Back to Journals » Clinical Ophthalmology » Volume 17
Optimizing Platelet and Leucocyte-Rich Plasma as Biomaterials for Ophthalmic Applications: Impact of Centrifugation Speed
Authors Castillo-Macías A, Zavala J, Ortega-Lara W ![]() , García-Herrera SM, Valdez-García JE
, García-Herrera SM, Valdez-García JE ![]()
Received 1 November 2023
Accepted for publication 6 December 2023
Published 9 December 2023 Volume 2023:17 Pages 3787—3797
DOI https://doi.org/10.2147/OPTH.S444840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Alberto Castillo-Macías,1 Judith Zavala,1 Wendy Ortega-Lara,1 Silvia Margarita García-Herrera,2 Jorge E Valdez-García1
1Instituto Tecnológcio y de Estudios Superiores de Monterrey, ITESM, Monterrey, Nuevo León, México; 2Medicina Diagnóstica, Monterrey, Nuevo León, México
Correspondence: Jorge E Valdez-García, Instituto Tecnológcio y de Estudios Superiores de Monterrey, ITESM, Av. Batallon de San Patricio 112, Real San Agustín, San Pedro Garza García, Monterrey, Nuevo León, 66260, México, Tel +52 81 8888, Email [email protected]
Purpose: To assess the impact of varying centrifugation speeds on platelet and leucocyte-rich plasma (L-PRP) in liquid and gel form cellularity and growth factor concentrations for potential use against ocular surface disorders.
Patients and Methods: L-PRP was collected from 16 healthy subjects using three different centrifugation speeds: 580, 1000, and 2000 g, each for 8 min at 25°C. Platelet and leukocyte counts were automatically evaluated. The concentrations of vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and transforming growth factor beta 1 (TGF-B1) were measured using enzyme-linked immunosorbent assays. L-PRP gel cellularity was assessed through hematoxylin-eosin and Masson’s trichrome staining, categorized as moderate or abundant, and statistically analyzed. L-PRP gel membrane’s chemical composition was analyzed using Fourier-transform infrared spectroscopy (FTIR), crystallization was investigated with X-ray diffraction (XRD), and ultrastructure was assessed using surface electron microscopy (SEM). Additionally, membrane degradation was evaluated over a 7-day period.
Results: No significant differences in cellularity and growth factor concentrations among centrifugation speeds (p > 0.05) were found. Moderate cellularity predominated at 580 g and 2000 g, while abundant cellularity was observed at 1000 g. No significant differences were found techniques (p = 0.16). Masson’s trichrome staining suggested the existence of abundant fibrin at 1000 g but without significant differences (p = 0.07). FTIR analysis exhibited the characteristic fibrin bands at all speeds, and XRD indicated a keratin-like pattern. SEM revealed greater porosity at 580 g and fibrin membrane degradation was lower at this speed (p = 0.0001).
Conclusion: Centrifugation speed did not significantly affect growth factor concentration or cellularity in both liquid and gel L-PRP. Further studies should explore the impact of different separation techniques for L-PRP used in ophthalmic applications.
Plain Language Summary: Background: Platelet and Leukocyte-rich plasma (L-PRP) is obtained from an individual’s blood. It is currently being utilized successfully and showing encouraging outcomes in ophthalmology for various illnesses. The issue of standardization, particularly the centrifugation speed, is one of the main obstacles to its wider application because the preparation protocols vary depending on the disease type and the setting.Goal: We carried out this study to evaluate the effect of centrifugation speed in obtaining platelet and leucocyte-rich plasma in liquid and gel form and its impact on the quality of the product.Results: We discovered that centrifugation speed affected Platelet and Leukocyte-rich plasma cellularity. Furthermore, the centrifugation speed influenced the platelet and leucocyte-rich plasma gel deterioration after seven days. These findings highlight the significance of standardizing procedures, particularly centrifugation speed, to produce a high-quality product that lasts longer and may yield more encouraging outcomes when applied in the field of ophthalmology.Conclusion: L-PRP is a product with great clinical potential. Standardization is the biggest barrier to widespread use. We observed differences depending on the type of centrifugation speed used for its preparation, which opens the way for us to continue carrying out future studies until we obtain a product with the best therapeutic potential in patients with ophthalmological diseases.
Keywords: platelet, leucocytes, centrifugation, growth factors
Introduction
Hemoderivatives have a wide range of medical applications. These physiologically active compounds are clinically effective in various therapeutic contexts, most notably in dermatology, traumatology, plastic surgery, and dentistry.1 In the field of regenerative medicine, blood products can be divided into three categories: autologous serum, platelet-rich plasma (PRP), and plasma rich in growth factors.2 PRP, composed of concentrated platelets and growth factors, is a product with tremendous potential because of its unique capacity to promote tissue regeneration.3 Ehrenfest et al proposed a classification of four distinct families based on fibrin architecture and leucocyte content.4 Low leukocyte content and low fibrin density following activation are characteristics of pure platelet-rich plasma (P-PRP), which qualifies it for usage in liquid solutions or as an active gel. However, apheresis equipment or other techniques are needed for its preparation. Platelet and Leukocyte-Rich Plasma (L-PRP) is a versatile material that can be used in liquid solutions or active gels due to its high leukocyte content and low-density fibrin mesh. Pure Platelet-Rich Fibrin (P-PRF) is not suited for injection or use like traditional fibrin glues since it is devoid of leukocytes and has a high density of fibrin mesh. It is only available in activated gel form. Platelet- and Leukocyte-Rich Fibrin (L-PRF) is only found in an activated gel state and is rich in leukocytes with a high-density fibrin network. Based on fibrin properties and cellular makeup, this classification scheme offers a sophisticated understanding of PRP variations and enables targeted uses. As such, it has become a vital tool in the field of regenerative medicine.4–6 In ophthalmology, PRP in liquid and gel form are used as adjuvant therapy for corneal ulcers, corneal epithelial defects, dry eye syndrome, autoimmune diseases, and epithelial regeneration support.7–10 Within the classification of PRP it has been observed that L-PRP has a positive effect on the stimulation of fibroblast activity, cell migration, and expression of genes related to extracellular matrix and adhesion molecules compared to P-PRP.11,12 Despite its potential application in ophthalmology, a few issues and limitations should be addressed before its wide application.13 Since there are no established standards for L-PRP preparation, the most significant point is standardizing L-PRP preparation, as its therapeutic effectiveness may be impacted by variations in content and quality among preparation techniques.13,14 Buffy coat separation and centrifugation speed are the two phases that impact L-PRP quality. The first stage in producing L-PRP is centrifugation speed. The type of centrifuge used, the target platelet concentration, the amount of blood processed, and the medical use of L-PRP all impact this decision.13,15 Ophthalmological L-PRP may require a different centrifugation speed than orthopedics or dermatology.16 Our main objective was to characterize blood products obtained at different centrifugation speeds to prepare L-PRP in liquid and gel form applicable to ophthalmologic settings.
Materials and Methods
This is an experimental study. Sixteen healthy subjects 20–85 years of age were recruited. After signing and accepting the informed consent, peripheral venous blood samples were obtained in three 10 mL tubes with 1 mL of sodium citrate. Sample collection was carried out at the Zambrano Hellion Medical Center (Ethics Committee 018–2022-CI-R, 2022) following the guidelines of the Declaration of Helsinki.
Preparation of Autologous L-PRP
Autologous L-PRP was prepared under sterile conditions inside a laminar flow hood. To prepare L-PRP, 30 mL of whole blood was added to 15 mL tubes with 1 mL of 3.2% NaCl. Subsequently, samples were centrifuged for 8 min at 25°C at the following speeds: 580 g, 1000 g, and 2000 g. PRP was aspirated by pipetting and placed in photoprotected plastic tubes and refrigerated at 4°C until quantification of growth factors.
For the preparation of the L-PRP in gel form, 30 mL of whole blood was mixed in 10 mL tubes with 1 mL of 3.2% sodium citrate. Samples were centrifuged for 8 min at 25°C at the following speeds: 580, 1000, and 2000 g. Then, 5 mL of platelet-poor plasma was aspirated and placed in photoprotected plastic tubes, before adding 500 μL of 1% calcium chloride and 1 mL of autologous thrombin. Finally, the mixture was incubated at 37°C for 1 h. To prepare autologous thrombin, 1 mL of the PRP previously prepared by pipetting was aspirated and placed in a sterilized glass bottle together with 100 μL of 1% calcium chloride and incubated at 37°C for 30 min. The membranes obtained had a diameter of 18–22 mm and a thickness of 1 mm.
Leucocyte and Platelet Quantification
Leucocyte and platelet quantification was carried out using an automated hemocytometer (Ac-T diff, Beckman Coulter, Brea, CA, USA). Samples were diluted to maintain linearity prior to automated analysis, based on the detection limits of the apparatus and manufacturer’s information.
Quantification of Growth Factors
Platelet derived growth factor AB (PDGF-AB), vascular endothelial growth factor (VEGF) and transforming growth factor B1 (TGF-B1) levels were quantified in PRP using enzyme-linked immunosorbent assay (ELISA) commercial kits (Invitrogen; ThermoFisher, Waltham, MA, USA). Absorbances were read at the manufacturer’s recommended wavelength using microplate readers. Samples were measured in duplicate at the appropriate dilutions required for the specific calibration curve.
Histological Analysis of L-PRP Gel
The L-PRP gel meshes were analyzed histologically. Once obtained, the mesh was fixed in 10% formalin for 24 h, dehydrated, and immersed in paraffin. Afterward, the block obtained was cut into sections, which were subjected to hematoxylin and eosin staining for analysis and evaluation of the distribution of platelets, leukocytes, and fibrin. To better observe fibrin, we also used Masson’s trichrome staining.
Chemical Analysis and Crystallization of L-PRP Gel
The chemical structure of the L-PRP gel was analyzed using Fourier-transform infrared spectroscopy (FTIR) in a Fourier-transform Spectrum 400 apparatus (Perkin Elmer, Waltham, MA, USA) at the wavenumber range of 4000–400 cm−1 under room temperature. Furthermore, XRD was used to assess the crystallinity of the platelet-rich fibrin membrane. XRD was recorded in the 2θ range between 10° –85° with a step size of 0.026 using a PANalytical Empyrean diffractometer (PANalytical, Almelo, The Netherlands) and CuKα radiation (λ = 1.5406 Å). The voltage applied was 45 kV and the current was 40 mA.
L-PRP Gel Ultrastructure Evaluation
Scanning electron microscopy was used for the structural evaluation of the L-PRP gel meshes. Samples were fixed with 2.5% glutaraldehyde for 2h at 4°C, post-fixed with osmium tetraoxide (1% OsO1 in 0.1M cacodylic acid buffer) for 2h at 4°C and dehydrated with alcohol at different concentrations (70 to 100%). Once dry, samples were covered with gold using a Quorum QR150 ES sputtering system (Quorum Technologies, Laughton, UK) and subjected to analysis with an EVO MA Scanning Electron Microscope (Carl Zeiss Microscopy).
In vitro Degradation of L-PRP Gel
The degradation study was carried out for 7 days. Once formed, the L-PRP gel meshes were weighed to obtain an initial weight (P0). Then, weight was measured every 24 h. The percentage of remaining mass was calculated using a mathematical formula ((Pd/P0) X 100).
Statistical Analysis
General descriptive analyses were performed using measures of central tendency. For the evaluation of normality, the Shapiro–Wilk test was performed. The results were compared by performing a two-way ANOVA test with the objective of determining the existence of significant differences between the groups. P values were 2-tailed and values <0.05 were considered statistically significant. The analysis of this data was carried out using IBM SPSS version 26 software.
Results
Patients
We included a total of 16 healthy participants with an average age of 30 years (SD: 15.2); 43.75% women and 56.25% men; (Table 1).
 |
Table 1 Clinical Characteristics of Healthy Subjects |
Leucocyte and Platelet Quantification
We obtained 6 mL of L-PRP from the entire blood taken from each healthy participant. The preparation of L-PRP gel meshes for investigations on leucocytes, platelets, chemical analysis, and degradation was also done (Figure 1). There was a significant difference (p = 0.01) in the concentration of leukocytes at a speed of 2000 g, with a concentration of 6.4 × 103/μL (SD: 0.6) (Table 2). However, there was no significant difference (p = 0.85) in the concentration of platelets, with the highest concentration of 880.8 × 103/μL (SD: 73.6) being found at 580 g (Figures 2 and 3).
 |
Table 2 Leucocyte and Platelet Count from Whole Blood and Platelet and Leucocyte-Rich Plasma (L-PRP) at Different Centrifugation Speeds |
 |
Figure 1 (a) L-PRP and (b) L-PRP gel mesh obtained from the whole blood of healthy subjects. |
 |
Figure 2 White blood cell concentration in whole blood and L-PRP at different centrifugation speeds. Results are presented as mean ± standard deviation (SD) *(p < 0.05). |
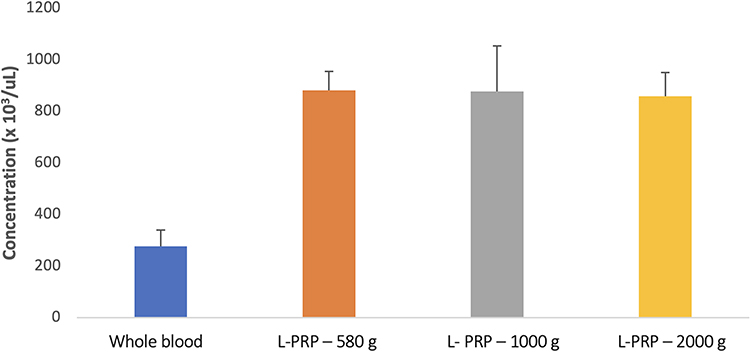 |
Figure 3 Platelet concentration in whole blood and L-PRP at different centrifugation speeds. Results are presented as mean ± standard deviation (SD). |
Quantification of Growth Factors
Commercial ELISA kits were used to make measurements of growth factors VEGF, PDGF, and TGF-B1 (Table 3). At 2000 g, the maximum VEGF concentration was 482 pg/mL (SD: 98.65). The maximum level of PDGF was measured at 580 g, at 1597.75 pg/mL (SD: 60.85). TGF-B1 was present in the maximum concentration at 1000 g, 843.05 pg/mL (SD: 90.70). The concentration of VEGF, PDGF, and TGF-B1 did not differ significantly among centrifugation speeds (p > 0.05).
 |
Table 3 Growth Factor Concentration from Platelet and Leucocyte-Rich Plasma (L-PRP) at Different Centrifugation Speeds |
Histological Analysis of L-PRP Gel
H&E staining assessed leucocyte and platelets while Masson’s trichrome stain determined the presence of fibrin in the histological examination. At 580 g and 2000 g, the observed cellularity was modest, but the 1000 g technique showed abundant cellularity; however, there were no significant differences (p = 0.16). With Masson’s trichrome staining, precipitates strongly resembling fibrin were frequently observed at 1000 g (Figure 4), but without significant differences to other speeds (p = 0.07).
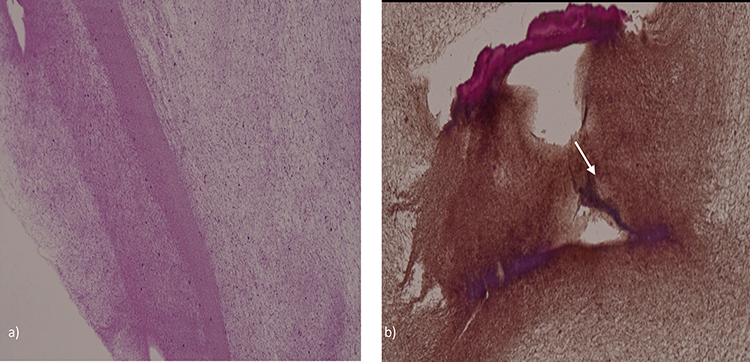 |
Figure 4 Histological analysis of L-PRP gel meshes. (a) H&E staining (40X) of platelet-rich fibrin membranes with abundant cellularity obtained at a centrifugation speed of 1000 g. (b) Masson´s trichrome staining (40X) of platelet-rich fibrin membranes at a centrifugation speed of 1000 g. The arrow indicates abundant precipitation, highly suggestive of fibrin. |
Chemical Analysis and Crystallization of L-PRP Gel
In FTIR, we could confirm that both samples were hydrated, as evidenced by the presence of a band at 3276 cm−1 associated with the OH functional group.17 A band at 1634 (1634–1639) cm−1 corresponded to the amide I functional group18 and featured vibration and tension in the v(C=O) bond. In addition, a second band associated to the amide II functional group19 with vibration and bending of the v(N–H) bond was observed at 1541 (1541–1546) cm−1. The presence of glycoproteins (C–O) on the membrane surface could be linked to the band at 1020 cm−1.20 These bands are in line with those described for fibrin.21 The fibrin membrane XRD pattern revealed a fibrous and regular organization with a distinctive peak at 26.4o (Figure 5).22
 |
Figure 5 Chemical analysis of L-PRP gel meshes. (A) FTIR of L-PRP gel meshes obtained at different centrifugation speeds. (a) 580 g, (b) 1000 g, and (c) 2000 g. (B) XRD analysis of L-PRP gel meshes obtained with different centrifugation speeds. (a) 580 g, (b) 1000 g, and (c) 2000 g. |
L-PRP Gel Ultrastructure Evaluation
A porous membrane can be observed in the sample centrifuged at 580 g (a) while cell immersion is best observed at 1000 g (b). Finally, the membrane walls were thinner at 2000 g (c) (Figure 6).
 |
Figure 6 SEM images of L-PRP gel meshes obtained at different centrifugation speeds (Bar: 2 μM): (a) 580 g, (b) 1000 g, and (c) 2000 g. |
In vitro Degradation Study of L-PRP Gel
The three fibrin membranes were degraded over seven days. At the end of that period, we observed significantly (p = 0.0001) less degradation at 580 g with an initial weight of 0.292 g and a final weight of 0.223. With 28.5% of degradation, there was also a significant difference (p = 0.000003) in percentage terms at 580 g (Figure 7).
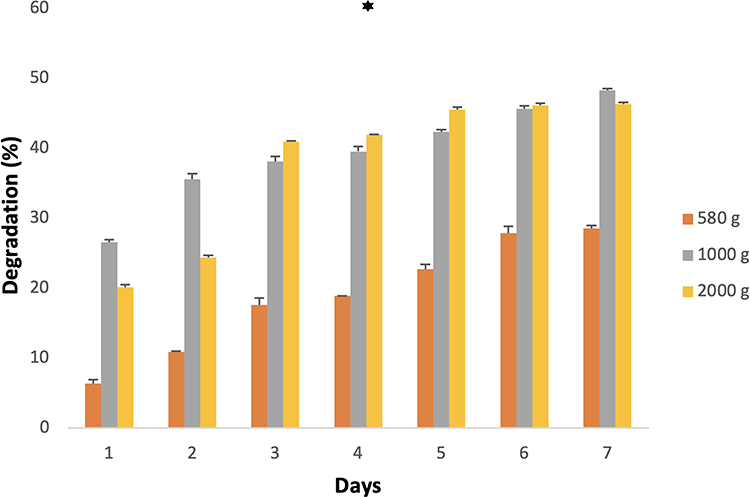 |
Figure 7 Degradation of L-PRP gel meshes at different centrifugation speeds over a period of seven days. *(p < 0.05). |
Discussion
The potential of PRP to treat disorders of the ocular surface has been investigated. The ocular surface illness Index score and conjunctival lissamine green staining decreased in response to PRP eye drops, indicating improvement in symptoms and indicators of ocular surface illness.23,24 PRP eye drops can be produced utilizing a variety of techniques, including platelet apheresis donation and platelet lysates.10,14 Distinct PRP products, including PRP eye drops and platelet gels, have been shown in clinical investigations to enhance patient signs and symptoms.10,18,25 Regarding PRP derivatives, L-PRP apparently has a better regenerative effect thanks to the microenvironment generated by the presence of leukocytes.11,12
In ophthalmology, PRP in gel form has been applied in several ways. It has been used as an adjuvant therapy to treat idiopathic macular holes, periocular chemical and thermal burns, corneal ulcers, and symptomatic dry eyes.18,25 At the site of damage or surgery, PRP offers a larger concentration of vital growth factors and cell adhesion molecules that improve wound healing and the surrounding physiological processes.17
One of the biggest obstacles to the broad use of PRP and its derivatives in clinical practice has been the need for standardization. To compare the variations in the products obtained and to be able to perform it more frequently in clinical practice, we reviewed protocols that included single-step centrifugation 2224 at different centrifugation speeds.13,15
Among both whole blood and L-PRP samples subjected to different centrifugation speeds, leukocytes were most abundant at 1000 g whereas platelets were most abundant at 580 g. Our cellularity findings coincide with previous work using these centrifugation speeds.13,18 Leukocyte concentration can vary depending on a person’s health status, whereas platelet concentration has been found to differ depending on age group and sex.19–21
The greatest PDGF concentration was obtained at 580 g, whereas that of VEGF was obtained at 2000 g and that of TGF-B1 at 1000 g. The concentration of growth factors observed in our study is similar to previously reported22,25,26 but we did not observe significant differences among the various centrifugation speeds in this respect.10,18,25
The different centrifugation speeds had no effect on cellularity or the presence of fibrin; however, fibrin membrane disintegration occurred to a lesser extent at 580 g. No differences were observed in the speeds in the concentration of growth factors, cellularity, and presence of fibrin due to obtaining L-PRP, since not only the centrifugation speed influence the preparation but also the separation of the buffy coat from the whole blood after centrifugation.26–29 Despite the several methods to separate it, there is no standardized protocol. Furthermore, activating L-PRP could have an impact on growth factor release due to platelet degranulation.
The L-PRP gel meshes were processed at three different centrifugation rates, and its composition and degradation were analyzed. The existence of a fibrin network was confirmed by FTIR.30 The sample spectra revealed signals in bands associated with fibrin, independently of centrifugation speed. Accordingly, XRD showed a fibrin structure and a crystalline area with keratin-like reflections.31,32 SEM analysis showed variations in membrane wall thickness, which may affect the effectiveness of the membranes by prolonging the time that platelets and leukocytes are trapped, regulating the release of growth factors continuously, and creating a microenvironment that encourages cell regeneration.31,33
The degradation process took place over a period of 7 days in accordance to what is reported on the literature.33–35 We found that membranes developed at a centrifugation speed of 580 g underwent the least amount of degradation. This can have a great impact on the days of useful life; however, it is advisable to carry out studies that evaluate whether the release of growth factors also remains constant until their absolute degradation.
This study has certain limitations. The first is the homogeneity of the population, which can be reduced by increasing the sample size and by separating the participants by age and sex, something which could significantly affect L-PRP’s cellularity. Additionally, the age of the population under study might be changed to one where ocular surface disorders are more common. The impact of chronic illnesses and medications on the efficacy of blood products must also be assessed, along with all cellular changes and growth factors in both health and sickness. Additionally, analysis using electron microscopy can be extended, establishing a stronger association with cellularity and efficiency. Future studies should aim to correlate the separation and obtaining of PRP with cellularity and its effectiveness, to assist with standardization and ultimate clinical adoption.
Conclusion
By characterizing L-PRP in terms of growth factors and cellularity, this work lays the foundation for a future standardization of centrifugation speeds. There were no significant differences in growth factor levels or in their chemical and structural properties between centrifugation speeds, but L-PRP gel meshes degraded less at 580 g, which could potentially impact quality. Autologous blood products hold a lot of promise for clinical use. With encouraging outcomes, its usage in ocular surface modifications has become more widespread. The standardization of its production, which may affect its effectiveness by influencing cellularity and the release of growth factors, is currently one of the challenges that must be solved.
Abbreviations
CGF, Concentrated growth factors; ELISA, Enzyme-linked immunosorbent assay; FTIR, Fourier transform infrared spectroscopy; PDGF, Platelet-derived growth factor; PLT, Platelets; PRP, Platelet-rich plasma; SD, Standard deviation; SEM, Surface electron microscopy; TGF, Transforming growth factor; uL, Microliter; VEGF, Vascular endothelial growth factor; WBC, White blood cells; XRD, X-ray diffraction.
Ethics Approval Statement
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of School of Medicine and Health Sciences of Monterrey Institute of Technology and Higher Education (April 22, 2022/No. 018-2022-CI-R). Consent was obtained by the study participants prior to study commencement.
Acknowledgments
We thank the laboratories of the School of Medicine and Health Sciences of the Technological Institute of Monterrey (EMIS), as well as the Biotechnology Laboratory and the Pathology Laboratory of Medicina Diagnóstica for their invaluable support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nikolidakis D, Jansen JA. The biology of platelet-rich plasma and its application in oral surgery: literature review. Tissue Eng Part B Rev. 2008;14(3):249–258. doi:10.1089/ten.teb.2008.0062
2. Acebes-Huerta A, Arias-Fernández T, Bernardo Á, et al. Platelet-derived bio-products: classification update, applications, concerns and new perspectives. Transfus Apher Sci. 2020;59(1):102716. doi:10.1016/j.transci.2019.102716
3. Nurden AT. Platelets, inflammation and tissue regeneration. Thromb Haemost. 2011;105(SUPPL. 1):S13–33. doi:10.1160/THS10-11-0720
4. Foster TE, Puskas BL, Mandelbaum BR, Gerhardt MB, Rodeo SA. Platelet-rich plasma: from basic science to clinical applications. Am J Sports Med. 2009;37(11):2259–2272. doi:10.1177/0363546509349921
5. Medzhitov R. Origin and physiological roles of inflammation. Nature. 2008;454(7203):428–435. doi:10.1038/nature07201
6. Andrae J, Gallini R, Betsholtz C. Role of platelet-derived growth factors in physiology and medicine. Genes Dev. 2008;22(10):1276–1312. doi:10.1101/gad.1653708
7. Alio JL, Rodriguez AE, WróbelDudzińska D. Eye platelet-rich plasma in the treatment of ocular surface disorders. Curr Opin Ophthalmol. 2015;26(4):325–332. doi:10.1097/ICU.0000000000000169
8. Alio JL, Abad M, Artola A, Rodriguez-Prats JL, Pastor S, Ruiz-Colecha J. Use of autologous platelet-rich plasma in the treatment of dormant corneal ulcers. Ophthalmology. 2007;114(7):1286–1294. doi:10.1016/j.ophtha.2006.10.044
9. Anitua E, Sanchez M, Nurden AT, Nurden P, Orive G, Andia I. New insights into and novel applications for platelet-rich fibrin therapies. Trends Biotechnol. 2006;24:227–234. doi:10.1016/j.tibtech.2006.02.010
10. Merolle L, Iotti B, Berni P, et al. Platelet-rich plasma lysate for treatment of eye surface diseases. J Vis Exp. 2022;186:
11. Devereaux J, Dargahi N, Fraser S, Nurgali K, Kiatos D, Apostolopoulos V. Leucocyte-rich platelet-rich plasma enhances fibroblast and extracellular matrix activity: implications in wound healing. Int J Mol Sci. 2020;21(18):6519. doi:10.3390/ijms21186519
12. Jayaram P, Mitchell PJT, Shybut TB, Moseley BJ, Lee B. Leukocyte-rich platelet-rich plasma is predominantly anti-inflammatory compared with leukocyte-poor platelet-rich plasma in patients with mild-moderate knee osteoarthritis: a prospective, Descriptive Laboratory Study. Am J Sports Med. 2023;51(8):2133–2140. doi:10.1177/03635465231170394
13. Fadadu PP, Mazzola AJ, Hunter CW, Davis TT. Review of concentration yields in commercially available platelet-rich plasma (PRP) systems: a call for PRP standardization. Reg Anesth Pain Med. 2019;44(6):652–659. doi:10.1136/rapm-2018-100356
14. Dhurat R, Sukesh M. Principles and methods of preparation of platelet-rich plasma: A Review and Author’s Perspective. J Cutan Aesthet Surg. 2014;7(4):189–197.
15. Croise B, Pare A, Joly A, Louisy A, Laure B, Goga D. Optimized centrifugation preparation of the platelet rich plasma: literature review. J Stomatol Oral Maxillofac Surg. 2019;2019:1.
16. Arora S, Doda V, Kotwal U, Dogra M. Quantification of platelets and platelet derived growth factors from platelet-rich plasma (PRP) prepared at different centrifugal force (g) and time. Transfus Apher Sci. 2016;54:103–110. doi:10.1016/j.transci.2016.01.028
17. Alio L, Arnalich-Montiel J, F E, Rodriguez A. The role of “eye platelet rich plasma” (E-Prp) for wound healing in ophthalmology. Curr Pharm Biotechnol. 2012;13(7):1257–1265. doi:10.2174/138920112800624355
18. Jung JU, Hee Lee S, Kyun Kim H. Effects of platelet-rich plasma on ocular surface in patients with dry eye syndrome: clinico-experimental analysis. J Korean Ophthalmol Soc. 2019;60:1169–1175. doi:10.3341/jkos.2019.60.12.1169
19. Mazzocca AD, McCarthy MB, Chowaniec DM, et al. Platelet- rich plasma differs according to preparation method and human variability. J Bone Joint Surg Am. 2012;94:308–316. doi:10.2106/JBJS.K.00430
20. Rubak P, Nissen PH, Kristensen SD, Hvas AM. Investigation of platelet function and platelet disorders using flow cytometry. Platelets. 2016;27(1):66–74. doi:10.3109/09537104.2015.1032919
21. Pik W, Diaz R, Borg-Stein J. Platelet-rich plasma. Phys Med Rehabil Clin N Am. 2016;27(4):825–853. doi:10.1016/j.pmr.2016.06.002
22. Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85(6):638–646. doi:10.1016/S1079-2104(98)90029-4
23. Amable PR, Carias RB, Teixeira MV, et al. Platelet-rich plasma preparation for regenerative medicine: optimization and quantification of cytokines and growth factors. Stem Cell Res Ther. 2013;4:67–74. doi:10.1186/scrt218
24. Nadelmann Jennifer B, Bunya VY, Ying G-S, et al. Effect of autologous platelet-rich plasma drops in the treatment of ocular surface disease. Clin Ophthalmol. 2022;16:4207–4213. doi:10.2147/OPTH.S391536
25. Panda BB, Mohapatra S, Parida S. Update on the role of Eye Platelet-Rich Plasma (E-PRP) in the treatment of ocular surface disorders. Indian J Clin Exp Ophthalmol. 2020;6:487–496. doi:10.18231/j.ijceo.2020.106
26. Kobayashi Y, Saita Y, Nishio H, et al. Leukocyte concentration and composition in platelet-rich plasma (PRP) influences the growth factor and protease concentrations. J Orthop Sci. 2016;21:683–689. doi:10.1016/j.jos.2016.07.009
27. Perez AG, Lana JF, Rodrigues AA, Luzo AC, Belangero WD, Santana MH. Relevant aspects of centrifugation step in the preparation of platelet-rich plasma. ISRN Hematol. 2014;2014:176060. doi:10.1155/2014/176060
28. Dohan DM, Choukroun J, Diss A, et al. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part II: platelet-related biologic features. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101(3):45–50. doi:10.1016/j.tripleo.2005.07.009
29. Fijnheer R, Pietersz RN, de Korte D, et al. Platelet activation during preparation of platelet concentrates: a comparison of the platelet‐rich plasma and the buffy coat methods. Transfusion. 1990;30:634–638. doi:10.1046/j.1537-2995.1990.30790385523.x
30. Bramanti E, Benedetti E, Sagripanti A, Papineschi F, Benedetti E. Determination of secondary structure of normal fibrin from human peripheral blood. Biopolymers. 1997;41(5):545–553. doi:10.1002/(SICI)1097-0282(19970415)41:5<545::AID-BIP6>3.0.CO;2-M
31. Sathian J, Sastry TP, Suguna L, Lakshminarayana Y, Radhakrishnan G. Fibrin as a matrix for grafting 2-hydroxyethyl methacrylate: preparation and characterization of the graft and its in vivo evaluation for wound healing. J Biomed Mater Res A. 2003;65(4):435–440. doi:10.1002/jbm.a.10489
32. Anitua E, Padilla S, Prado R, Alkhraisat MH. Platelet-rich plasma: are the obtaining methods, classification and clinical outcome always connected? Regen Med. 2022;17(12):887–890. doi:10.2217/rme-2022-0118
33. Dohan Ehrenfest DM, Bielecki T, Jimbo R, et al. Do the fibrin architecture and leukocyte content influence the growth factor release of platelet concentrates? An evidence-based answer comparing a pure platelet-rich plasma (P-PRP) gel and a leukocyte and platelet-rich fibrin (L-PRF). Curr Pharm Biotechnol. 2012;13(7):1145–1152. doi:10.2174/138920112800624382
34. Isobe K, Watanebe T, Kawabata H, et al. Mechanical and degradation properties of advanced platelet-rich fibrin (A-PRF), concentrated growth factors (CGF), and platelet-poor plasma-derived fibrin (PPTF). Int J Implant Dent. 2017;2017:1–6.
35. Miron RJ, Zucchelli G, Pikos MA, et al. Use of platelet-rich fibrin in regenerative dentistry: a systematic review. Clin Oral Investig. 2017;21:1913–1927. doi:10.1007/s00784-017-2133-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.