Back to Journals » Risk Management and Healthcare Policy » Volume 19
Optimizing Operational Efficiency and Patient Satisfaction in Tumor Day Wards: An HFMEA-Based Process Redesign Study
Authors Li R, Li J ![]() , Song L, Yuan F
, Song L, Yuan F
Received 1 November 2025
Accepted for publication 3 February 2026
Published 3 March 2026 Volume 2026:19 573659
DOI https://doi.org/10.2147/RMHP.S573659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Ranran Li,1 Jiahui Li,2 Lina Song,3 Fang Yuan1
1Thoracic Radiation Oncology Ward 5, Affiliated Cancer Hospital of Shandong First Medical University, Jinan, Shandong Province, 250117, People’s Republic of China; 2Department of Anesthesia Surgery, The Fifth People’s Hospital of Jinan, Jinan, Shandong Province, 250022, People’s Republic of China; 3Orthopedic Three Wards, the Fifth People’s Hospital of Jinan, Jinan, 250022, People’s Republic of China
Correspondence: Fang Yuan, Department of Thoracic Radiation Oncology Ward 5, Affiliated Cancer Hospital of Shandong First Medical University, No. 440, Jiyan Road, Jinan, Shandong Province, 250117, People’s Republic of China, Email [email protected]
Objective: To explore the application of Healthcare Failure Mode and Effect Analysis (HFMEA) in optimizing the operational workflow of oncology day wards.
Methods: A retrospective controlled study was conducted with 658 patients treated in our day ward from August 2021 to March 2022. The control group (n=344, August to November 2021) received standard care, while the experimental group (n=314, December 2021 to March 2022) underwent HFMEA-based process redesign. Key interventions included establishing a multidisciplinary team, developing a patient admission assessment tool, optimizing infusion chair allocation, creating a WeChat-based communication platform, and implementing electronic health education. Risk Priority Numbers (RPNs) were calculated using a severity-occurrence matrix. Primary outcomes included RPN reduction rates, treatment waiting times, and patient satisfaction scores.
Results: Compared with the control group, the experimental group showed significant improvements in several key metrics. The RPN improvement rates for the treatment, evaluation, and treatment processes were 48.01%, 52.94%, and 61.59%, respectively. The experimental group also demonstrated higher satisfaction scores from 3 to 4 points in waiting time, infusion process, health education, service attitude aspects. Additionally, the median waiting time decreased from 16 minutes to 7 minutes (P< 0.05). However, there was no statistically significant difference between the two groups in patients’ satisfaction with the admission process, diagnosis and treatment technology, technical operation, treatment environment, and discharge environment (P> 0.05).
Conclusion: The optimized day ward operation process based on HFMEA has demonstrated significant benefits in reducing medical risks, shortening patient treatment waiting time, and improving patient satisfaction. These improvements are particularly relevant for healthcare institutions facing similar challenges.
Keywords: healthcare failure mode and effect analysis, HFMEA, tumor, day-time wards, management
Background
With the increasing patient volume in our hospital and the ongoing reform of national medical insurance policies, we established a day ward in April 2021 to reduce patient hospitalization costs, shorten hospital stays, and enhance the efficiency of medical service turnover. In the context of this study, the “day ward” refers specifically to a dedicated oncology unit designed for patients requiring systemic anti-tumor treatments (eg, chemotherapy, immunotherapy, or targeted therapy). Patients admitted to this unit complete their scheduled treatments and are discharged within the same working day, typically without an overnight stay. During the operation of the day ward in our department, it generally functioned in accordance with the hospital’s management requirements for day wards. However, given that our department has consistently been in a high-volume operational state, several challenges have emerged in the day ward’s operation. Frequent delays in treatment initiation due to poor coordination between different units.1 Limited space and resources lead to long waiting times for patients, exacerbating their anxiety and discomfort.2 Inadequate information sharing between medical staff and patients, resulting in misunderstandings and dissatisfaction.3 Many patients felt disconnected from the care environment due to the rapid turnover of patients in the day ward. Limited time for healthcare providers to interact with each patient, leading to a perception of impersonal care.4 Patients felt their concerns were not adequately addressed, further reducing their overall satisfaction. These issues not only affect patient experience but also have broader implications for the healthcare system, including increased stress on medical staff, potential for medical errors, and reduced overall efficiency. Although day wards have been implemented in some hospitals with increased bed pressure in China,5 there are no mature management models worth learning from. Therefore, addressing these challenges is crucial for improving patient outcomes and operational efficiency.
Healthcare Failure Mode and Effects Analysis (HFMEA) is a prospective crisis analysis system developed specifically for medical and health institutions. It examines potential failure links in process operations, identifies reasons for failure and potential adverse effects, proposes corrective measures, optimizes processes, and minimizes process failures.6 HFMEA is a proactive risk management method that uses a two-dimensional risk analysis based on the severity of adverse consequences and the probability of events to maximize medical safety.7 Internationally, HFMEA has demonstrated transformative impacts across diverse healthcare settings, with notable applications and outcomes. It has been used in outpatient safety departments reduced patient identification errors by 63% through standardized checklists.8 Structured HFMEA protocols lowered violent incident rates among schizophrenia patients by 41% via behavioral risk stratification.9 In elderly cancer patients, HFMEA-driven chemotherapy protocols minimized adverse drug reactions (ADR) more than 50%.10 Preoperative HFMEA reduced operating room (OR) turnover time nearly 20% in cardiac surgery units.11 Closed-loop HFMEA interventions cut IV medication errors up to 70% in neonatal ICUs.12,13 HFMEA redesign cut emergency department (ED) patient wait times by 30% during COVID-19 surges.14,15 Beyond these specific applications, HFMEA has also seen methodological advancements that enhance its effectiveness and adaptability. Combining HFMEA with the Systems-Theoretic Accident Model (STAMP) improves error root-cause identification.16 These advancements and applications underscore HFMEA’s versatility and its value in addressing complex healthcare challenges.
In our study, we applied HFMEA to address the operational issues in our day ward, aiming to improve patient satisfaction and streamline processes. By leveraging the theoretical foundation and successful international applications of HFMEA, we sought to develop a tailored solution for our specific context.
General Information
Given the retrospective nature of this study, a post-hoc power analysis was performed to verify the statistical power of the actual sample size obtained. Based on the actual enrollment of 344 patients in the control group and 314 in the experimental group, assuming a medium effect size (Cohen’s d = 0.5) and a significance level (α) of 0.05, the calculated power (1-β) exceeded 0.99. This result confirms that the available sample size significantly surpassed the minimum requirement (n = 64 per group for 0.80 power) and was sufficient to robustly detect clinically significant differences in patient satisfaction and waiting time. While the primary objective of this study was to apply HFMEA for the prospective analysis and redesign of the day ward’s operational processes, retrospective patient data were collected to empirically validate the clinical impact of these process interventions. A total of 658 patients who received treatment in the day ward of our department from August 2021 to March 2022 were selected. Among them, 344 patients admitted from August 2021 to November 2021 were assigned to the control group, and 314 patients treated from December 2021 to March 2022 were assigned to the experimental group. In the control group, there were 209 male and 135 female patients, aged 40 to 78 years, with an average age of (61.74±11.06) years. The disease types included 207 cases of lung cancer, 74 cases of esophageal/gastric cardia cancer, 54 cases of breast cancer, 6 cases of thymic cancer, and 3 cases of mediastinal tumors. The treatment methods were chemotherapy in 156 cases, targeted/immunotherapy in 124 cases, and concurrent chemotherapy + targeted/immunotherapy in 64 cases. In the experimental group, there were 194 male and 120 female patients, aged 37 to 74 years, with an average age of (62.91±10.70) years. The disease types included 173 cases of lung cancer, 88 cases of esophageal/gastric cardia cancer, 41 cases of breast cancer, 8 cases of thymic cancer, and 4 cases of mediastinal tumors. The treatment methods were chemotherapy in 149 cases, targeted/immunotherapy in 122 cases, and concurrent chemotherapy + targeted/immunotherapy in 43 cases. There were no statistically significant differences in age, gender, disease type, and treatment method between the two groups (P>0.05), and they were comparable. The results showed that there were no significant differences between the control and experimental groups in terms of these characteristics, indicating that the two groups were comparable at baseline. The study was approved by the ethics committee of Affiliated Cancer Hospital of Shandong First Medical University.
Research Method
The control group followed the original day ward operation process, representing the baseline standard of care prior to the HFMEA intervention. This baseline model operated on a conventional “first-come, first-served” basis without the specific process optimizations introduced later. Specifically, the baseline characteristics were: (1) Admission Criteria: Patients were admitted based solely on the attending physician’s prescription for chemotherapy or immunotherapy, lacking a standardized, multi-dimensional risk assessment tool to evaluate suitability for day-stay safety; (2) Resource Management: Infusion chairs were unnumbered and occupied randomly by patients upon arrival, often resulting in disorder during peak hours; (3) Scheduling: Treatments were administered sequentially based on patient arrival times rather than a staggered appointment system, leading to unpredictable waiting periods; (4) Health Education: Education was provided primarily through verbal instructions by nurses during catheterization or drug administration, which was often fragmented due to time constraints and heavy workload. The experimental group received diagnosis and treatment using the renovated process based on HFMEA, which includes the following specific steps:
Project Team Formation
In July 2021, a multidisciplinary project team was established to oversee the implementation of HFMEA in the day ward. The team consisted of six members, including 1 head nurse, 1 attending physician, 1 resident physician, 1 primary nurse, and 2 responsible nurses, all of whom held intermediate or above professional titles. The team was carefully selected to ensure a diverse range of expertise and perspectives, which is crucial for a comprehensive analysis. The responsibilities of each team member were clearly defined to ensure efficient collaboration and accountability. The head nurse provided overall guidance and coordinated the project. The attending physician and resident physician contributed their clinical expertise and ensured that the medical aspects of the day ward operations were thoroughly assessed. The primary nurse and responsible nurses were tasked with collecting detailed data on the current operation status of the day ward, including patient flow, treatment delays, and staff feedback. They also played a key role in implementing the corrective measures developed by the team. All team members participated in analyzing the failure modes of the day ward operation and developing corrective measures. This collaborative approach ensured that all aspects of the day ward operations were scrutinized and that the proposed improvements were practical and effective.
Drawing the Day Ward Operation Process Flowchart
To gain a comprehensive understanding of the current-day ward operation, the team meticulously mapped out the entire process (Figure 1), breaking it down into four distinct modules: admission, assessment, treatment, and discharge. Each module was further divided into detailed sub-processes to identify potential points of failure. The team held several brainstorming sessions to discuss the completeness and accuracy of the process flowchart. They reviewed existing protocols, observed day-to-day operations, and gathered input from frontline staff and patients. This iterative process ensured that the flowchart accurately reflected the actual workflow and identified any gaps or inefficiencies.
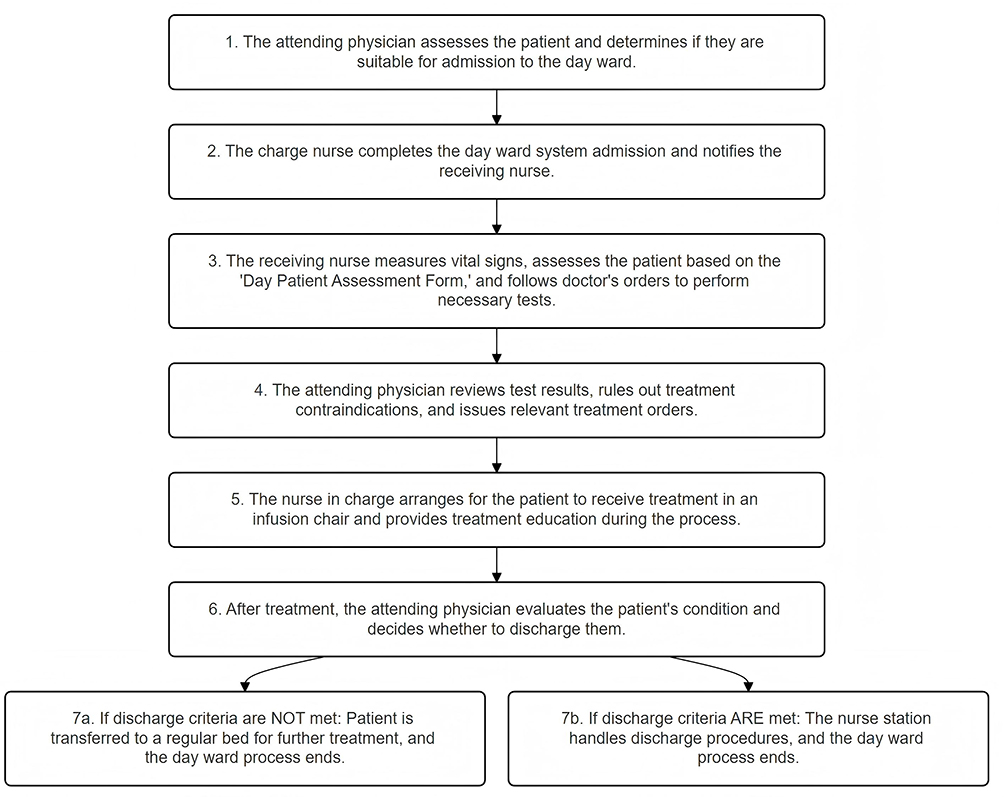 |
Figure 1 The Operational process flow of The Day Ward. |
Failure Modes and Effects Analysis
The core of the HFMEA process involved conducting a thorough process error analysis to identify potential failure modes. The team collected feedback from medical staff and patients on the daily operation of the day ward, focusing on areas where errors or inefficiencies were most likely to occur. This feedback was used to identify potential failure modes corresponding to each process step.
Conducting Process Error Analysis to Identify Failure Modes
The team brainstormed and listed potential failure modes of the day ward. It is crucial to note that this study strictly adhered to the Healthcare Failure Mode and Effect Analysis (HFMEA) model developed by the US Department of Veterans Affairs (VA) National Center for Patient Safety.17 Unlike traditional FMEA, this healthcare-specific model replaces the “Detection” parameter with a “Decision Tree” to guide action planning. Consequently, the risk assessment relies on a two-dimensional Hazard Scoring Matrix based on Severity (S) and Probability (O). The Severity of failure is categorized into four levels: catastrophic (score 4; may cause death/injury), critical (score 3; causes serious dissatisfaction), moderate (score 2; minor performance loss), and minor (score 1; unnoticed by patients). The Probability of failure is similarly categorized: frequent (score 4; likely to occur multiple times/year), occasional (score 3; occurs every 1–2 years), infrequent (score 2; occurs every 2–5 years), and rare (score 1; unlikely to occur). The Risk Priority Number (RPN), or Hazard Score, was calculated as S × O. A score of ≥8 or a Severity score of 4 indicated a high-priority failure mode requiring intervention.18 Through this analysis, the admission, assessment, and treatment stages were identified as critical areas for optimization; the specific failure modes, causes, and predicted effects are detailed in Table 1.
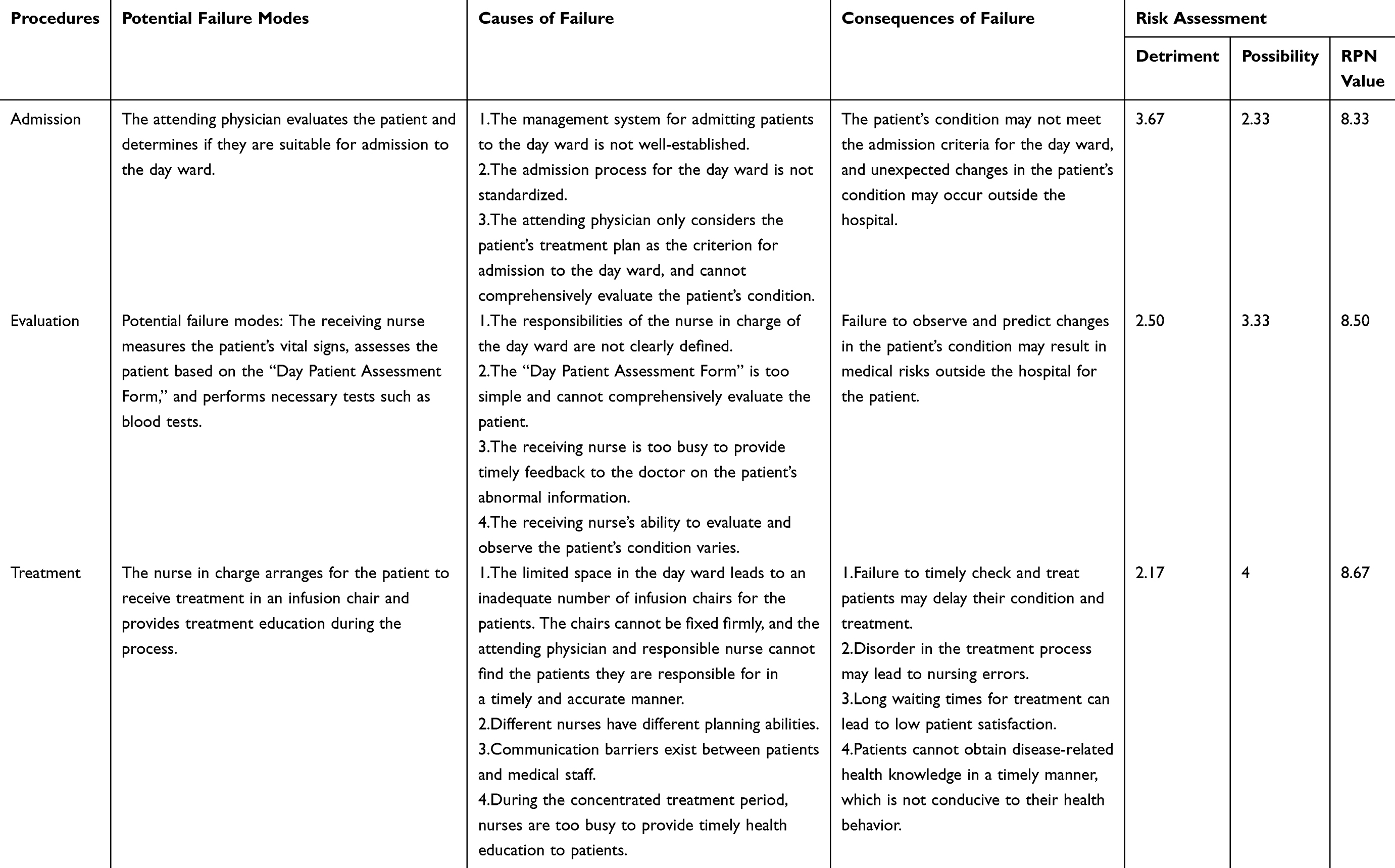 |
Table 1 Failure Modes of the Day Ward and Their Associated Risks |
Developing and Implementing Improvement Measures
Establishing a Management System for the Day Ward
The project team presented the results of the failure mode analysis in the departmental management meeting. The management team members engaged in extensive discussions and ultimately formulated a comprehensive management system and performance plan for the day ward. This system clarified the responsibilities and performance evaluation criteria for each position in the department, ensuring that all staff members understood their roles and were held accountable for their performance.
Developing < the Patient Admission Assessment Form for the Day Ward >
To ensure that only suitable patients were admitted to the day ward, the team developed a detailed Patient Admission Assessment Form. The admitting nurse assessed each patient based on this form, considering factors such as the patient’s medical condition, treatment requirements, and potential risks. If the assessment score exceeded a predefined threshold, the attending physician conducted a reassessment to determine the patient’s risk level. Only patients with low or no risk were admitted to the day ward. This rigorous screening process helped to minimize the risk of complications and ensure patient safety.
Accurate Positioning of Infusion Chairs
To improve the efficiency and organization of the day ward, the infusion chairs were rearranged and numbered according to the departmental layout. A detailed distribution map was created and shared with the departmental work group, making it easy for staff to locate patients quickly and accurately. This measure significantly reduced the time spent on patient positioning and improved overall workflow efficiency.
Establishing a <wechat Management Group for Day Patients>
To enhance communication and coordination, the team established a WeChat Management Group that included both medical staff and day patients. The group served multiple functions:
①Facilitating the department to count the number of day patients.
②Answering questions from day patients during treatment.
③Notifying day patients of relevant treatment matters, including treatment time, infusion chair number, and the responsible nurse.
④Providing medication guidance and health education to patients.
⑤Ensuring effective communication between patients outside the ward and medical staff. The second-line duty medical staff were responsible for monitoring the group and responding to patient inquiries promptly. For patients who could not join the group due to technical or other reasons, the primary nurse made a note and informed the responsible nurse, who then notified the patient of the relevant matters by phone or face-to-face communication and conducted health education before or during treatment.
Departmental Appointment Treatment Services
To further streamline the treatment process, the team implemented a system of designated fixed shifts to provide appointment treatment services for day ward patients. The scheduling took into account various factors, including patient examination times, infusion durations, and other treatment requirements. If necessary, staggered treatment was performed to avoid overcrowding and ensure smooth patient flow. An appointment treatment registration form was created and uploaded to the WeChat group for day patients, allowing them to access their appointment details conveniently.
Providing Electronic Health Education
To enhance patient education and engagement, the team provided electronic versions of health education materials. The responsible nurse sent targeted health education content to patients based on their individual treatment plans and reminded them of important information through the WeChat group. For patients who had not joined the group, the responsible nurse conducted health education sessions before or during treatment to ensure that all patients received the necessary information After implementing these measures, the project team conducted RPN analysis of the day ward operation process and formed a new day ward operation process flowchart in Figure 2.
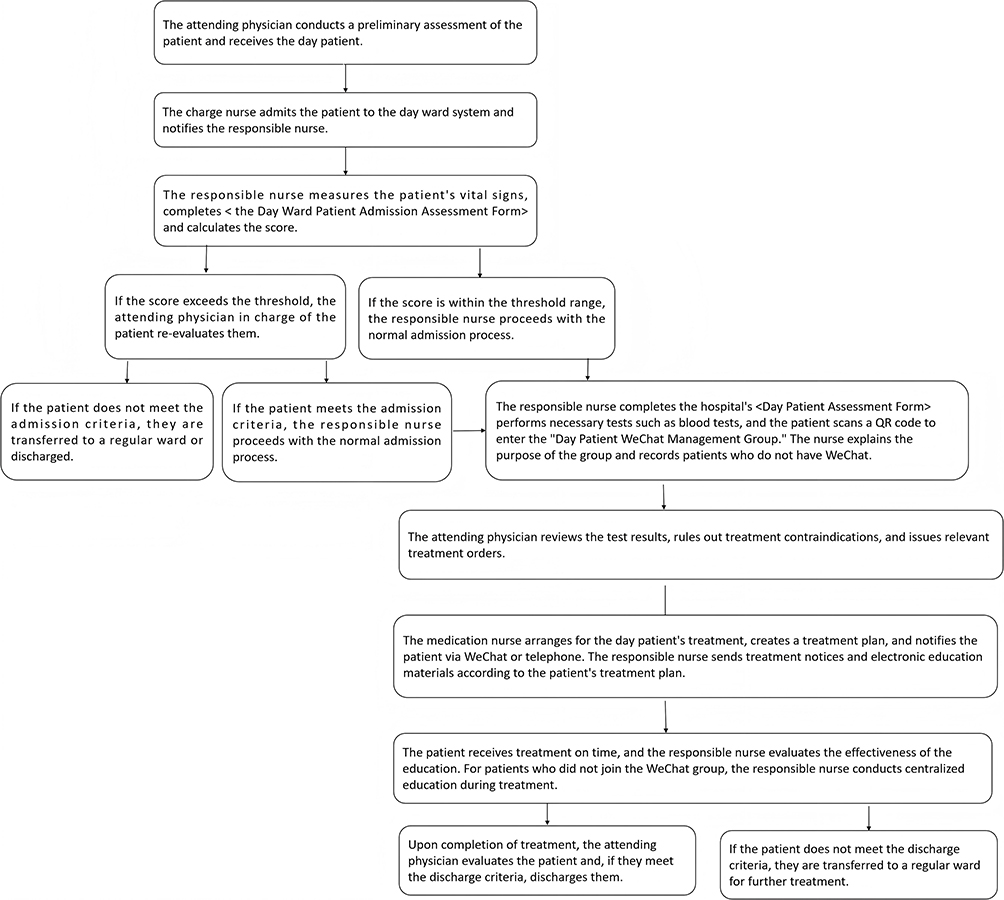 |
Figure 2 The process of the day ward after the implementation of HFMEA. |
Bias Control Measures
To minimize the potential biases inherent in the retrospective pre-post design, several methodological controls were implemented. (1) Selection Bias Control: We conducted a comprehensive comparison of baseline characteristics (including age, gender, disease type, and treatment modality) between the control and experimental groups. As reported in the General Information section, there were no statistically significant differences between the two groups (P>0.05), ensuring baseline comparability. (2) Measurement Bias Control: To avoid subjectivity in data collection, objective operational data (specifically waiting times) were retrieved directly from the hospital’s electronic information system using PDA timestamps rather than relying on manual recording or self-reporting by staff. (3) Instrument Reliability: To mitigate instrumentation bias, the patient satisfaction survey underwent rigorous internal consistency testing, yielding a Cronbach’s alpha coefficient of 0.85 prior to data analysis.
Observation Indicators
To provide a comprehensive evaluation of the day ward’s operational transformation, we selected three primary outcome measures targeting distinct domains: risk management (RPN), operational efficiency (Waiting Time), and service quality (Patient Satisfaction). (1) Treatment Waiting Time: Selected as the core indicator of efficiency. In this retrospective analysis, the robustness of this measure is secured by the use of objective digital timestamps extracted from the hospital’s PDA system, which effectively eliminates the recall bias or manual recording errors often associated with retrospective data collection. (2) Patient Satisfaction: Chosen to reflect the patient-centered impact of the process redesign. To ensure data quality, surveys were administered immediately upon patient discharge during the respective study periods (real-time collection), minimizing the risk of long-term memory bias. (3) RPN Scores: Utilized to quantify the theoretical reduction in safety risks, calculated through the standardized HFMEA consensus process.
Comparison of RPN Scores Between the Control Group and the Experimental Group
The Risk Priority Number (RPN) scores were calculated for both the control and experimental groups based on the Failure Modes and Effects Analysis (HFMEA) framework. The RPN score is calculated as Severity * Occurrence (Likelihood).
Patient Satisfaction
To assess patient satisfaction, we conducted a self-administered survey titled “Day Patient Satisfaction Survey.” The survey was designed to capture patients’ perceptions of various aspects of their care experience in the day ward. The survey included a total of 11 items, covering the following domains admission and discharge processes, treatment, health education, treatment environment, staff technical skills and attitude. Each item was rated using a Likert 5-point scoring method, with the following levels and corresponding scores, very dissatisfied (1), dissatisfied (2), neutral (3), satisfied (4), very satisfied (5). Patients were asked to rate their satisfaction with each item upon discharge or transfer from the day ward. To ensure the reliability and validity of the survey instrument, we conducted a pilot study with a small sample of patients (n=30) to test the questionnaire. The pilot study results indicated that the survey items were clear and comprehensible. Additionally, we performed a reliability analysis using Cronbach’s alpha, which yielded a coefficient of 0.85, indicating good internal consistency. The survey was then finalized and used for data collection in both the control and experimental groups.
Patient Waiting Time for Treatment
Measured the patient waiting time for treatment to evaluate the efficiency of the day ward operations. The waiting time was defined as the interval between the patient’s arrival at the ward and the start of their first treatment. The time when the patient enters the ward and reports to the nurse station. The time when the first treatment is scanned by the PDA. The waiting time was calculated by subtracting the start time from the end time.
Statistical Analysis
SPSS 22.0 will be used for statistical analysis. Given the non-normal distribution of the data, we represented the measurement data using the median (M) and interquartile range (P25, P75). The Mann–Whitney U non-parametric test will be used to compare the differences in waiting time and satisfaction between the two groups before and after the intervention. A p-value of less than 0.05 will be considered statistically significant. Additionally, we reported the Z-value from the Mann–Whitney U-test, which provides a measure of the standardized difference between the two groups.
Results
- Comparison of RPN values and improvement of potential failure modes in the control group and experimental group before and after the implementation of HFMEA (Table 2).
- Treatment waiting time for patients in the control group and experimental group (Table 3).
- Patient satisfaction in the control group and experimental group (Table 4).
 |
Table 2 Comparison of RPN Values Before and After the Implementation of HFMEA Between Groups |
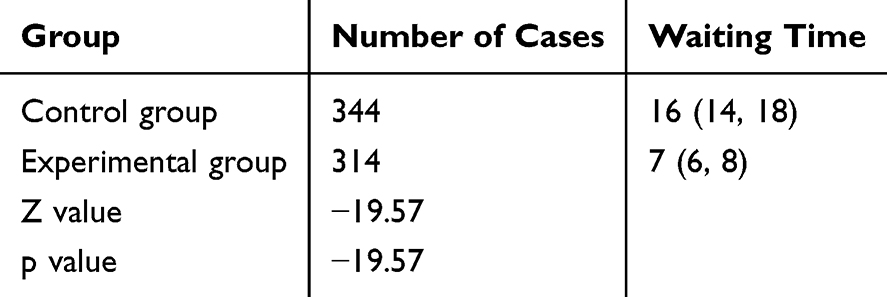 |
Table 3 Comparison of Waiting Time Between the Two Groups Before and After the Implementation of HFMEA, Presented as Median (P25, P75) |
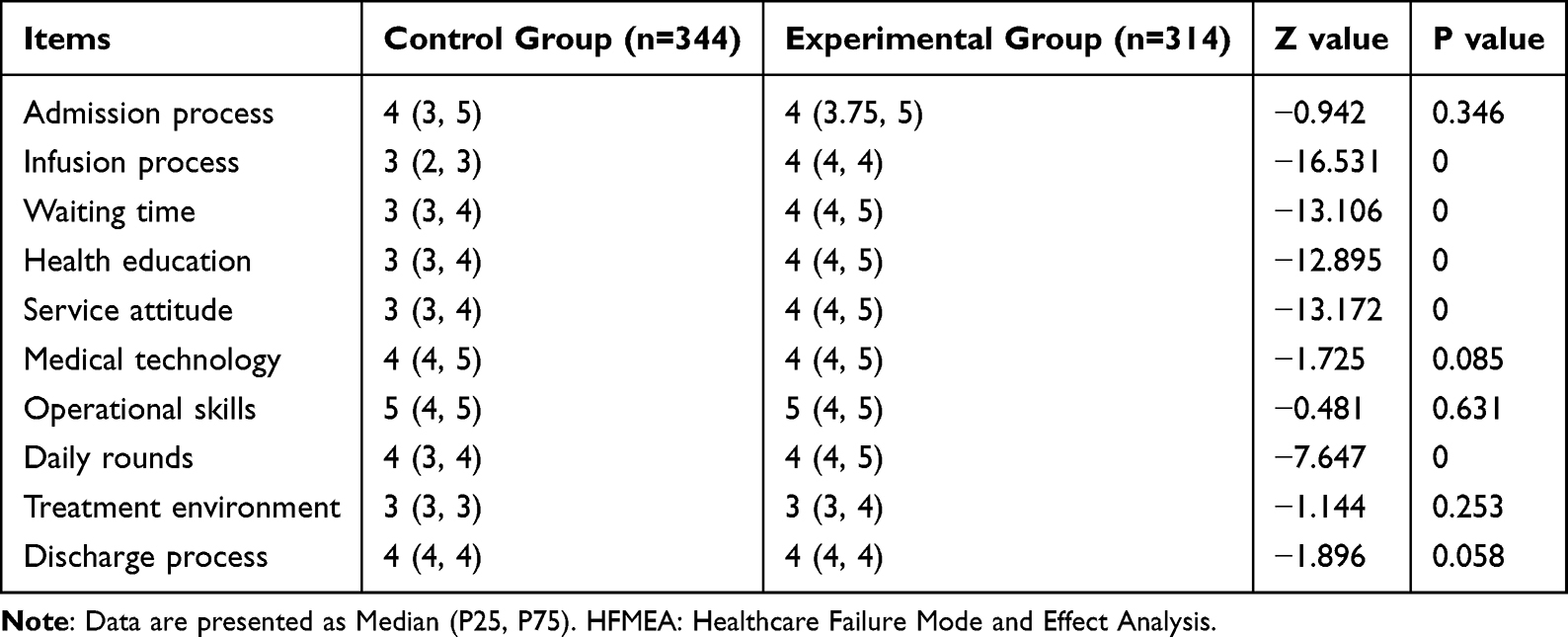 |
Table 4 Comparison of Patient Satisfaction Between the Two Groups Before and After the Implementation of HFMEA, Presented as Median (P25, P75) |
Discussion
Day wards have been recognized as a valuable strategy for enhancing the effective utilization of medical resources and alleviating the economic burden on chemotherapy patients.18 In our hospital, we established day wards to optimize patient safety, ensure that responsible medical staff are well-acquainted with each patient’s condition and treatment plan, and facilitate convenient communication between doctors and patients. However, the current model of day wards in our setting is compromised by several limitations, including the lack of comprehensive planning, suboptimal ward layout, and an unsatisfactory treatment environment, all of which negatively impact the overall medical experience of patients.19 Despite having clear admission criteria for day ward patients, our project team employed the HFMEA system to meticulously review the day ward process within our department. By integrating the department’s specific context, we applied a hazard scoring matrix to identify potential failure modes in the patient reception and evaluation stages. The resultant RPN scores of 8.33 and 8.50, respectively, highlight the necessity for targeted interventions to address these critical areas.
Initially, the department developed the Day Ward Management System at the managerial level to standardize the diagnostic and treatment practices of attending physicians, enhance staff engagement through systematic improvements, elevate service quality, and ensure medical safety.20 This comprehensive management system delineated roles and responsibilities, optimized processes, and significantly boosted overall operational efficiency. Similar initiatives have been implemented in various healthcare settings to address operational inefficiencies and enhance patient outcomes. A study by Hammoudeh S implemented a structured management system in an outpatient department, resulting in a 30% reduction in patient waiting times and a 25% increase in patient satisfaction.21 These inputs were synthesized into the Day Ward Patient Admission Evaluation Form, which was utilized to assess the suitability of patients for admission. In cases where the evaluation results diverged from the attending physician’s assessment, the chief diagnosis team’s input was incorporated, thereby ensuring patient safety through a robust three-level control mechanism. Through the clarification of responsibilities and refinement of processes, the RPN values for the two stages were substantially reduced, with improvement rates of 48.01% and 52.94%, respectively. The reduction in RPN values indicates a significant decrease in the risk of adverse events and process failures. This not only enhances patient safety but also improves the overall efficiency and reliability of the day ward operations. The improved management system and refined processes ensure that patients receive timely and appropriate care, reducing the likelihood of delays and errors.
Through interviews with day ward patients, several key issues were identified, including the absence of designated infusion chairs, ambiguous accountability of the nursing staff, prolonged waiting times for infusions, delayed fluid replacement, and concerns regarding the unavailability of physicians to address changes in patients’ conditions after leaving the ward. These challenges compromised patient safety and sense of belonging, resulting in an elevated RPN value of 8.67 for this stage. These factors were also identified as the primary contributors to the low patient satisfaction with the day ward.22,23 To address these issues, the project team implemented a series of targeted interventions. First, the infusion chairs in the day ward were rearranged and assigned specific numbers. This initiative aimed to enhance the treatment environment for day ward patients and facilitate rapid location by both patients and medical staff. Additionally, the nursing service model for day ward patients continued to follow the ward’s overall responsibility care model, in which nurses were accountable for providing comprehensive nursing services to patients. Study reported a 35% increase in patient satisfaction following the implementation of digital communication platform in a hospital setting.24 We established a WeChat group for day ward patients to provide appointment scheduling and staggered infusion services. Patients were notified via the WeChat group or phone calls, which significantly reduced the waiting time for infusions. This staggered appointment infusion service not only optimized the utilization rate of infusion chairs but also effectively maintained treatment order,25 and improved patient satisfaction. The reduction in waiting time and the improved organization of the treatment environment directly translate into enhanced patient experience. Shorter waiting times mean less anxiety and discomfort for patients, leading to higher satisfaction levels. The clear assignment of responsibilities and the use of technology to facilitate communication and coordination further contribute to a more efficient and patient-centered care environment.
The health education model based on the WeChat platform has been shown to alleviate patients’ discomfort during treatment, enhance their understanding of disease and treatment protocols, and improve nurse satisfaction.26 Given the relatively brief face-to-face interaction time between day ward patients and medical staff, effective health education interventions are crucial. Oksholm T reported significant improvements in patient satisfaction and clinical outcomes following the implementation of a health education intervention.27 In line with these findings, our project team actively leveraged the WeChat group function to disseminate health education materials tailored to each patient’s treatment plan. These materials, sorted and curated by the department, were shared with patients or their accompanying caregivers through the WeChat group. The comprehension of these materials was assessed on the day of treatment to ensure that patients received timely and relevant disease-related health knowledge. Additionally, secondary duty medical staff from the department were available online in the WeChat group, providing a communication bridge for patients to report any discomfort during treatment. Based on this real-time feedback, medical staff were able to provide effective relief measures. Enhanced health education and real-time communication through the WeChat platform empower patients with knowledge about their condition and treatment, reducing anxiety and improving their overall experience. Timely feedback and relief from medical staff further enhance patient satisfaction and trust in the healthcare system. This approach not only improves patient outcomes but also fosters a more collaborative and responsive care environment.
This study employed HFMEA to optimize risk management within the operational process of the day ward. Through a systematic and comprehensive analysis, we identified potential failure modes and subsequently reengineered the workflow to address these vulnerabilities. These targeted interventions effectively mitigated operational risks, reduced patient waiting times for infusions, and enhanced patient satisfaction. The implementation of HFMEA yielded substantial improvements in both process efficiency and patient outcomes, thereby underscoring its utility in enhancing the overall quality of care in the day ward setting. However, HFMEA itself has several limitations that may impact the results and generalizability of our study. One key limitation is the influence of subjective judgment and the personal cognitive level of project team members on the evaluation of potential failure modes.28 The identification and prioritization of failure modes rely heavily on the expertise and experience of the team members, which can introduce variability and bias.29 To mitigate this, we recommend diversifying the group members to include a broader range of perspectives and expertise. This approach can help reduce the impact of individual biases and enhance the robustness of the analysis. Beyond the inherent limitations of HFMEA, our study is also subject to several other limitations that should be considered when interpreting the results. Our study was conducted in a single center with a relatively small sample size. This limits the generalizability of our findings to other healthcare settings or populations. A larger, multi-center study would be necessary to validate our results and assess their applicability in diverse contexts. The single-center design of our study means that the results may be influenced by specific characteristics of our hospital and patient population. Factors such as local healthcare policies, resource availability, and patient demographics can vary significantly between institutions, potentially affecting the outcomes observed. Our study did not incorporate the perspectives of patient families, who often play a crucial role in the healthcare experience. Including patient families in the project team from the beginning could provide valuable insights into the patient experience and contribute to more comprehensive and patient-centered improvements. Future studies should consider involving patient families to enhance the clinical value of the interventions.
Conclusion
In summary, the optimized day ward operation process based on HFMEA is not only effective in reducing medical risks and improving patient satisfaction but also highly adaptable to various healthcare settings. We recommend that other institutions, especially those with day wards, high patient volume, outpatient departments with complex treatment protocols, similar short-stay units, consider implementing similar HFMEA-based interventions to enhance their operations.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
All experimental protocols were approved by the Ethics Committee of Affiliated Cancer Hospital of Shandong First Medical University. Informed consent was obtained from all the participants. All methods were carried out in accordance with Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was not funded by any funding.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Ibrahim H, Harhara T, Athar S, et al. Multi-disciplinary discharge coordination team to overcome discharge barriers and address the risk of delayed discharges. Risk Manage Healthcare Policy. 2022;15:141–12. doi:10.2147/RMHP.S347693
2. Gagliardi AR, Yip CYY, Irish J, et al. The psychological burden of waiting for procedures and patient‐centred strategies that could support the mental health of wait‐listed patients and caregivers during the COVID‐19 pandemic: a scoping review. Health Expectations. 2021;24(3):978–990. doi:10.1111/hex.13241
3. Atinga RA, Gmaligan MN, Ayawine A, et al. “It’s the patient that suffers from poor communication”: analyzing communication gaps and associated consequences in handover events from nurses’ experiences. SSM-Qual Res Health. 2024;6:100482. doi:10.1016/j.ssmqr.2024.100482
4. Kauppi W, Proos M, Olausson S. Ward nurses’ experiences of the discharge process between intensive care unit and general ward. Nurs Critical Care. 2018;23(3):127–133. doi:10.1111/nicc.12336
5. Zhang F, Xia Q, Zhang L, et al. A bibliometric and visualized analysis of early mobilization in intensive care unit from 2000 to 2021. Front Neurol. 2022;13:848545. doi:10.3389/fneur.2022.848545
6. Mora A, Ayala L, Bielza R, et al. Improving safety in blood transfusion using failure mode and effect analysis. Transfusion. 2019;59(2):516–523. doi:10.1111/trf.15137
7. Huang Y, Li N, Luo B, et al. Effect of hazard analysis critical control points system in the assembly of reusable medical devices. Sci Rep. 2025;15(1):9234. doi:10.1038/s41598-025-93615-z
8. Dastjerdi HA, Khorasani E, Yarmohammadian MH, et al. Evaluating the application of failure mode and effects analysis technique in hospital wards: a systematic review. J Injury Violence Res. 2017;9(1):51. doi:10.5249/jivr.v9i1.794
9. Zu F, Zhang Y, Chen Z, et al. Effect evaluation of violence in hospitalized schizophrenia patients based on HFMEA model. Chin J Nurs Manage. 2020;20(05):780–786.
10. Deandrea S, Tidone E, Bellini A, et al. Implementation of failure mode and effects analysis to the specimens flow in a population-based colorectal cancer screening programme using immunochemical faecal occult blood tests: a quality improvement project in the Milan colorectal cancer screening programme. BMJ Open Quality. 2018;7(1):e000299. doi:10.1136/bmjoq-2017-000299
11. Vecchia M, Sacchi P, Marvulli LN, et al. Healthcare application of Failure Mode and Effect Analysis (FMEA): is there room in the infectious disease setting? A scoping review. Healthcare Multidisciplin Digital Publish Instit. 2025;13(1):82.
12. Pueyo-López C, Sánchez-Cuervo M, Vélez-Díaz-Pallarés M, et al. Healthcare failure mode and effect analysis in the chemotherapy preparation process. J Oncol Pharm Pract. 2021;27(7):1588–1595. doi:10.1177/1078155220962189
13. Pirouzi M, A GH, Ravaghi H, et al. Health care failure mode and effect analysis in the operating room setting. Qual Manage Healthcare. 2020;29(4):234–241.
14. Ouellette-Piazzo K, Asfaw B, Cowen J. CT healthcare failure mode effect analysis (HFMEA): the misadministration of IV contrast in outpatients. Radiol Manage. 2007;29(1):36–44.
15. Holmes J, Chipman M, Barbour T, et al. A simulation systems testing program using HFMEA methodology can effectively identify and mitigate latent safety threats for a new on-site helipad. Joint Commission J Qual Patient Saf. 2022;48(1):12–24. doi:10.1016/j.jcjq.2021.09.013
16. Zhang Y, Dong C, Guo W, et al. Systems theoretic accident model and process (STAMP): a literature review. Safety Science. 2022;152:105596. doi:10.1016/j.ssci.2021.105596
17. DeRosier J, Stalhandske E, Bagian JP, Nudell T. Using health care failure mode and effect analysis: the VA National Center for Patient Safety’s prospective risk analysis system. Jt Comm J Qual Improv. 2002;28(5):248–267. doi:10.1016/s1070-3241(02)28025-6
18. Tan X, Luo L, Zhao W, et al. Investigation on the opening demand of oncology day chemotherapy ward in Sichuan Provincial Second- and Tertiary Hospital. China Med Sci. 2021;11(06):164–167.
19. Luo L, Wang G, Tan X, et al. Investigation on the management status of oncology day chemotherapy ward in secondary and tertiary hospitals in Sichuan Province. Chin J Modern Nurs. 2020;(03):287–292.
20. Zeng R, Liu J, Weng Y, et al. Preliminary study on the construction of modern hospital management system in county-level hospitals. Chin J Hospital Manage. 2021;37(Z1):12–13.
21. Hammoudeh S, Amireh A, Jaddoua S, et al. The impact of lean management implementation on waiting time and satisfaction of patients and staff at an outpatient pharmacy of a comprehensive cancer center in Jordan. Hospital Pharmacy. 2021;56(6):737–744. doi:10.1177/0018578720954147
22. Fan G, Xu X, Lin Z, et al. Differences between two types of day ward management mode and their effects. Chin J Nurs Manage. 2015;15(10):1244–1247.
23. Wang L, Wang F, Shu C. Research on the development status of tumor day ward in China. J Nurs Train. 2016;31(19):1750–1752.
24. Kitsios F, Stefanakakis S, Kamariotou M, et al. Digital service platform and innovation in healthcare: measuring users’ satisfaction and implications. Electronics. 2023;12(3):662. doi:10.3390/electronics12030662
25. Zhang H, Lu Y, Yu W, et al. Exploration and practice of intraday chemotherapy mode in cancer hospital. Chin J Nurs Manage. 2020;20(01):7–10.
26. Shi J, Wang X. Application effect of nursing education model based on WeChat platform in patients undergoing day surgery in thoracic surgery. Int J Nurs. 2022;18(41):3345–3348.
27. Oksholm T, R GK, Hunskår I, et al. The effect of transitions intervention to ensure patient safety and satisfaction when transferred from hospital to home health care—A systematic review. J Adv Nurs. 2023;79(6):2098–2118. doi:10.1111/jan.15579
28. Gao M, Shang S. Research analysis on FMEA Failure Mode and Effect Analysis: based on SCI/SSCI Journal Literature since 2015. Shanghai J Manage Sci. 2019;41(1):118–125.
29. Li S, Zhan Y, Xin Yu J, Li M, Chen Y. Visual analysis of International Research Hotspots on Patient Safety Based on Web of Science. Chin J Pract Nurs. 2021;37(15):1176–1184.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.