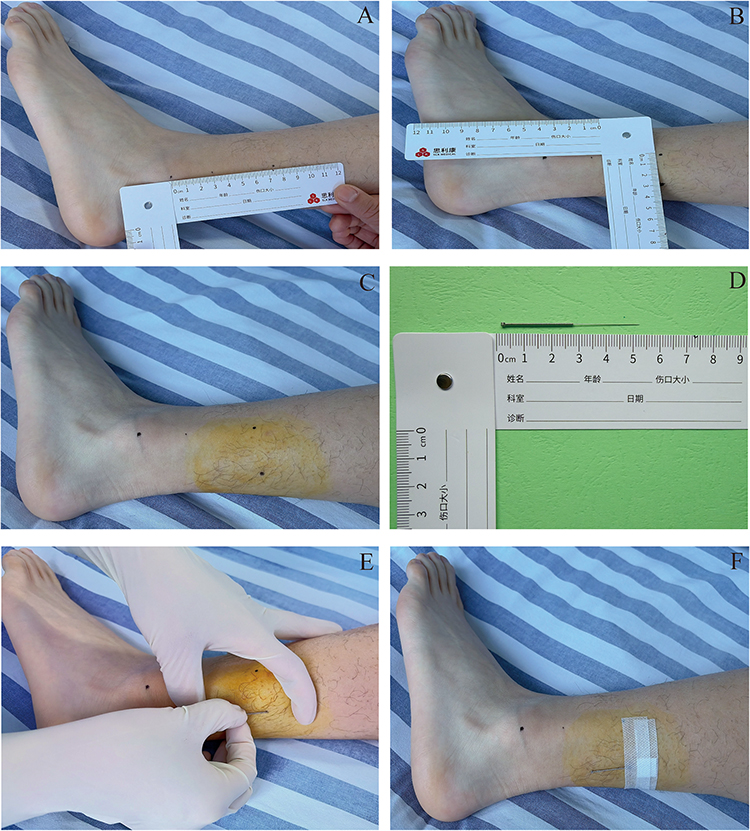 |
Figure 2 Wrist-Ankle Acupuncture: Location and Needling Process. (A–C) Wrist-Ankle Acupuncture Needling Technique Location Diagram. (D) Wrist-Ankle Acupuncture Needle, 2.5cm in length. (E and F) Wrist-Ankle Acupuncture Needling Procedure. |
The absence of strong soreness, numbness, or distension was considered appropriate. Needles were retained for 30 minutes and could be extended to several hours if pain was pronounced. Treatment was administered once daily for 7 consecutive days.
Combined Group
Patients in the combined group received both ultrasound-guided pudendal nerve block and wrist-ankle acupuncture, using the same procedures as described for the respective single-intervention groups.
Rescue Analgesia
Rescue analgesia was administered when patients reported severe pain, defined as a VAS score ≥ 7. In such cases, oral tramadol hydrochloride sustained-release tablets (0.1 g; Farmaceutici Formenti S.p.A., Italy; registration No. H20140977) were provided. The number of rescue analgesic administrations and total dosage were recorded.
Outcome Measures
Primary Outcomes
Pain intensity: Postoperative pain was assessed using the visual analogue scale (VAS) at 6, 12, 24, 48, and 72 hours after surgery. The VAS ranged from 0 (no pain) to 10 (worst imaginable pain).
Duration of analgesia: Defined as the time interval from completion of the analgesic intervention to the first report of a VAS score ≥ 4.
Rescue analgesia rate: The proportion of patients requiring rescue analgesia and the number of rescue analgesic administrations within 72 hours postoperatively.
Secondary Outcomes
Inflammatory markers: Venous blood samples were collected preoperatively and at 48 and 72 hours postoperatively. Serum levels of C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α) were measured using enzyme-linked immunosorbent assay (ELISA).
Sleep quality: Sleep quality was assessed preoperatively and at 72 hours postoperatively using the Pittsburgh Sleep Quality Index (PSQI), which comprises seven components with a total score ranging from 0 to 21, with higher scores indicating poorer sleep quality.
Postoperative complications: Postoperative complications, including urinary retention, vascular puncture injury, and nerve injury, were recorded. Planned telephone follow-up was conducted on postoperative day 7 to assess delayed complications, such as persistent numbness or deep or incisional infection.
Patient satisfaction: Patient satisfaction with postoperative analgesia was evaluated at 72 hours using a 5-point Likert scale, ranging from 1 (very dissatisfied) to 5 (very satisfied).
Statistical Analysis
Statistical analyses were performed using SPSS software (version 25.0; IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation and were compared using one-way analysis of variance (ANOVA). Repeated-measures ANOVA was used for longitudinal data. Categorical variables are expressed as frequencies or percentages and were compared using the chi-square test or Fisher’s exact test, as appropriate. A two-sided P value < 0.05 was considered statistically significant.
Results
Comparison of Analgesic Outcomes Among the Three Groups
VAS pain scores at all postoperative time points (6, 12, 24, 48, and 72 hours) were significantly lower in the combined group than in both the PNB group and the wrist-ankle acupuncture group (all P < 0.01). In addition, the duration of analgesia was significantly longer in the combined group compared with the other two groups (P < 0.001).
The rescue analgesia rate in the combined group was 15.0%, which was significantly lower than that observed in the PNB group (37.5%) and the wrist-ankle acupuncture group (32.5%) (P < 0.05). Similarly, the number of rescue analgesic administrations was significantly reduced in the combined group compared with the single-intervention groups (Table 2).
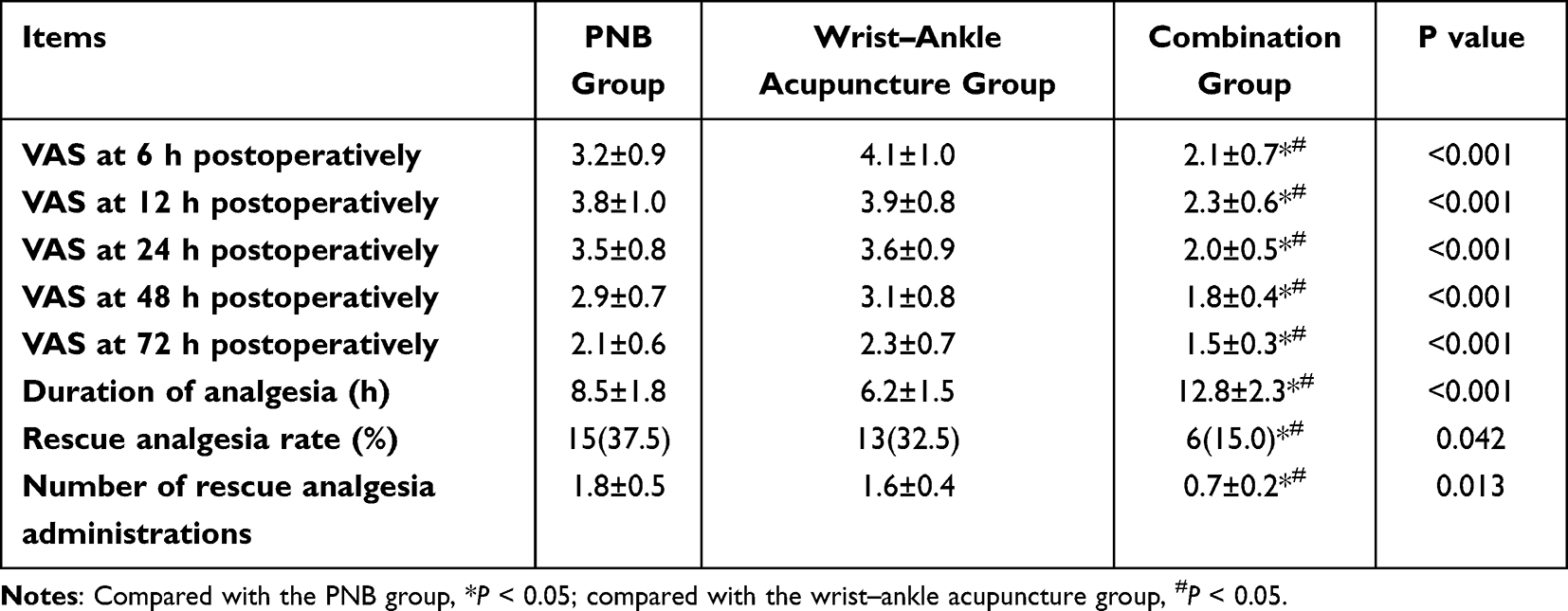 |
Table 2 Comparison of postoperative analgesic outcomes among the three groups (n = 40) |
Comparison of Inflammatory Marker Levels
Serum levels of C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α) increased at 48 and 72 hours postoperatively in all three groups compared with preoperative values. However, the magnitude of increase was significantly lower in the combined group than in the PNB group and the wrist-ankle acupuncture group at both postoperative time points (all P < 0.05) (Table 3).
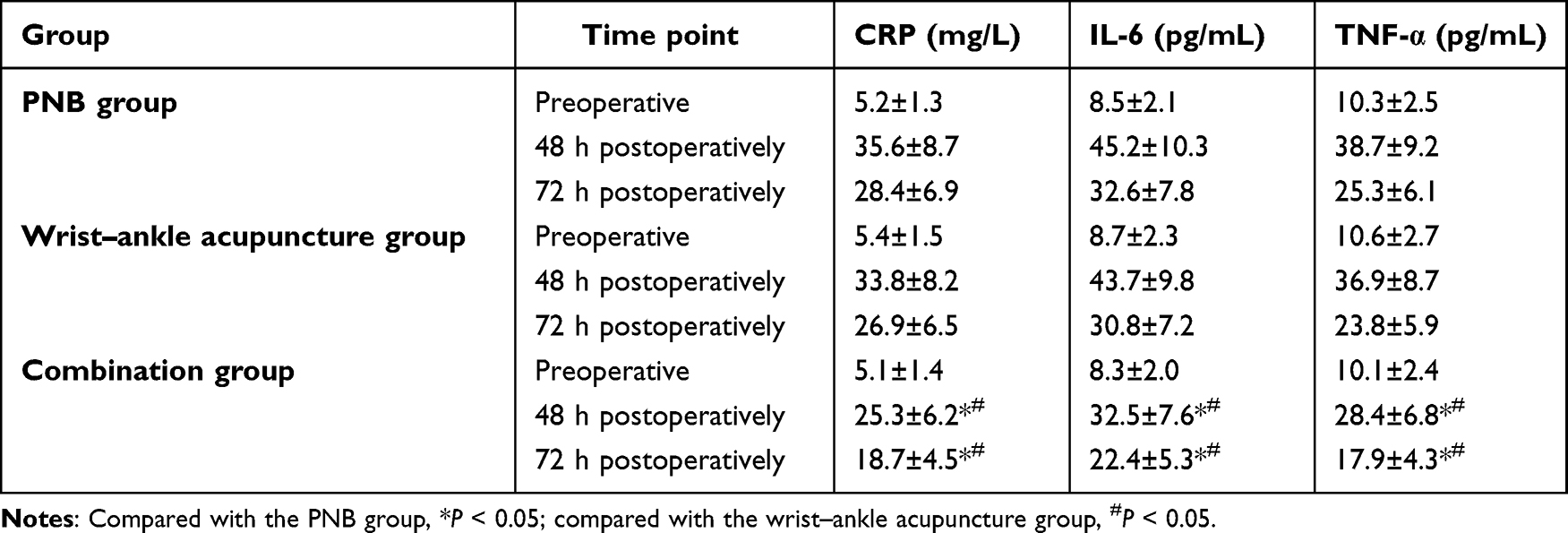 |
Table 3 Comparison of Inflammatory Factor Levels Among the Three Groups (n = 40, Mean ± SD) |
Sleep Quality, Patient Satisfaction, and Adverse Events
At 72 hours postoperatively, the Pittsburgh Sleep Quality Index (PSQI) scores were significantly lower in the combined group than in the PNB group and the wrist-ankle acupuncture group (P < 0.05), indicating better sleep quality. Patient satisfaction scores were also significantly higher in the combined group compared with the other two groups (P < 0.05).
No statistically significant differences were observed among the three groups with respect to the incidence of adverse events (P > 0.05). Detailed outcomes are presented in Table 4.
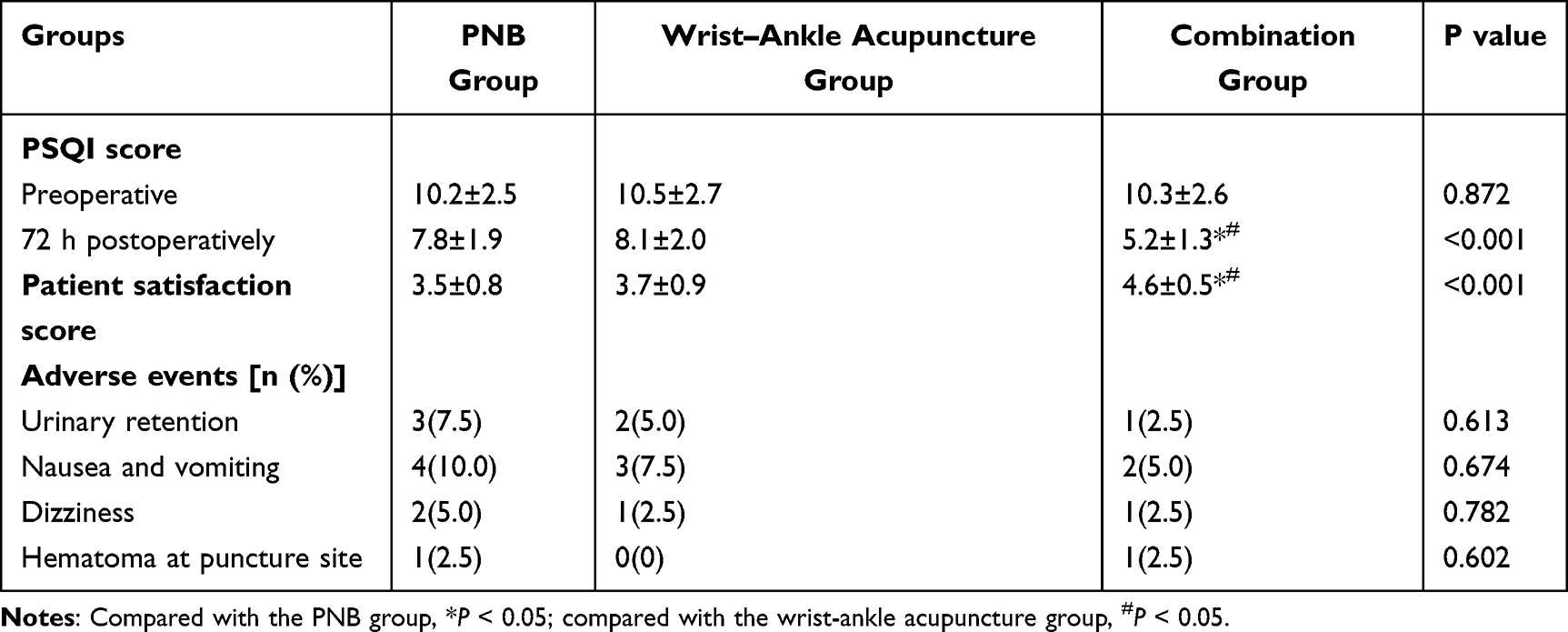 |
Table 4 Comparison of Sleep Quality, Patient Satisfaction, and Adverse Events Among the Three Groups (n = 40) |
Surgery-Related Economic and Time Indicators
To evaluate the impact of different analgesic regimens on surgical resource utilization, this study compared medical supply costs, labor costs, and total operation time among the three groups. Medical supply costs included the expenses of analgesia-related consumables (eg., puncture needles, local anesthetics, acupuncture needles, etc). Labor costs were calculated based on the number of medical staff required for the procedure and the operation time, converted according to the average wage standard of our hospital. Total operation time was defined as the duration from the start of anesthesia to the end of surgery. All cost data were calculated in Renminbi (CNY), and statistical analysis was performed using the independent samples t-test.
The results showed that the total medical supply cost in the combination group was slightly higher than that in the PNB group and the wrist-ankle acupuncture group (P < 0.05), primarily due to the concurrent use of two analgesic techniques in the combination group. Regarding labor costs, the combination group was slightly higher than the wrist-ankle acupuncture group, but showed no significant difference compared with the PNB group (P > 0.05). There were no significant differences in total operation time among the three groups (P > 0.05), indicating that the combined analgesic procedure did not significantly prolong operating room occupancy time (Table 5).
 |
Table 5 Comparison of Surgery-Related Economic and Time Indicators Among the Three Groups (n = 40, Mean ± SD) |
Discussion
Synergistic Effects of the Combined Analgesic Strategy
In this prospective randomized controlled trial, we demonstrated that the combination of ultrasound-guided pudendal nerve block and wrist-ankle acupuncture provided superior postoperative analgesia following perianal abscess surgery compared with either intervention alone. The combined approach resulted in lower pain intensity, prolonged analgesic duration, reduced rescue analgesia requirements, attenuation of postoperative inflammatory responses, and improved sleep quality, without an increase in adverse events.6,7 These findings support the clinical value of a multimodal analgesic strategy integrating regional anesthesia with complementary therapy.8
The observed synergistic effects may be explained by the complementary mechanisms of the two interventions. Pudendal nerve block provides targeted regional analgesia by interrupting nociceptive transmission from the perianal region through the administration of ropivacaine, which stabilizes neuronal membranes and inhibits sodium ion influx, thereby preventing action potential generation and propagation.14 This mechanism effectively controls incision-related nociceptive input.
In contrast, wrist-ankle acupuncture is thought to exert analgesic effects through modulation of central and peripheral nervous system activity. Previous studies have suggested that this technique may activate endogenous analgesic pathways and promote the release of endogenous opioids, such as β-endorphins and enkephalins, which act on opioid receptors in both the central and peripheral nervous systems.9,12 In addition, wrist-ankle acupuncture has been reported to influence autonomic nervous system activity, which may contribute to the alleviation of smooth muscle spasm and reduction of sphincter-related pain.13
Postoperative pain following perianal abscess surgery is multifactorial, involving tissue injury-related nociceptive pain, inflammation-induced pain, and sphincter spasm-associated discomfort.2,3 While pudendal nerve block primarily addresses nociceptive pain by blocking sensory nerve conduction, wrist-ankle acupuncture may provide broader systemic modulation, including attenuation of inflammatory responses and reduction of muscle spasm. The combination of these mechanisms likely accounts for the more comprehensive and sustained analgesic effect observed in the combined group.
Comparison with Previous Studies
The analgesic outcomes observed in the present study are consistent with previous reports evaluating regional nerve block and wrist-ankle acupuncture as individual interventions. Prior studies have demonstrated that ultrasound-guided pudendal nerve block significantly reduces postoperative pain scores and analgesic consumption following anorectal surgery.7,8 Our findings in the PNB group corroborate these results, while the additional improvement observed in the combined group suggests that adjunctive wrist-ankle acupuncture further enhances analgesic efficacy.
Similarly, earlier studies have reported that wrist-ankle acupuncture can accelerate pain relief and reduce postoperative analgesic requirements in patients undergoing various surgical procedures.9 In the present study, wrist-ankle acupuncture alone provided a degree of postoperative analgesia; however, the combined intervention yielded superior outcomes, highlighting the potential synergistic benefit of integrating acupuncture with regional anesthesia.
With respect to inflammatory responses, previous research has shown that pudendal nerve block may reduce postoperative inflammatory marker levels. The more pronounced reduction in CRP, IL-6, and TNF-α observed in the combined group suggests that wrist-ankle acupuncture may further modulate postoperative inflammation, possibly through neuroendocrine regulation and cytokine expression pathways.14,15 These findings align with earlier evidence indicating that acupuncture-based interventions can influence inflammatory processes.
Improvements in sleep quality and patient satisfaction observed in the combined group are also consistent with the notion that effective pain control contributes to better postoperative recovery experiences. Adequate analgesia reduces pain-related sleep disturbances and enhances overall patient comfort, which may explain the higher satisfaction scores associated with the combined approach.
Clinical Implications
The results of this study have important clinical implications for postoperative pain management after perianal abscess surgery. The combined use of ultrasound-guided pudendal nerve block and wrist-ankle acupuncture offers a feasible multimodal analgesic option that addresses both local nociceptive input and systemic pain modulation. By providing more sustained analgesia and reducing reliance on rescue analgesics,16,17 this approach aligns with enhanced recovery after surgery (ERAS) principles, which emphasize optimization of perioperative care to minimize physiological stress and promote early recovery.6,18,19
Furthermore, the favorable safety profile observed in this study suggests that the combined strategy does not increase the risk of adverse events. Both interventions are minimally invasive when performed appropriately, and ultrasound guidance enhances the precision and safety of pudendal nerve block. The relative simplicity of wrist-ankle acupuncture may facilitate its integration into routine clinical practice.
Factors Influencing Analgesic Efficacy
The findings of this study demonstrate that the combination of ultrasound-guided pudendal nerve block and wrist-ankle acupuncture provides superior postoperative analgesia compared with either intervention alone. However, it is important to recognize that the analgesic efficacy of these interventions may be influenced by patient- and disease-related factors, particularly the extent and severity of the perianal abscess.20
Impact of Abscess Extent on Analgesic Outcomes
In clinical practice, perianal abscesses vary considerably in size, depth, and anatomical involvement. Patients with large or complex abscesses typically experience more extensive tissue destruction, greater intraoperative dissection, and a more pronounced postoperative inflammatory response.21 These factors may contribute to increased baseline pain intensity and may diminish the effectiveness of regional analgesic techniques. In the present study, post hoc observations suggested that patients with larger abscesses tended to require earlier rescue analgesia and reported higher VAS scores.22,23 This finding implies that the severity of the underlying surgical condition may modulate the duration and magnitude of analgesia provided by peripheral nerve blocks and acupuncture.
Radiological Abscess Volume and Postoperative Pain
The extent of abscess involvement may represent a clinically relevant factor influencing postoperative pain intensity.24 Larger or more complex abscesses are typically associated with greater tissue destruction, more extensive surgical dissection, and heightened inflammatory responses, all of which may contribute to increased postoperative nociception.
In the present study, baseline abscess classification (low-position versus high-position abscess) was comparable among groups, suggesting that randomization likely minimized major imbalances in disease severity. However, quantitative volumetric assessment based on preoperative MRI was not incorporated into the study design. Given that radiological abscess volume may correlate with the magnitude of postoperative inflammation and pain perception, its omission represents a potential confounding factor.
Previous research has demonstrated that greater tissue injury and inflammatory burden are associated with elevated levels of pro-inflammatory cytokines such as IL-6 and TNF-α,14,15,25,26 which are closely linked to postoperative pain severity. Furthermore, studies in anorectal surgery have reported that regional anesthesia techniques may attenuate inflammatory marker elevation compared with systemic analgesia. Therefore, stratification according to abscess volume in future trials may help clarify whether the observed analgesic benefits are consistent across different levels of disease severity.
Prospective studies incorporating imaging-based volumetric analysis and predefined subgroup stratification are warranted to further delineate the interaction between abscess burden, inflammatory response, and analgesic efficacy.
Clinical Implications and Future Considerations
These observations underscore the need for individualized analgesic strategies based on the anatomical characteristics of the abscess.25–27 The potential correlation between abscess volume and postoperative pain suggests that preoperative imaging findings could be used to stratify patients according to anticipated analgesic needs. Future studies should include prespecified subgroup analyses based on abscess size and anatomical classification.
Expanding Applications of Acupuncture in Clinical Practice: From Postoperative Analgesia to Psychological Well-Being
The effects of wrist-ankle acupuncture are likely mediated by the neuroregulatory properties, including modulation of somatosensory afferent pathways and activation of endogenous analgesic systems.12,28 These mechanisms extend to broader domains of patient well-being, including psychological and occupational health. Acupuncture has been shown to influence the autonomic nervous system and HPA axis, thereby reducing stress responses.29 As highlighted by Shaska et al (2025), regular acupuncture treatment significantly reduces subjective stress levels and improves mental health in high-stress professions by restoring parasympathetic tone.10 This suggests acupuncture’s therapeutic potential extends beyond symptom management to fundamental pathways of neuroendocrine regulation.30
Applicability Analysis in Low- and Lower-Middle-Income Countries
This combined strategy demonstrates high clinical applicability in LMICs. First, equipment requirements are becoming more manageable with the availability of portable ultrasound devices.31 Wrist-ankle acupuncture requires only disposable sterile needles, making it suitable for primary healthcare facilities. Second, the procedure is relatively simple with a short training period, helping to alleviate the shortage of specialists.28 Third, while supply costs are slightly higher, the reduction in rescue analgesia and hospital stay translates into significant indirect economic benefits. This approach aligns with the WHO’s principles of “safe, effective, and economical” pain management by reducing reliance on expensive and potentially addictive opioids.5,6
Limitations and Future Directions
Several limitations of this study should be acknowledged. First, this was a single-center trial with a relatively limited sample size, which may restrict the generalizability of the findings. Multicenter studies with larger sample sizes are warranted to confirm the efficacy and safety of this combined analgesic strategy across diverse clinical settings.
Second, subgroup analyses according to abscess type and surgical complexity were not performed. Given the heterogeneity of perianal abscess presentations, future studies should investigate whether the effectiveness of the combined approach varies according to abscess location or severity.
Finally, economic evaluations were not conducted in the present study. Future research incorporating health economic analyses may help determine the cost-effectiveness of this multimodal analgesic strategy. Additional mechanistic studies exploring neurophysiological and molecular pathways may further elucidate the synergistic effects observed and support continued optimization of postoperative pain management protocols.
Conclusion
This prospective randomized controlled trial demonstrated that ultrasound-guided pudendal nerve block combined with wrist-ankle acupuncture provides superior postoperative analgesia compared with either intervention alone in patients undergoing perianal abscess surgery. The combined strategy significantly reduced postoperative pain intensity, prolonged the duration of analgesia, decreased rescue analgesic requirements, attenuated inflammatory responses, and improved sleep quality and patient satisfaction, without increasing adverse events.
These findings suggest that integrating targeted regional anesthesia with complementary neuromodulatory therapy may enhance multimodal analgesic efficacy in anorectal surgery. The combined approach appears to be safe and clinically feasible, offering an opioid-sparing option for postoperative pain management.
Further multicenter studies with larger sample sizes and predefined subgroup analyses are warranted to confirm these findings and to determine optimal patient selection strategies.
Data Sharing Statement
All shared data will be fully deidentified to protect participant privacy and confidentiality. The data and study documents will be available for 5 years from the date of the manuscript’s publication, and can be accessed by contacting the corresponding author at Cui Zhang ([email protected]). No additional ethical approval is required for data reuse, in line with the original study’s IRB/EC approval.
Ethical and Consent Statements
This study was conducted in accordance with the Declaration of Helsinki (2013 revision) and approved by the Institutional Review Board (Ethics Committee) of the Sichuan Second Hospital of traditional Chinese Medicine (Approval No. Ke 202204-28-27). Informed written consent was obtained from all eligible participants prior to their enrollment in the study, and all participants were informed of their right to withdraw from the study at any time without penalty.
Author Contributions
Junyi Yang and Cui Zhang contributed to the conception and design of the study and drafted the manuscript. Linhua Feng, Xizhong Zhao, and Ping Tang were responsible for data collection and statistical analysis. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Sichuan Administration of Traditional Chinese Medicine (Project No. 2022-4-725).
Disclosure
Cui Zhang and Junyi Yang are co-first authors for this study. The authors declare that they have no competing interests for this work.
References
1. Ghandour S, El-Boghdadly K, Elsharkawy AM, et al. Ultrasound-guided transperineal pudendal nerve block for postoperative analgesia after anorectal surgery: a randomized, double-blind, placebo-controlled trial. Br J Anaesth. 2019;122(4):486–13.
2. Jiang JJ, Wang JL, Huang XY, et al. Effect of ultrasound-guided pudendal nerve block on postoperative analgesia after procedure for prolapse and hemorrhoids. J Clin Anesthesiol. 2019;35(7):647–650. Article in Chinese.
3. Joshi GP, Neugebauer EA. Evidence-based management of pain after hemorrhoidectomy surgery. Br J Surg. 2010;97(8):1155–1168. doi:10.1002/bjs.7161
4. Ong CK, Lirk P, Tan CH, Seymour RA. An evidence-based update on nonsteroidal anti-inflammatory drugs. Clin Med Res. 2007;5(1):19–34. doi:10.3121/cmr.2007.698
5. Benyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician. 2008;11(2 Suppl):S105–S120. doi:10.36076/ppj.2008/11/S105
6. Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in Enhanced Recovery After Surgery (ERAS) guidelines. Anesthesiol Clin. 2017;35(2):e115–e143. doi:10.1016/j.anclin.2017.01.018
7. He J, Wu S, Wu J, et al. Ultrasound-guided pudendal nerve block for postoperative analgesia in patients undergoing anorectal surgery: a systematic review and meta-analysis. J Clin Anesth. 2021;75:110488. doi:10.1016/j.jclinane.2021.110488
8. Gao B, Zhang G, Shi Q, et al. Analgesic efficacy of ultrasound-guided pudendal nerve block in patients undergoing hemorrhoidectomy: a randomized controlled trial. BMC Anesthesiol. 2021;21(1):159. doi:10.1186/s12871-021-01384-9
9. Zhu LB, Chan WC, Lo KC, Yum TP, Li L. Wrist-ankle acupuncture for the treatment of pain: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2014;2014:261707. doi:10.1155/2014/261709
10. Shaska E, Leivaditis V, Nikolopoulou A, et al. Harnessing acupuncture for burnout management: a systematic review of its efficacy and applications in high-stress professions. Surg Chron. 2025;30(2):250–260.
11. Han XR, Zhao WR, Chen MD, et al. Current research status of wrist–ankle acupuncture for relieving postoperative pain in surgical patients: a scoping review. Nurs Res China. 2023;37(22):4048–4053. Article in Chinese.
12. Zhong ZR. Application effect of wrist–ankle acupuncture in postoperative analgesia after clavicle fracture. Chin Foreign Med Res. 2023;21(23):128–131. Article in Chinese.
13. Zhang H. Clinical study of wrist–ankle acupuncture as an adjuvant therapy for postoperative pain in patients with perianal abscess. J Shandong Med Coll. 2021;43(3):187–189. Article in Chinese.
14. Kavoussi B, Ross BE. The neuroimmune basis of anti-inflammatory acupuncture. Integr Cancer Ther. 2007;6(3):251–257. doi:10.1177/1534735407305892
15. Zijlstra FJ, Van Den Berg-de Lange I, Huygen FJ, Klein J. Anti-inflammatory actions of acupuncture. Mediators Inflamm. 2003;12(2):59–69. doi:10.1080/0962935031000114943
16. Chang CY, Deng SY, Yi W, et al. Clinical observation of compound Shengji ointment in reducing pain during postoperative dressing changes after hemorrhoid and fistula surgery. Shizhen Guoyi Guoyao. 2007;18(5):1200–1201. Article in Chinese.
17. Hu YE, Hong WX. Effect of early postoperative cleansing enema nursing after hemorrhoid surgery. Jiangxi Med J. 2007;42(11):1086–1087. Article in Chinese.
18. Li Y, Wang WW, Yang JY, et al. Clinical study of ultrasound-guided modified pudendal nerve block for analgesia after perianal abscess surgery. Hebei Med J. 2023;45(23):3570–3573. Article in Chinese.
19. Ma JY, Li ZC, Yu HS, et al. Analgesic effect of nimesulide combined with anxiolytic drugs after anorectal surgery. Chin Mod Doctor. 2008;46(12):102–103. Article in Chinese.
20. Zhang DH, Liu C. Clinical observation of one-stage radical surgery for perianal abscess. Shaanxi Med J. 2008;37(8):1090–1091. Article in Chinese.
21. Li Y, Hou MH, Chen XL. Analysis of postoperative complications and nursing care in elderly patients undergoing radical surgery for rectal cancer. Chin J Proctol. 2004;24(8):29–30. Article in Chinese.
22. Lü C, Zou JL, Shen SH, et al. Comparison of visual analogue scale and verbal rating scale in postoperative pain assessment. Clin Gen Pract Educ. 2004;2(4):214–215. Article in Chinese.
23. Li CC, Xiong YX, Xie J. Techniques for one-stage radical treatment of perianal abscess. Chin Gen Pract. 2005;8(8):667–668. Article in Chinese.
24. deHondt SM, deHondt RA, deHondt P. MRI-based volumetric analysis of perianal abscesses. Eur J Radiol. 2018;105:12–18.
25. Büyükkoçak Ü, Caglayan O, Daphan C, et al. Similar effects of general and spinal anaesthesia on perioperative stress response in patients undergoing haemorrhoidectomy. Mediat Inflammat. 2006;2006(1):97257. doi:10.1155/MI/2006/97257
26. Yan J, Li G, Ma L, Xu H. Comparison of curative effect of incision and drainage with cutting seton as well as incision and drainage on ischiorectal abscess and postanal space abscess. Biomed Res Tokyo. 2017;28(21):9538–9542.
27. Hu J. New concepts in postoperative analgesia for anal diseases. Chin J Proctol. 2004;24(9):32–34. Article in Chinese.
28. Dai XC, Chen C, Zhao LZ. Summary of treatment experience in 1,174 cases of perianorectal abscess. Chin J Proctol. 2005;25(5):16–17. Article in Chinese.
29. Xiong DL, Liang Y. Effect of traditional Chinese medicine pain nursing on quality of life in patients with perianal abscess. World Latest Med Inf. 2020;(37):241. Article in Chinese.
30. Yan LP, Ma C, Li SD, et al. Reflections and suggestions on clinical research and application of acupuncture analgesia. Chin Acupunct Moxibustion. 2004;24(12):869–871. Article in Chinese.
31. Zhang Y. Application of auricular acupressure during colonoscopy. Chin J Nurs. 2005;40(2):83. Article in Chinese.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Ultrasound-Guided Erector Spinae Plane Block at Different Injection Depths for Percutaneous Kyphoplasty: A Randomized Controlled Trial
Liu Y, Yu Y, Gao X, Wang Q, Wang Y, Xia X
Drug Design, Development and Therapy 2026, 20:601168
Published Date: 16 June 2026